
The Impact of Self-Employment on the Health of Migrant Workers: Evidence from China Migrants Dynamic Survey

Abstract
:1. Introduction
2. Theoretical Analysis and Hypotheses
2.1. Direct Impact of Self-Employment on the Health of Migrant Workers
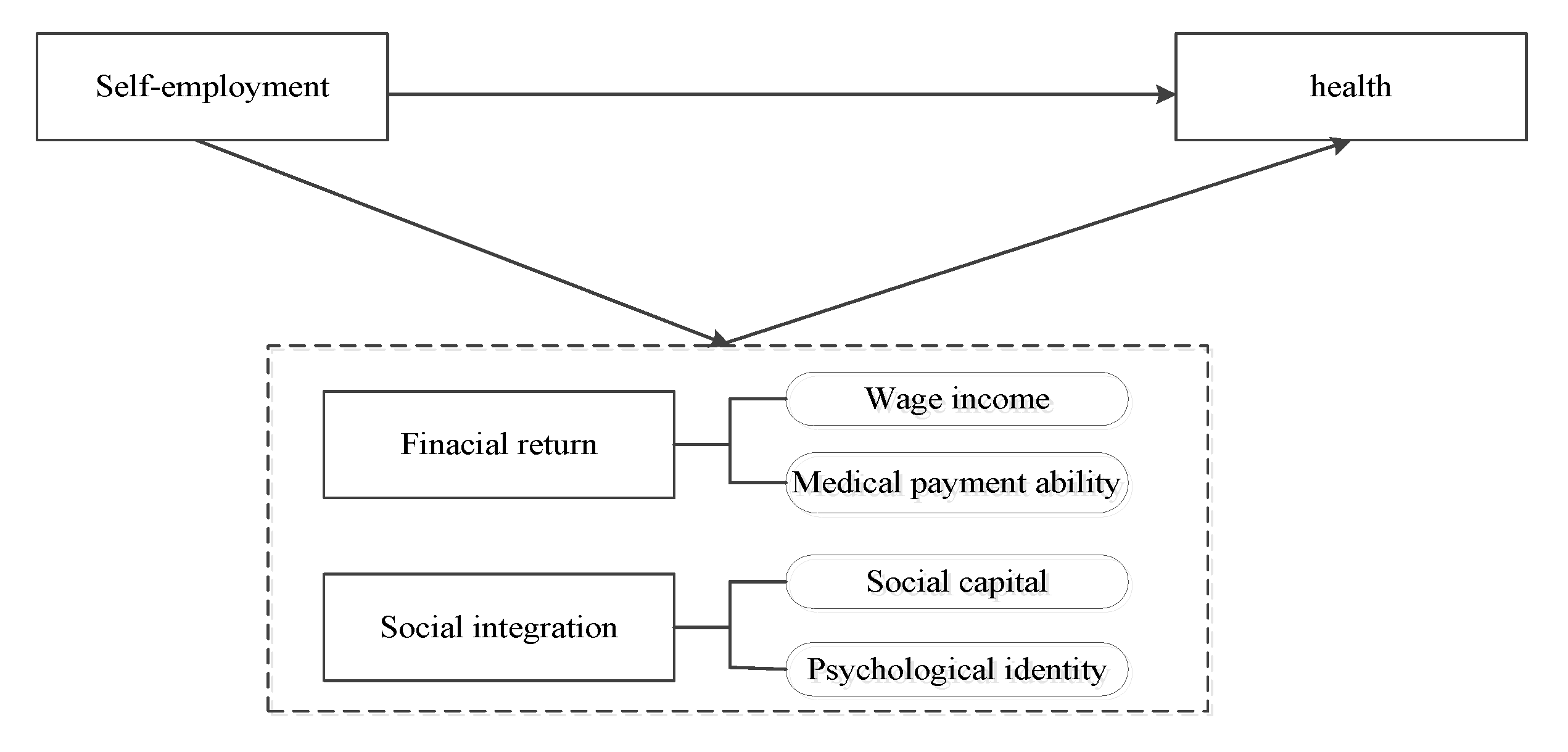
2.2. Indirect Impact of Self-Employment on the Health of Migrant Workers
3. Materials and Methods
3.1. Data Sources
3.2. Variable Definition
3.2.1. Explained Variables
3.2.2. Explanatory Variables
3.2.3. Other Variables
3.3. Methods
4. Results
4.1. Descriptive Results
- (1)
- In the whole sample, about 42.43% of migrant workers engaged in self-employment had the group characteristics of higher age, higher proportion of male and Han nationality, and lower education level compared with wage workers. Specifically, the average age of the self-employed was-37.939 years, about 3.5 years significantly older than that of wage workers. Below the age of 35, there were more wage workers, while after the age of 35, the situation changed and the proportion of self-employed migrant workers gradually exceeded that of wage workers. In fact, this distribution characteristic is consistent with reality: on the one hand, workers tend to choose to be employed when they are young to accumulate more human and monetary capital, and then turn to being self-employed when they are middle-aged. On the other hand, the greater family support pressures faced by migrant workers in their middle age may also motivate or force individuals to engage in self-employment activities. The proportion of male migrant workers who were self-employed was roughly 1.3 percentage points larger than that of female, and the proportion of Han nationality migrant workers who were self-employed was over 90%. The average educational attainment of self-employed was 9.258 years, while the wage for workers was 10.205.
