
Episodic Future Thinking about Smoking-Related Illness: A Preliminary Investigation of Effects on Delay Discounting, Cigarette Craving, and Cigarette Demand

Abstract
:1. Introduction
2. Methods
2.1. Participants

{kind=link}
{kind=link}
{kind=link}
| Group | |||||
|---|---|---|---|---|---|
| Characteristic | EFT, n = 50 | EFT-SRI, n = 50 | ERT, n = 51 | ERT-SRI, n = 48 | Overall, n = 199 |
| Gender n (%) | |||||
| Male | 29 (58%) | 27 (54%) | 25 (49%) | 25 (52%) | 106 (53%) |
| Female | 21 (42%) | 23 (46%) | 26 (51%) | 23 (48%) | 93 (47%) |
| Racen (%) | |||||
| White/Caucasian | 40 (80%) | 46 (92%) | 45 (88%) | 44 (92%) | 175 (88%) |
| Black/African American | 3 (6.0%) | 2 (4.0%) | 4 (7.8%) | 2 (4.2%) | 11 (5.5%) |
| Asian | 5 (10%) | 1 (2.0%) | 1 (2.0%) | 1 (2.1%) | 8 (4.0%) |
| Other/Did not specify | 2 (4.0%) | 1 (2.0%) | 1 (2.0%) | 1 (2.1%) | 5 (2.5%) |
| Ethnicity n (%) | |||||
| Not Hispanic/Latino | 47 (94%) | 44 (88%) | 46 (90%) | 44 (92%) | 181 (91%) |
| Hispanic/Latino | 3 (6.0%) | 6 (12%) | 5 (9.8%) | 4 (8.3%) | 18 (9.0%) |
| Education n (%) | |||||
| High school or less | 18 (36%) | 18 (36%) | 20 (39%) | 20 (42%) | 76 (38%) |
| Associate’s degree | 5 (10%) | 6 (12%) | 7 (14%) | 4 (8.3%) | 22 (11%) |
| Bachelor’s degree | 22 (44%) | 21 (42%) | 19 (37%) | 20 (42%) | 82 (41%) |
| Post-graduate degree | 5 (10%) | 5 (10%) | 5 (9.8%) | 4 (8.3%) | 19 (9.5%) |
| Mean Household income (±SD) | 71,300 ± 41,303 | 52,900 ± 35,255 | 62,451 ± 38,799 | 47,708 ± 32,255 | 58,719 ± 37,926 |
| Mean Age (±SD) | 34.98 ± 8.71 | 36.46 ± 10.65 | 34.82 ± 10.35 | 33.27 ± 9.49 | 34.90± 9.82 |
| Mean cigarettes/day (±SD) | 12.62 ± 6.42 | 13.70 ± 6.87 | 14.00 ± 5.70 | 14.31 ± 7.57 | 13.65 ± 6.64 |
| Mean FTND score (±SD) | 4.20 ± 2.14 | 4.20 ± 2.18 | 4.59 ± 2.29 | 4.62 ± 2.39 | 4.40 ± 2.24 |
2.2. Procedures
2.3. EFT Generation Task
2.4. ERT Generation Task
2.5. EFT + SRI and ERT + SRI Generation Tasks
2.6. Delay Discounting Task
2.7. Cigarette Craving Questionnaire
