
The Effectiveness of Planning Interventions for Improving Physical Activity in the General Population: A Systematic Review and Meta-Analysis of Randomized Controlled Trials



Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.2.1. Population
2.2.2. Interventions
2.2.3. Comparators
2.2.4. Outcomes
2.2.5. Study Design
2.3. Data Abstraction and Risk of Bias Assessment
2.4. Statistical Analyses
3. Results
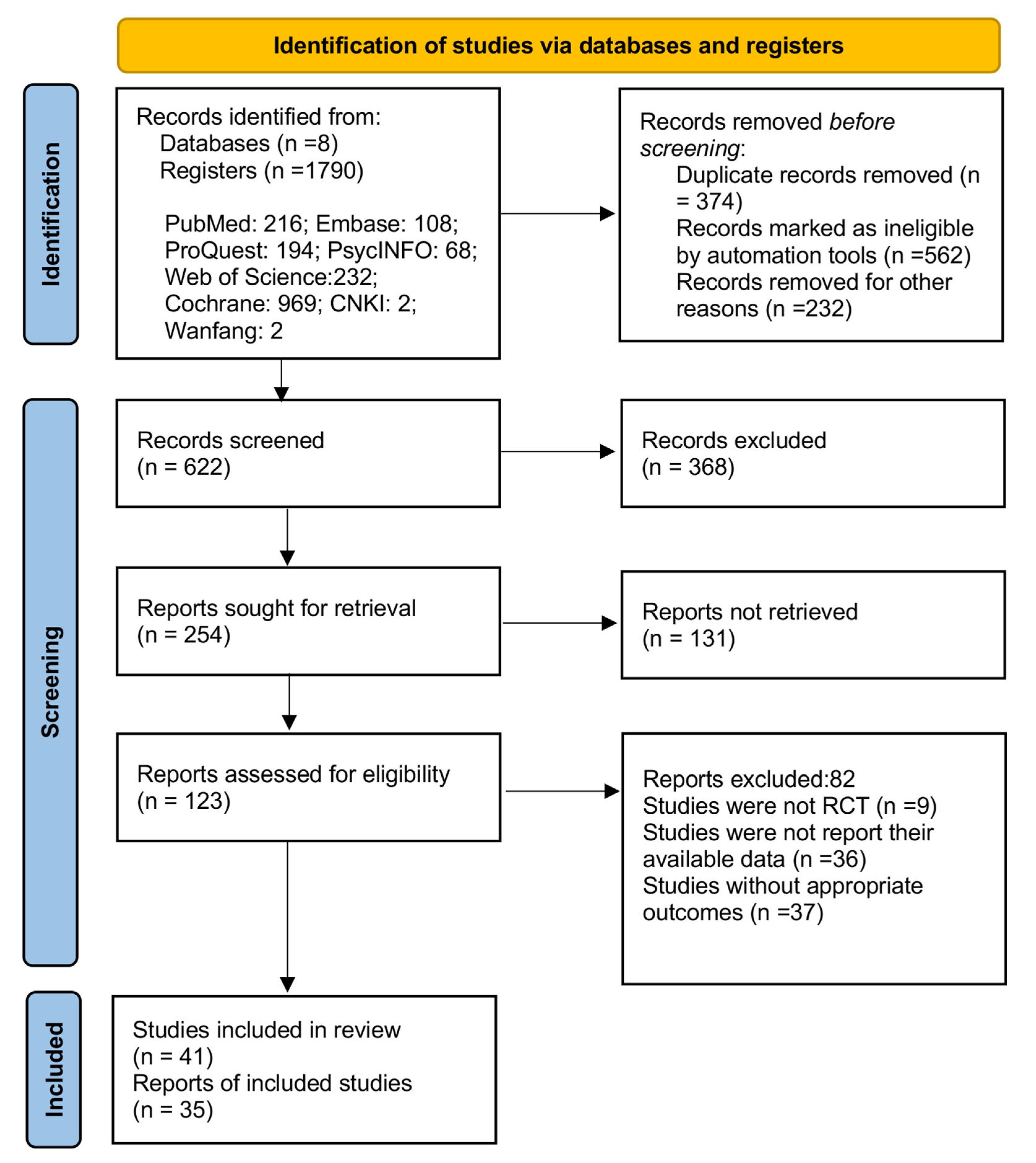
3.1. Literature Selection
3.2. Characteristics of Studies
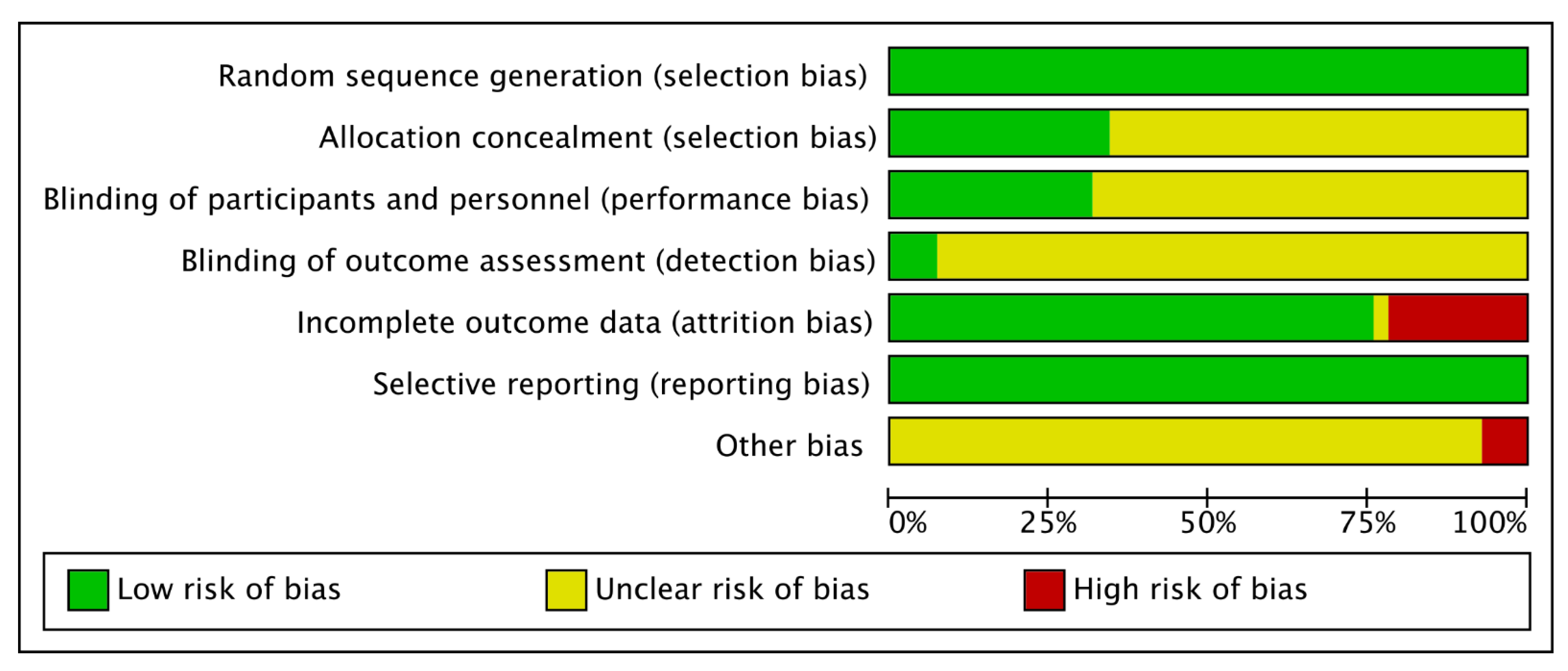
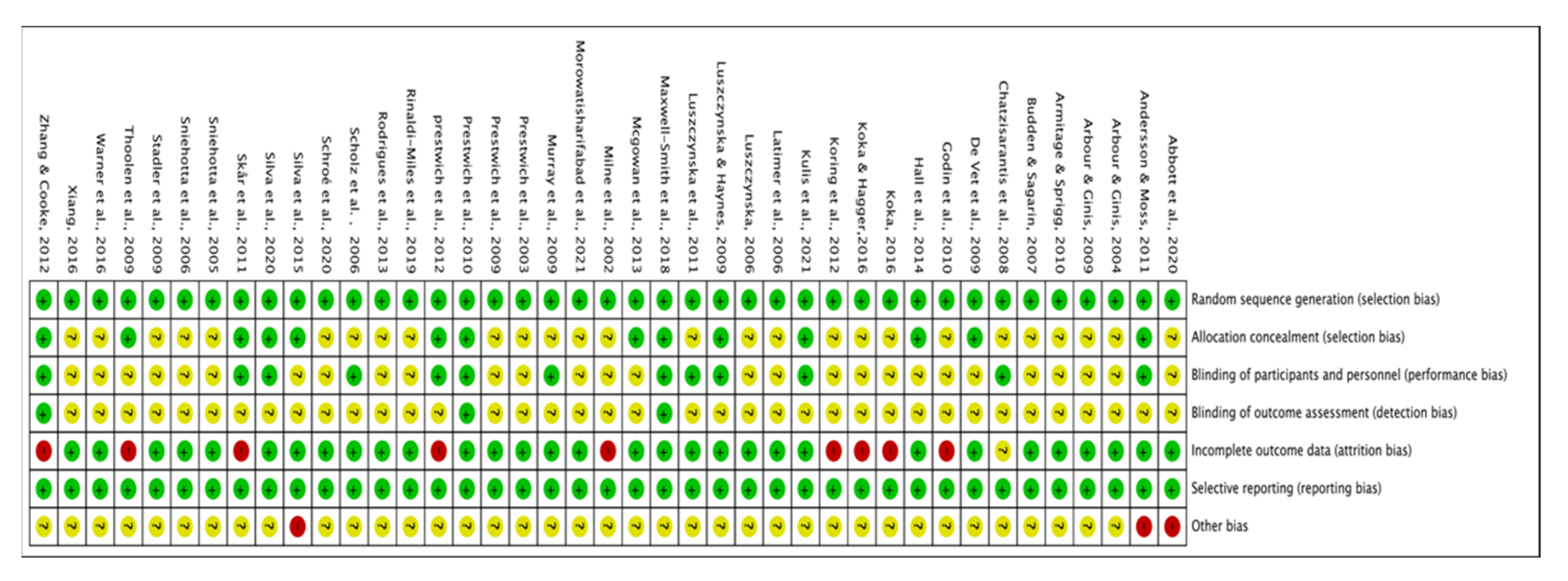
3.3. Quality of Included Studies
3.4. Primary Outcome
3.5. Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haseler, T.; Haseler, C. Lack of physical activity is a global problem. BMJ 2022, 376, o348. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World: At-a-Glance; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Lee, S.; Lee, C.; An, J. Psycho-social correlates of leisure-time physical activity (LTPA) among older adults: A multivariate analysis. Eur. Rev. Aging Phys. Act. 2020, 17, 6. [Google Scholar] [CrossRef] [PubMed]
- Elsawy, B.; Higgins, K.E. Physical activity guidelines for older adults. Am. Fam. Physician 2010, 81, 55–59. [Google Scholar]
- Lim, C.; Donovan, A.M.; Harper, N.J.; Naylor, P.-J. Nature Elements and Fundamental Motor Skill Development Opportunities at Five Elementary School Districts in British Columbia. Int. J. Environ. Res. Public Health 2017, 14, 1279. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, J.; Rhodes, R.; Bredin, S.S.D.; Oh, P.; Warburton, D.E.R. Effectiveness of approaches to increase physical activity behavior to prevent chronic disease in adults: A brief commentary. J. Clin. Med. 2019, 8, 295. [Google Scholar] [CrossRef] [Green Version]
- Swann, C.; Rosenbaum, S.; Lawrence, A.; Vella, S.A.; McEwan, D.; Ekkekakis, P. Updating goal-setting theory in physical activity promotion: A critical conceptual review. Health Psychol. Rev. 2021, 15, 34–50. [Google Scholar] [CrossRef] [Green Version]
- Pears, S.; Sutton, S. Effectiveness of acceptance and commitment therapy (ACT) interventions for promoting physical activity: A systematic review and meta-analysis. Health Psychol. Rev. 2021, 15, 159–184. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Janssen, I.; Bredin, S.S.D.; Warburton, D.E.R.; Bauman, A. Physical activity: Health impact, prevalence, correlates and interventions. Psychol. Health 2017, 32, 942–975. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155. [Google Scholar] [CrossRef]
- Whatnall, M.C.; Sharkey, T.; Hutchesson, M.J.; Haslam, R.L.; Bezzina, A.; Collins, C.E.; Ashton, L.M. Effectiveness of interventions and behaviour change techniques for improving physical activity in young adults: A systematic review and meta-analysis. J. Sports Sci. 2021, 39, 1754–1771. [Google Scholar] [CrossRef] [PubMed]
- Direito, A.; Carraça, E.; Rawstorn, J.; Whittaker, R.; Maddison, R. mHealth technologies to influence physical activity and sedentary behaviors: Behavior change techniques, systematic review and meta-analysis of randomized controlled trials. Ann. Behav. Med. 2017, 51, 226–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuckey, M.I.; Carter, S.W.; Knight, E. The role of smartphones in encouraging physical activity in adults. Int. J. Gen. Med. 2017, 10, 293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howlett, N.; Trivedi, D.; Troop, N.A.; Chater, A.M. Are physical activity interventions for healthy inactive adults effective in promoting behavior change and maintenance, and which behavior change techniques are effective? A systematic review and meta-analysis. Transl. Behav. Med. 2019, 9, 147–157. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Processes 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Rhodes, R.E.; de Bruijn, G.J. How big is the physical activity intention–behaviour gap? A meta-analysis using the action control framework. Br. J. Health Psychol. 2013, 18, 296–309. [Google Scholar] [CrossRef] [Green Version]
