
Association of Peripheral Arterial Occlusive Disease and Deep Venous Thrombosis with Risk of Consequent Sepsis Event: A Retrospective Population-Based Cohort Study

 , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
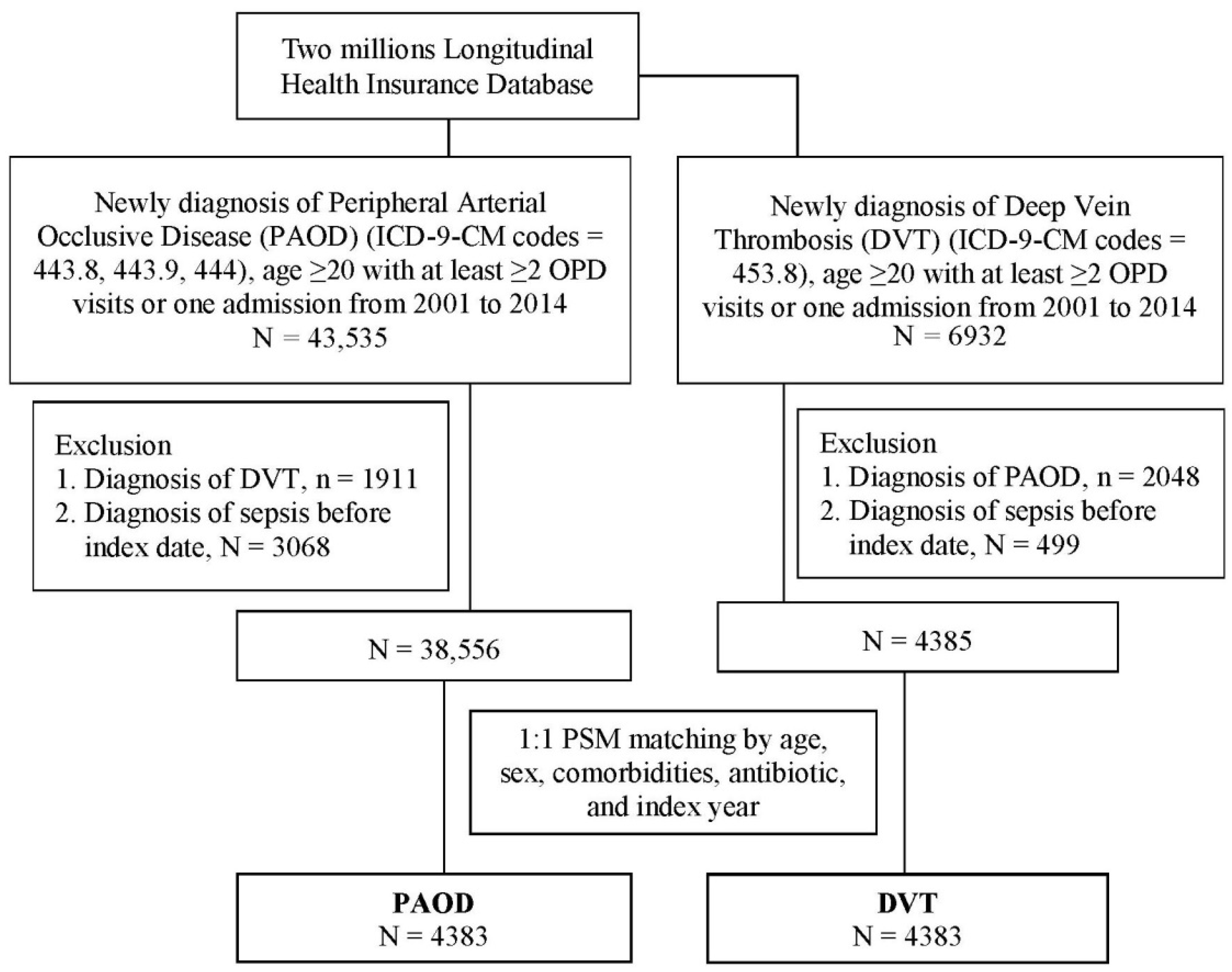
2.1. Study Design and Participants
2.2. Study Group and Outcome
2.3. Covariates and Matching
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
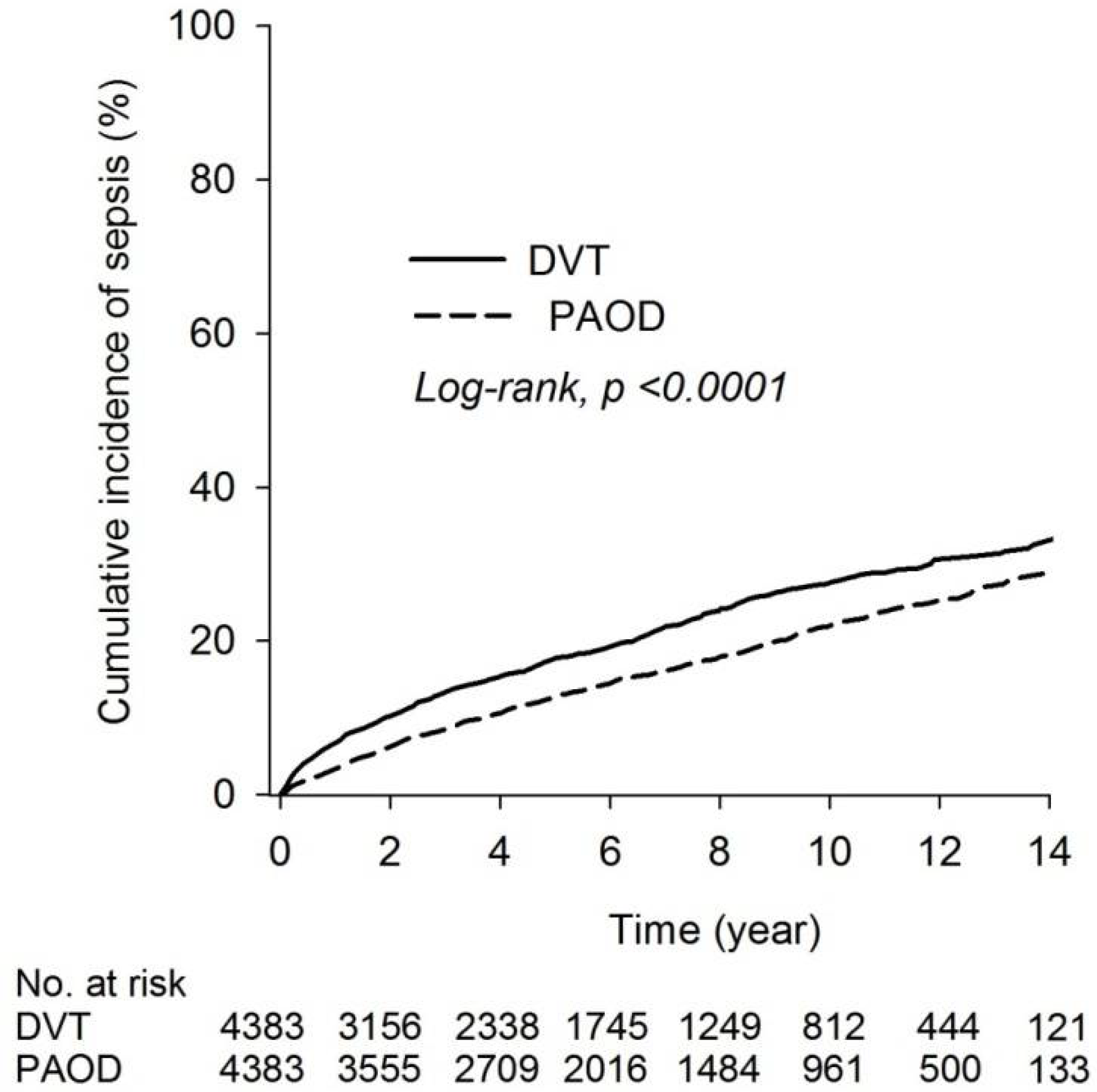
3.2. Risk of Sepsis between DVT and PAOD Group
3.3. Comparison of Risk of Sepsis between DVT and PAOD Group
3.4. Subgroup Analysis of Sepsis Risk in DVT Group Relative to PAOD Group after PSM
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Poredos, P.; Poredos, P. Peripheral arterial occlusive disease and perioperative risk. Int. Angiol. 2018, 37, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Costantini, V.; Lenti, M. Treatment of acute occlusion of peripheral arteries. Thromb. Res. 2002, 106, V285–V294. [Google Scholar] [CrossRef]
- Hsu, P.C.; Chiu, C.A.; Chu, C.Y.; Lee, W.H.; Su, H.M.; Lin, T.H.; Voon, W.C.; Lai, W.T.; Sheu, S.H. CHADS2 Score and Risk of New-onset Peripheral Arterial Occlusive Disease in Patients without Atrial Fibrillation: A Nationwide Cohort Study in Taiwan. J. Atheroscler. Thromb. 2015, 22, 490–498. [Google Scholar] [CrossRef] [Green Version]
- Hooi, J.D.; Stoffers, H.E.; Kester, A.D.; Rinkens, P.E.; Kaiser, V.; van Ree, J.W.; Knottnerus, J.A. Risk factors and cardiovascular diseases associated with asymptomatic peripheral arterial occlusive disease: The Limburg PAOD Study. Scand. J. Prim. Health Care 1998, 16, 177–182. [Google Scholar] [CrossRef]
- Cote, L.P.; Greenberg, S.; Caprini, J.A.; Tafur, A.; Choi, C.; Muñoz, F.J.; Skride, A.; Valero, B.; Porras, J.A.; Ciammaichella, M.; et al. Comparisons Between Upper and Lower Extremity Deep Vein Thrombosis: A Review of the RIETE Registry. Clin. Appl. Thromb. Hemost. 2017, 23, 748–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jezovnik, M.K.; Fareed, J.; Poredos, P. Patients With a History of Idiopathic Deep Venous Thrombosis Have Long-Term Increased Levels of Inflammatory Markers and Markers of Endothelial Damage. Clin. Appl. Thromb. 2017, 23, 124–131. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.L.; Chu, P.H.; Lee, C.H.; Pai, P.Y.; Lin, P.Y.; Shyu, K.G.; Chang, W.T.; Chiu, K.M.; Huang, C.L.; Lee, C.Y.; et al. Management of Venous Thromboembolisms: Part I. The Consensus for Deep Vein Thrombosis. Acta Cardiol. Sin. 2016, 32, 1–22. [Google Scholar] [CrossRef]
