
The Prevalence of Diabetes among Hypertensive Polish in Relation to Sex-Difference in Body Mass Index, Waist Circumference, Body Fat Percentage and Age

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Analysis
2.2. Statistical Analysis
3. Results
3.1. Analysed Group Characteristics
3.2. Diabetic Patients
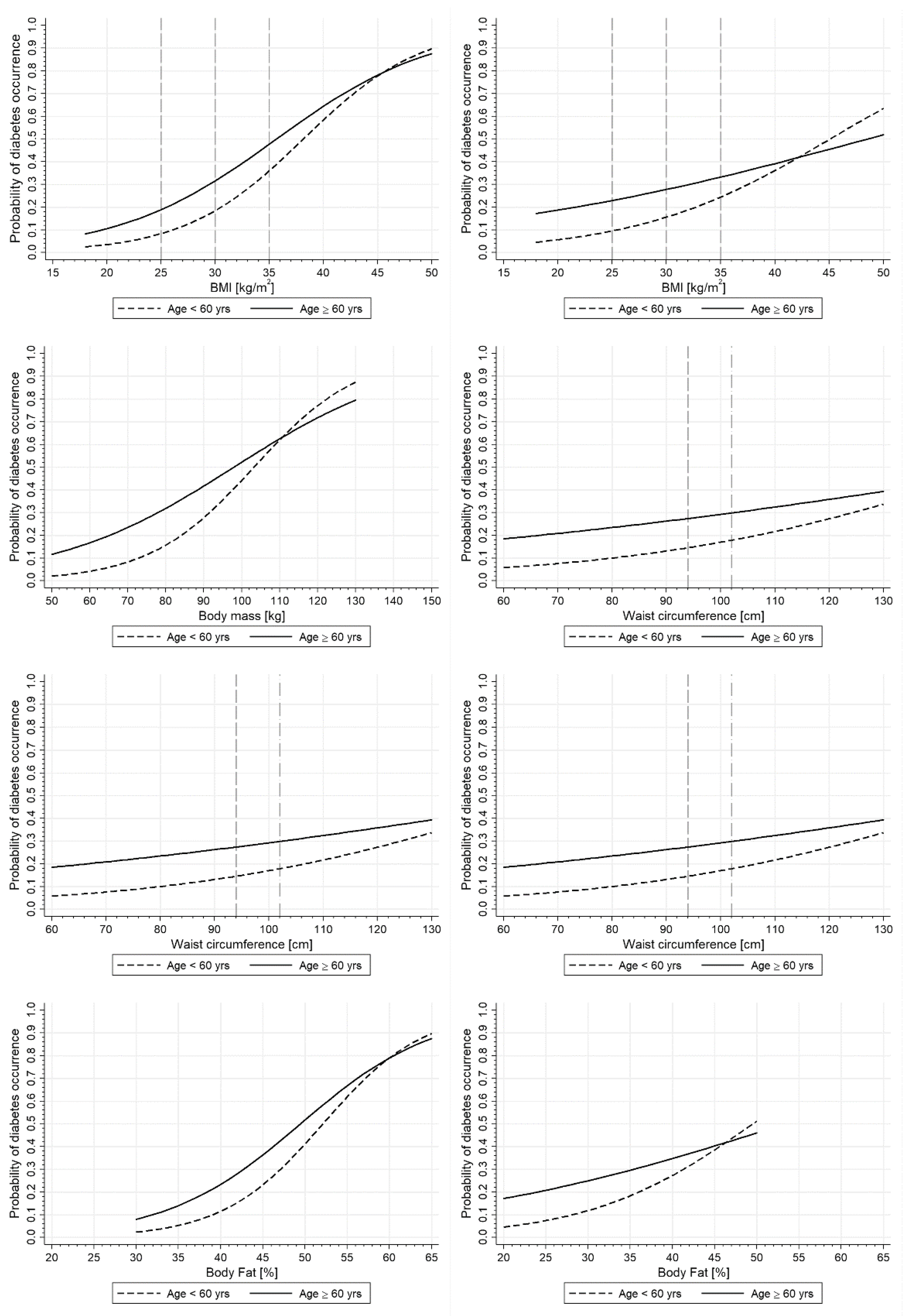
3.3. Sex-Specific Age-Stratified Differences in the Prevalence of Diabetes in Relation to Anthropometric Parameters
3.4. Prevalence of Diabetes in Specific BMI and WC Cutoff Points in Men and Women (Adjusted for Lifestyle)
3.5. Association between Sex and the Prevalence of Diabetes in Logistic-Regression Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hill, J.J. Obesity: An emerging threat. J. Natl. Black Nurses Assoc. JNBNA 2018, 29, 36–39. [Google Scholar]
- Dite, P.; Blaho, M.; Bojkova, M.; Jabandziev, P.; Kunovsky, L. Nonalcoholic Fatty Pancreas Disease: Clinical Consequences. Dig. Dis. 2020, 38, 143–149. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in diabetes since 1980: A pooled analysis of 751 population-based studies with 4.4 million participants. Lancet 2016, 387, 1513–1530, Erratum in: Lancet 2017, 389, e2. [Google Scholar]
- Kodoth, V.; Scaccia, S.; Aggarwal, B. Adverse Changes in wcposition During the Menopausal Transition and Relation to Cardiovascular Risk: A Contemporary Review. Womens Health Rep. (New Rochelle) 2022, 3, 573–581. [Google Scholar]
- Makizako, H.; Shimada, H.; Doi, T.; Tsutsumimoto, K.; Lee, S.; Lee, S.C.; Harada, K.; Hotta, R.; Nakakubo, S.; Bae, S.; et al. Age-dependent changes in physical performance and body composition in community-dwelling Japanese older adults. J. Cachexia Sarcopenia Muscle 2017, 8, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Mackenzie, T.A.; Barre, L.K.; Lopez-Jimenez, F.; Bartels, S.J. Sarcopenia, sarcopenic obesity and mortality in older adults: Results from the National Health and Nutrition Examination Survey III. Eur. J. Clin. Nutr. 2014, 68, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Ming, Y.; Robson, P.J.; Eurich, D.T.; Vena, J.E.; Xu, J.; Johnso, J.A. Anthropometric changes and risk of diabetes: Are there sex differences? A longitudinal study of Alberta’s Tomorrow Project. BMJ Open 2019, 9, e023829. [Google Scholar]
- Tatsumi, Y.; Watanabe, M.; Nakai, M.; Kokubo, Y.; Higashiyama, A.; Nishimura, K.; Kobayashi, T.; Takegami, M.; Nakao, Y.M.; Watanabe, T.; et al. Changes in Waist Circumference and the Incidence of Type 2 Diabetes in Community-Dwelling Men and Women: The Suita Study. J. Epidemiology 2015, 25, 489–495. [Google Scholar] [CrossRef]
