
A Survey on the Knowledge, Attitudes, and Practices of Lebanese Physicians Regarding Air Pollution

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Knowledge of Pollutants and Sources of Air Pollution
3.2. Practices Related to the Discussion of Air Pollution with Patients
3.3. Attitudes Related to Inclusion of Air Pollution in Practice and Training
3.4. Correlation between Demographics of the Participants and Their Knowledge and Attitudes about Air Pollution
3.5. Correlation between Knowledge of Physicians and Their Practices and Attitudes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Questionnaire
- 1.
- Which of the below do you think are sources of air pollution?
Humidity Yes No Do not know Construction work Yes No Do not know Cars Yes No Do not know Incinerators Yes No Do not know Urban gardens Yes No Do not know Diesel generators Yes No Do not know Dust storms Yes No Do not know Trees Yes No Do not know - 2.
- Which of the below substances do you think are air pollutants?
Dust Yes No Do not know Smoke other than tobacco Yes No Do not know Water vapor Yes No Do not know Smell of perfume Yes No Do not know Smell of sewage Yes No Do not know - 3.
- Below is a list of living conditions. To what extent do you agree that each case is associated with exposure to air pollution?
Living Condition Strongly Agree Agree Neutral Disagree Strongly Disagree Living near an open and well-ventilated road intersection Living near a gas station Living near a diesel generator’s exhaust Living near car or bus parking Living near a construction site Living in a house with a garden Living near a garbage incinerator Staying indoors most of the time Living on higher-level floors (>third floor) Living near a busy traffic intersection Living near an open garbage dump Smoking electronic cigarettes (IQOS) Smoking tobacco cigarettes Smoking arguileh Living on lower-level floors (≤third floor) Living near an airport Living near an agricultural field Living with a person who smokes - 4.
- To what extent do you agree that each of the below working conditions is associated with exposure to air pollution?
Work Condition: Working… Strongly Agree Agree Neutral Disagree Strongly Disagree at a gas station in a place where smoking is NOT allowed as a tour guide at a clinic in a hospital in an automobile repair shop at a gardening shop at a construction site in a chemical lab with paints in a place where smoking is allowed as a teacher in a place where only vaping (ICOS) is allowed as a farmer - 5.
- To what extent do you think that each of the below household sources or activities is associated with increased exposure to air pollution?