- Fowkes, F.J.; Price, J.F.; Fowkes, F.G. Incidence of diagnosed deep vein thrombosis in the general population: Systematic review. Eur. J. Vasc. Endovasc. Surg. 2003, 25, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Yeh, Y.T.; Tsai, S.E.; Chen, Y.C.; Yang, S.F.; Yeh, H.W.; Wang, B.Y.; Yeh, L.T.; Shih, N.C.; Wang, Y.H.; Chen, Y.Y.; et al. Deep Venous Thrombosis and Risk of Consequent Sepsis Event: A Retrospective Nationwide Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 7879. [Google Scholar] [CrossRef]
- Takemoto, T.; Soh, J.; Ohara, S.; Fujino, T.; Koga, T.; Nishino, M.; Hamada, A.; Chiba, M.; Shimoji, M.; Suda, K.; et al. The prevalence and risk factors associated with preoperative deep venous thrombosis in lung cancer surgery. Surg. Today 2021, 51, 1480–1487. [Google Scholar] [CrossRef]
- Sancini, A.; Tomei, G.; Schifano, M.P.; Nardone, N.; Andreozzi, G.; Scimitto, L.; Fiaschetti, M.; De Sio, S.; Scala, B.; Capozzella, A.; et al. Phlebopathies and occupation. Ann. Di Ig. Med. Prev. Comunita 2012, 24, 131–144. [Google Scholar]
- Shaydakov, M.E.; Comerota, A.J.; Lurie, F. Primary venous insufficiency increases risk of deep vein thrombosis. J. Vasc. Surg. Venous Lymphat. Disord. 2016, 4, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Cecconi, M.; Evans, L.; Levy, M.; Rhodes, A. Sepsis and septic shock. Lancet 2018, 392, 75–87. [Google Scholar] [CrossRef]
- Lelubre, C.; Vincent, J.L. Mechanisms and treatment of organ failure in sepsis. Nat. Rev. Nephrol. 2018, 14, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Lever, A.; Mackenzie, I. Sepsis: Definition, epidemiology, and diagnosis. BMJ 2007, 335, 879–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.J.; Chen, F.L.; Chen, J.H.; Wu, M.M.; Chen, Y.L.; Chien, D.S.; Ko, Y. Epidemiology of sepsis in Taiwan. Medicine 2019, 98, e15725. [Google Scholar] [CrossRef]
- Van den Berg, M.; Boers, G.H.; Franken, D.G.; Blom, H.J.; Van Kamp, G.J.; Jakobs, C.; Rauwerda, J.A.; Kluft, C.; Stehouwert, C.D. Hyperhomocysteinaemia and endothelial dysfunction in young patients with peripheral arterial occlusive disease. Eur. J. Clin. Investig. 1995, 25, 176–181. [Google Scholar] [CrossRef] [Green Version]