- Heckhausen, H.; Gollwitzer, P.M. Thought contents and cognitive functioning in motivational versus volitional states of mind. Motiv. Emot. 1987, 11, 101–120. [Google Scholar] [CrossRef]
- Leventhal, H.; Leventhal, E.A.; Contrada, R.J. Self-regulation, health, and behavior: A perceptual-cognitive approach. Psychol. Health 1998, 13, 717–733. [Google Scholar] [CrossRef]
- Gollwitzer, P.M. Implementation intentions: Strong effects of simple plans. Am. Psychol. 1999, 54, 493–503. [Google Scholar] [CrossRef]
- Carraro, N.; Gaudreau, P. Predicting physical activity outcomes during episodes of academic goal conflict: The differential role of action planning and coping planning. Personal. Soc. Psychol. Bull. 2015, 41, 1291–1305. [Google Scholar] [CrossRef]
- Belanger-Gravel, A.; Godin, G.; Amireault, S. A meta-analytic review of the effect of implementation intentions on physical activity. Health Psychol. Rev. 2013, 7, 23–54. [Google Scholar] [CrossRef]
- Carraro, N.; Gaudreau, P. Spontaneous and experimentally induced action planning and coping planning for physical activity: A meta-analysis. Psychol. Sport Exerc. 2013, 14, 228–248. [Google Scholar] [CrossRef]
- Da Silva, M.A.V.; São-João, T.M.; Brizon, V.C.; Franco, D.H.; Mialhe, F.L. Impact of implementation intentions on physical activity practice in adults: A systematic review and meta-analysis of randomized clinical trials. PLoS ONE 2018, 13, e0206294. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Chapter 8: Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Collaboration: London, UK, 2013. [Google Scholar]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Juni, P.; Bartlett, C.; Holenstein, F.; Sterne, J. How important are comprehensive literature searches and the assessment of trial quality in systematic reviews? Empirical study. Health Technol. Assess. 2003, 7, 1–76. [Google Scholar] [CrossRef]
- Milne, S.; Orbell, S.; Sheeran, P. Combining motivational and volitional interventions to promote exercise participation: Protection motivation theory and implementation intentions. Br. J. Health Psychol. 2002, 7, 163–184. [Google Scholar] [CrossRef]
- Prestwich, A.; Lawton, R.; Conner, M. The use of implementation intentions and the decision balance sheet in promoting exercise behaviour. Psychol. Health 2003, 18, 707–721. [Google Scholar] [CrossRef] [Green Version]
- Arbour, K.P.; Ginis, K.A.M. Helping middle-aged women translate physical activity intentions into action: Combining the theory of planned behavior and implementation intentions. J. Appl. Biobehav. Res. 2004, 9, 172–187. [Google Scholar] [CrossRef]
- Sniehotta, F.F.; Scholz, U.; Schwarzer, R.; Fuhrmann, B.; Kiwus, U.; Völler, H. Long-term effects of two psychological interventions on physical exercise and self-regulation following coronary rehabilitation. Int. J. Behav. Med. 2005, 12, 244–255. [Google Scholar] [CrossRef] [Green Version]
- Latimer, A.E.; Ginis, K.A.M.; Arbour, K.P. The efficacy of an implementation intention intervention for promoting physical activity among individuals with spinal cord injury: A randomized controlled trial. Rehabil. Psychol. 2006, 51, 273–280. [Google Scholar] [CrossRef]
- Luszczynska, A. An implementation intentions intervention, the use of a planning strategy, and physical activity after myocardial infarction. Soc. Sci. Med. 2006, 62, 900–908. [Google Scholar] [CrossRef] [PubMed]
- Scholz, U.; Knoll, N.; Sniehotta, F.F.; Schwarzer, R. Physical activity and depressive symptoms in cardiac rehabilitation: Long-term effects of a self-management intervention. Soc. Sci. Med. 2006, 62, 3109–3120. [Google Scholar] [CrossRef] [PubMed]
- Sniehotta, F.F.; Scholz, U.; Schwarzer, R. Action plans and coping plans for physical exercise: A longitudinal intervention study in cardiac rehabilitation. Br. J. Health Psychol. 2006, 11, 23–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budden, J.S.; Sagarin, B.J. Implementation intentions, occupational stress, and the exercise intention-behavior relationship. J. Occup. Health Psychol. 2007, 12, 391–401. [Google Scholar] [CrossRef]
