
Effects of Exercise Intervention on Students’ Test Anxiety: A Systematic Review with a Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection and Exclusion Criteria of Study
2.3. Data Extraction and Quality Evaluation
2.3.1. Data Extraction and Processing
2.3.2. Study Quality Evaluation
2.4. Statistical Analysis
3. Results
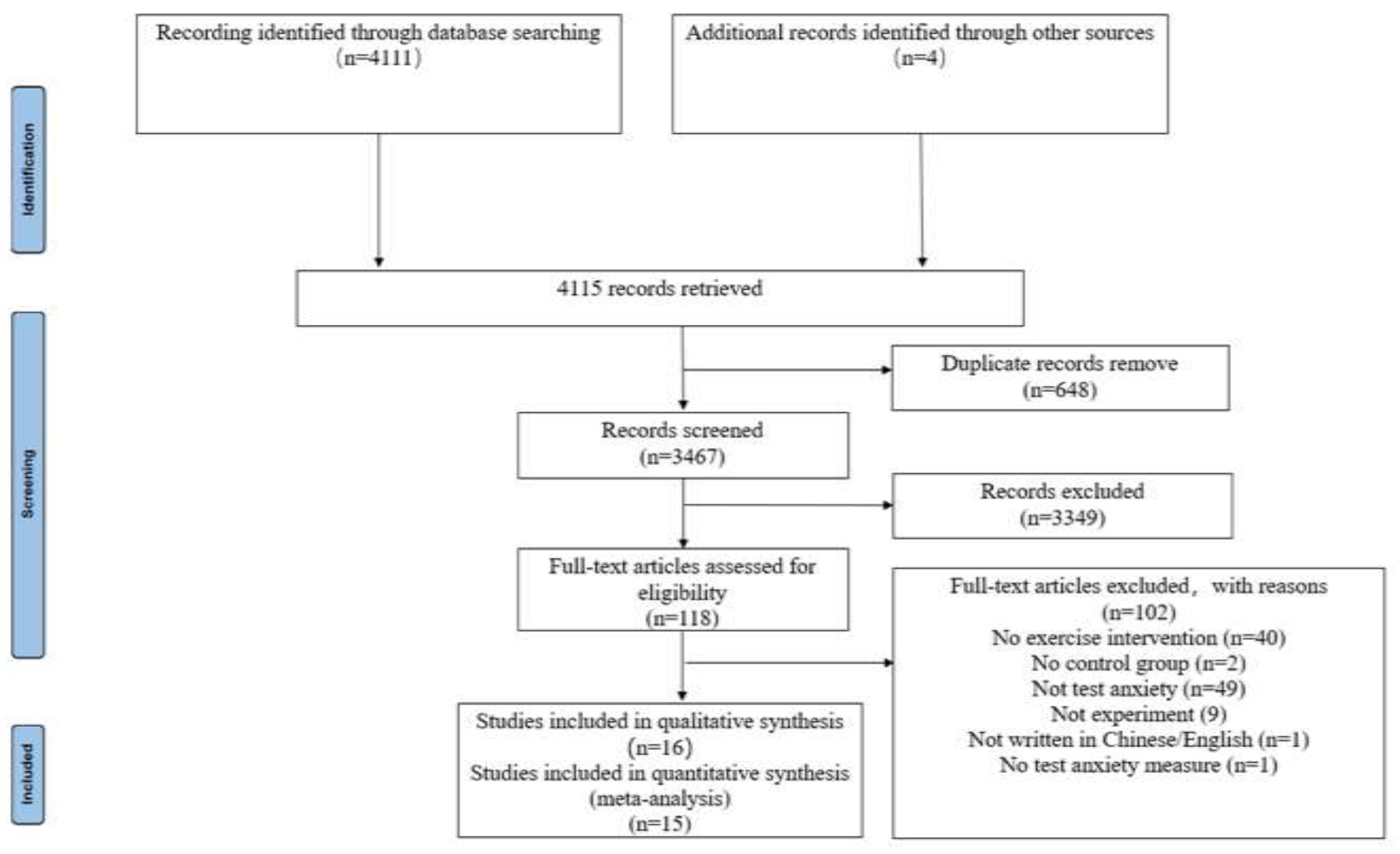
3.1. Selection Outcomes
3.2. The Basic Characteristics of Included Studies
3.2.1. Country
3.2.2. Study Sample
3.2.3. Measurement of Study Results
3.2.4. Intervention Characteristics
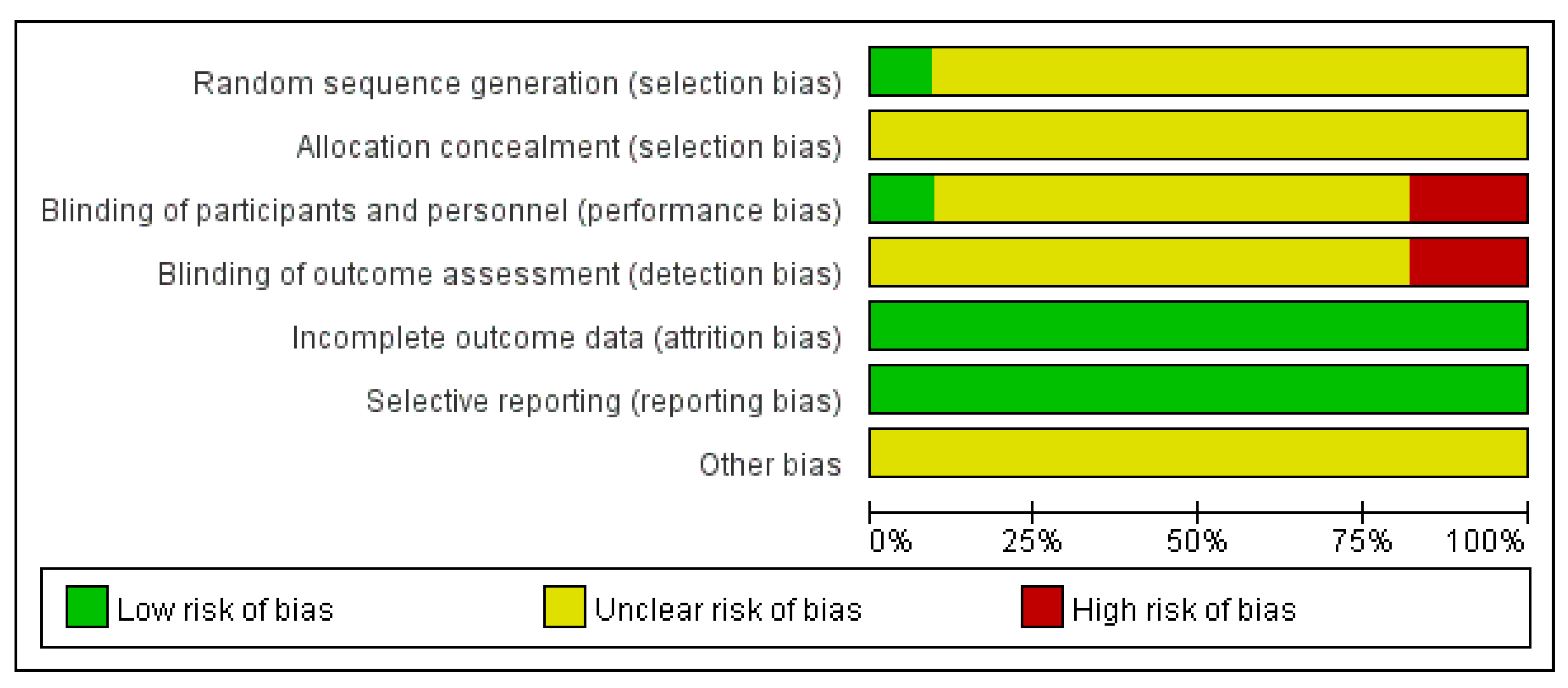
3.3. Assessment of the Risks of Study Bias
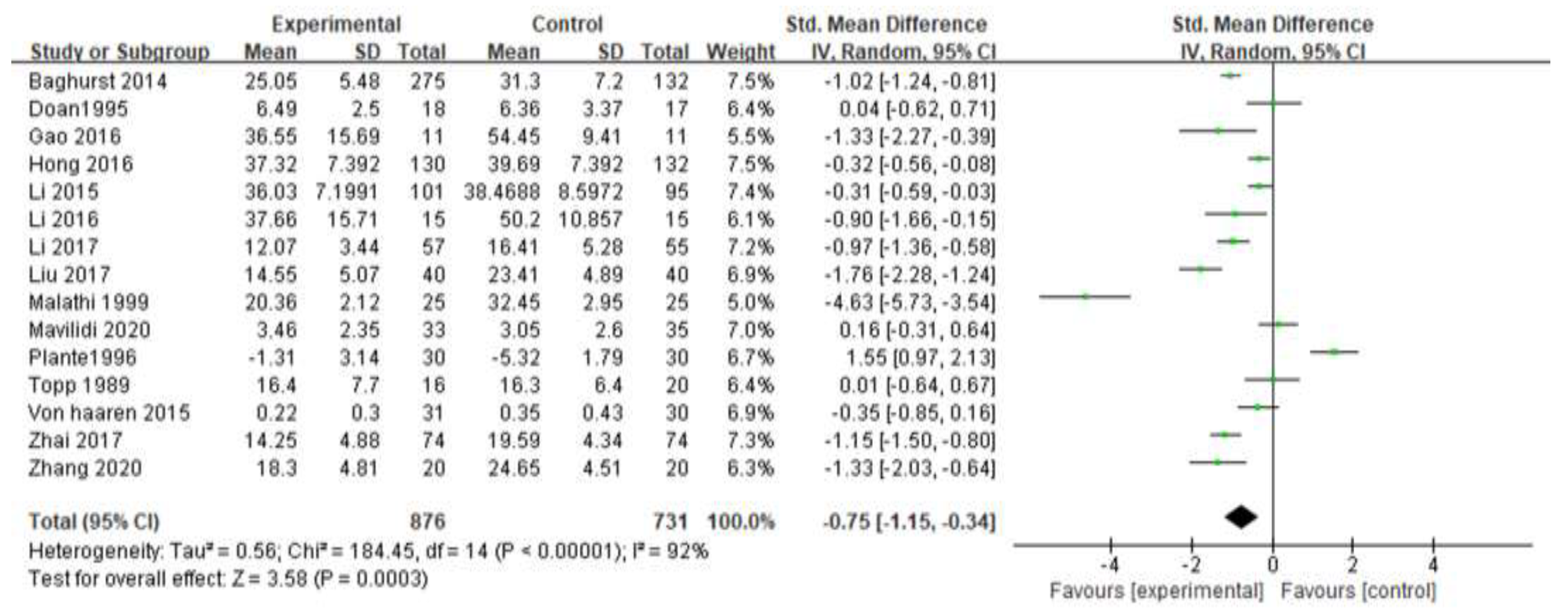