Household Item Strongly Agree Agree Neutral Disagree Strongly Disagree Chimney Candles Wood heaters Indoor smoking Detergents [Odex or Flash] Watching television Air conditioning unit Vacuum cleaners Pets Indoor cooking Pesticides and insecticides Mold and fungi on the walls Air fresheners Glues/adhesives Taking a shower Open windows at home Lighting charcoal for arguileh at home Diesel heaters indoors - 6.
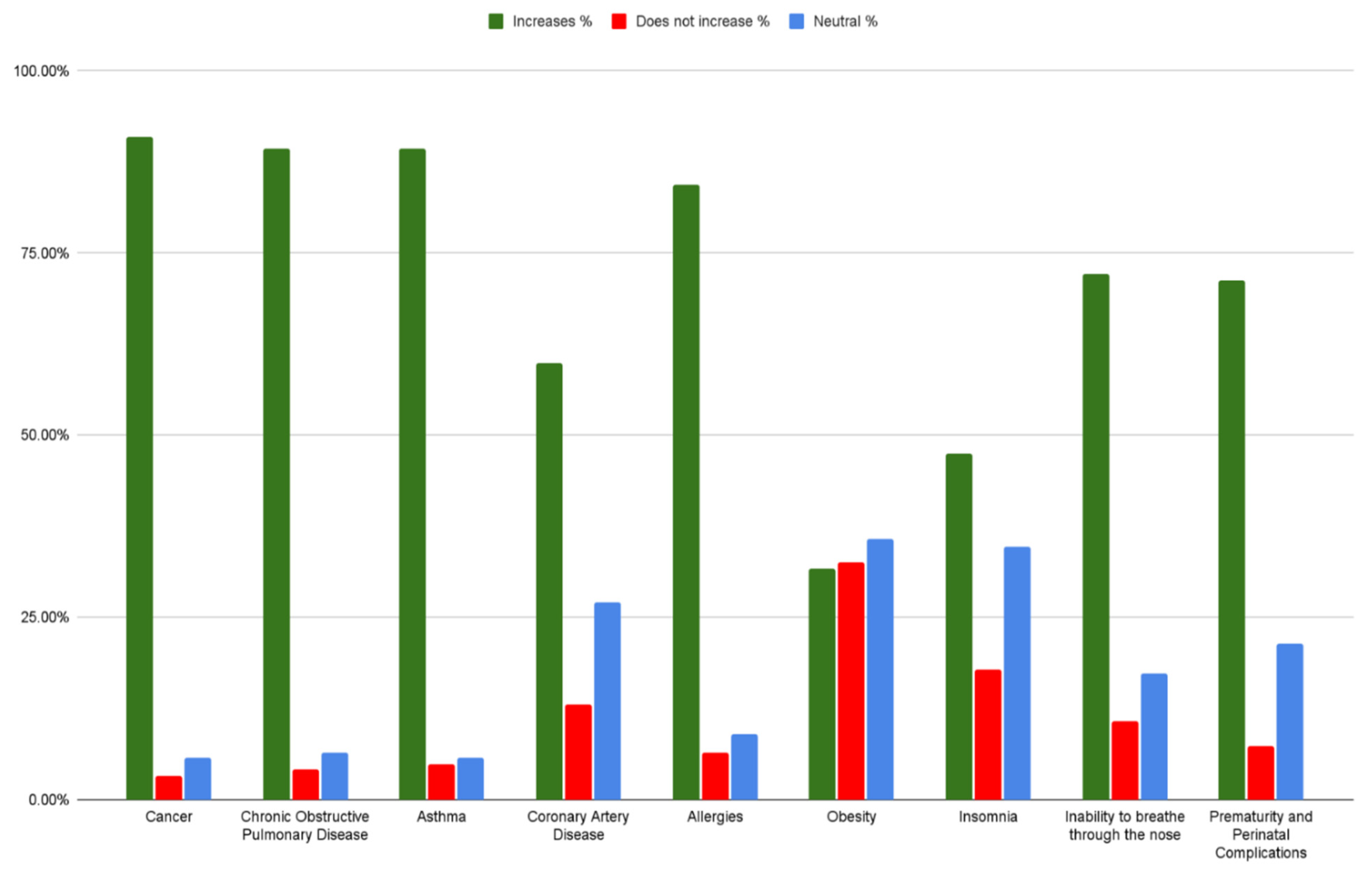
- To what extent do you think that air pollution increases the risk for the following health conditions?
Health Problem Majorly
Increases RiskModerately
Increases RiskNeutral Increases Risk a Little Does Not
Increase Risk at AllCancer Chronic obstructive pulmonary disease Asthma Coronary artery disease Allergies Obesity Insomnia Inability to breathe through the nose Prematurity and perinatal complications - 7.
- Do you think that increased air pollution levels are linked to the severity of an illness or disease?
Not at all A little bit Moderately A lot Extremely - 8.
- How often do you ask your patients whether they are exposed to air pollutants?
Not at all Rarely Sometimes Most of the
timeAlways - 9.
- What would trigger you to ask your patient about his or her exposure to air pollution?
- I always ask as part of my routine history taking.
- I ask if the patient mentions particular symptom(s); please specify:_________________________.
- I ask if the patient or caregiver mentions something that suggests such exposure.Give an example: ______________________________
- I ask if the case is difficult to diagnose and requires further investigation.
- 10.
- How important it is to you to ask your patients about their exposure to air pollutants?
Not at all important Somewhat important Important Very important Extremely important - 11.
- Do you think that you have a role in reducing air pollution?
- No, I do not have a role.
- Yes, I do have a role as a physician.
- Yes, I do have a role as a citizen.
- b and c
- 12.
- How confident are you in your ability to counsel your patients to reduce their exposure to air pollution?
Not at all confident Somewhat confident Confident Very confident Extremely confident - 13.
- How interested are you in attending training/continuing education about air pollution?
Not at all interested Somewhat interested Interested Very interested Extremely interested - 14.
- To what extent do you support the application of a plan (national or institutional) that includes a section on air pollution during patients’ regular medical assessment to raise awareness about air pollution exposure?
Strongly support Support Neutral Do not support Strongly do not
support
Appendix A.2. Demographics
- 1.
- What is your sex?
- Male
- Female
- 2.
- How old are you?
- <30 years
- 30–39 years
- 40–49 years
- 50+ years
- 3.
- How long have you been practicing?