- Iwashima, Y.; Horio, T.; Suzuki, Y.; Kihara, S.; Rakugi, H.; Kangawa, K.; Funahashi, T.; Ogihara, T.; Kawano, Y. Adiponectin and inflammatory markers in peripheral arterial occlusive disease. Atherosclerosis 2006, 188, 384–390. [Google Scholar] [CrossRef]
- Signorelli, S.S.; Mazzarino, M.C.; Spandidos, D.A.; Malaponte, G. Proinflammatory circulating molecules in peripheral arterial disease. Int. J. Mol. Med. 2007, 20, 279–286. [Google Scholar] [CrossRef] [Green Version]
- Vazquez-Garza, E.; Jerjes-Sanchez, C.; Navarrete, A.; Joya-Harrison, J.; Rodriguez, D. Venous thromboembolism: Thrombosis, inflammation, and immunothrombosis for clinicians. J. Thromb. Thrombolysis 2017, 44, 377–385. [Google Scholar] [CrossRef]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kou, C.J.; Batzlaff, C.; Bezzant, M.L.; Sjulin, T. Phlegmasia Cerulea Dolens: A Life-Threatening Manifestation of Deep Vein Thrombosis. Cureus 2020, 12, e8587. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, M.J.; Mouyis, M.; Thomas, M. Deep vein thrombosis. BMJ 2018, 360, k351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsakiris, D.A.; Tschöpl, M.; Jäger, K.; Haefeli, W.E.; Wolf, F.; Marbet, G.A. Circulating cell adhesion molecules and endothelial markers before and after transluminal angioplasty in peripheral arterial occlusive disease. Atherosclerosis 1999, 142, 193–200. [Google Scholar] [CrossRef]
- Brevetti, G.; Schiano, V.; Chiariello, M. Cellular adhesion molecules and peripheral arterial disease. Vasc. Med. 2006, 11, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Diaz, J.A. Inflammation and acute venous thrombosis. US Oncol. Hematol. 2011, 7, 68. [Google Scholar] [CrossRef] [Green Version]
- Della Valle, P.; Pavani, G.; D’Angelo, A. The protein C pathway and sepsis. Thromb. Res. 2012, 129, 296–300. [Google Scholar] [CrossRef]
- Liang, Y.; Huang, X.; Jiang, Y.; Qin, Y.; Peng, D.; Huang, Y.; Li, J.; Sooranna, S.R.; Pinhu, L. Endothelial protein C receptor polymorphisms and risk of sepsis in a Chinese population. J. Int. Med. Res. 2017, 45, 504–513. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.H.; Hsu, T.C.; Lee, M.G.; Chao, C.C.; Lee, W.C.; Lai, C.C.; Lee, C.C. Nationwide Trend of Sepsis: A Comparison Among Octogenarians, Elderly, and Young Adults. Crit. Care Med. 2018, 46, 926–934. [Google Scholar] [CrossRef]