3.4. Impacts of Exercise Intervention on Students’ Test Anxiety
3.5. Subgroup Analysis
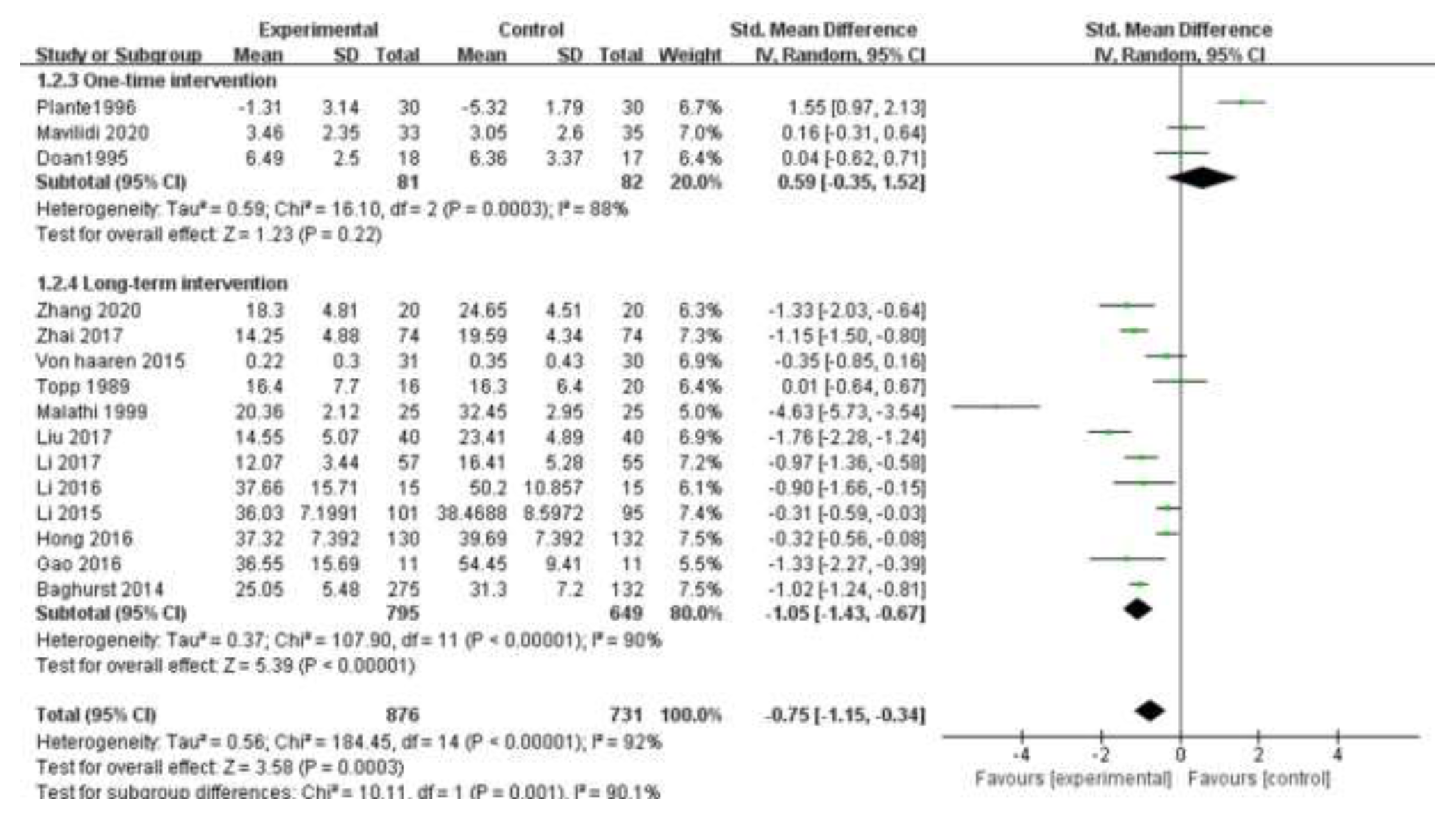
3.5.1. Intervention Time
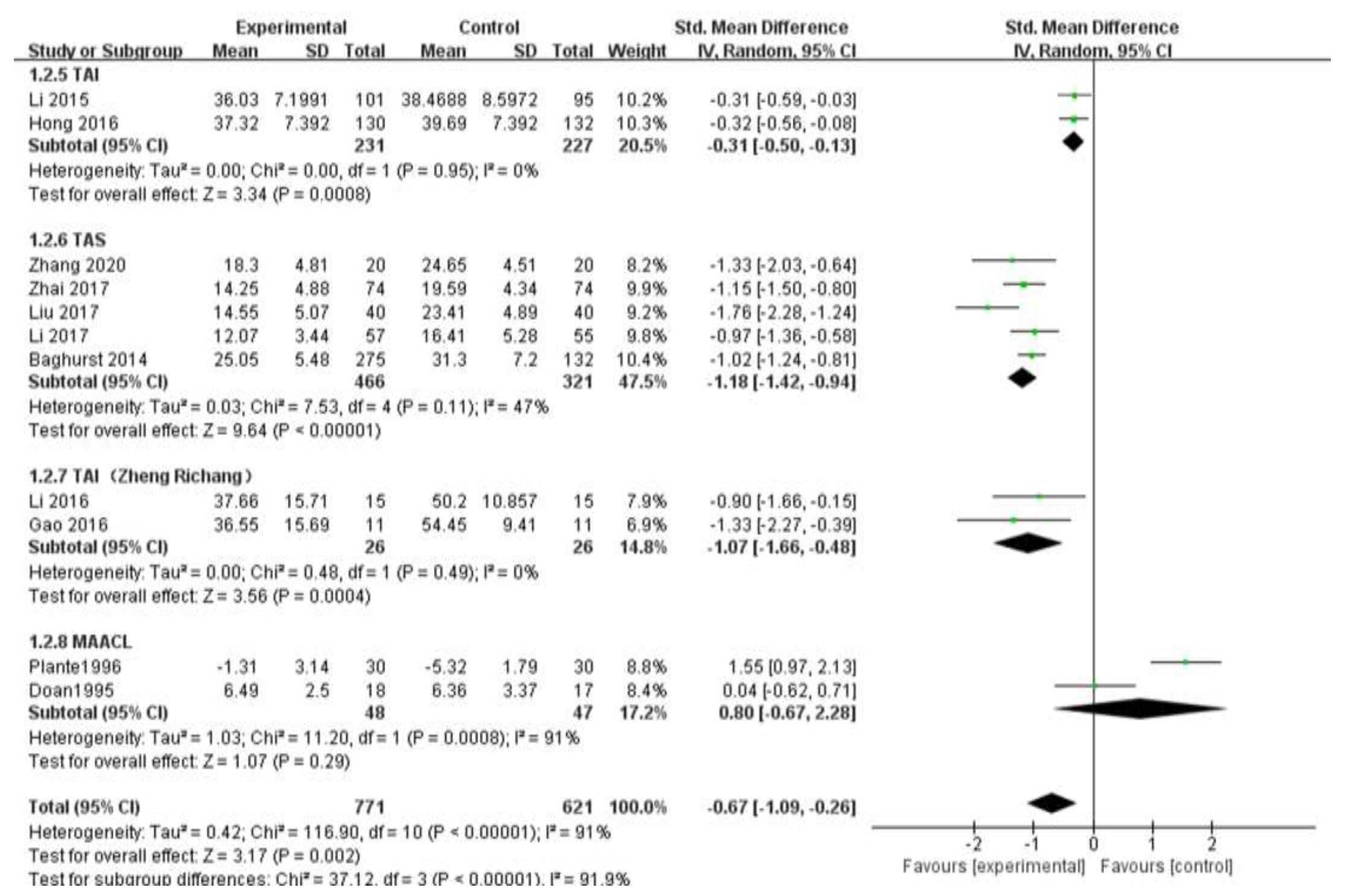
3.5.2. Measurement Scale
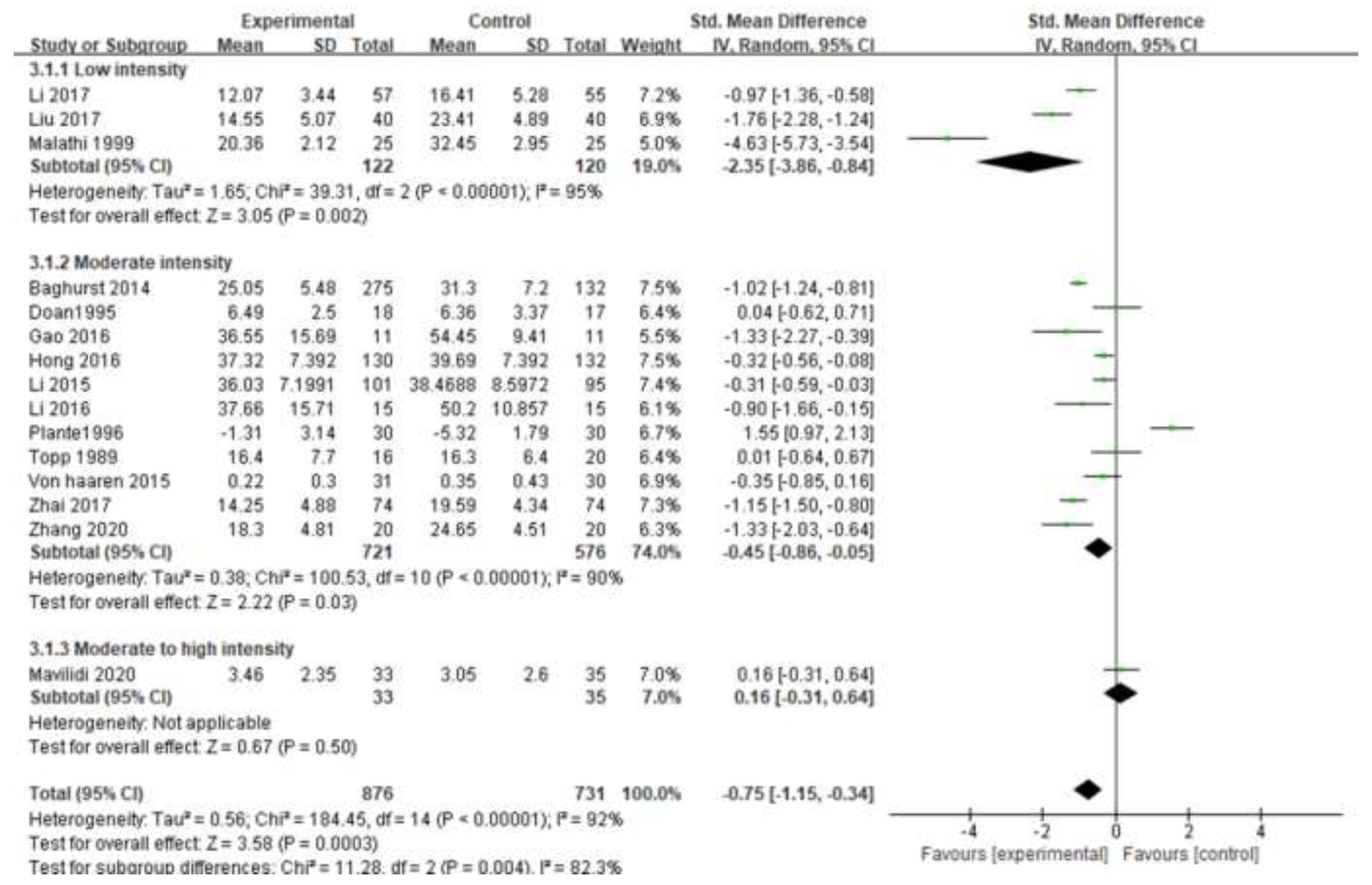
3.5.3. Exercise Intensity
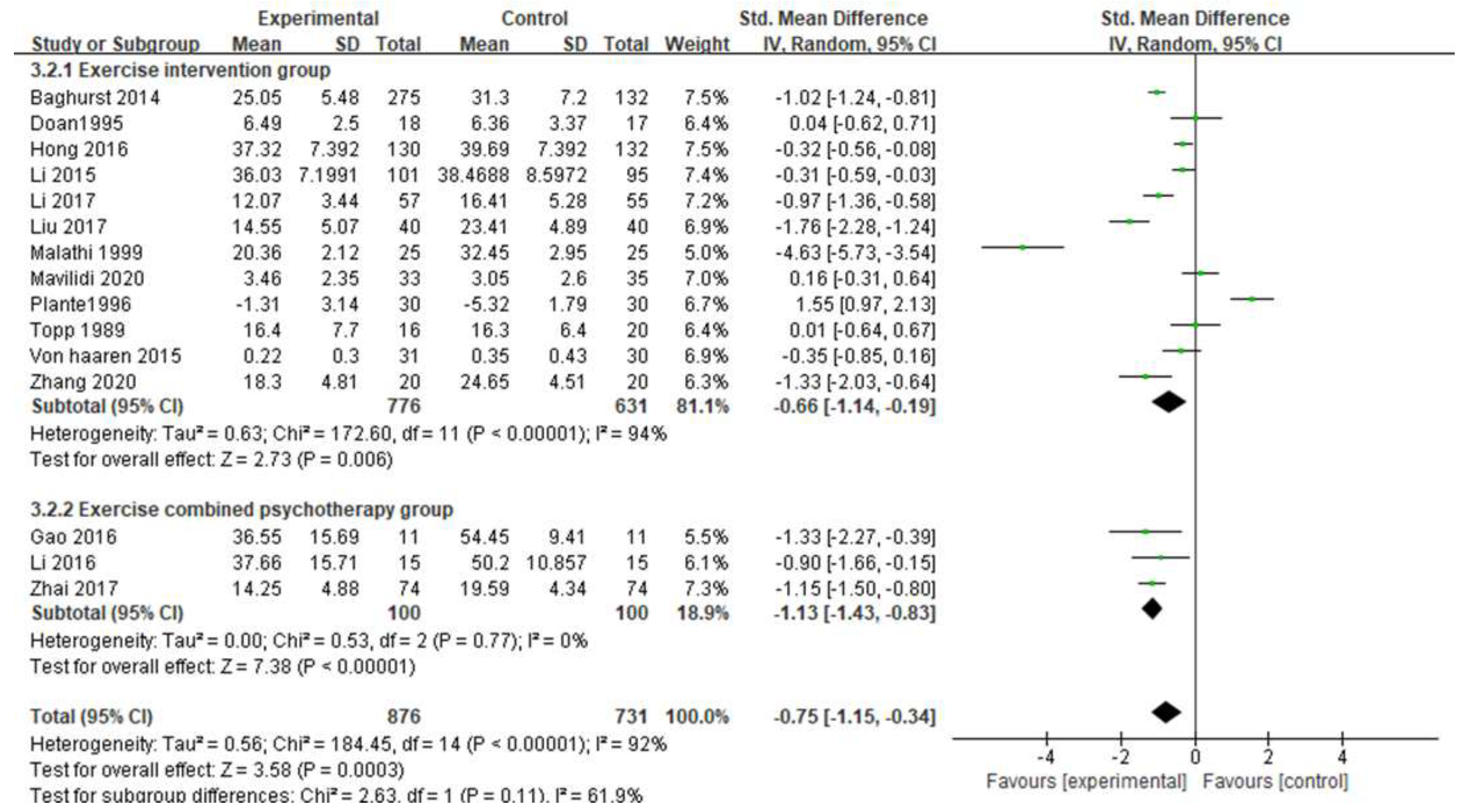
3.5.4. Intervention Method
3.5.5. Exercise Frequency
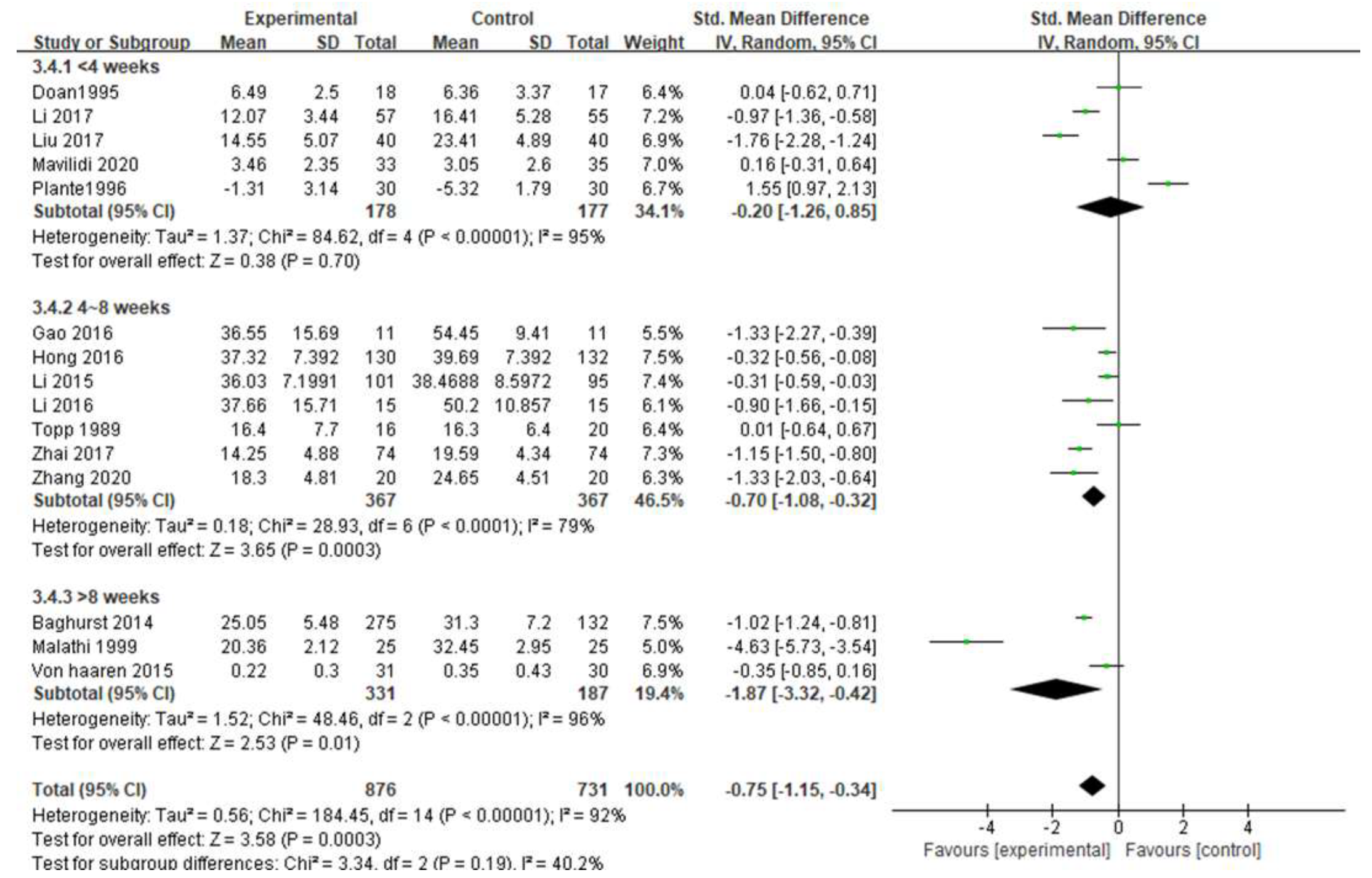
3.5.6. Intervention Period
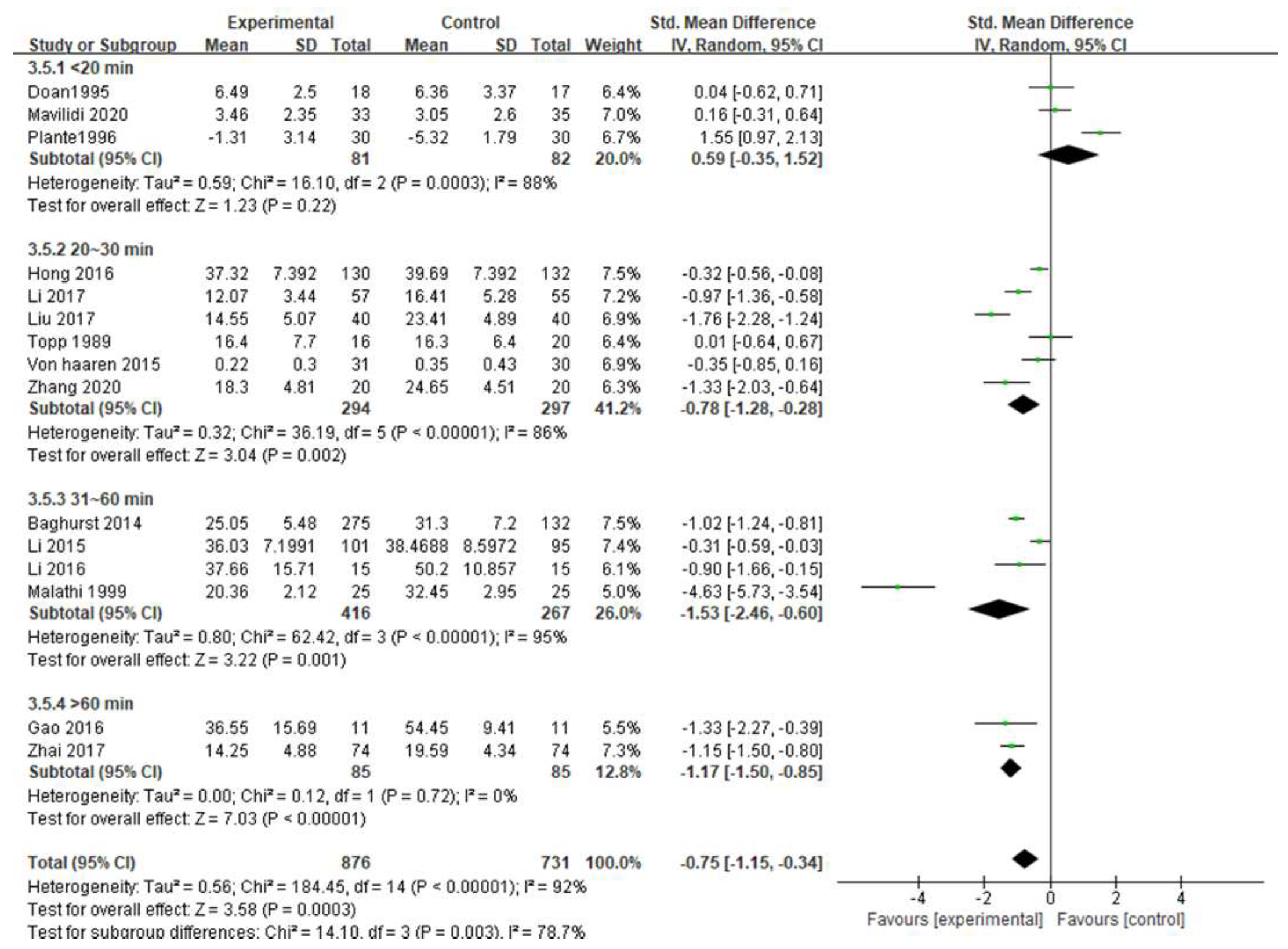
3.5.7. Exercise Duration
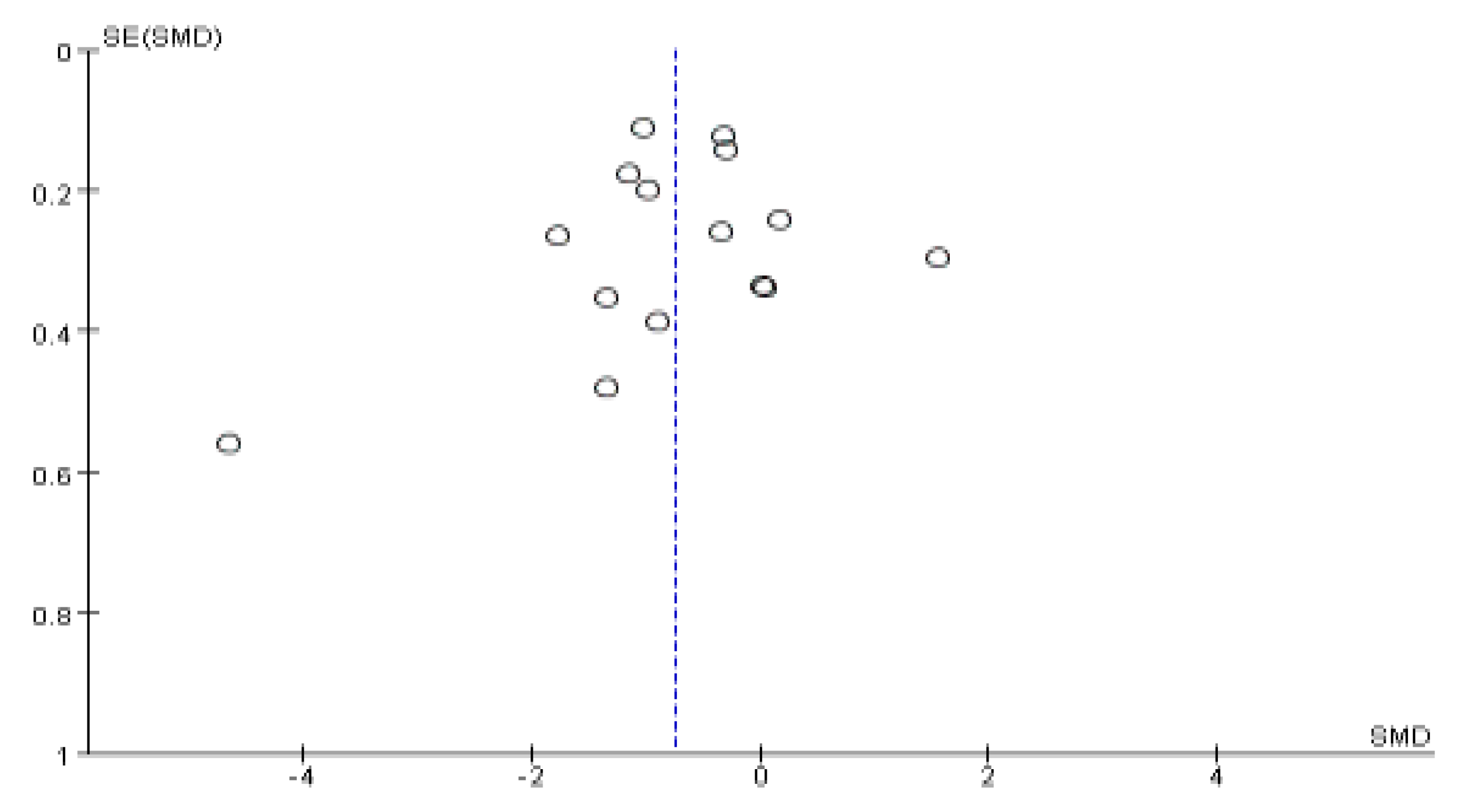
3.6. Publication Bias