- Chatzisarantis, N.L.; Hagger, M.S.; Thøgersen-Ntoumani, C. The Effects of Self-Discordance, Self-Concordance, and Implementation Intentions on Health Behavior. J. Appl. Biobehav. Res. 2008, 13, 198–214. [Google Scholar] [CrossRef]
- Arbour, K.P.; Martin Ginis, K.A. A randomised controlled trial of the effects of implementation intentions on women’s walking behaviour. Psychol. Health 2009, 24, 49–65. [Google Scholar] [CrossRef]
- De Vet, E.; Oenema, A.; Sheeran, P.; Brug, J. Should implementation intentions interventions be implemented in obesity prevention: The impact of if-then plans on daily physical activity in Dutch adults. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 11. [Google Scholar] [CrossRef] [Green Version]
- Luszczynska, A.; Haynes, C. Changing nutrition, physical activity and body weight among student nurses and midwives: Effects of a planning intervention and self-efficacy beliefs. J. Health Psychol. 2009, 14, 1075–1084. [Google Scholar] [CrossRef]
- Murray, T.C.; Rodgers, W.M.; Fraser, S.N. Examining implementation intentions in an exercise intervention: The effects on adherence and self-efficacy in a naturalistic setting 1. J. Appl. Soc. Psychol. 2009, 39, 2303–2320. [Google Scholar] [CrossRef]
- Prestwich, A.; Perugini, M.; Hurling, R. Can the effects of implementation intentions on exercise be enhanced using text messages? Psychol. Health 2009, 24, 677–687. [Google Scholar] [CrossRef]
- Stadler, G.; Oettingen, G.; Gollwitzer, P.M. Physical activity in women: Effects of a self-regulation intervention. Am. J. Prev. Med. 2009, 36, 29–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thoolen, B.J.; Ridder, D.d.; Bensing, J.; Gorter, K.; Rutten, G. Beyond good intentions: The role of proactive coping in achieving sustained behavioural change in the context of diabetes management. Psychol. Health 2009, 24, 237–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armitage, C.J.; Sprigg, C.A. The roles of behavioral and implementation intentions in changing physical activity in young children with low socioeconomic status. J. Sport Exerc. Psychol. 2010, 32, 359–376. [Google Scholar] [CrossRef] [PubMed]
- Godin, G.; Belanger-Gravel, A.; Amireault, S.; Gallani, M.-C.B.J.; Vohl, M.-C.; Perusse, L. Effect of Implementation Intentions to Change Behaviour: Moderation by Intention Stability. Psychol. Rep. 2010, 106, 147–159. [Google Scholar] [CrossRef]
- Prestwich, A.; Perugini, M.; Hurling, R. Can implementation intentions and text messages promote brisk walking? A randomized trial. Health Psychol. 2010, 29, 40–49. [Google Scholar] [CrossRef] [Green Version]
- Andersson, E.K.; Moss, T.P. Imagery and implementation intention: A randomised controlled trial of interventions to increase exercise behaviour in the general population. Psychol. Sport Exerc. 2011, 12, 63–70. [Google Scholar] [CrossRef]
- Luszczynska, A.; Schwarzer, R.; Lippke, S.; Mazurkiewicz, M. Self-efficacy as a moderator of the planning-behaviour relationship in interventions designed to promote physical activity. Psychol. Health 2011, 26, 151–166. [Google Scholar] [CrossRef]
- Skår, S.; Sniehotta, F.F.; Molloy, G.J.; Prestwich, A.; Araújo-Soares, V. Do brief online planning interventions increase physical activity amongst university students? A randomised controlled trial. Psychol. Health 2011, 26, 399–417. [Google Scholar] [CrossRef]
- Koring, M.; Richert, J.; Parschau, L.; Ernsting, A.; Lippke, S.; Schwarzer, R. A combined planning and self-efficacy intervention to promote physical activity: A multiple mediation analysis. Psychol. Health Med. 2012, 17, 488–498. [Google Scholar] [CrossRef]