- Less than 1 year
- 1–5 years
- 6–10 years
- 11–15 years
- 16–20 years
- 20+ years
- 4.
- What is your specialty?
- Cardiology
- Pulmonary medicine
- Family medicine
- Oncology
- Pediatrics
- Infectious diseases
- Allergy
- Obstetrics
- Otolaryngology (ENT)
- Emergency medicine
- General practice
- 5.
- Do you hold an educational degree other than your medical degree, such as in public health?
- No
- Yes. Please specify:
- 6.
- In what Muhafaza do you practice?
- Beirut
- Mount Lebanon
- North Lebanon
- Bekaa
- South Lebanon
References
- World Health Organization. Ambient Air Pollution. 13 November 2021. Available online: https://www.who.int/data/gho/data/themes/air-pollution/ambient-air-pollution (accessed on 31 January 2022).
- Beelen, R.; Raaschou-Nielsen, O.; Stafoggia, M.; Andersen, Z.J.; Weinmayr, G.; Hoffmann, B.; Wolf, K.; Samoli, E.; Fischer, P.; Nieuwenhuijsen, M.; et al. Effects of long-term exposure to air pollution on natural-cause mortality: An analysis of 22 European cohorts within the multicentre ESCAPE project. Lancet 2014, 383, 785–795. [Google Scholar] [CrossRef]
- Rajagopalan, S.; Brauer, M.; Bhatnagar, A.; Bhatt, D.L.; Brook, J.R.; Huang, W.; Münzel, T.; Newby, D.; Siegel, J.; Brook, R.D.; et al. Personal-Level Protective Actions against Particulate Matter Air Pollution Exposure: A Scientific Statement from the American Heart Association. Circulation 2020, 142, e411–e431. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [Green Version]
- Rotily, M.; Trémolières, L.; Armengaud, A.; Charpin, D. Knowledge, opinions and attitudes of physicians regarding air pollution in the Bouches-du-Rhône. Rev. Mal. Respir. 1999, 16, 575. [Google Scholar] [PubMed]
- Glencross, D.A.; Ho, T.-R.; Camiña, N.; Hawrylowicz, C.M.; Pfeffer, P.E. Air pollution and its effects on the immune system. Free Radic. Biol. Med. 2020, 151, 56–68. [Google Scholar] [CrossRef] [PubMed]
- Steinemann, A. Volatile emissions from common consumer products. Air Qual. Atmos. Health 2015, 8, 273–281. [Google Scholar] [CrossRef]
- Nakhlé, M.M.; Farah, W.; Ziadé, N.; Abboud, M.; Salameh, D.; Annesi-Maesano, I. Short-term relationships between emergency hospital admissions for respiratory and cardiovascular diseases and fine particulate air pollution in Beirut, Lebanon. Environ. Monit. Assess. 2015, 187, 196. [Google Scholar] [CrossRef] [PubMed]
- Künzli, N.; Rapp, R.; Perez, L. “Breathe Clean Air”: The role of physicians and healthcare professionals. Breathe 2014, 10, 214–219. [Google Scholar] [CrossRef] [Green Version]
- Farah, W.; Nakhlé, M.M.; Abboud, M.; Annesi-Maesano, I.; Zaarour, R.; Saliba, N.; Germanos, G.; Gerard, J. Time series analysis of air pollutants in Beirut, Lebanon. Environ. Monit. Assess. 2014, 186, 8203–8213. [Google Scholar] [CrossRef]
- Xie, S.; Yu, T.; Zhang, Y.; Zeng, L.; Qi, L.; Tang, X. Characteristics of PM10, SO2, NO(x) and O3 in ambient air during the dust storm period in Beijing. Sci. Total Environ. 2005, 345, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Oh, J.Y.; Lee, Y.S.; Min, K.H.; Hur, G.Y.; Lee, S.Y.; Kang, K.H.; Shim, J.J. Harmful impact of air pollution on severe acute exacerbation of chronic obstructive pulmonary disease: Particulate matter is hazardous. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 1053–1059. [Google Scholar] [CrossRef] [Green Version]