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- He, M.; Huang, G.G.; Cao, R.; Ni, J.C. Investigation and analysis of 419 primary and middle school students’ examination anxiety. Chin. Med. Her. 2006, 28, 145. [Google Scholar]
- Zhao, H.F.; Li, Q. Investigation and analysis of 1297 primary and middle school students’ examination anxiety. Med. J. Chin. People’s Health 2007, 1079–1081. [Google Scholar]
- Yuan, F.; Li, Z.S.; Yang, Y.L.; Mu, Y. Prevalence of anxiety tested with Test Anxiety Scale (TAS) in senior three students: A Meta-analysis. Chin. J. Sch. Health 2018, 39, 1324–1328. [Google Scholar] [CrossRef]
- Mandler, G.; Sarason, S.B. A study of anxiety and learning. J. Abnorm. Psychol. 1952, 47, 166–173. [Google Scholar] [CrossRef]
- Zheng, R.C. Diagnosis and Treatment of Test Anxiety; Heilongjiang Science and Technology Press: Harbin, China, 1990. [Google Scholar]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Bauman, A.E. Updating the evidence that physical activity is good for health: An epidemiological review 2000–2003. J. Sci. Med. Sport 2004, 7, 6–19. [Google Scholar] [CrossRef]
- Blumenthal, J.A.; Babyak, M.A.; Doraiswamy, P.M.; Watkins, L.; Hoffman, B.M.; Barbour, K.A.; Herman, S.; Craighead, W.E.; Brosse, A.L.; Waugh, R.; et al. Exercise and pharmacotherapy in the treatment of major depressive disorder. Psychosom. Med. 2007, 69, 587–596. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 1985, 98. [Google Scholar] [CrossRef]