- (2)
- In terms of work characteristics, the average monthly income of self-employed was CNY 1359.80 higher than that of wage workers, but at the same time, the self-employed worked 11 h more per week. This suggests that migrant workers are self-employed out of economic rationality, but higher income is accompanied by more working hours. In addition, self-employed migrant workers accounted for a higher proportion of urban employees’ medical insurance and health records.
- (3)
- Moreover, in terms of regional characteristics, the proportion of self-employed migrant workers in the central and western regions was significantly higher than that in the eastern and northeastern regions. It shows that the areas with a relatively inactive economy are likely to increase the proportion of self-employment. A total of 75.3% of self-employed migrant workers were mainly concentrated in the living service industry, while the secondary and productive service industries accounted for 21.3% and 3.4%, respectively.
- (4)
- The mean value of health of the self-employed was 3.823, indicating that the self-employed migrant workers health is above the average level, which was lower than that of wage workers. At the same time, compared to employed migrant workers, self-employed migrant workers were significantly more represented in non-manual labor industries, had significantly fewer difficulties with job instability, and had significantly higher wages, social capital, and psychological identity than employed migrant workers. However, there were no significant difference between the two groups in terms of time flexibility and medical payment ability.
4.2. Empirical Results
4.2.1. Influence of Self-Employment on Health
4.2.2. Influence of Heterogeneous Forms of Self-Employment on Health
4.2.3. Influence of Self-Employment on Health by Gender and Nationality
4.3. Mechanism Analysis
4.3.1. Direct Mechanism Analysis
4.3.2. Indirect Mechanism Analysis
5. Discussion
- We selected the cross-sectional data of the 2017 CMDS as the research sample for this paper. However, the influence of self-employment on migrant workers health is a dynamic process. Thus, future research could use panel data to further expand and verify the relationship in greater detail.
- Studying the relationship between self-employment and health also involves many missing variables, such as previous unhealthy habits, illness, original industry choices, risk appetite and perseverance, and even genes [73,74]; if these variables can be controlled, the processing effect will be cleaner, but it falls outside the scope of this paper to discuss them due to the availability of data and samples.
- The choice of instrumental variables can be further deliberated on. Previous studies have used the number of self-employed members in the household, immigration variable status, and the presence of insurance for children as instrumental variables [37], but the above data were not collected in the database we selected. The regional registered unemployment rates can also be used [28], but the classical literature confirms that a 1% increase in the U.S. unemployment rate will reduce overall mortality by 0.5% [75]. Therefore, based on data availability and “relative safety”, this paper only constructs a higher latitude district-level self-employment rate as an instrumental variable, which is, of course, a less than perfect and skillful approach.
6. Conclusions and Implications
- (1)
- The health status of self-employed migrant workers is better than that of wage workers, and this relationship is more pronounced after the introduction of instrumental variables, indicating that self-employed migrant workers experience more health benefits; the conclusions are still robust after replacing health indicators in the analysis model.
- (2)
- Most self-employed migrant workers in China are still necessity self-employed (35.40% of the total self-employed sample) and compared with wage workers, opportunity self-employment and necessity self-employment both have a significant positive effect on health, but opportunity self-employment has a higher effect on self-rated health and a lower effect on the likelihood of sickness and the morbidity rate.
- (3)
- Self-employed women are free from labor market discrimination and constraints, but the health effects of self-employment are not yet evident for ethnic minorities.