- Destaillats, H.; Singer, B.; Salthammer, T. Does vaping affect indoor air quality? Indoor Air 2020, 30, 793–794. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.H.; Bernabé, K.; Moors, K.; Yan, B.; Chillrud, S.N.; Whyatt, R.; Camann, C.; Kinney, P.L.; Perera, F.P.; Miller, R.L. Effects of Floor Level and Building Type on Residential Levels of Outdoor and Indoor Polycyclic Aromatic Hydrocarbons, Black Carbon, and Particulate Matter in New York City. Atmosphere 2011, 2, 96–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Sharkawy, M.F.; Noweir, M.E.H. Indoor air quality levels in a University Hospital in the Eastern Province of Saudi Arabia. J. Fam. Community Med. 2014, 21, 39–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajagopalan, S.; Landrigan, P.J. Pollution and the Heart. N. Engl. J. Med. 2021, 385, 1881–1892. [Google Scholar] [CrossRef] [PubMed]
- Saeeditehrani, S.; Parsapour, A.; Nedjat, S.; Kadivar, M.; Larijani, B. Physicians’ attitude toward their ethical responsibility regarding air pollution: A qualitative research. J. Med. Ethics Hist. Med. 2017, 10, 7. [Google Scholar] [PubMed]
- Zielonka, T.M. Awareness of Polish physicians regarding the impact of air pollution on health. Arch. Environ. Occup. Health 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zielonka, T. The Awareness of Pulmonologists and Patients with Respiratory Diseases about the Impact of Air Pollution on Health in Poland. J. Clin. Med. 2021, 10, 2606. [Google Scholar] [CrossRef] [PubMed]
- Mirabelli, M.C.; Damon, S.A.; Beavers, S.F.; Sircar, K.D. Patient–Provider Discussions about Strategies to Limit Air Pollution Exposures. Am. J. Prev. Med. 2018, 55, e49–e52. [Google Scholar] [CrossRef] [PubMed]
- Tehrani, S.S.; Larijani, B.; Parsapour, A.; Rashidpouraie, R.; Madani, M. Evaluating physicians’ knowledge, attitude and practice of their ethical responsibilities towards the environmental problem and air pollution. J. Air Pollut. Health 2021, 6, 149–160. [Google Scholar]
- Manogaran, S.; Bahuguna, V.; Shukla, T.; Prabhakaran, P. Understanding Knowledge, Attitude and Practice of Health Practitioners towards Health Effects of Air Pollution in India; Centre for Environmental Health: Mumbai, India, 2020. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Frequency | Percent |
|---|---|---|
| Sex (n = 100) | 52 | 52 |
| ||
| Age (n = 112) | ||
| 27 | 24.1 |
| 27 | 24.1 |
| 21 | 18.8 |
| 37 | 33 |
| Years of practice (n = 112) | ||
| 20 | 17.9 |
| 20 | 17.9 |
| 14 | 12.5 |
| 13 | 11.6 |
| 14 | 12.5 |
| 31 | 27.7 |
| Specialty (n = 112) | ||
| 27 | 24.1 |
| 27 | 24.1 |
| 14 | 12.5 |
| 12 | 10.7 |
| 11 | 9.8 |
| 8 | 7.1 |
| 6 | 5.4 |
| 7 | 6.3 |
| Non-medical degree | 17 | 15.3 |
| (Master’s in public health, epidemiology, medical teaching, clinical nutrition) | ||
| Muhafaza (n = 109) | ||
| 61 | 56 |
| 25 | 22.9 |
| 10 | 9.2 |
| 9 | 8.3 |
| 4 | 3.7 |
| Living Condition | Strongly Agree | Agree | Neutral | Disagree | Strongly Disagree |
|---|---|---|---|---|---|
| Living near an open and well-ventilated road intersection | 24 (19.5) | 50 (40.7) | 25 (20.3) | 16 (13.0) | 8 (6.5) |