- Ergene, T. Effective interventions on test anxiety reduction-A meta-analysis. School Psychol. Int. 2003, 24, 313–328. [Google Scholar] [CrossRef]
- Huntley, C.D.; Young, B.; Jha, V.; Fisher, P.L. The efficacy of interventions for test anxiety in university students: A protocol for a systematic review and meta-analysis. Int. J. Educ. Res. 2016, 77, 92–98. [Google Scholar] [CrossRef] [Green Version]
- Il, L.S.; Bak, B. Meta-analysis Study of Test Anxiety on a Domestic and International level. Korean J. Educ. Psychol. 2013, 27, 529–553. [Google Scholar]
- Espinola, C.W.; Khoo, Y.; Parmar, R.; Demchenko, I.; Frey, B.N.; Milev, R.V.; Ravindran, A.V.; Parikh, S.V.; Ho, K.; Rotzinger, S.; et al. Pretreatment anxious depression as a predictor of side effect frequency and severity in escitalopram and aripiprazole adjunctive therapy. Brain Behav. 2022, 12, e2555. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Li, T.; Deeks, J.J. Chapter 6: Choosing effect measures and computing estimates of effect. In Cochrane Handbook for Systematic Reviews of Interventions; Version 6.2; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Updated February 2021; Cochrane: London, UK, 2021; Available online: www.training.cochrane.org/handbook (accessed on 28 February 2022).