- Escobar-Morreale, H.F.; Alvarez-Blasco, F.; Botella-Carretero, J.I.; Luque-Ramírez, M. The striking similarities in the metabolic associations of female androgen excess and male androgen deficiency. Hum. Reprod. 2014, 29, 2083–2091. [Google Scholar] [CrossRef]
- Paquette, A.; Chapados, N.A.; Bergeron, R.; Lavoie, J.M. Fatty acid oxidation is decreased in the liver of ovariectomized rats. Horm. Metab. Res. 2009, 41, 511515. [Google Scholar] [CrossRef]
- Aune, D.; Norat, T.; Leitzmann, M.; Tonstad, S.; Vatten, L.J. Physical activity and the risk of type 2 diabetes: A systematic review and dose-response meta-analysis. Eur. J. Epidemiol. 2015, 30, 529–542. [Google Scholar] [CrossRef] [PubMed]
- Alwash, S.M.; McIntyre, H.D.; Mamun, A. The association of general obesity, central obesity and visceral body fat with the risk of gestational diabetes mellitus: Evidence from a systematic review and meta-analysis. Obes. Res. Clin. Pract. 2021, 15, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Forte, R.; Pesce, C.; De Vito, G.; Boreham, C.A. The Body Fat-Cognition Relationship in Healthy Older Individuals: Does Gynoid vs Android Distribution Matter? J. Nutr. Health Aging 2017, 21, 284–291. [Google Scholar] [CrossRef]
- Mauvais-Jarvis, F. Sex differences in metabolic homeostasis, diabetes, and obesity. Biol. Sex Differ. 2015, 6, 14. [Google Scholar] [CrossRef]
- Pavankumar, P.; Abate, N. Body Fat Distribution and Insulin Resistance. Nutrients 2013, 5, 2019–2027. [Google Scholar]
- Haghighatdoost, F.; Amini, M.; Feizi, A.; Iraj, B. Are body mass index and waist circumference significant predictors of diabetes and prediabetes risk: Results from a population based cohort study. World J. Diabetes 2017, 8, 365–373. [Google Scholar] [CrossRef]
- Ryu, S.; Chang, Y.; Jung, H.S.; Yun, K.E.; Kwon, M.J.; Choi, Y. Relationship of sitting time and physical activity with non-alcoholic fatty liver disease. J. Hepatol. 2015, 63, 1229–1237. [Google Scholar] [CrossRef] [PubMed]
- Adams, L.A.; Waters, O.R.; Knuiman, M.W.; Elliott, R.R.; Olynyk, J.K. NAFLD as a risk factor for the development of diabetes and the metabolic syndrome: An eleven-year follow-up study. Am. J. Gastroenterol. 2009, 104, 861–867. [Google Scholar] [CrossRef]