2.8. Cigarette Purchase Task
2.9. Positive and Negative Affect Scale
2.10. Data Analysis
3. Results
3.1. Demographic Characteristics
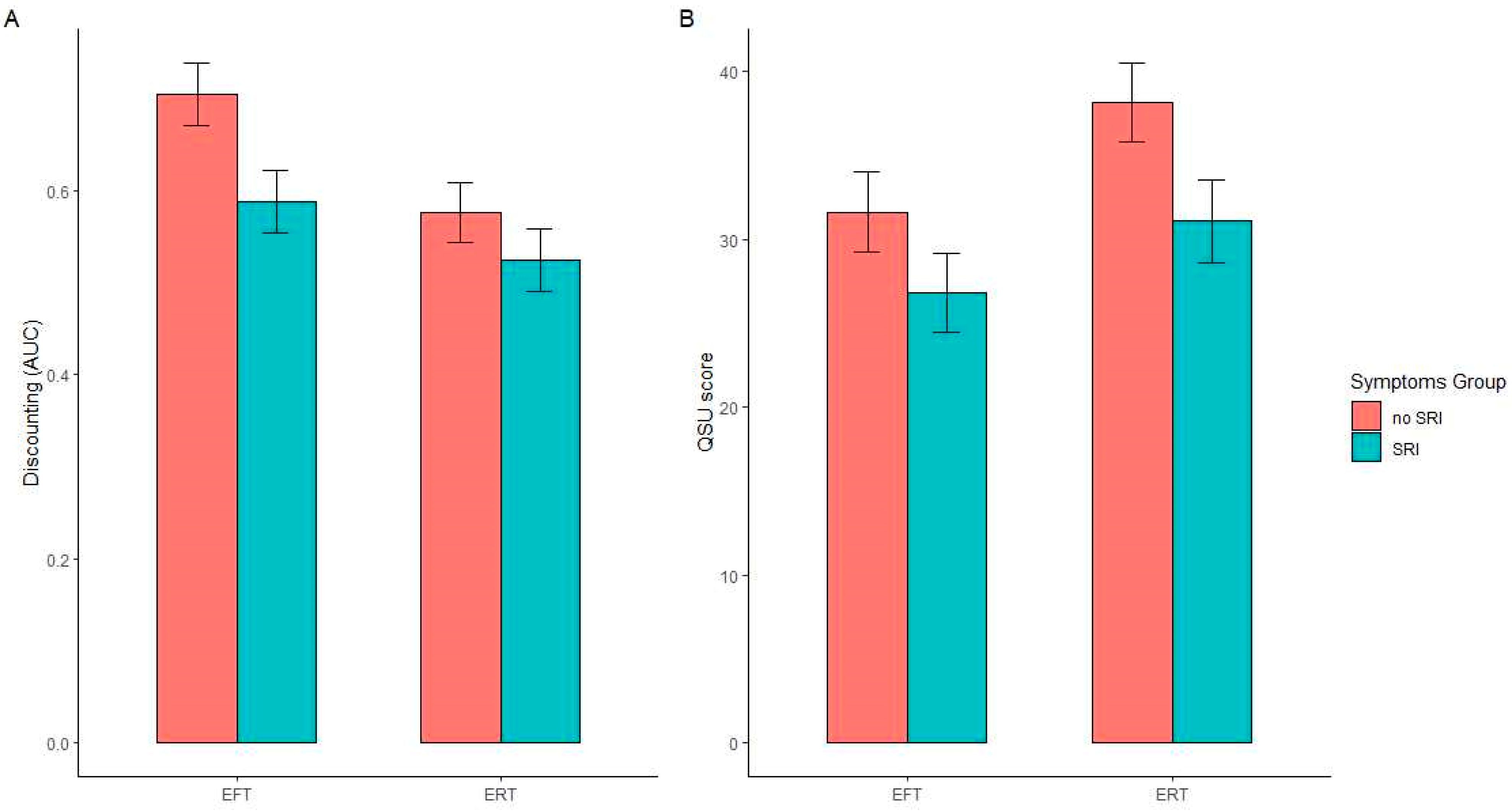
3.2. Delay Discounting
3.3. Cigarette Craving

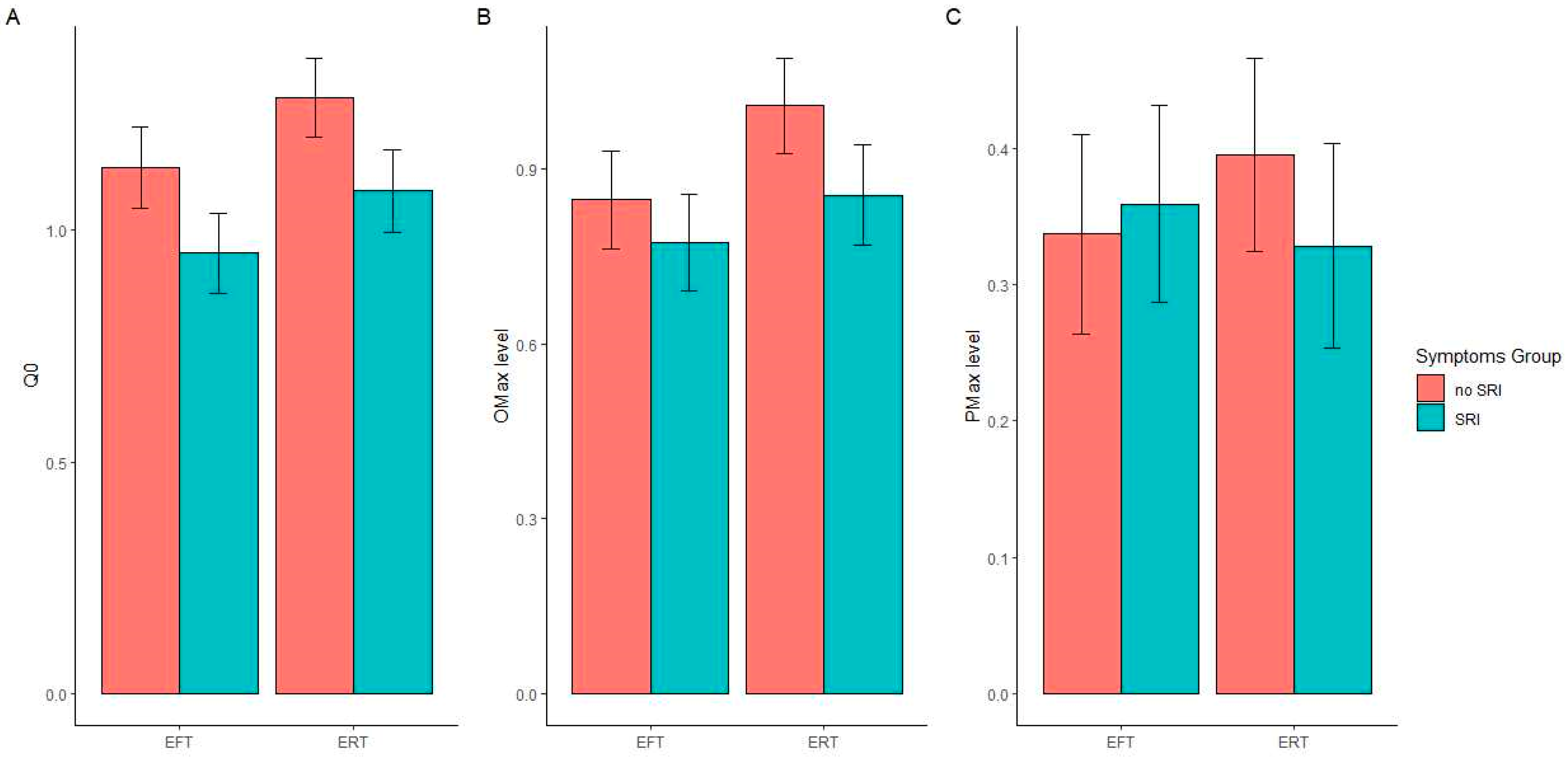
3.4. Cigarette Demand

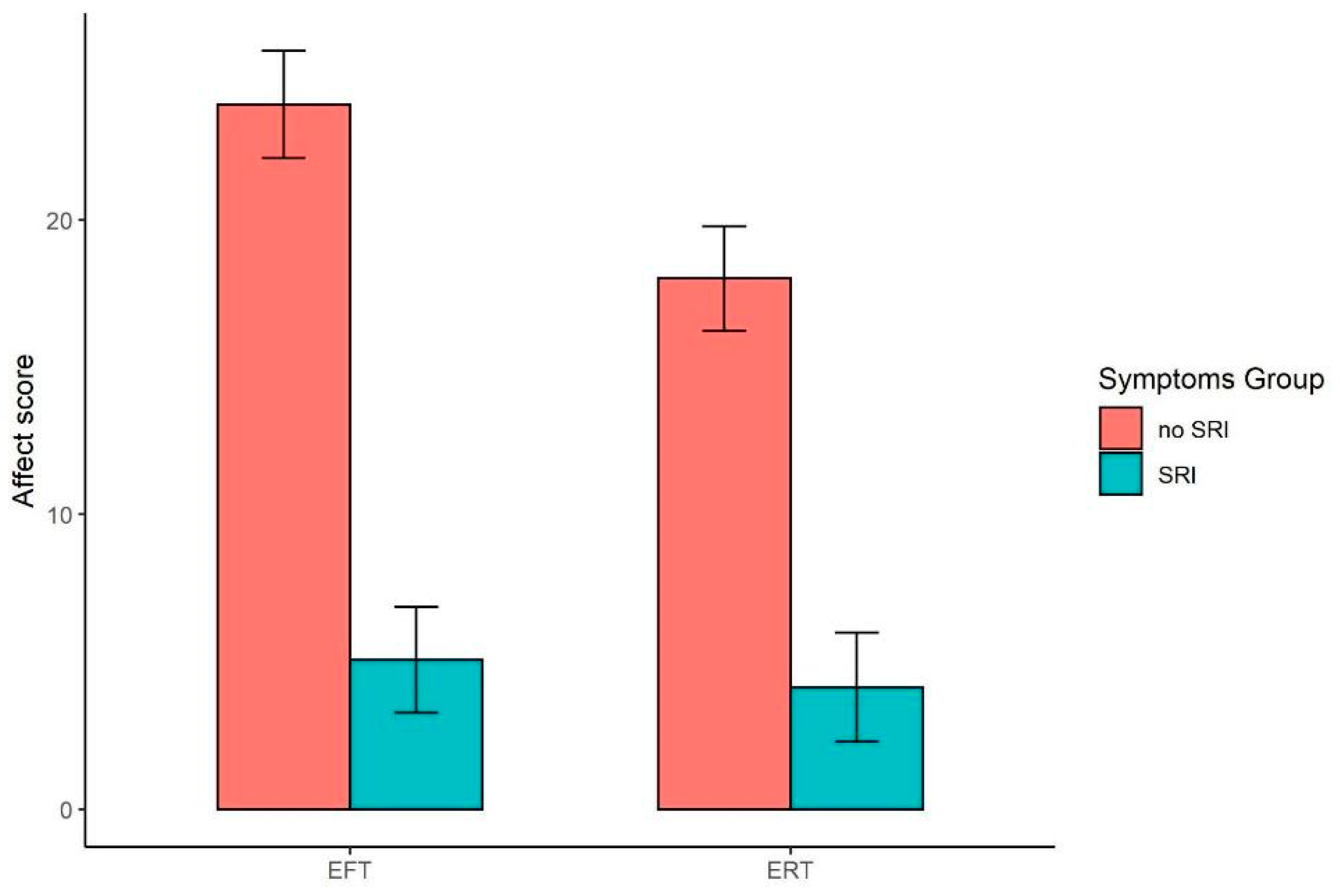
3.5. Affect
4. Discussion
4.1. Combined Effects of Episodic Future Thinking and Smoking-Related Illness
4.2. Concordance with Prior Findings on Effects of Positive Episodic Future Thinking
4.3. Concordance with Prior Findings on Effects of Negative Episodic Future Thinking
4.4. Clinical Implications
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anthonisen, N.R.; Skeans, M.A.; Wise, R.A.; Manfreda, J.; Kanner, R.E.; Connett, J.E.; Lung Health Study Research Group. The Effects of a Smoking Cessation Intervention on 14.5-Year Mortality: A Randomized Clinical Trial. Ann. Intern. Med. 2005, 142, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, E.; Travis, W.D. World Cancer Report. Lyon: Lung Cancer; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Madden, G.J.; Johnson, P.S. A Delay-Discounting Primer. In Impulsivity: The Behavioral and Neurological Science of Discounting; Madden, G.J., Ed.; American Psychological Association, XVI: Washington, DC, USA, 2010; Volume 453, pp. 11–37. [Google Scholar]
- Bickel, W.K.; Koffarnus, M.N.; Moody, L.; Wilson, A.G. The Behavioral- and Neuro-Economic Process of Temporal Discounting: A Candidate Behavioral Marker of Addiction. Neuropharmacology 2014, 76, 518–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, F.; Johnson, M.W.; Bickel, W.K. Delay Discounting in Current and Never-before Cigarette Smokers: Similarities and Differences across Commodity, Sign, and Magnitude. J. Abnorm. Psychol. 2003, 112, 382–392. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.S.; Tegge, A.N.; Turner, J.K.; Bickel, W.K. Episodic Future Thinking Reduces Delay Discounting and Cigarette Demand: An Investigation of the Good-Subject Effect. J. Behav. Med. 2018, 41, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Madden, G.J.; Petry, N.M.; Badger, G.J.; Bickel, W.K. Impulsive and Self-Control Choices in Opioid-Dependent Patients and Non-Drug-Using Control Patients: Drug and Monetary Rewards. Exp. Clin. Psychopharmacol. 1997, 5, 256–262. [Google Scholar] [CrossRef]
- Vuchinich, R.E.; Simpson, C.A. Hyperbolic Temporal Discounting in Social Drinkers and Problem Drinkers. Exp. Clin. Psychopharmacol. 1998, 6, 292–305. [Google Scholar] [CrossRef]
- Petry, N.M. Pathological Gamblers, with and without Substance Use Disorders, Discount Delayed Rewards at High Rates. J. Abnorm. Psychol. 2001, 110, 482–487. [Google Scholar] [CrossRef]
- Audrain-McGovern, J.; Rodriguez, D.; Epstein, L.H.; Cuevas, J.; Rodgers, K.; Wileyto, E.P. Does Delay Discounting Play an Etiological Role in Smoking or Is It a Consequence of Smoking? Drug Alcohol Depend. 2009, 103, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Stein, J.S.; Madden, G.J. Delay Discounting and Drug Abuse: Empirical, Conceptual, and Methodological Considerations. In The Wiley-Blackwell Handbook of Addiction Psychopharmacology; MacKillop, J., Ed.; John Wiley & Sons: New York, NY, USA, 2013; Volume 766, pp. 165–208. [Google Scholar]
- Atance, C.M.; O’Neill, D.K. Episodic Future Thinking. Trends Cogn. Sci. 2001, 5, 533–539. [Google Scholar] [CrossRef]
- Daniel, T.O.; Stanton, C.M.; Epstein, L.H. The Future Is Now: Reducing Impulsivity and Energy Intake Using Episodic Future Thinking. Psychol. Sci. 2013, 24, 2339–2342. [Google Scholar] [CrossRef]
- Peters, J.; Büchel, C. Episodic Future Thinking Reduces Reward Delay Discounting through an Enhancement of Prefrontal-Mediotemporal Interactions. Neuron 2010, 66, 138–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snider, S.E.; LaConte, S.M.; Bickel, W.K. Episodic Future Thinking: Expansion of the Temporal Window in Individuals with Alcohol