| Living near a gas station | 48 (39.3) | 48 (39.3) | 20 (16.4) | 6 (4.9) | 0 |
| Living near a diesel generator | 91 (73.4) | 20 (16.1) | 7 (5.6) | 3 (2.4) | 3 (2.4) |
| Living near car or bus parking | 64 (51.6) | 47 (37.9) | 9 (7.3) | 3 (2.4) | 1 (0.8) |
| Living near a construction site | 55 (45.1) | 43 (35.2) | 14 (11.5) | 6 (4.9) | 4 (3.3) |
| Living in a house with a garden | 14 (11.6) | 11 (9.1) | 6 (5.0) | 33 (27.3) | 57 (47.1) |
| Living near a garbage incinerator | 72 (60.0) | 26 (21.7) | 11 (9.2) | 4 (3.3) | 7 (5.8) |
| Staying indoors most of the time | 9 (7.3) | 20 (16.3) | 56 (45.5) | 25 (20.3) | 13 (10.6) |
| Living on higher-level floors (>third floor) | 6 (5.0) | 18 (14.9) | 54 (44.6) | 37 (30.6) | 6 (5.0) |
| Living near a busy traffic intersection | 65 (52.8) | 38 (30.9) | 9 (7.3) | 8 (6.5) | 3 (2.4) |
| Living near an open garbage dump | 73 (59.3) | 34 (27.6) | 8 (6.5) | 4 (3.3) | 4 (3.3) |
| Smoking electronic cigarettes (e-cigarette, IQOS) | 50 (41.7) | 32 (26.7) | 25 (20.8) | 8 (6.7) | 5 (4.2) |
| Smoking tobacco cigarettes | 85 (68.5) | 21 (16.9) | 11 (8.9) | 2 (1.6) | 5 (4.0) |
| Smoking arguileh (hookah) | 87 (70.7) | 20 (16.3) | 8 (6.5) | 2 (1.6) | 6 (4.9) |
| Living on the lower-level floors (<third floor) | 10 (8.3) | 44 (36.4) | 56 (46.3) | 10 (8.3) | 1 (0.8) |
| Living near the airport | 40 (32.5) | 49 (39.8) | 22 (17.9) | 6 (4.9) | 6 (4.9) |
| Living near an agricultural field | 6 (5.0) | 18 (14.9) | 39 (32.2) | 33 (27.3) | 25 (20.7) |
| Living with a person who smokes | 67 (54.0) | 37 (29.8) | 9 (7.3) | 7 (5.6) | 4 (3.2) |
| Work Condition | Strongly Agree | Agree | Neutral | Disagree | Strongly Disagree |
|---|---|---|---|---|---|
| Working at a gas station | 67 (54.9) | 38 (31.1) | 12 (9.8) | 2 (1.6) | 3 (2.5) |
| Working in a place where smoking is NOT allowed | 10 (8.1) | 11 (8.9) | 17 (13.8) | 27 (22.0) | 58 (47.2) |
| Working as a tour guide | 11 (9.0) | 19 (15.6) | 51 (41.8) | 28 (23.0) | 13 (10.7) |
| Working at a clinic | 8 (6.5) | 15 (12.2) | 38 (30.9) | 45 (36.6) | 17 (13.8) |
| Working in a hospital | 8 (6.5) | 20 (16.3) | 37 (30.1) | 47 (38.2) | 11 (8.9) |
| Working in an automobile repair shop | 40 (32.5) | 58 (47.2) | 16 (13.0) | 8 (6.5) | 1 (0.8) |
| Working at a gardening shop | 4 (3.3) | 18 (15.0) | 30 (25.0) | 41 (34.2) | 27 (22.5) |
| Working at a construction site | 51 (41.5) | 50 (40.7) | 15 (12.2) | 7 (5.7) | 0 |
| Working in a chemical lab | 42 (34.4) | 50 (41.0) | 18 (14.8) | 7 (5.7) | 5 (4.1) |
| Working with paints | 64 (51.6) | 42 (33.9) | 9 (7.3) | 5 (4.0) | 4 (3.2) |
| Working in a place where smoking is allowed | 70 (56.5) | 35 (28.2) | 9 (7.3) | 8 (6.5) | 2 (1.6) |
| Working as a teacher | 6 (4.9) | 21 (17.2) | 38 (31.1) | 34 (27.9) | 23 (18.9) |
| Working in a place where only vaping (e.g., IQOS) is allowed | 27 (23.3) | 44 (37.9) | 34 (29.3) | 8 (6.9) | 3 (2.6) |
| Working as a farmer | 5 (4.2) | 32 (26.9) | 31 (26.1) | 30 (25.2) | 21 (17.6) |
| Household Item | Strongly Agree | Agree | Neutral | Disagree | Strongly Disagree |
|---|---|---|---|---|---|
| Chimney | 52 (42.6) | 47 (38.5) | 17 (13.9) | 4 (3.3) | 2 (1.6) |