- Prestwich, A.; Conner, M.T.; Lawton, R.J.; Ward, J.K.; Ayres, K.; McEachan, R.R.C. Randomized Controlled Trial of Collaborative Implementation Intentions Targeting Working Adults’ Physical Activity. Health Psychol. 2012, 31, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Cooke, R. Using a combined motivational and volitional intervention to promote exercise and healthy dietary behaviour among undergraduates. Diabetes Res. Clin. Pract. 2012, 95, 215–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGowan, E.L.; North, S.; Courneya, K.S. Randomized controlled trial of a behavior change intervention to increase physical activity and quality of life in prostate cancer survivors. Ann. Behav. Med. 2013, 46, 382–393. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, R.C.; João, T.M.; Gallani, M.C.; Cornélio, M.E.; Alexandre, N.M. The “Moving Heart Program”: An intervention to improve physical activity among patients with coronary heart disease. Rev. Latino-Am. Enferm. 2013, 21, 180–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, P.A.; Zehr, C.; Paulitzki, J.; Rhodes, R. Implementation intentions for physical activity behavior in older adult women: An examination of executive function as a moderator of treatment effects. Ann. Behav. Med. 2014, 48, 130–136. [Google Scholar] [CrossRef]
- Da Silva, M.A.; Gouvêa, G.R.; Claro, A.F.; Agondi Rde, F.; Cortellazzi, K.L.; Pereira, A.C.; Meneghim Mde, C.; Mialhe, F.L. Impact of the activation of intention to perform physical activity in type II diabetics: A randomized clinical trial. Cien. Saude Colet. 2015, 20, 875–886. [Google Scholar] [CrossRef] [Green Version]
- Koka, A. An intervention crossing two types of action planning with mental simulation for the promotion of physical activity among adolescents. Int. J. Adolesc. Med. Health 2016, 29. [Google Scholar] [CrossRef]
- Warner, L.M.; Wolff, J.K.; Ziegelmann, J.P.; Schwarzer, R.; Wurm, S. Revisiting self-regulatory techniques to promote physical activity in older adults: Null-findings from a randomised controlled trial. Psychol. Health 2016, 31, 1145–1165. [Google Scholar] [CrossRef]
- Xiang, M.Q. The Promotion Strategies of Pupils’ Exercise Intention and Behavior:the Action Planning Intervention Based on TPB. J. Nanjing Sport Inst. 2016, 15, 14–20. [Google Scholar] [CrossRef]
- Koka, A.; Hagger, M.S. A brief intervention to increase physical activity behavior among adolescents using mental simulations and action planning. Psychol. Health Med. 2017, 22, 701–710. [Google Scholar] [CrossRef] [Green Version]
- Maxwell-Smith, C.; Hince, D.; Cohen, P.A.; Bulsara, M.K.; Boyle, T.; Platell, C.; Tan, P.; Levitt, M.; Salama, P.; Tan, J.; et al. A randomized controlled trial of WATAAP to promote physical activity in colorectal and endometrial cancer survivors. Psychooncology 2019, 28, 1420–1429. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi-Miles, A.; Das, B.M.; Kakar, R.S. Evaluating the effectiveness of implementation intentions in a pedometer worksite intervention. Work 2019, 64, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Abbott, S.; de Wit, J.; Rawstorne, P.; Reynolds, R. Mental contrasting and implementation intentions to increase physical activity in sedentary, disadvantaged adults: A pilot intervention. Sport Exerc. Perform. Psychol. 2020, 9, 261–275. [Google Scholar] [CrossRef]
- Schroé, H.; Van Dyck, D.; De Paepe, A.; Poppe, L.; Loh, W.W.; Verloigne, M.; Loeys, T.; De Bourdeaudhuij, I.; Crombez, G. Which behaviour change techniques are effective to promote physical activity and reduce sedentary behaviour in adults: A factorial randomized trial of an e- and m-health intervention. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 127. [Google Scholar] [CrossRef]
- Vieira da Silva, M.A.; Sao-Joao, T.M.; Cornelio, M.E.; Mialhe, F.L. Effect of implementation intention on walking in people with diabetes: An experimental approach. Rev. Saude Publica 2020, 54, 103. [Google Scholar] [CrossRef]
- Kulis, E.; Szczuka, Z.; Keller, J.; Banik, A.; Boberska, M.; Kruk, M.; Knoll, N.; Radtke, T.; Scholz, U.; Rhodes, R.E.; et al. Collaborative, dyadic, and individual planning and physical activity: A dyadic randomized controlled trial. Health Psychol. 2022, 41, 134–144. [Google Scholar] [CrossRef]
- Morowatisharifabad, M.A.; Asadpour, M.; Zakeri, M.A.; Abdolkarimi, M. The Effect of Integrated Intervention Based on Protection Motivation Theory and Implementation Intention to Promote Physical Activity and Physiological Indicators of Patients with Type 2 Diabetes. BioMed Res. Int. 2021, 2021, 6637656. [Google Scholar] [CrossRef]