Dependence. Alcohol. Clin. Exp. Res. 2016, 40, 1558–1566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, J.S.; Wilson, A.G.; Koffarnus, M.N.; Daniel, T.O.; Epstein, L.H.; Bickel, W.K. Unstuck in Time: Episodic Future Thinking Reduces Delay Discounting and Cigarette Smoking. Psychopharmacology 2016, 233, 3771–3778. [Google Scholar] [CrossRef] [PubMed]
- Sze, Y.Y.; Stein, J.S.; Bickel, W.K.; Paluch, R.A.; Epstein, L.H. Bleak Present, Bright Future: Online Episodic Future Thinking, Scarcity, Delay Discounting, and Food Demand. Clin. Psychol. Sci. 2017, 5, 683–697. [Google Scholar] [CrossRef]
- Stein, J.S.; Heckman, B.W.; Pope, D.A.; Perry, E.S.; Fong, G.T.; Cummings, K.M.; Bickel, W.K. Delay Discounting and E-Cigarette Use: An Investigation in Current, Former, and Never Cigarette Smokers. Drug Alcohol Depend. 2018, 191, 165–173. [Google Scholar] [CrossRef]
- Athamneh, L.N.; Brown, J.; Stein, J.S.; Gatchalian, K.M.; LaConte, S.M.; Bickel, W.K. Future Thinking to Decrease Real-World Drinking in Alcohol Use Disorder: Repairing Reinforcer Pathology in a Randomized Proof-of-Concept Trial. Exp. Clin. Psychopharmacol. 2021, 30, 326–337. [Google Scholar] [CrossRef]
- Sze, Y.Y.; Daniel, T.O.; Kilanowski, C.K.; Collins, R.L.; Epstein, L.H. Web-Based and Mobile Delivery of an Episodic Future Thinking Intervention for Overweight and Obese Families: A Feasibility Study. JMIR Mhealth Uhealth 2015, 3, e97. [Google Scholar] [CrossRef]
- Daniel, T.O.; Said, M.; Stanton, C.M.; Epstein, L.H. Episodic Future Thinking Reduces Delay Discounting and Energy Intake in Children. Eat. Behav. 2015, 18, 20–24. [Google Scholar] [CrossRef]
- Lin, H.; Epstein, L.H. Living in the Moment: Effects of Time Perspective and Emotional Valence of Episodic Thinking on Delay Discounting. Behav. Neurosci. 2014, 128, 12–19. [Google Scholar] [CrossRef] [Green Version]
- Du, W.; Green, L.; Myerson, J. Cross-Cultural Comparisons of Discounting Delayed and Probabilistic Rewards. Psychol. Rec. 2002, 52, 479–492. [Google Scholar] [CrossRef]