- Rowe, T.A.; McKoy, J.M. Sepsis in Older Adults. Infect. Dis. Clin. N. Am. 2017, 31, 731–742. [Google Scholar] [CrossRef]
- Barter, J.; Kumar, A.; Stortz, J.A.; Hollen, M.; Nacionales, D.; Efron, P.A.; Moldawer, L.L.; Foster, T.C. Age and Sex Influence the Hippocampal Response and Recovery Following Sepsis. Mol. Neurobiol. 2019, 56, 8557–8572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girard, T.D.; Ely, E.W. Bacteremia and sepsis in older adults. Clin. Geriatr. Med. 2007, 23, 633–647. [Google Scholar] [CrossRef] [PubMed]
- Campanelli, F.; Landoni, G.; Cabrini, L.; Zangrillo, A. Gender differences in septic intensive care unit patients. Minerva Anestesiol. 2018, 84, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Choudhry, M.A.; Bland, K.I.; Chaudry, I.H. Gender and susceptibility to sepsis following trauma. Endocr. Metab. Immune Disord. Drug Targets 2006, 6, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Adrie, C.; Azoulay, E.; Francais, A.; Clec’h, C.; Darques, L.; Schwebel, C.; Nakache, D.; Jamali, S.; Goldgran-Toledano, D.; Garrouste-Orgeas, M.; et al. Influence of gender on the outcome of severe sepsis: A reappraisal. Chest 2007, 132, 1786–1793. [Google Scholar] [CrossRef] [PubMed]
- Frink, M.; Pape, H.C.; van Griensven, M.; Krettek, C.; Chaudry, I.H.; Hildebrand, F. Influence of sex and age on mods and cytokines after multiple injuries. Shock 2007, 27, 151–156. [Google Scholar] [CrossRef]
- Sakr, Y.; Elia, C.; Mascia, L.; Barberis, B.; Cardellino, S.; Livigni, S.; Fiore, G.; Filippini, C.; Ranieri, V.M. The influence of gender on the epidemiology of and outcome from severe sepsis. Crit. Care 2013, 17, R50. [Google Scholar] [CrossRef] [Green Version]
- Trentzsch, H.; Nienaber, U.; Behnke, M.; Lefering, R.; Piltz, S. Female sex protects from organ failure and sepsis after major trauma haemorrhage. Injury 2014, 45 (Suppl. S3), S20–S28. [Google Scholar] [CrossRef]
- Im, Y.; Kang, D.; Ko, R.E.; Lee, Y.J.; Lim, S.Y.; Park, S.; Na, S.J.; Chung, C.R.; Park, M.H.; Oh, D.K.; et al. Time-to-antibiotics and clinical outcomes in patients with sepsis and septic shock: A prospective nationwide multicenter cohort study. Crit. Care 2022, 26, 19. [Google Scholar] [CrossRef]