- Mavilidi, M.F.; Ouwehand, K.; Riley, N.; Chandler, P.; Paas, F. Effects of an Acute Physical Activity Break on Test Anxiety and Math Test Performance. Int. J. Environ. Res. Public Health 2020, 17, 1523. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Li, P. Alleviating effect of Taijiquan practice on high school students’ examination tension syndrome. Contemp. Sports Technol. 2017, 7, 179–181. [Google Scholar]
- Zhai, W.; Ma, M.K.; Abulizi, M. Analysis of the intervention effect of sand table game combined with physical exercise on Uyghur Examination anxiety students in Vocational Colleges. Chin. J. Sch. Health 2017, 38, 1080–1083. [Google Scholar]
- Liu, C.; Wang, Y. The Regulation of the Stress State by Shadow Boxing on Qi Depression Student during Date of Examination. Sichuan Sports Sci. 2017, 36, 62–64. [Google Scholar]
- Thompson, H.R.; Duvall, J.; Padrez, R.; Rosekrans, N.; Madsen, K.A. The impact of moderate-vigorous intensity physical education class immediately prior to standardized testing on student test-taking behaviors. Ment. Health Phys. Act. 2016, 11, 7–12. [Google Scholar] [CrossRef]
- Gao, L. Compilation of “Physical Activity Combined with Test Anxiety Group Counseling Manual” and Its preliminary Application; Yunnan Normal University: Kunming, China, 2016. [Google Scholar]
- Li, H. Compilation and Application of “Emotion Center Therapy Combined with Sports Game Group Auxiliary Manual”—A Study on Test Anxiety Based on Physiological Arousal; Yunnan Normal University: Kunming, China, 2016. [Google Scholar]
- Li, K.W.; Liu, P.; Shi, F. The Intervention of Aerobic Exercise to Middle School Students’ Anxiety over Test. J. Wenshan Univ. 2015, 28, 83–85. [Google Scholar]
- von Haaren, B.; Haertel, S.; Stumpp, J.; Hey, S.; Ebner-Priemer, U. Reduced emotional stress reactivity to a real-life academic examination stressor in students participating in a 20-week aerobic exercise training: A randomised controlled trial using Ambulatory Assessment. Psychol. Sport Exerc. 2015, 20, 67–75. [Google Scholar] [CrossRef]
- Malathi, A.; Damodaran, A. Stress due to exams in medical students—Role of yoga. Indian J. Physiol. Pharmacol. 1999, 43, 218–224. [Google Scholar] [PubMed]
- Plante, T.G.; Marcotte, D.; Manuel, G.; Willemsen, E. The influence of brief episodes of aerobic exercise activity, soothing mu-sic-nature scenes condition, and suggestion on coping with test-taking anxiety. Int. J. Stress Manag. 1996, 3, 155–166. [Google Scholar] [CrossRef]
- Doan, B.; Plante, T.G.; Digregorio, M.P.; Manuel, G.M. Influence of aerobic exercise activity and relaxation training on coping with test-taking anxiety. Anxiety Stress Coping 1995, 8, 101–111. [Google Scholar] [CrossRef]
- Zhang, F.; Zhang, Q. A Study on the intervention of Sports games on test anxiety of Senior Three Students. Zhongxiaoxue Xinli Jiankang Jiaoyu 2020, 18–22. [Google Scholar] [CrossRef]
- Hong, J.J. An Empirical Study on the Aerobic Exercise to Alleviate the Test Anxiety of Middle School Students—Taking a High School in Shuangliu County as an Example; Sichuan Normal University: Chengdu, China, 2016. [Google Scholar]
- Baghurst, T.; Kelley, B.C. An Examination of Stress in College Students over the Course of a Semester. Health Promot. Pract. 2014, 15, 438–447. [Google Scholar] [CrossRef]
- Topp, R. Effect of relaxation or exercise on undergraduates’ test anxiety. Percept. Motor Skill 1989, 69, 35–41. [Google Scholar] [CrossRef]
- Thayer, R.E. Energy, tiredness, and tension effects of a sugar snack versus moderate exercise. J. Personal. Soc. Psychol. 1987, 52, 119–125. [Google Scholar] [CrossRef]
- Petruzzello, S.J.; Landers, D.M.; Hatfield, B.D.; Kubitz, K.A.; Salazar, W. A meta-analysis on the anxiety-reducing effects of acute and chronic exercise. Outcomes and mechanisms. Sports Med. 1991, 11, 143–182. [Google Scholar] [CrossRef]
- Haakstad, L.; Torset, B.; Bo, K. What is the effect of regular group exercise on maternal psychological outcomes and common pregnancy complaints? An assessor blinded RCT. Midwifery 2016, 32, 81–86. [Google Scholar] [CrossRef]
- Zhao, Y.X.; Hao, Y.H.; Jing, X.Z. Smartphone addiction intervention through sports combining with group psychological training among college students. Chin. J. Sch. Health 2021, 42, 556–559. [Google Scholar]
- Mao, D.H. The effect of basketball and group psychological counseling on the interpersonal competence of college students. Chin. J. Sch. Health 2017, 38, 1088–1091. [Google Scholar]
- Tsai, S.P.; Baun, W.B.; Bernacki, E.J. Relationship of employee turnover to exercise adherence in a corporate fitness program. J. Occup. Environ. Med. 1987, 29, 572–575. [Google Scholar]
- Philippot, A.; Dubois, V.; Lambrechts, K.; Grogna, D.; Robert, A.; Jonckheer, U.; Chakib, W.; Beine, A.; Bleyenheuft, Y.; De Volder, A.G. Impact of physical exercise on depression and anxiety in adolescent inpatients: A randomized controlled trial. J. Affect Disord. 2022, 301, 145–153. [Google Scholar] [CrossRef]
- Huang, J.F.; Wang, D.D.; Wang, J.H. Clinical Evidence of Tai Chi Exercise Prescriptions: A Systematic Review. Evid.-Based Complementary Altern. Med. 2021, 2021, 5558805. [Google Scholar] [CrossRef]
- Zhu, Z.H. The Intervention Effect of Sports Exercise on the Self-Esteem and Anxiety of College Students; Huazhong Normal University: Wuhan, China, 2021. [Google Scholar]
- He, C. Meta-analysis of the Effects of Exercise Intervention on College Students’ Anxiety. Sichuan Sports Sci. 2022, 41, 50–55. [Google Scholar]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef] [Green Version]
- Morgan, W.P.; Costill, D.L.; Flynn, M.G.; Raglin, J.S.; O’Connor, P.J. Mood disturbance following increased training in swimmers. Med. Sci. Sports Exerc. 1988, 20, 408–414. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| #1 | Population | Students OR Primary school students OR middle school students OR high school students OR college students OR adolescent OR Student OR School Enrollment OR Enrollment, School OR Enrollments, School OR School Enrollments |
| #2 | Intervention | Exercise OR Sports OR Exercises OR Physical Activity OR Activities, Physical OR Activity, Physical OR Physical Activities OR Exercise, Physical OR Exercises, Physical OR Physical Exercise OR Physical Exercises OR Acute Exercise OR Acute Exercises OR Exercise, Acute OR Exercises, Acute OR Exercise, Isometric OR Exercises, Isometric OR Isometric Exercises OR Isometric Exercise OR Exercise, Aerobic OR Aerobic Exercise OR Aerobic Exercises OR Exercises, Aerobic OR Exercise Training OR Exercise Trainings OR Training, Exercise OR Trainings, Exercise OR Physical Education and Training OR Physical Education, Training OR Physical Education OR Education, Physical |