- Chudek, A.; Owczarek, A.J.; Ficek, J.; Almgren-Rachtan, A.; Chudek, J. Lower utilization of home blood pressure monitoring in younger, poorly educated hypertensive males—Real-life data. Blood Press. 2020, 29, 95–102. [Google Scholar] [CrossRef]
- A Healthy Lifesty—WHO Recommendations. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 30 April 2022).
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar]
- Molina-Luque, R.; Yañez, A.M.; Bennasar-Veny, M.; Romero-Saldaña, M.; Molina-Recio, G.; López-González, Á.A. A Comparison of Equation Córdoba for Estimation of Body Fat (ECORE-BF) with Other Prediction Equations. Int. J. Environ. Res. Public Health 2020, 17, 7940. [Google Scholar] [CrossRef] [PubMed]
- Olszanecka-Glinianowicz, M.; Chudek, J.; Kocełak, P.; Szromek, A.; Zahorska-Markiewicz, B. Body fat changes and activity of tumor necrosis factor α system—A 5-year follow-up study. Metabolism 2011, 60, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Janice, L. Atkins. Chapter 7—Stéphane Walrand. Effects of Sarcopenic Obesity on Cardiovascular Disease and All-Cause Mortality. In Nutrition and Skeletal Muscle; Academic Press: Cambridge, MA, USA, 2019; pp. 93–103. [Google Scholar]
- Ćwirlej-Sozańska, A.; Widelak, M.; Wiernasz, M.; Wawrzykowska, I.; Turkosz, N. An assessment of the work ability, disability and quality of life of working people of pre-retirement and retirement age in Poland—A cross-sectional pilot study. Int. J. Occup. Med. Environ. Health 2021, 34, 69–85. [Google Scholar] [CrossRef] [PubMed]
- Stepaniak, U.; Micek, A.; Waśkiewicz, A.; Bielecki, W.; Drygas, W.; Janion, M.; Kozakiewicz, K.; Niklas, A.; Puch-Walczak, A.; Pająk, A. Prevalence of general and abdominal obesity and overweight among adults in Poland. Results of the WOBASZ II study (2013–2014) and comparison with the WOBASZ study (2003–2005). Pol. Arch. Intern. Med. 2016, 126, 662–671. [Google Scholar] [CrossRef]
- Topor-Madry, R.; Wojtyniak, B.; Strojek, K.; Rutkowski, D.; Bogusławski, S.; Ignaszewska-Wyrzykowska, A.; Jarosz-Chobot, P.; Czech, M.; Kozierkiewicz, A.; Chlebus, K.; et al. Prevalence of diabetes in Poland: A combined analysis of national databases. Diabet. Med. 2019, 36, 1209–1216. [Google Scholar] [CrossRef]
- Petrie, J.R.; Guzik, T.J.; Touyz, R.M. Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms. Can. J. Cardiol. 2018, 34, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes—Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2020, 10, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Puzianowska-Kuźnicka, M.; Januszkiewicz-Caulier, J.; Kuryłowicz, A.; Mossakowska, M.; Zdrojewski, T.; Szybalska, A.; Skalska, A.; Chudek, J.; Franek, E. Prevalence and socioeconomic predictors of diagnosed and undiagnosed diabetes in oldest-old and younger Caucasian seniors: Results from the PolSenior study. Endokrynol. Pol. 2021, 72, 249–255. [Google Scholar] [CrossRef]