- (4)
- Self-employment not only directly promotes the health of migrant workers through less physical labor, more flexible time, and more stable nature of work, but also indirectly promotes the health of migrant workers through economic return and social integration.
- (1)
- Health should be taken into account as an important objective in employment policy formulation, and a social security system should be established to match labor mobility, focusing on solving the problems of urban-rural “fragmentation” of basic social insurance, inadequate transfer connections, and high transfer costs so as to protect the health rights and interests of self-employed migrant workers.
- (2)
- Opportunistic self-employment can create more jobs and is an important source of economic vitality. Based on the fact that opportunity self-employment depends more on the optimization of external conditions, it is important to promote the improvement of the business environment, alleviate financial constraints, and provide training on business laws to relieve the work pressure of self-employed workers and improve their health level. For the necessity self-employment, we can provide more convenient services in terms of employment skills and job security to improve their health benefits.
- (3)
- The importance of social security subsidies for self-employed women, cultivating women’s entrepreneurship or entrepreneurial skills, and improving the childcare welfare system to eliminate the health gender disparity of self-employment should be emphasized. Employment support policies for ethnic minorities need to be further improved, such as strengthening vocational skills education and legislating against employment discrimination. In addition, it is necessary to improve the income of migrant workers through multiple channels, pay attention to the cultivation of migrant workers’ social ability, and enhance their psychological identity with urban integration.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Labour Organization (ILO). Pandemic Realities for Asia-Pacific’s 48 Million International Migrants. Available online: https://www.ilo.org/asia/media-centre/news/WCMS_793027/lang--en/index.htm (accessed on 19 May 2021).
- National Bureau of Statistics of China. Statistical Communiqué of the People’s Republic of China on the 2021 National Economic and Social Development. Available online: http://www.stats.gov.cn/xxgk/sjfb/zxfb2020/202202/t20220228_1827971.html (accessed on 28 February 2022).
- Gao, Q.; Yang, S.; Li, S. Labor contracts and social insurance participation among migrant workers in China. J. China Econ. Rev. 2012, 23, 1195–1205. [Google Scholar] [CrossRef]
- Wu, W.P.; Wang, H.S. As immigrant in metropolis: The analysis on housing condition of the floating population in Beijing and Shanghai. Sociol. Stud. 2002, 3, 92–110. [Google Scholar] [CrossRef]
- Wang, Y.P.; Wang, Y.; Wu, J. Housing migrant workers in rapidly urbanizing regions: A study of the Chinese model in Shenzhen. Hous. Stud. 2010, 25, 83–100. [Google Scholar] [CrossRef]
- Zhu, Y.; Chen, P.Y.; Zhao, W. Injured workers in China: Injustice, conflict and social unrest. Int. Labour Rev. 2014, 153, 635–647. [Google Scholar] [CrossRef]
- Zhang, Q. Occupational injury occurrence and related risk factors among Chinese migrant workers. Procedia Eng. 2012, 43, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Wing Chan, K.; Buckingham, W. Is China abolishing the hukou system? China Quart. 2008, 195, 582–606. [Google Scholar] [CrossRef] [Green Version]
- Guo, W.; Lu, J.Y.; Liu, L.P. Healthy China in an age of mobility: Socioeconomic status, health literacy, and health outcomes. Popul. J. 2022, 44, 691. [Google Scholar] [CrossRef]