- Davies, S.W.; Efird, J.T.; Guidry, C.A.; Hranjec, T.; Metzger, R.; Swenson, B.R.; Sawyer, R.G. Characteristics of surgical patients receiving inappropriate empiric antimicrobial therapy. J. Trauma Acute Care Surg. 2014, 77, 546–554. [Google Scholar] [CrossRef] [Green Version]
- Wuillemin, W.A.; Solenthaler, M. Hyperhomocysteinemia: A risk factor for arterial and venous thrombosis. VASA. Z. Fur Gefasskrankh. 1999, 28, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.H.; Lin, C.L.; Lee, F.Y.; Wang, Y.C.; Kao, C.H. Leptospirosis and Peripheral Artery Occlusive Disease: A Nationwide Cohort Analysis. Medicine 2016, 95, e3127. [Google Scholar] [CrossRef] [PubMed]
- Samama, M.M. An epidemiologic study of risk factors for deep vein thrombosis in medical outpatients: The Sirius study. Arch. Intern. Med. 2000, 160, 3415–3420. [Google Scholar] [CrossRef] [PubMed]
- Smeeth, L.; Cook, C.; Thomas, S.; Hall, A.J.; Hubbard, R.; Vallance, P. Risk of deep vein thrombosis and pulmonary embolism after acute infection in a community setting. Lancet 2006, 367, 1075–1079. [Google Scholar] [CrossRef]
- Tichelaar, Y.I.; Kluin-Nelemans, H.J.; Meijer, K. Infections and inflammatory diseases as risk factors for venous thrombosis. A systematic review. Thromb. Haemost. 2012, 107, 827–837. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Before PSM Matching | After PSM Matching | |||||
|---|---|---|---|---|---|---|
| PAOD (N = 38,556) | DVT (N = 4385) | ASD | PAOD (N = 4383) | DVT (N = 4383) | ASD | |
| Age, Mean ± SD | 63.31 ± 14.72 | 62.36 ± 16.31 | 0.061 | 62.65 ± 15.77 | 62.36 ± 16.31 | 0.018 |
| Female sex | 20,194 (52.4) | 2617 (59.7) | 0.148 | 2596 (59.2) | 2615 (59.7) | 0.009 |
| Hypertension | 18,823 (48.8) | 1845 (42.1) | 0.136 | 1893 (43.2) | 1845 (42.1) | 0.022 |
| Hyperlipidemia | 7899 (20.5) | 629 (14.3) | 0.163 | 610 (13.9) | 629 (14.4) | 0.012 |
| Diabetes | 10,483 (27.2) | 764 (17.4) | 0.236 | 750 (17.1) | 764 (17.4) | 0.008 |
| Ischemic heart disease | 6892 (17.9) | 667 (15.2) | 0.072 | 679 (15.5) | 667 (15.2) | 0.008 |
| Chronic kidney disease | 2038 (5.3) | 326 (7.4) | 0.088 | 308 (7.0) | 326 (7.4) | 0.016 |