- Hagger, M.S.; Luszczynska, A. Implementation intention and action planning interventions in health contexts: State of the research and proposals for the way forward. Appl. Psychol. Health Well Being 2014, 6, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Schwarzer, R. Modeling health behavior change: How to predict and modify the adoption and maintenance of health behaviors. Appl. Psychol. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Schwarzer, R. Health Action Process Approach (HAPA) as a Theoretical Framework to Understand Behavior Change. Actual. Psicol. 2016, 30, 119–130. [Google Scholar] [CrossRef]
- Scholz, U.; Sniehotta, F.F.; Burkert, S.; Schwarzer, R. Increasing physical exercise levels: Age-specific benefits of planning. J. Aging Health 2007, 19, 851–866. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.Q.; Zhang, R.; Schwarzer, R.; Hagger, M.S. A meta-analysis of the health action process approach. Health Psychol. 2019, 38, 623–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleig, L.; Pomp, S.; Parschau, L.; Barz, M.; Lange, D.; Schwarzer, R.; Lippke, S. From intentions via planning and behavior to physical exercise habits. Psychol. Sport Exerc. 2013, 14, 632–639. [Google Scholar] [CrossRef]
- Schwarzer, R.; Warner, L.; Fleig, L.; Gholami, M.; Salvatore, S.; Cianferotti, L.; Ntzani, E.; Roman-Viñas, B.; Trichopoulou, A.; Brandi, M.L. Psychological mechanisms in a digital intervention to improve physical activity: A multicentre randomized controlled trial. Br. J. Health Psychol. 2018, 23, 296–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sniehotta, F.F.; Scholz, U.; Schwarzer, R. Bridging the intention-behaviour gap: Planning, self-efficacy, and action control in the adoption and maintenance of physical exercise. Psychol. Health 2005, 20, 143–160. [Google Scholar] [CrossRef]
- Norman, P.; Conner, M. The theory of planned behavior and exercise: Evidence for the mediating and moderating roles of planning on intention-behavior relationships. J. Sport Exerc. Psychol. 2005, 27, 488–504. [Google Scholar] [CrossRef]
- Hamilton, K.; Schwarzer, R. Making plans to facilitate young children’s physical activity: The role of psycho-social mediators and moderators. J. Child Fam. Stud. 2017, 2. [Google Scholar]
- Schwarzer, R.; Lippke, S.; Luszczynska, A. Mechanisms of health behavior change in persons with chronic illness or disability: The Health Action Process Approach (HAPA). Rehabil. Psychol. 2011, 56, 161. [Google Scholar] [CrossRef]
- Sutton, S. How does the health action process approach (HAPA) bridge the intention–behavior gap? An examination of the model’s causal structure. Appl. Psychol. 2008, 57, 66–74. [Google Scholar] [CrossRef]
- Moyers, S.A.; Hagger, M.S. Planning and implementation intention interventions in physical activity. In Motivation and Self-Regulation in Sport and Exercise; Routledge: New York, NY, USA, 2021; pp. 166–183. ISBN 978-1-003-17669-5. [Google Scholar]
- Kettle, V.E.; Madigan, C.D.; Coombe, A.; Graham, H.; Thomas, J.J.C.; Chalkley, A.E.; Daley, A.J. Effectiveness of physical activity interventions delivered or prompted by health professionals in primary care settings: Systematic review and meta-analysis of randomised controlled trials. BMJ 2022, 376, e068465. [Google Scholar] [CrossRef]
- Romain, A.J.; Bortolon, C.; Gourlan, M.; Carayol, M.; Decker, E.; Lareyre, O.; Ninot, G.; Boiché, J.; Bernard, P. Matched or nonmatched interventions based on the transtheoretical model to promote physical activity. A meta-analysis of randomized controlled trials. J. Sport Health Sci. 2018, 7, 50–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conner, M.; Sandberg, T.; Norman, P. Using action planning to promote exercise behavior. Ann. Behav. Med. 2010, 40, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Godin, G.; Shephard, R. A simple method to assess exercise behavior in the community. Can. J. Appl. Sport Sci. 1985, 10, 141–146. [Google Scholar] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troiano, R.P.; McClain, J.J.; Brychta, R.J.; Chen, K.Y. Evolution of accelerometer methods for physical activity research. Br. J. Sports Med. 2014, 48, 1019–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borenstein, M.; Cooper, H.; Hedges, L.; Valentine, J. Effect sizes for continuous data. Handb. Res. Synth. Meta-Anal. 2009, 2, 221–235. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Publication | Sample Size | Female (%) | Age | Country | Participant | Intervention Strategy | Delivery Mode | Duration | Reinforcement | Instrument | Outcome | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IG | CG | IG | CG | ||||||||||
| Kulis et al., 2021 | 82 | 76 | 64.40 | 43.86 ± 17.02 | Poland | Inactive adults | AP + CP | Session and online | 36 W | 3 sessions + 4 Phone | Accelerometer | No. MVPA min/day | |
| Schroé et al., 2020 | 38 | 46 | 72.80 | 35.66 ± 15.83 | 33.33 ± 16.93 | Dutch | General adults | AP + CP | Session and online | 5 W | every week by email | IPAQ | No. MVPA min/week |
| Maxwell-Smith et al., 2018 | 34 | 34 | 50.00 | 65.26 ± 7.41 | 62.88 ± 8.37 | Australia | Cardiovascular risk survivors | AP + CP | Session and online | 12 W | 3 phones | Accelerometer | No. MVPA min/week |
| Abbott et al., 2020 | 14 | 13 | 63.33 | 37.7 ± 13.4 | 48.90 ± 14.50 | Australia | Inactive adults | AP | Session and online | 12 W | weekly via online | IPAQ | No. MVPA min/week |
| Koka, 2016 | 54 | 64 | 50.63 | 14.79 ± 0.71 | Estonia | Adolescents | AP | Session | 1 M | No | Items (not validated) | No. times of LTPA > 30 min/week | |
| Milne et al., 2002 | 79 | 93 | 73.00 | 20.04 ± 2.23 | UK | Undergraduate students | AP | Session | 2 W | No | Items (not validated) | No. times MVPA > 20 min/week | |
| Arbour and Ginis, 2004 | 24 | 19 | 100 | 45.38 ± 7.55 | 47.78 ± 7.03 | Canada | Sedentary adults | AP | Session | 8 W | No | Diary (not validate) | No. times PA at the recommended level/week |
| Latimer et al., 2006 | 19 | 18 | 43.24 | 40.89 ± 11.56 | 40.94 ± 10.85 | North America | Spinal Cord Injury patients | AP | Session | 8 W | 2 emails | PARA–SCI | Physical activity duration (min/day) |
| Luszczynska, 2006 | 59 | 55 | 36.00 | 54:25 ± 6.85 | Poland | Myocardial infarction patients | AP | Session | 8 W | No | Item (not validated) | Scores expressing frequency | |
| Prestwich et al., 2009 | 29 | 34 | 58.06 | 23.76 ± 4.64 | UK | Inactive undergraduate students | AP | Session and online | 4 W | phone | Item (not validated) | No. times of MVPA > 30 min/week | |
| Stadler et al., 2009 | 133 | 133 | 100 | 41.33 ± 5.91 | 41.22 ± 6.48 | Germany | General adults | AP + CP | Session | 16 W | 4 sessions | BTDPAR | No. MVPA min/week |
| Armitage and Sprigg, 2010 | 39 | 38 | 49.35 | 8.06 ± 1.63 | UK | Children | AP | Session | 6 W | 2 sessions | Items (validated) | Scores expressing frequency | |
| Prestwich et al., 2010 | 40 | 46 | 63.76 | 22.19 ± 5.01 | 23.62 ± 4.49 | UK | Inactive adults | AP | Session and online | 4 W | 3 text messages by mobile phone | Items (validated) | No. days exercised for 30 min/week |
| Andersson and Moss, 2011 | 13 | 14 | 78.03 | 27.00 ± 6.80 | 26.20 ± 6.70 | UK | Inactive adults | AP | Online | 2 W | No | LTEQ | MVPA Occasions/week |
| Luszczynska et al., 2011 | 36 | 22 | 56.90 | 48.17 ± 17.89 | Poland | Diabetes patients | AP | Session | 4 W | No | One Item | Scores expressing frequency | |
| Koring et al., 2012 | 445 | 438 | 67.95 | 42.92 ± 14.91 | 43.86 ± 13.66 | Germany | General adults | AP + CP | Online | 3 W | No | IPAQ | MVPA min/week |
| Zhang and Cooke, 2012 | 22 | 21 | 48.81 | 20.56 ± 1.62 | UK | Undergraduate students | AP + CP | Online | 4 W | No | Items (not validated) | No. times MVPA > 20 min/week | |
| Mcgowan et al., 2013 | 141 | 141 | 0 | 68.40 | 67.90 | Canada | Prostate cancer survivors | AP + CP | Session | 1 M | No | The index of LTEQ | No. MVPA min/week |
| Rodrigues et al., 2013 | 69 | 67 | 36.00 | 56.70 ± 9.10 | Brazil | Coronary heart disease patients | AP + CP | Session and online | 2 M | 4 telephones | Baecke-HPA | No. times walked at least 30 min last month | |