- Karl, G.; Andrea, D. Health inequalities in the diverse world of self-Employment: A Swedish National cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 12301. [Google Scholar] [CrossRef]
- Oreopoulos, P.; von Wachter, T.; Heisz, A. The short- and long-term career effects of graduating in a recession. Am. Econ. J. Appl. Econ. 2012, 4, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Light, A. Job mobility and wage growth: Evidence from the NLSY79. J. Mon. Labor Rev. 2005, 128, 33–39. [Google Scholar]
- Smith, J.P. Healthy bodies and thick wallets: The dual relation between health and economic Status. J. Econ. Perspect. 1999, 13, 145–166. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.F.; Yang, M.J.; Song, Y.P. Self-employment and income of migrant workers: An empirical analysis based on propensity score. Chin. Rural Econ. 2013, 10, 30–52. [Google Scholar]
- Huang, Z.L. Can self employment increase farmers’ income. Issues Agric. Econ. 2017, 8, 40–47. [Google Scholar]
- Zhu, Z.S. Rural migrant’s self-employment choices and their returns: An empirical test based on the China Migrants Dynamic Survey in 2014. Popul. Econ. 2018, 5, 100–112. [Google Scholar] [CrossRef]
- Gustafsson, B.; Zhang, Y.D. Self-employment in rural China: Its development, chara cteristics, and relation to income. China World Econ. 2022, 30, 136–165. [Google Scholar] [CrossRef]
- Schneck, S. Self-employment as a source of income inequality. Eurasian Bus. Rev. 2019, 10, 45–64. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Z.K.; Leng, C.X. How does self-employment affect the citizenization of migrant workers: Evidence from the China Migrants Dynamic Survey. Nankai Econ. Stud. 2020, 5, 109–129. [Google Scholar] [CrossRef]
- Goncalves, J.; Martins, S.P. The Effect of Self-Employment on Health: Evidence from Longitudinal Social Security Data; IZA Discussion Paper No. 11305; Institute of Labor Economics (IZA): Bonn, Germany, 2018. [Google Scholar] [CrossRef]
- Goldsby, M.G.; Kuratko, D.F.; Bishop, J.W. Entrepreneurship and fitness: An examination of rigorous exercise and goal attainment among small business owners. J. Small Bus. Manag. 2010, 43, 78–92. [Google Scholar] [CrossRef]
- Shepherd, D.A.; Patzelt, H. Harsh evaluations of entrepreneurs who fail: The role of sexual orientation, use of environmentally friendly technologies, and observers’ perspective taking. J. Manage. Stud. 2014, 52, 253–284. [Google Scholar] [CrossRef]
- David, G.B. Self-Employment: More May Not Be Better; NBER Working Paper No. 10286; National Bureau of Economic Research (NBER): Cambridge, MA, USA, 2004. [Google Scholar] [CrossRef]
- Taris, T.W.; Geurts, S.A.E.; Schaufeli, W.B.; Blonk, R.W.B.; Lagerveld, S.E. All day and all of the night: The relative contribution of two dimensions of workaholism to well-being in self-employed workers. Work. Stress 2008, 22, 153–165. [Google Scholar] [CrossRef]
- Stephan, U.; Roesler, U. Health of entrepreneurs versus employees in a national representative sample. J. Occup. Organ. Psychol. 2010, 83, 717–738. [Google Scholar] [CrossRef]
- Hessels, J.; Rietveld, C.A.; Peter, V. Self-employment and work-related stress: The mediating role of job control and job demand. J. Bus. Ventur. 2017, 32, 178–196. [Google Scholar] [CrossRef]
- Anderson, P. Happiness and health: Well-being among the self-employed. J. Socio-Econ. 2008, 37, 213–216. [Google Scholar] [CrossRef]
- Cheng, M.W.; Zhang, Y.S. The impact of self-employment on residents’ health: Evidence from China Health and Nutrition Survey. J. Guangxi Univ. (Philos. Soc. Sci.) 2022, 44, 115–125. [Google Scholar] [CrossRef]
- Ding, S.L.; Liu, C.H. The impact of informal employment on residents’ health: Experience from China Labor-force Dynamic Survey. J. China Inst. Ind. Relat. 2016, 30, 45–55. [Google Scholar]