| COPD | 2936 (7.6) | 322 (7.3) | 0.010 | 335 (7.6) | 322 (7.4) | 0.011 |
| Intracranial bleeding | 307 (0.8) | 62 (1.4) | 0.059 | 52 (1.2) | 61 (1.4) | 0.018 |
| Stroke | 4801 (12.5) | 431 (9.8) | 0.083 | 423 (9.7) | 431 (9.8) | 0.006 |
| Malignancy | 1666 (4.3) | 679 (15.5) | 0.380 | 699 (16.0) | 677 (15.5) | 0.014 |
| Rheumatoid Arthritis | 468 (1.2) | 52 (1.2) | 0.003 | 39 (0.9) | 52 (1.2) | 0.029 |
| SLE | 76 (0.2) | 31 (0.7) | 0.076 | 17 (0.4) | 30 (0.7) | 0.041 |
| Sjogren’s syndrome | 292 (0.8) | 31 (0.7) | 0.006 | 18 (0.4) | 31 (0.7) | 0.040 |
| Ankylosing spondylitis | 83 (0.2) | 16 (0.4) | 0.028 | 14 (0.3) | 16 (0.4) | 0.008 |
| Psoriasis | 144 (0.4) | 21 (0.5) | 0.016 | 10 (0.2) | 21 (0.5) | 0.042 |
| Antibiotic | 9837 (25.5) | 1260 (28.7) | 0.072 | 1238 (28.3) | 1259 (28.7) | 0.011 |
| Before PSM | After PSM | |||
|---|---|---|---|---|
| PAOD | DVT | PAOD | DVT | |
| N | 38,556 | 4385 | 4383 | 4383 |
| Person-years | 229,482.07 | 23,772.84 | 26,954 | 23,756 |
| No. of sepsis | 5859 | 846 | 694 | 846 |
| ID (95% C.I.) | 25.53 (24.88–26.19) | 35.59 (33.27–38.07) | 25.75 (23.90–27.74) | 35.61 (33.29–38.09) |
| Relative risk (95% C.I.) | Reference | 1.39 (1.30–1.50) | Reference | 1.38 (1.25–1.53) |
| Univariate | Multivariate † | |||
|---|---|---|---|---|
| HR (95% C.I.) | p Value | HR (95% C.I.) | p Value | |
| Group | ||||
| PAOD | Reference | Reference | ||
| DVT | 1.37 (1.24–1.51) | <0.001 | 1.42 (1.29–1.58) | <0.001 |
| Age | 1.06 (1.05–1.06) | <0.001 | 1.05 (1.04–1.05) | <0.001 |
| Sex | ||||
| Female | Reference | Reference | ||
| Male | 1.39 (1.26–1.54) | <0.001 | 1.11 (1.00–1.23) | 0.059 |
| Hypertension | 2.05 (1.85–2.26) | <0.001 | 0.96 (0.86–1.08) | 0.511 |
| Hyperlipidemia | 1.12 (0.97–1.30) | 0.116 | - | - |
| Diabetes | 2.25 (2.01–2.53) | <0.001 | 1.54 (1.37–1.74) | <0.001 |
| Ischemic heart disease | 1.76 (1.56–1.99) | <0.001 | 1.02 (0.90–1.16) | 0.759 |
| Chronic kidney disease | 2.89 (2.50–3.34) | <0.001 | 2.42 (2.09–2.80) | <0.001 |
| COPD | 2.56 (2.22–2.96) | <0.001 | 1.46 (1.26–1.70) | <0.001 |
| Intracranial bleeding | 2.80 (2.07–3.77) | <0.001 | 1.88 (1.38–2.55) | <0.001 |
| Stroke | 2.70 (2.37–3.07) | <0.001 | 1.58 (1.38–1.82) | <0.001 |
| Malignancy | 2.12 (1.87–2.41) | <0.001 | 1.84 (1.62–2.09) | <0.001 |
| Rheumatoid Arthritis | 1.18 (0.74–1.88) | 0.481 | - | - |