| Hall et al., 2014 | 24 | 28 | 100 | 73.30 ± 7.17 | 73.11 ± 6.66 | Canada | Older Adult Women | AP + CP | Session and online | 4 W | 4 telephones | Stanford 7-day Recall | No. times of half-hour VPA/week |
| Silva et al., 2015 | 15 | 15 | 66.67 | 61.27 ± 6.26 | 59.87 ± 12.61 | Brazil | Type II diabetics patients | AP + CP | Session and online | 2 M | Telephone | IPAQ | No. MVPA min/week |
| Sniehotta et al., 2005 | 65 | 79 | 18.50 | 57.70 ± 10.30 | Germany | Cardiac rehabilitation patients | AP + CP | Session and online | 4 M | Diary | Adapted version of KPAS | No. general exercise min/week | |
| Sniehotta et al., 2006 | 62 | 81 | 22.00 | 59.30 ± 10.00 | Germany | Cardiac rehabilitation patients | AP + CP | Session | 2 M | No | Items (not validated) | No. all activity min/week | |
| Murray et al., 2009 | 29 | 23 | 100 | 30.50 ± 9.80 | Canada | General adults | AP | Session | 11 W | 3 times repetition | checklist at the gym (not validated) | No. sessions/week | |
| Thoolen et al., 2009 | 119 | 108 | 40.00 | 62.00 ± 4.90 | 61.90 ± 5.60 | Dutch | Diabetes patients | AP + CP | Session | 12 M | 4 sessions | PASE | Scores expressing amount |
| Prestwich et al., 2003 | 18 | 18 | 51.20 | 21.31 ± 4.39 | UK | General adults | AP | Session | 4 W | No | Items not validated | No. sessions/week | |
| Xiang, 2016 | 31 | 32 | 46.03 | 10. 25 ±0. 43 | China | Elementary school students | AP | Session | 1 M | Physical education course | Physical Activity Questionnaire for Children | Scores expressing frequency | |
| Godin et al., 2010 | 108 | 113 | 61.60 | 38.20 ± 10.20 | 37.10 ± 11.00 | Canada | General adults | AP | Online | 6 M | No | Items (not validated) | Scores expressing frequency |
| Scholz et al., 2006 | 103 | 95 | 17.70 | 58.50 ± 10.60 | Germany | Cardiac rehabilitation patients | AP + CP | Session and online | 12 W | Diary | Adapted version of the IPAQ | No. MVPA min/week | |
| Luszczynska and Haynes, 2009 | 104 | 78 | 89.00 | 28.73 ± 9.51 | UK | General adults | AP + CP | Session | 4 M | Repeat 3 times | Items (not validated) | Score expressing frequency | |
| Skår et al., 2011 | 335 | 315 | 63.40 | 22.80 ± 6.70 | UK | University students | AP + CP | Online | 6 W | No | Items (validated) | Scores expressing frequency | |
| De Vet et al., 2009 | 172 | 206 | 67.00 | 45.90 ± 10.34 | Dutch | General adults | AP | Session | 6 M | No | SQUASH | No. all activity min/week | |
| Chatzisarantis et al., 2008 | 92 | 35 | 72.44 | 20.71 ± 6.95 | Singapore | Sedentary students | AP | Session | 5 W | No | LTEQ | Scores expressing frequency | |
| Prestwich et al., 2012 | 45 | 57 | 79.44 | 42.33 ± 10.62 | 41.55 ± 10.71 | UK | General adults | AP | Session | 6 M | No | SWET | Scores expressing frequency |
| Warner et al., 2016 | 25 | 67 | 75.20 | 70.34 ± 4.89 | Germany | General adults | AP + CP | Session | 14 M | No | the index of the validated PRISCUS-PAQ | No. overall PA min/week | |
| Koka and Hagger, 2016 | 62 | 72 | NR | 14–15 | NR | High-school students | AP | Session | 3 M | No | Items (not validated) | Times of MVPA > 30 min/week | |
| Arbour and Ginis 2009 | 35 | 32 | 100 | 48.17 ± 9.61 | NR | Sedentary women | AP | Session | 11 W | Record daily steps | Pedometer | Steps/day | |
| Budden, 2007 | NR | NR | 60.00 | NR | NR | NR | General adults | AP | Session | 1 W | No | Items (not validated) | Scores expressing frequency and duration |
| Morowatisharifabad et al., 2021 | 63 | 62 | 77.60 | 25–65 | Iran | Type II diabetics patients | AP + CP | Session | 3 M | 9 sessions | IPAQ | METs level of PA/week | |
| Silva et al., 2020 | 33 | 32 | 67.69 | 60.21 ± 10.83 | 63.25 ± 10.33 | Brazil | Type II diabetics patients | AP + CP | Session | 12 M | 3 on-site sessions | GSLTPAQ | Scores expressing frequency |
| Rinaldi-Miles et al., 2019 | 26 | 28 | 87.00 | 47.70 ± 9.019 | USA | Inactive adults | AP + CP | Session and online | 8 W | N | Pedometer | Steps/day | |
| Moderator | Category | Heterogeneity Test | SMD and 95% CI | Double-Tails Test | Studies | Sample Size | |||
|---|---|---|---|---|---|---|---|---|---|
| x2 | p | I2 (%) | Z | p | |||||