- Zhou, C.; Bai, B. Can self-employment promote or restrain the consumption of rural migrants? J. Agrotech. Econ. 2020, 6, 103–115. [Google Scholar] [CrossRef]
- Karasek, R.A. Job demands, job decision latitude, and mental strain: Implications for job redesign. Admin. Sci. Quart. 1979, 24, 285. [Google Scholar] [CrossRef]
- Theorell, T.; Karasek, R.A. Current issues relating to psychosocial job strain and cardiovascular disease research. J. Occup. Health Psychol. 1996, 1, 9–26. [Google Scholar] [CrossRef]
- Hundley, G. Why and when are the self-employed more satisfied with their work? Ind. Relat. 2001, 40, 293–316. [Google Scholar] [CrossRef]
- Hyytinen, A.; Ilmakunnas, P.; Toivanen, O. The return-to-entrepreneurship puzzle. Labour Econ. 2013, 20, 57–67. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, B.H. Does entrepreneurship pay? An empirical analysis of the returns to self-employment. J. Political Econ. 2000, 108, 604–631. [Google Scholar] [CrossRef] [Green Version]
- Hoffer, A.; Gvillo, R.; Shughart, W.; Thomas, M. Income-expenditure elasticities of less-healthy consumption goods. J. Entrep. Public Policy 2017, 6, 127–148. [Google Scholar] [CrossRef]
- Yoon, J.; Bernell, S.L. The effect of self-employment on health, access to care, and health behavior. Health 2013, 12, 2116–2127. [Google Scholar] [CrossRef] [Green Version]
- Zou, Y.C.; Ao, D. A study on the difference of social capital between self-employed and employed. Sociol. Stud. 2011, 26, 198–224. [Google Scholar] [CrossRef]
- Wang, W.B.; Zhao, Y.D. An analysis of self-employers’ social networks. Society 2012, 32, 78–97. [Google Scholar] [CrossRef]
- Zhou, G.S.; Fan, G.; Shen, G.J. The income disparity, the social capital and health: A case study based on China Family Panel Studies. Manag. World 2014, 7, 12–21+51+187. [Google Scholar] [CrossRef]
- Akaeda, N. Welfare states and the health impact of social capital: Focusing on the crowding-out and crowding-in perspectives. Soc. Indic. Res. 2021, 157, 841–862. [Google Scholar] [CrossRef]
- Bolin, K.; Lindgren, B.; Lindström, M.; Nystedt, P. Investments in social capital-implications of social interactions for the production of health. Soc. Sci. Med. 2003, 56, 2379–2390. [Google Scholar] [CrossRef]
- Yang, J.H.; Zhang, J.J.; Wu, M. My home is where my heart is: Regional disparity and self-identity of migrants in China Popul. Econmics 2016, 4, 21–33. [Google Scholar] [CrossRef]
- Tajfel, H.; Billig, M.G.; Bundy, R.P.; Flament, C. Social categorization and intergroup behaviour. Eur. J. Soc. Psychol. 1971, 1, 149–178. [Google Scholar] [CrossRef]
- Cui, Y. A Study on Migrants’ Psychological Integration and Self-identity. Sociol. Stud. 2012, 27, 141–160+244. [Google Scholar] [CrossRef]
- Li, Z.G.; Liang, Q.; Lin, S.N. Identity, characteristics and mechanism of migrants in large Chinese cities of transitional China. Sci. Geogr. Sin. 2020, 40, 40–49. [Google Scholar] [CrossRef]
- Yue, Z.S.; Li, S.Z.; Jin, X.Y.; Feldman, W.M. From ascribed to acquired: Migrant workers’ social networks and migrant interation in China. Society 2011, 6, 130–152. [Google Scholar] [CrossRef]
- Li, S.Z.; Wang, W.B.; Yue, Z.S. Study on the difference of urban residence intention between self-employed and employed migrant workers. Popul. Econmics 2014, 10, 12–21. [Google Scholar] [CrossRef]
- Xu, J.; Tian, Y.; Wang, S.T.; Lu, Y.X. Effects of income and psychological identification on the mental health of China’s migrated agricultural population. Iran. J. Public Health 2018, 47, 1317–1326. [Google Scholar] [PubMed]
- Yu, H.Y.; Yu, L.W. Social convergence, social supportand health of floating population: An empirical analysis based on Zhejiang. Zhejiang Soc. Sci. 2018, 6, 86–95+157–158. [Google Scholar] [CrossRef]