| SLE | 2.16 (1.30–3.59) | 0.003 | 4.18 (2.50–6.99) | <0.001 |
| Sjogren’s syndrome | 1.11 (0.56–2.23) | 0.762 | - | - |
| Ankylosing spondylitis | 0.42 (0.10–1.66) | 0.215 | - | - |
| Psoriasis | 1.37 (0.65–2.87) | 0.411 | - | - |
| Antibiotic | 1.59 (1.43–1.76) | <0.001 | 1.38 (1.24–1.53) | <0.001 |
| Peripheral Artery Occlusive Disease (PAOD) | Deep Venous Thrombosis (DVT) | |||||
|---|---|---|---|---|---|---|
| N | No. of Sepsis | N | No. of Sepsis | HR (95% C.I.) | p Value | |
| Age 1 | ||||||
| 20–39 | 423 | 16 | 447 | 38 | 2.28 (1.25–4.16) | 0.007 |
| 40–64 | 1790 | 164 | 1868 | 231 | 1.50 (1.22–1.83) | <0.001 |
| ≥65 | 2170 | 514 | 2068 | 577 | 1.34 (1.19–1.51) | <0.001 |
| p for interaction = 0.2031 | ||||||
| Sex 2 | ||||||
| Female | 2596 | 371 | 2615 | 488 | 1.43 (1.24–1.63) | <0.001 |
| Male | 1787 | 323 | 1768 | 358 | 1.45 (1.24–1.69) | <0.001 |
| p for interaction = 0.9210 | ||||||
| Antibiotic 2 | ||||||
| No | 3145 | 432 | 3124 | 549 | 1.44 (1.27–1.63) | <0.001 |
| Yes | 1238 | 262 | 1259 | 297 | 1.39 (1.18–1.65) | <0.001 |
| p for interaction = 0.5823 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, B.-Y.; Chou, Y.-H.; Chung, C.-T.; Yang, S.-F.; Tzeng, S.-L.; Wang, Y.-H.; Chou, M.-C.; Yeh, C.-B.; Chan, C.-H. Association of Peripheral Arterial Occlusive Disease and Deep Venous Thrombosis with Risk of Consequent Sepsis Event: A Retrospective Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 6710. https://doi.org/10.3390/ijerph19116710
Wang B-Y, Chou Y-H, Chung C-T, Yang S-F, Tzeng S-L, Wang Y-H, Chou M-C, Yeh C-B, Chan C-H. Association of Peripheral Arterial Occlusive Disease and Deep Venous Thrombosis with Risk of Consequent Sepsis Event: A Retrospective Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(11):6710. https://doi.org/10.3390/ijerph19116710
Chicago/Turabian StyleWang, Bo-Yuan, Ying-Hsiang Chou, Chi-Tzu Chung, Shun-Fa Yang, Shu-Ling Tzeng, Yu-Hsun Wang, Ming-Chih Chou, Chao-Bin Yeh, and Chi-Ho Chan. 2022. "Association of Peripheral Arterial Occlusive Disease and Deep Venous Thrombosis with Risk of Consequent Sepsis Event: A Retrospective Population-Based Cohort Study" International Journal of Environmental Research and Public Health 19, no. 11: 6710. https://doi.org/10.3390/ijerph19116710