- St-Onge, M.-P. Relationship between body composition changes and changes in physical function and metabolic risk factors in aging. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Atlantis, E.; Martin, S.A.; Haren, M.T.; Taylor, A.W.; Wittert, G.A. Lifestyle factors associated with age-related differences in body composition: The Florey Adelaide Male Aging Study. Am. J. Clin. Nutr. 2008, 88, 95–104. [Google Scholar]
- IDF Diabetes Atlas Ninth Edition 2019. Available online: https://www.diabetesatlas.org/upload/resources/material/20200302_133351_IDFATLAS9e-final-web.pdf (accessed on 24 July 2022).




{kind=link}
{kind=link}
{kind=link}
| Men [N = 6126] | Women [N = 6163] | |||
|---|---|---|---|---|
| <60 Years [N = 3149] | ≥60 Years [N = 2977] | <60 Years [N = 2528] | ≥60 Years [N = 3635] | |
| Age [years] | 48 ± 8 | 69 ± 7 | 50 ± 7 | 70 ± 7 |
| Active or passed smokers [N; %] | 1640; 52.1 | 1148; 38.8 # | 813; 32.3 | 754; 20.9 # |
| Alcohol consumers [N; %] | 1844; 58.9 | 1103; 37.4 # | 586; 23.6 | 506; 14.1 # |
| Sedentary lifestyle [N; %] | 1715; 67.8 | 1736; 76.4 # | 1510; 76.3 | 2083; 84.0 # |
| Body mass [kg] | 92.7 ± 13.6 | 91.8 ± 14.9 * | 77.3 ± 13.8 | 79.0 ± 13.2 # |
| BMI [kg/m2] | 29.6 ± 4.4 | 30.2 ± 4.9 # | 28.1 ± 5.3 | 29.6 ± 5.0 # |
| Underweight (BMI < 18.5) [N; %] | 0 | 18; 0.6 | 18; 0.7 | 0 |
| Normal weight (BMI 18.5–24.9) [N; %] | 338; 10.7 | 292; 9.8 | 698; 27.6 | 565; 15.5 # |
| Overweight (BMI 25.0–29.9) [N; %] | 1519; 48.2 | 1276; 42.9 # | 991; 39.2 | 1435; 39.5 |
| Obesity (BMI ≥ 30) [N; %] | 1292; 41.1 | 1391; 46.7 # | 821; 32.5 | 1635; 45.0 # |
| Body fat [%] | 32.7 ± 4.7 | 33.4 ± 5.2 # | 41.3 ± 5.6 | 42.9 ± 5.2 # |
| Waist circumference [WC] [cm] | 95.8 ± 13.2 | 96.4 ± 13.2 | 87.5 ± 13.4 | 90.6 ± 14.4 # |
| WC < 80 (W) and 94 (M) [N; %] | 1272; 40.4 | 1185; 39.8 | 775; 30.7 | 902; 24.8 # |
| WC 80–87.5 (W) and 94–101.5 (M) [N; %] | 877; 27.8 | 819; 27.5 | 486; 19.2 | 708; 19.5 |
| WC ≥ 88 (W) and 102 (M) [N; %] | 1000; 31.8 | 973; 32.7 | 1267; 50.1 | 2025; 55.7 # |
| Diabetes [N; %] | 521; 16.5 | 854; 28.7 # | 453; 17.9 | 1152; 31.7 # |
| Other diseases [N; %] | ||||
| Coronary artery disease | 628; 19.9 | 1305; 43.8 # | 337; 13.3 | 1353; 37.2 # |