- Craft, W.H.; Tegge, A.N.; Freitas-Lemos, R.; Tomlinson, D.C.; Bickel, W.K. Are Poor Quality Data Just Random Responses?: A Crowdsourced Study of Delay Discounting in Alcohol Use Disorder. Exp. Clin. Psychopharmacol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.S.; Brown, J.M.; Tegge, A.N.; Freitas-Lemos, R.; Koffarnus, M.N.; Bickel, W.K.; Madden, G.J. Choice Bundling Increases Valuation of Delayed Losses More Than Gains in Cigarette Smokers. Front. Behav. Neurosci. 2021, 15, 796502. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.S.; Madden, G.J. Choice Bundling, Unpacked: Observed and Predicted Effects on Intertemporal Choice in an Additive Model of Hyperbolic Delay Discounting. PLoS ONE 2021, 16, e0259830. [Google Scholar] [CrossRef] [PubMed]
- Toll, B.A.; Katulak, N.A.; McKee, S.A. Investigating the Factor Structure of the Questionnaire on Smoking Urges-Brief (QSU-Brief). Addict. Behav. 2006, 31, 1231–1239. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, E.A.; Bickel, W.K. Modeling Drug Consumption in the Clinic Using Simulation Procedures: Demand for Heroin and Cigarettes in Opioid-Dependent Outpatients. Exp. Clin. Psychopharmacol. 1999, 7, 412–426. [Google Scholar] [CrossRef]
- MacKillop, J.; Murphy, J.G. A Behavioral Economic Measure of Demand for Alcohol Predicts Brief Intervention Outcomes. Drug Alcohol Depend. 2007, 89, 227–233. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and Validation of Brief Measures of Positive and Negative Affect: The PANAS Scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Johnson, M.W.; Bickel, W.K. An Algorithm for Identifying Nonsystematic Delay-Discounting Data. Exp. Clin. Psychopharmacol. 2008, 16, 264–274. [Google Scholar] [CrossRef] [Green Version]
- Myerson, J.; Green, L.; Warusawitharana, M. Area under the Curve as a Measure of Discounting. J. Exp. Anal. Behav. 2001, 76, 235–243. [Google Scholar] [CrossRef] [Green Version]