| Intervention strategy | Action Planning | 45.54 | <0.001 | 62.7 | 0.41 (0.24, 0.44) | 4.80 | <0.001 | 18 | 1801 |
| Action Planning and Coping Planning | 41.87 | <0.001 | 61.8 | 0.30 (0.19, 0.42) | 5.00 | <0.001 | 17 | 3638 | |
| Overall | 88.06 | <0.001 | 61.4 | 0.35 (0.25, 0.44) | 7.02 | <0.001 | 35 | 5439 | |
| Between | 1.03 | 0.310 | |||||||
| Publication Year | ≥2012 | 20.92 | 0.074 | 37.9 | 0.29 (0.16, 0.42) | 4.42 | <0.001 | 14 | 2138 |
| <2012 | 66.95 | <0.001 | 70.1 | 0.38 (0.24, 0.51) | 5.36 | <0.001 | 21 | 3301 | |
| Overall | 88.06 | <0.001 | 61.4 | 0.35 (0.25, 0.44) | 7.02 | <0.001 | 35 | 5439 | |
| Between | 0.80 | 0.371 | |||||||
| Duration | ≥5W | 70.00 | <0.001 | 68.6 | 0.36 (0.23, 0.49) | 5.49 | <0.001 | 23 | 3556 |
| <5W | 18.05 | 0.080 | 39.1 | 0.31 (0.17, 0.46) | 4.31 | <0.001 | 12 | 1883 | |
| Overall | 88.06 | <0.001 | 61.4 | 0.35 (0.25, 0.44) | 7.02 | <0.001 | 35 | 5439 | |
| Between | 0.24 | 0.628 | |||||||
| Delivery Mode | Sessions | 47.54 | <0.001 | 62.1 | 0.41 (0.27, 0.55) | 5.85 | <0.001 | 19 | 2569 |
| Online | 8.27 | 0.082 | 51.6 | 0.14 (−0.02, 0.31) | 1.69 | 0.090 | 5 | 1824 | |
| Sessions and online | 20.66 | 0.024 | 51.6 | 0.34 (0.15, 0.53) | 3.59 | <0.001 | 11 | 1046 | |
| Overall | 88.06 | <0.001 | 61.4 | 0.35 (0.25, 0.44) | 7.02 | <0.001 | 35 | 5439 | |
| Between | 6.20 | 0.045 | |||||||
| Reinforcement | Yes | 28.24 | 0.042 | 39.8 | 0.41 (0.28, 0.53) | 6.48 | <0.001 | 17 | 1950 |
| No | 48.48 | <0.001 | 67.0 | 0.28 (0.15, 0.42) | 4.12 | <0.001 | 18 | 3489 | |
| Overall | 88.06 | <0.001 | 61.4 | 0.35 (0.25, 0.44) | 7.02 | <0.001 | 35 | 5439 | |
| Between | 1.74 | 0.187 | |||||||
| Participants | Patients | 20.52 | 0.025 | 51.3 | 0.45 (0.29, 0.61) | 5.54 | <0.001 | 11 | 1437 |
| Healthy population | 57.19 | <0.001 | 59.8 | 0.29 (0.18, 0.40) | 5.01 | <0.001 | 24 | 4002 | |
| Overall | 88.06 | <0.001 | 61.4 | 0.35 (0.25, 0.44) | 7.02 | <0.001 | 35 | 5439 | |
| Between | 2.62 | 0.105 | |||||||
| Female/Male | ≥1 | 58.17 | <0.001 | 60.5 | 0.30 (0.19, 0.42) | 5.14 | <0.001 | 24 | 3975 |
| <1 | 20.66 | 0.024 | 51.6 | 0.43 (0.27, 0.58) | 5.31 | <0.001 | 11 | 1464 | |
| Overall | 88.06 | <0.001 | 61.4 | 0.35 (0.25, 0.44) | 7.02 | <0.001 | 35 | 5439 | |
| Between | 1.54 | 0.215 | |||||||
| Students | Yes | 25.77 | <0.001 | 72.8 | 0.35 (0.24, 0.45) | 2.68 | 0.007 | 8 | 1313 |
| No | 60.91 | 0.001 | 57.3 | 0.34 (0.09, 0.59) | 6.44 | <0.001 | 27 | 4126 | |
| Overall | 88.06 | <0.001 | 61.4 | 0.35 (0.25, 0.44) | 7.02 | <0.001 | 35 | 5439 | |
| Between | 0.00 | 0.951 | |||||||
| Sample Size | ≥100 | 58.90 | <0.001 | 66.0 | 0.27 (0.17, 0.38) | 5.09 | <0.001 | 21 | 4734 |
| <100 | 14.59 | 0.334 | 0.0 | 0.55 (0.38, 0.71) | 6.53 | <0.001 | 14 | 705 | |
| Overall | 88.06 | <0.001 | 61.4 | 0.35 (0.25, 0.44) | 7.02 | <0.001 | 35 | 5439 | |
| Between | 7.45 | 0.006 | |||||||
| Instrument | Objective | 2.69 | 0.101 | 62.9 | 0.08 (−0.39, 0.54) | 0.32 | 0.749 | 2 | 226 |
| Self-report(validated) | 63.95 | <0.001 | 67.2 | 0.37 (0.25, 0.49) | 5.99 | <0.001 | 22 | 4189 | |
| Self-report(no) | 15.31 | 0.121 | 34.7 | 0.36 (0.20, 0.52) | 4.34 | <0.001 | 11 | 1024 | |
| Overall | 88.06 | <0.001 | 61.4 | 0.35 (0.25, 0.44) | 7.02 | <0.001 | 35 | 5439 | |
| Between | 1.46 | 0.481 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peng, S.; Othman, A.T.; Yuan, F.; Liang, J. The Effectiveness of Planning Interventions for Improving Physical Activity in the General Population: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 7337. https://doi.org/10.3390/ijerph19127337
Peng S, Othman AT, Yuan F, Liang J. The Effectiveness of Planning Interventions for Improving Physical Activity in the General Population: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2022; 19(12):7337. https://doi.org/10.3390/ijerph19127337
Chicago/Turabian StylePeng, Sanying, Ahmad Tajuddin Othman, Fang Yuan, and Jinghong Liang. 2022. "The Effectiveness of Planning Interventions for Improving Physical Activity in the General Population: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 19, no. 12: 7337. https://doi.org/10.3390/ijerph19127337