| Peripheral artery disease | 223; 7.1 | 388; 13.0 # | 69; 2.7 | 399; 11.0 # |
| Heart failure | 175; 5.6 | 605; 20.3 # | 63; 2.5 | 539; 14.8 # |
| Severe chronic kidney disease | 142; 4.5 | 415; 13.9 # | 79; 3.1 | 237; 6.5 # |
| Hypercholesterolemia | 1537; 48.8 | 1710; 57.4 # | 1019; 40.3 | 1816; 50.0 # |
| Diabetics [N = 2980] | Non-Diabetics [N = 9309] | |
|---|---|---|
| Age [years] | 65 ± 12 | 58 ± 13 # |
| Age ≥ 60 years [N; %] | 2006; 67.3 | 4606; 49.5 # |
| Sex | ||
| Men [N; %] | 1375; 46.1 | 4751; 51.0 # |
| Women [N; %] | 1605; 53.9 | 4558; 49.0 # |
| Active or passed smokers [N; %] | 1146; 38.7 | 3209; 34.6 # |
| Pack-years [N] | 24 ± 15 | 19 ± 13 # |
| Alcohol consumers [N; %] | 795; 27.0 | 3244; 35.2 # |
| Sedentary lifestyle [N; %] | 2475; 83.1 | 6862; 73.7 # |
| Body mass [kg] | ||
| Men | 95.0 ± 12.5 | 91.5 ± 14.6 # |
| Women | 85.1 ± 14.1 | 75.9 ± 12.4 # |
| Body mass index (BMI) [kg/m2] | 31.6 ± 4.7 | 28.8 ± 4.8 # |
| Underweight BMI < 18.5 kg/m2) | 0 | 36; 0.4 # |
| Normal weight (BMI 18.5–24.9 kg/m2) | 158; 5.3 | 1735; 18.6 # |
| Overweight (BMI 25.0–29.9 kg/m2) | 961; 32.2 | 4260; 45.8 # |
| Obesity (BMI ≥ 30 kg/m2) | 1861; 62.4 | 3278; 35.2 # |
| Body fat [%] | 40.3 ± 7.4 | 36.8 ± 6.6 # |
| Waist circumference (WC) | ||
| WC < 80 cm (W) 94 cm (M) | 604; 20.3 | 3530; 37.9 # |
| WC 80–87.5 cm (W) 94–101.5 cm (M) | 647; 21.7 | 2243; 24.1 # |
| WC ≥ 88 cm (W) 102 cm (M) | 1729; 58.0 | 3536; 38.0 # |
| Co-morbidities [N; %] | ||
| Coronary artery disease | 1440; 48.3 | 2183; 23.5 # |
| Peripheral artery disease | 289; 9.7 | 790; 8.5 * |
| Heart failure | 567; 19.0 | 815; 8.8 # |
| Severe chronic kidney disease | 377; 12.7 | 496; 5.3 # |
| Hypercholesterolemia | 1689; 56.7 | 4393; 47.2 # |
| BMI (kg/m2) | Body Mass (kg) | Waist Circumference (cm) | Body Fat (%) | |||||
|---|---|---|---|---|---|---|---|---|
| <60 years | ||||||||
| Probability of DM | Women | Men | Women | Men | Women | Men | Women | Men |
| 25% | 32.1 | 35.3 | 88.1 | 113.5 | 100.7 | 116.1 | 45.6 | 38.9 |
| 50% | 38.4 | 45.1 | 103.2 | 151.3 | 125.7 | 152.2 | 52.1 | 49.7 |
| ≥60 years | ||||||||
| 25% | 27.6 | 27.2 | 72.0 | 82.0 | 83.7 | 85.5 | 40.7 | 30.1 |
| 50% | 35.7 | 48.5 | 97.9 | 150.5 | 109.9 | 158.8 | 49.5 | 53.4 |
| Number (N) | Diabetes N (%) | Univariate OR (95%CI) | Model for BMI ≥ 30 kg/m2 OR (95%CI) | Model for WC ≥ 80/94 cm OR (95%CI) | Model for WC ≥ 88/102 cm OR (95%CI) | |
|---|---|---|---|---|---|---|