- Stein, J.S.; Koffarnus, M.N.; Snider, S.E.; Quisenberry, A.J.; Bickel, W.K. Identification and Management of Nonsystematic Purchase Task Data: Toward Best Practice. Exp. Clin. Psychopharmacol. 2015, 23, 377. [Google Scholar] [CrossRef]
- Hursh, S.R.; Silberberg, A. Economic Demand and Essential Value. Psychol. Rev. 2008, 115, 186–198. [Google Scholar] [CrossRef]
- Koffarnus, M.N.; Franck, C.T.; Stein, J.S.; Bickel, W.K. A Modified Exponential Behavioral Economic Demand Model to Better Describe Consumption Data. Exp. Clin. Psychopharmacol. 2015, 23, 504–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bidwell, L.C.; MacKillop, J.; Murphy, J.G.; Tidey, J.W.; Colby, S.M. Latent Factor Structure of a Behavioral Economic Cigarette Demand Curve in Adolescent Smokers. Addict. Behav. 2012, 37, 1257–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fredrickson, B.L.; Losada, M.F. Positive Affect and the Complex Dynamics of Human Flourishing. Am. Psychol. 2005, 60, 678–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, R.M.; Reynolds, C.F.; Thase, M.E.; Frank, E.; Fasiczka, A.L.; Haaga, D.A.F. Optimal and Normal Affect Balance in Psychotherapy of Major Depression: Evaluation of the Balanced States of Mind Model. Behav. Cogn. Psychother. 2002, 30, 439–450. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA; Academic Press: Cambridge, MA, USA, 1988; pp. 18–74. [Google Scholar]
- Fields, S.A.; Lange, K.; Ramos, A.; Thamotharan, S.; Rassu, F. The Relationship between Stress and Delay Discounting: A Meta-Analytic Review. Behav. Pharmacol. 2014, 25, 434–444. [Google Scholar] [CrossRef]
- Bulley, A.; Miloyan, B.; Pepper, G.V.; Gullo, M.J.; Henry, J.D.; Suddendorf, T. Cuing Both Positive and Negative Episodic Foresight Reduces Delay Discounting but Does Not Affect Risk-Taking. Q. J. Exp. Psychol. 2019, 72, 1998–2017. [Google Scholar] [CrossRef]
- Calluso, C.; Tosoni, A.; Cannito, L.; Committeri, G. Concreteness and Emotional Valence of Episodic Future Thinking (EFT) Independently Affect the Dynamics of Intertemporal Decisions. PLoS ONE 2019, 14, e0217224. [Google Scholar] [CrossRef]