- Benz, M.; Frey, B.S. The value of doing what you like: Evidence from the self-employed in 23 countries. J. Econ. Behav. Organ 2008, 68, 445–455. [Google Scholar] [CrossRef]
- Djankov, S.; Lopez de Silanes, F.; La Porta, R.; Shleifer, A. The law and economics of self-dealing. J. Financ. Econ. 2008, 88, 430–465. [Google Scholar] [CrossRef] [Green Version]
- Knabe, A.; Rätzel, S. Scarring or scaring? The psychological impact of past unemployment and future unemployment risk. Economica 2009, 78, 283–293. [Google Scholar] [CrossRef] [Green Version]
- Sameeksha, D. Measuring entrepreneurship: Type, motivation, and growth. In IZA World of Labor; Institute for the Study of Labor (IZA): Bonn, Germany, 2017; p. 327. [Google Scholar] [CrossRef] [Green Version]
- Binder, M.; Coad, A. Life satisfaction and self-employment: A matching approach. Small Bus. Econ. 2012, 40, 1009–1033. [Google Scholar] [CrossRef] [Green Version]
- Segovia, J.S.; Ravanal, E.C. Complexities of socio-labor integration in Chile: Migrating Colombian women’s experiences. Int. J. Environ. Res. Public Health 2021, 18, 11643. [Google Scholar] [CrossRef] [PubMed]
- Mills, M.B. Gender and inequality in the global labor force. Annu. Rev. Anthropol. 2003, 32, 41–62. [Google Scholar] [CrossRef]
- Gao, X.D.; Tao, S.G. A study of the settlement of the floating population of the minority ethnic groups in Shanghai. J. Yunnan Minzu Univ. (Soc. Sci.) 2015, 32, 81–86. [Google Scholar] [CrossRef]
- Siebers, H.; van Gastel, J. Why migrants earn less: In search of the factors producing the ethno-migrant pay gap in a Dutch public organization. Work. Employ Soc. 2015, 29, 371–391. [Google Scholar] [CrossRef]
- Chiswick, B.R.; Lee, Y.L.; Miller, P.W. Immigrant selection on systems and immigrant health. Contemp. Econ. Policy 2008, 26, 555–578. [Google Scholar] [CrossRef] [Green Version]
- Ortiza, C.; Cuadrado, L.T.; Blázqueza, R.C.; Barriuso, P.R.; Galán, I. Clustering of unhealthy lifestyle behaviors, self-rated health and disability. Prev. Med. 2022, 155, 106911. [Google Scholar] [CrossRef]
- Tervo, H. Self-employment transitions and alternation in finnish rural and urban labour markets. Pap. Reg. Sci. 2008, 87, 55–76. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Z.S. Self-employment behavior of migrant workers in China: Scale, characteristics and entry mechanism. Mod. Econ. Res. 2019, 12, 116–125. [Google Scholar] [CrossRef]
- Moore, C.S.; Mueller, R.E. The transition from paid to self-employment in Canada: The importance of push factors. Appl. Econ. 2002, 34, 791–801. [Google Scholar] [CrossRef]
- Xie, E. Transitions to non-farm self-employment in China. Econ. Res. J. 2012, 47, 54–66. [Google Scholar]
- Gielnik, M.M.; Zacher, H.; Frese, M. Focus on opportunities as a mediator of the relationship between business owners’ age and venture growth. J. Bus. Ventur. 2012, 27, 127–142. [Google Scholar] [CrossRef]
- Rietveld, C.A.; van Kippersluis, H.; Thurik, A.R. Self-Employment and health: Barriers or benefits? Health Econ. 2014, 24, 1302–1313. [Google Scholar] [CrossRef] [PubMed]
- Festinger, L.A. Theory of social comparison processes. Hum. Relat. 1954, 7, 117–140. [Google Scholar] [CrossRef]
- Lee, J.; Kim, M.H. The effect of employment transitions on physical health among the elderly in South Korea: A longitudinal analysis of the Korean Retirement and Income Study. Soc. Sci. Med. 2017, 181, 122–130. [Google Scholar] [CrossRef]
- Nikolova, M. Switching to self-employment can be good for your health. J. Bus. Ventur. 2019, 34, 664–691. [Google Scholar] [CrossRef]
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W.B. The job demands-resources model of burnout. J. Appl. Psychol. 2001, 86, 499–512. [Google Scholar] [CrossRef]