| #3 | Outcomes | Test Anxiety OR Anxiety, Test OR Exam Anxiety OR Anxiety, Exam OR Exam Stress OR Stress, Exam OR Pre-Exam Anxiety OR Anxiety, Pre-Exam OR Pre Exam Anxiety OR Test fear |
| #4 | #1 AND #2 AND #3 | |
| Authors (Year)/Country | Study Type | Sample Size | Intervention Program | Exercise Intensity | Dosage of Intervention (Time; Frequency; Duration) | Measuring Tools | Follow-Up | ||
|---|---|---|---|---|---|---|---|---|---|
| Intervention Group | Control Group | Intervention Group | Control Group | ||||||
| Mavilidi et al. (2020) /Australia [17] | RCT | 33 | 35 | Physical fitness | Word game | Medium and high intensity | 10 min | Likert Scale (1–9) | No follow-up |
| Zhang and Zhang (2020)/China [29] | Non-RCT | 20 | 20 | Sports games | Blank | Predicted moderate intensity | 20 min; 2/week; 7 weeks | TAS | No follow-up |
| Li and Li (2017)/China [18] | RCT | 57 | 55 | Tai chi | Blank | Predicted low intensity | 30 min; 2/week; 2 weeks | TAS | No follow-up |
| Zhai et al. (2017)/China [19] | RCT | 74 | 74 | Sand tray combined with physical exercise | Blank | Moderate intensity | Sand: 120 min; 1/week PE: 70 min; 1/week; 8 weeks | TAS | 3 months |
| Liu and Wang (2017)/China [20] | RCT | 40 | 40 | Tai chi | Blank | Predicted low intensity | 30 min/day; 5 days | TAS | No follow-up |
| Thompson et al. (2016)/USA [21] | Cluster-RCT | 359 | 432 | PE lesson | Blank | Medium and high intensity | 40 min | CTAS | No follow-up |
| Gao (2016)/ China [22] | RCT | 11 | 11 | Psychotherapy combined with physical exercise | Blank | Predicted moderate intensity | Psychotherapy: 80 min; 1/week PE: 20 min; 1/week 8 weeks | TAI | No follow-up |
| Li (2016)/ China [23] | RCT | 15 | 15 | Emotional therapy combined with sports games | Blank | Predicted medium and low intensity | Emotional therapy: 60 min; 1/week Sports games: 15–20 min; 1/week 8 weeks | TAI | No follow-up |
| Hong (2016)/China [30] | Non-RCT | 130 | 132 | Aerobic exercise | Blank | Predicted moderate intensity | 30 min; 2/week; 2 months | TAI | No follow-up |
| Li et al. (2015)/China [24] | RCT | 101 | 95 | Jogging, sports games | Blank | Moderate intensity | 30~40 min; 2~3/week; 1 month | TAI | No follow-up |
| von Haaren et al. (2015)/Germany [25] | RCT | 31 | 30 | Aerobic running | Blank | Predicted moderate intensity | 30 min; 2/week; 20 weeks | NA | No follow-up |
| Baghurst and Kelley (2014)/USA [31] | Non-RCT | CV: 131 PA: 144 | C: 132 SM:124 | CV: Aerobic or anaerobic fitness PA: Ball game | C: Blank SM: Stress management | Predicted medium and high intensity | 50 min; 3/week; 16 weeks | TAS | No follow-up |
| Malathi and Damodaran (1999)/India [26] | RCT | 25 | 25 | Yoga | Reading writing | Predicted low intensity | 60 min; 3/week; 3 months | STAI | No follow-up |
| Plante et al. (1996)/USA [27] | RCT | 30 | 30 | Aerobic exercise | Watch videos | Predicted moderate intensity | 15 min | TASC MAACL | No follow-up |
| Doan et al. (1995) /USA [28] | RCT | 1.18 2.17 | 17 | 1. Cycling 2. Relaxation exercise | Reading magazines | Moderate intensity | 15 min | TASC MAACL | No follow-up |
| Topp (1989) /USA [32] | Non-RCT | 1.16 2.9 | 20 | 1. Aerobic dance 2. Relax group | Blank | Medium and high intensity | 30 min; 3/week; 7 weeks | TAQ | No follow-up |
| Item | Hong, 2016 | Zhang and Zhang, 2020 | Topp, 1989 | Baghurst and Kelley, 2014 |
|---|---|---|---|---|
| A clearly stated aim | 2 | 2 | 2 | 2 |
| Inclusion of consecutive patients | 2 | 2 | 2 | 2 |
| Prospective collection of data | 2 | 2 | 2 | 2 |
| Endpoints appropriate to the aim of the study | 2 | 2 | 2 | 2 |
| Unbiased assessment of the study endpoint | 0 | 1 | 1 | 1 |
| Follow-up period appropriate to the aim of the study | 0 | 0 | 0 | 0 |
| Loss to follow up less than 5% | 0 | 0 | 0 | 0 |
| Prospective calculation of the study size | 0 | 0 | 0 | 0 |
| Additional criteria in the case of comparative studies | ||||
| An adequate control group | 2 | 2 | 2 | 2 |
| Contemporary groups | 2 | 2 | 2 | 2 |
| Baseline equivalence of groups | 2 | 2 | 2 | 2 |
| Adequate statistical analyses | 2 | 2 | 2 | 2 |
| Final score | 16 | 17 | 17 | 17 |
| Maximum score | 24 | 24 | 24 | 24 |
| Moderator | Category | Number of Studies | SMD | CI | I2 | Heterogeneity p |
|---|---|---|---|---|---|---|
| Intervention time | One-time | 3 | 0.59 | −0.35, 1.52 | 88% | 0.0003 |
| Long-time | 12 | −1.05 ** | −1.43, −0.67 | 90% | <0.00001 | |
| Measurement scale | TAQ | 1 | 0.01 | −0.64, 0.67 | / | / |
| NA | 1 | −0.35 | −0.85, 0.16 | / | / | |
| Likert Scale | 1 | 0.16 | −0.31, 0.64 | / | / | |
| STAI | 1 | −4.63 | −5.73, −3.54 | / | / | |
| TAI | 2 | −0.31 ** | −0.50, −0.13 | 0% | 0.95 | |
| TAS | 5 | −1.18 ** | −1.42, −0.94 | 47% | 0.11 | |
| TAS(Zheng) | 2 | −1.07 ** | −1.66, −0.48 | 0% | 0.49 | |
| MAACL | 2 | 0.80 | −0.67, 2.28 | 91% | 0.0008 | |
| Exercise intensity | Low intensity | 3 | −2.35 ** | −3.86, −0.84 | 95% | <0.00001 |
| Medium intensity | 11 | −0.45 * | −0.86, −0.05 | 90% | <0.00001 | |
| Medium to high intensity | 1 | 0.16 | −0.31, 0.64 | / | / | |
| Intervention method | Exercise | 12 | −0.66 ** | −1.14, −0.19 | 94% | <0.00001 |
| Exercise combined with psychology | 3 | −1.13 ** | −1.43, −0.83 | 0% | 0.77 | |
| Exercise frequency | 1/week | 6 | −0.25 | −1.15, 0.64 | 93% | <0.00001 |
| 2–3/week | 7 | −0.96 ** | −1.50, −0.41 | 93% | <0.00001 | |
| ˃3/week | 2 | −1.35 ** | −2.12, −0.57 | 82% | 0.02 | |
| Intervention period | <4 weeks | 5 | −0.20 | −1.26, 0.85 | 95% | <0.00001 |
| 4–8 weeks | 7 | −0.70 ** | −1.08, −0.32 | 79% | <0.0001 | |
| ˃8 weeks | 3 | −1.87 * | −3.32, −0.42 | 96% | <0.00001 | |
| Exercise duration | <20 min | 3 | 0.59 | −0.35, 1.52 | 88% | 0.0003 |
| 20–30 min | 6 | −0.78 ** | −1.28, −0.28 | 86% | <0.00001 | |
| 31–60 min | 4 | −1.53 ** | −2.46, −0.60 | 95% | <0.00001 | |
| ˃60 min | 2 | −1.17 ** | −1.50, −0.85 | 0% | 0.72 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Li, W.; Wang, J. Effects of Exercise Intervention on Students’ Test Anxiety: A Systematic Review with a Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6709. https://doi.org/10.3390/ijerph19116709
Zhang X, Li W, Wang J. Effects of Exercise Intervention on Students’ Test Anxiety: A Systematic Review with a Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(11):6709. https://doi.org/10.3390/ijerph19116709
Chicago/Turabian StyleZhang, Xueyan, Wenhao Li, and Jinghao Wang. 2022. "Effects of Exercise Intervention on Students’ Test Anxiety: A Systematic Review with a Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 11: 6709. https://doi.org/10.3390/ijerph19116709