- Liu, L.; Feng, T.; Chen, J.; Li, H. The Value of Emotion: How Does Episodic Prospection Modulate Delay Discounting? PLoS ONE 2013, 8, e81717. [Google Scholar] [CrossRef]
- Zhang, S.; Peng, J.; Qin, L.; Suo, T.; Feng, T. Prospective Emotion Enables Episodic Prospection to Shift Time Preference. Br. J. Psychol. 2018, 109, 487–499. [Google Scholar] [CrossRef]
- O’Neill, J.; Daniel, T.O.; Epstein, L.H. Episodic Future Thinking Reduces Eating in a Food Court. Eat. Behav. 2016, 20, 9–13. [Google Scholar] [CrossRef] [PubMed]

| Group | |||||
|---|---|---|---|---|---|
| Measure | Criterion | EFT | EFT-SRI | ERT | ERT-SRI |
| Delay discounting | Trend | 15 | 5 | 7 | 4 |
| Bounce | 0 | 0 | 2 | 0 | |
| Cigarette demand | Trend a | 2 | 8 | 0 | 7 |
| Bounce | 0 | 0 | 0 | 0 | |
| Reversal | 0 | 0 | 0 | 0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruhi-Williams, P.; King, M.J.; Stein, J.S.; Bickel, W.K. Episodic Future Thinking about Smoking-Related Illness: A Preliminary Investigation of Effects on Delay Discounting, Cigarette Craving, and Cigarette Demand. Int. J. Environ. Res. Public Health 2022, 19, 7136. https://doi.org/10.3390/ijerph19127136
Ruhi-Williams P, King MJ, Stein JS, Bickel WK. Episodic Future Thinking about Smoking-Related Illness: A Preliminary Investigation of Effects on Delay Discounting, Cigarette Craving, and Cigarette Demand. International Journal of Environmental Research and Public Health. 2022; 19(12):7136. https://doi.org/10.3390/ijerph19127136
Chicago/Turabian StyleRuhi-Williams, Perisa, Mary J. King, Jeffrey S. Stein, and Warren K. Bickel. 2022. "Episodic Future Thinking about Smoking-Related Illness: A Preliminary Investigation of Effects on Delay Discounting, Cigarette Craving, and Cigarette Demand" International Journal of Environmental Research and Public Health 19, no. 12: 7136. https://doi.org/10.3390/ijerph19127136