- He, Y.F. Self-employed or employed: Based on the difference in income of female migrants in China. J. Xiangtan Univ. (Philos. Soc. Sci.) 2019, 43, 36–44. [Google Scholar] [CrossRef]
- Nicolaou, N.; Shane, S.; Cherkas, L.; Hunkin, J.; Spector, D.T. Is the tendency to engage in entrepreneurship genetic? Manag. Sci. 2008, 54, 167–179. [Google Scholar] [CrossRef] [Green Version]
- Patel, P.C.; Rietveld, C.A.; Wolfe, M.T.; Wiklund, J. The polygenic risk score of subjective well-being, self-employment, and earnings among older individuals. Entrep. Theory. Pract. 2021, 45, 440–466. [Google Scholar] [CrossRef]
- Ruhm, C.J. Understanding the relationship between macroeconomic conditions and health. In the Elgar Companion to Health Economics, 2nd ed.; Andrew, M.J., Ed.; Edward Elgar Publishing: Cheltenham, UK, 2012; pp. 5–14, Chapter 1. [Google Scholar] [CrossRef]


{kind=link}
| Variable Classes | Variable Name | Variable Meaning and Assignment |
|---|---|---|
| Explained variables | Self-rated health | Self-rated health: 1 = very poor (unable to take care of myself); 2 = poor (unhealthy but able to take care of myself); 3 = average; 4 = good. |
| Explanatory variables | Self-employment | Whether to engage in self-employed activities: 1 = yes; 0 = no |
| Opportunity self-employment | Whether or not hire other worker:1 = yes; 0 = no | |
| Necessity self-employed | Whether it is solo entrepreneurs: 1 = yes; 0 = no | |
| Control variables | Age | Age in years |
| Gender | 1 = male; 0 = female | |
| Nationality | 1 = Han nationality; 0 = others | |
| Education | Education in years | |
| Work_time | Hours worked last week | |
| Income | The logarithm of monthly average total income | |
| Medical Insurance | Availability of Urban Employee Medical Insurance: 1 = yes; 0 = no | |
| Health record | Availability of health records: 1 = yes; 0 = no | |
| industry | 1 = productive services; 2 = secondary industry; 3 = living services | |
| region | 1 = East; 2 = Central; 3 = West; 4 = Northeast. | |
| Other variables | Manual labor | Whether or not in a labor-intensive industry: 1 = yes; 0 = no |
| Flexible time | Whether or not lack of time to see a doctor:1 = no; 0 = yes | |
| Working stability | Whether or not face difficulties of unstable work: 1 = no; 0 = yes | |
| Wage | The logarithm of last month’s total income | |
| Medical payment ability | Whether or not lack of money to see a doctor: 1 = no; 0 = yes | |
| Social capital | Whether the person interacts most is local residents: 1 = yes; 0 = no | |
| Psychological identity | Whether they identify themselves as local people: 1 = not at all, 2 = not; 3 = basically; 4 = fully |
| Index | Self-Employed | Wage Workers | Difference between Group |
|---|---|---|---|
| Health | 3.823 | 3.845 | 0.0208 *** |
| Age | 37.939 | 34.431 | −3.508 *** |
| Age groups | |||
| 18–24 | 0.047 | 0.150 | 0.104 *** |
| 25–34 | 0.341 | 0.408 | 0.067 *** |
| 35–44 | 0.354 | 0.257 | −0.096 *** |
| 45–54 | 0.221 | 0.154 | −0.067 *** |
| 54–60 | 0.037 | 0.030 | −0.008 *** |
| Gender | 0.598 | 0.585 | −0.013 *** |
| Nationality | 0.920 | 0.904 | −0.015 *** |
| Education | 9.258 | 10.205 | 0.947 *** |
| Work_time | 65.211 | 53.732 | −11.408 *** |
| Income | 7796.68 | 6436.976 | −1359.80 *** |
| Medical insure | 0.039 | 0.023 | −0.015 *** |
| Health record | 0.271 | 0.238 | −0.033 *** |
| Industry groups | |||
| Productive services | 0.034 | 0.080 | 0.047 *** |
| Secondary industry | 0.213 | 0.516 | 0.388 *** |
| Living services | 0.753 | 0.403 | −0.035 *** |
| Region | |||
| East | 0.313 | 0.515 | 0.203 *** |
| Central | 0.245 | 0.149 | −0.096 *** |
| West | 0.398 | 0.276 | −0.121 *** |
| Northeast | 0.045 | 0.060 | 0.015 *** |
| Manual labor | 0.237 | 0.567 | 0.330 *** |