| Candles | 11 (9.1) | 46 (38.0) | 44 (36.4) | 15 (12.4) | 5 (4.1) |
| Wood heaters | 32 (26.4) | 56 (46.3) | 23 (19.0) | 10 (8.3) | 0 |
| Indoor smoking | 91 (74.0) | 22 (17.9) | 5 (4.1) | 2 (1.6) | 3 (2.4) |
| Detergents [Odex or Flash] | 56 (45.5) | 43 (35.0) | 14 (11.4) | 10 (8.1) | 0 |
| Watching television | 7 (5.9) | 15 (12.6) | 29 (24.4) | 29 (24.4) | 39 (32.8) |
| Air conditioning unit | 6 (5.0) | 34 (28.3) | 45 (37.5) | 28 (23.3) | 7 (5.8) |
| Vacuum cleaners | 9 (7.4) | 31 (25.6) | 47 (38.8) | 23 (19.0) | 11 (9.1) |
| Pets | 7 (5.7) | 31 (25.4) | 37 (30.3) | 29 (23.8) | 18 (14.8) |
| Indoor cooking | 4 (3.3) | 31 (25.4) | 42 (34.4) | 31 (25.4) | 14 (11.5) |
| Pesticides and insecticides | 69 (56.1) | 33 (26.8) | 12 (9.8) | 7 (5.7) | 2 (1.6) |
| Mold and fungi on the walls | 53 (43.1) | 37 (30.1) | 23 (18.7) | 9 (7.3) | 1 (0.8) |
| Air fresheners | 10 (8.4) | 42 (35.3) | 46 (38.7) | 17 (14.3) | 4 (3.4) |
| Glues/adhesives | 27 (22.1) | 43 (35.2) | 34 (27.9) | 12 (9.8) | 6 (4.9) |
| Taking a shower | 3 (2.5) | 14 (11.6) | 21 (17.4) | 35 (28.9) | 48 (39.7) |
| Open windows at home | 9 (7.4) | 15 (12.3) | 35 (28.7) | 29 (23.8) | 34 (27.9) |
| Lighting charcoal for arguileh at home | 71 (57.7) | 33 (26.8) | 12 (9.8) | 4 (3.3) | 3 (2.4) |
| Diesel heaters indoors | 73 (59.3) | 28 (22.8) | 10 (8.1) | 8 (6.5) | 4 (3.3) |
| Questionnaire Items | Demographic Characteristics | p-Value | |
|---|---|---|---|
| Muhafaza | |||
| Beirut | Outside Beirut | ||
| Cars | 58 (95.1%) | 39 (83.0%) | 0.039 |
| Incinerators | 57 (95.0%) | 37 (78.7%) | 0.011 |
| Household candles | 33 (54.1%) | 15 (31.9%) | 0.021 |
| Household wood heaters | 51 (83.6%) | 26 (56.5%) | 0.002 |
| Indoor diesel heaters | 54 (88.5%) | 34 (72.3%) | 0.032 |
| Risk of developing cancer | 58 (96.7%) | 39 (83.0%) | 0.016 |
| Sex | |||
| Male | Female | ||
| Living near a garbage incinerator | 36 (70.6%) | 40 (90.9%) | 0.014 |
| Smoking tobacco | 39 (75.0%) | 44 (93.6%) | 0.012 |
| Living with a person who smokes | 40 (76.9%) | 43 (91.5%) | 0.049 |
| Household detergents | 45 (86.7%) | 33 (70.2%) | 0.047 |
| Age | |||
| Under 40 years | 40 years and older | ||
| Living near a gas station | 37 (68.5%) | 49 (86.0%) | 0.028 |
| Confidence in counseling patients | 23 (42.6%) | 38 (65.5%) | 0.015 |
| Support of national assessment plan | 20 (37.0%) | 48 (82.8%) | 0.000 |
| Years of Practice | |||
| Under 10 years | 10 years and more | ||
| Confidence in counseling patients | 23 (42.6%) | 38 (65.5%) | 0.015 |
| Support of national assessment plan | 21 (38.9%) | 47 (81.0%) | 0.000 |
| Specialty | |||
| Internal medicine | Other specialties | ||
| Dust storms | 29 (64.4%) | 27 (42.9%) | 0.027 |
| Support of national assessment plan | 37 (80.4%) | 31 (47.0%) | 0.000 |
| Questionnaire Items on Knowledge | Questionnaire Items on Practices and Attitudes | p-Value | |
|---|---|---|---|
| Asking patients about their exposure to air pollution | |||
| Yes | No | ||
| Construction work | 82 (91.1%) | 19 (76.0%) | 0.041 |
| Diesel generators | 84 (92.3%) | 18 (72.0%) | 0.006 |
| Smoking, other than tobacco | 85 (94.4%) | 20 (80.0%) | 0.023 |
| Smoking arguileh (hookah) | 82 (91.1%) | 18 (72.0%) | 0.012 |