| Age ≥ 60 years | Y (6612) | 2006 (30.3) | 2.10 (1.93–2.29) # | 1.87 (1.70–2.04) # | 1.95 (1.79–2.14) # | 1.96 (1.79–2.14) # |
| N (5677) | 974 (17.2) | Ref | Ref | Ref | Ref | |
| Gender | M (N = 6126) | 1375 (22.4) | 0.82 (0.76–0.89) # | 0.89 (0.82–0.98) * | Not significant | 1.15 (1.05–1.26) * |
| W (N = 6163) | 1605 (26.0) | Ref | Ref | Ref | Ref | |
| Alcohol consumers | Y (4039) | 795 (19.7) | 0.68 (0.62–0.75) # | 0.84 (0.76–0.93) # | 0.81 (0.73–0.89) # | 0.77 (0.70–0.85) # |
| N (8250) | 2185 (26.5) | Ref | Ref | Ref | Ref | |
| Sedentary lifestyle | Y (9337) | 2475 (26.5) | 1.75 (1.57–1.94) # | 1.44 (1.29–1.61) # | 1.50 (1.35–1.68) # | 1.50 (1.35–1.68) # |
| N (2952) | 505 (17.1) | Ref | Ref | Ref | Ref | |
| BMI ≥ 30 kg/m2 | Y (N = 5139) | 1861 (36.2) | 6.23 (5.25–7.41) # | 2.89 (2.25–3.15) # | – | – |
| BMI 18.5–24.9 (1893) | 158 (8.3) | Ref | Ref | NI | NI | |
| WC ≥ 80 cm (W) 94 cm (M) | Y (8155) | 2376 (29.1) | 2.40 (2.18–2.65) # | – | 2.29 (2.07–2.53) # | – |
| N (4134) | 604 (14.6) | Ref | NI | Ref | NI | |
| WC ≥ 88 cm (W) 102 cm (M) | Y (5265) | 1729 (32.8) | 2.86 (2.58–3.17) # | – | – | 2.21 (2.02–2.41) # |
| WC < 80/94 (4134) | 604 (14.6) | Ref | NI | NI | Ref |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bednarek, A.M.; Owczarek, A.J.; Chudek, A.; Almgren-Rachtan, A.; Wieczorowska-Tobis, K.; Olszanecka-Glinianowicz, M.; Chudek, J. The Prevalence of Diabetes among Hypertensive Polish in Relation to Sex-Difference in Body Mass Index, Waist Circumference, Body Fat Percentage and Age. Int. J. Environ. Res. Public Health 2022, 19, 9458. https://doi.org/10.3390/ijerph19159458
Bednarek AM, Owczarek AJ, Chudek A, Almgren-Rachtan A, Wieczorowska-Tobis K, Olszanecka-Glinianowicz M, Chudek J. The Prevalence of Diabetes among Hypertensive Polish in Relation to Sex-Difference in Body Mass Index, Waist Circumference, Body Fat Percentage and Age. International Journal of Environmental Research and Public Health. 2022; 19(15):9458. https://doi.org/10.3390/ijerph19159458
Chicago/Turabian StyleBednarek, Anna Maria, Aleksander Jerzy Owczarek, Anna Chudek, Agnieszka Almgren-Rachtan, Katarzyna Wieczorowska-Tobis, Magdalena Olszanecka-Glinianowicz, and Jerzy Chudek. 2022. "The Prevalence of Diabetes among Hypertensive Polish in Relation to Sex-Difference in Body Mass Index, Waist Circumference, Body Fat Percentage and Age" International Journal of Environmental Research and Public Health 19, no. 15: 9458. https://doi.org/10.3390/ijerph19159458