| Working with paint | 82 (90.1%) | 17 (68.0%) | 0.006 |
| Working where vaping is allowed | 61 (70.9%) | 6 (24.0%) | 0.000 |
| Pesticides and insecticides | 79 (86.8%) | 17 (68.0%) | 0.027 |
| Increases risk of CAD | 60 (65.9%) | 10 (40.0%) | 0.019 |
| Increases risk of severe illness | 73 (80.2%) | 14 (56.0%) | 0.013 |
| Importance of asking patients about air pollution exposure | |||
| Important | Not important | ||
| Incinerators | 85 (91.4%) | 14 (73.7%) | 0.028 |
| Smoking arguileh (hookah) | 84 (90.3%) | 14 (73.7%) | 0.046 |
| Role in reducing air pollution | |||
| Yes | No | ||
| Construction work | 96 (89.7%) | 3 (60.0%) | 0.043 |
| Living on lower-level floors | 47 (44.3%) | 0 (0.0%) | 0.050 |
| Living near an airport | 81 (75.7%) | 1 (20.0%) | 0.006 |
| Confidence in counseling patients on air pollution | |||
| Yes | No | ||
| Living near a traffic intersection | 49 (77.8%) | 46 (92.0%) | 0.040 |
| Increases risk of cancer | 53 (85.5%) | 50 (98.0%) | 0.019 |
| Increases risk of asthma | 53 (84.1%) | 49 (96.1%) | 0.039 |
| Interest in attending continuing education about air pollution | |||
| Yes | No | ||
| Living near a gas station | 68 (84.0%) | 20 (62.5%) | 0.013 |
| Living on lower-level floors | 39 (48.8%) | 9 (28.1%) | 0.046 |
| Living near an airport | 65 (80.2%) | 17 (53.1%) | 0.004 |
| Working at a gas station | 73 (91.3%) | 23 (71.9%) | 0.008 |
| Support of national air pollution assessment plan | |||
| Yes | No | ||
| Dust storms | 41 (60.3%) | 16 (37.2%) | 0.018 |
| Living near diesel generator | 66 (94.3%) | 36 (81.8%) | 0.035 |
| Living near garbage incinerator | 60 (89.6%) | 30 (69.8%) | 0.009 |
| Smoking tobacco | 65 (91.4%) | 33 (75.0%) | 0.017 |
| Living near an airport | 57 (81.4%) | 26 (59.1%) | 0.009 |
| Working where smoking is allowed | 63 (90.0%) | 33 (75.0%) | 0.033 |
| Household mold and fungi on walls | 55 (78.6%) | 27 (61.4%) | 0.047 |
| Increases the risk of allergies | 63 (90.0%) | 33 (75.0%) | 0.033 |
| Increases the risk of severe illness | 58 (82.9%) | 27 (61.4%) | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assi, H.I.; Meouchy, P.; El Mahmoud, A.; Massouh, A.; Bou Zerdan, M.; Alameh, I.; Chamseddine, N.; Kazarian, H.; Zeineldine, S.; Saliba, N.A.; et al. A Survey on the Knowledge, Attitudes, and Practices of Lebanese Physicians Regarding Air Pollution. Int. J. Environ. Res. Public Health 2022, 19, 7907. https://doi.org/10.3390/ijerph19137907
Assi HI, Meouchy P, El Mahmoud A, Massouh A, Bou Zerdan M, Alameh I, Chamseddine N, Kazarian H, Zeineldine S, Saliba NA, et al. A Survey on the Knowledge, Attitudes, and Practices of Lebanese Physicians Regarding Air Pollution. International Journal of Environmental Research and Public Health. 2022; 19(13):7907. https://doi.org/10.3390/ijerph19137907
Chicago/Turabian StyleAssi, Hazem I., Paul Meouchy, Ahmad El Mahmoud, Angela Massouh, Maroun Bou Zerdan, Ibrahim Alameh, Nathalie Chamseddine, Houry Kazarian, Salah Zeineldine, Najat A. Saliba, and et al. 2022. "A Survey on the Knowledge, Attitudes, and Practices of Lebanese Physicians Regarding Air Pollution" International Journal of Environmental Research and Public Health 19, no. 13: 7907. https://doi.org/10.3390/ijerph19137907