| Flexible time | 0.966 | 0.967 | −0.001 |
| Working stability | 0.806 | 0.774 | −0.032 *** |
| Wage | 4556.779 | 3859.6 | −697.180 *** |
| Medical payment ability | 0.987 | 0.986 | −0.001 |
| social capital | 0.311 | 0.251 | −0.006 *** |
| Psychological identity | 2.968 | 2.829 | −0.139 *** |
| Observations | 41,068 | 55,724 |
| Variables | Oprobit | IV-Oprobit | ||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |
| Self_employment | −0.041 *** | 0.056 *** | 0.063 *** | 0.230 *** |
| (0.010) | (0.010) | (0.012) | (0.037) | |
| Age groups (base:18–24) | ||||
| 25–34 | −0.215 *** | −0.252 *** | −0.274 *** | |
| (0.021) | (0.021) | (0.021) | ||
| 35–44 | −0.446 *** | −0.483 *** | −0.516 *** | |
| (0.021) | (0.021) | (0.022) | ||
| 45–54 | −0.727 *** | −0.759 *** | −0.790 *** | |
| (0.022) | (0.022) | (0.023) | ||
| 55–60 | −0.990 | −1.012 *** | −1.038 *** | |
| (0.030) | (0.030) | (0.030) | ||
| Gender | 0.087 *** | 0.093 *** | 0.088 *** | |
| (0.010) | (0.011) | (0.010) | ||
| Nationality | 0.070 *** | 0.068 *** | 0.061 *** | |
| (0.017) | (0.017) | (0.018) | ||
| education | 0.026 *** | 0.022 *** | 0.024 *** | |
| (0.002) | (0.002) | (0.002) | ||
| Work_time | −0.002 *** | −0.003 *** | ||
| (0.000) | (0.000) | |||
| lncome | 0.095 *** | 0.079 *** | ||
| (0.010) | (0.010) | |||
| Medical insurance | −0.086 *** | −0.096 *** | ||
| (0.028) | (0.028) | |||
| Health record | 0.097 *** | 0.096 *** | ||
| (0.012) | (0.012) | |||
| Industry (base: productive services) | ||||
| Secondary industry | 0.047 * | 0.050 * | ||
| (0.022) | (0.022) | |||
| Living services | 0.045 * | −0.000 | ||
| (0.022) | (0.024) | |||
| Region (base: East) | ||||
| Middle | −0.196 *** | −0.219 *** | −0.211 *** | −0.237 *** |
| (0.013) | (0.014) | (0.014) | (0.015) | |
| West | −0.153 *** | −0.133 *** | −0.115 *** | −0.145 *** |
| (0.011) | (0.012) | (0.012) | (0.014) | |
| Northeast | −0.185 | −0.137 *** | −0.110 *** | −0.114 *** |
| (0.022) | (0.022) | (0.022) | (0.022) | |
| Pseudo R2 | 0.004 | 0.043 | 0.045 | |
| Lnsig_2 | −0.912 *** | |||
| (0.002) | ||||
| atanhrho_12 | −0.074 *** | |||
| (0.016) | ||||
| LR chi2/Wald chi2 | 357.20 *** | 3887.78 *** | 4124.94 *** | 53,636.20 *** |
| Log likelihood | −45,269.725 | −43,504.435 | −43,385.855 | −92,405.983 |
| Observations | 96,792 | 96,792 | 96,792 | 96,792 |
| Sample | Treated | Controls | ATT | Standar Error | T-Value | |
|---|---|---|---|---|---|---|
| Health | Unmatched | 3.824 | 3.845 | −0.021 | 0.003 | −7.89 |
| K-value Neighbor (K = 4) | 3.824 | 3.797 | 0.027 | 0.004 | 5.63 | |
| Caliper and Radius (cal = 0.01) | 3.824 | 3.799 | 0.025 | 0.005 | 4.52 | |
| Kernel and Local Linear | 3.825 | 3.801 | 0.024 | 0.007 | 3.90 |
| Variables | Mode 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 |
|---|---|---|---|---|---|---|---|
| Diarrhea | Fever | Skin Rashes | Jaundice | Conjunctivitis | Cold | Sick | |
| Self-employment | −0.094 ** | −0.139 *** | −0.381 *** | 0.171 | −0.199 *** | −0.208 *** | −0.535 *** |
| (0.039) | (0.040) | (0.056) | (0.180) | (0.068) | (0.031) | (0.030) | |
| Control variables | Control | Control | Control | Control | Control | Control | Control |
| Constant | −2.031 *** | −1.501 *** | −2.884 *** | −2.000 *** | −2.756 *** | −0.993 *** | −1.745 *** |
| (0.105) | (0.110) | (0.151) | (0.489) | (0.184) | (0.084) | (0.082) | |
| Wald chi2 | 684.72 *** | 354.41 *** | 195.39 *** | 65.34 *** | 99.16 *** | 1055.37 *** | 1786.20 *** |
| Observations | 96,792 | 96,792 | 96,792 | 96,792 | 96,792 | 96,792 | 96,792 |
| Variables | Oprobit | Probit |
|---|---|---|
| Model 1 Health | Model 2 Likelihood of Sick | |
| Opportunity self-employed | 0.069 *** | −0.139 *** |
| (0.023) | (0.019) | |
| Necessity self-employed | 0.062 *** | −0.186 *** |
| (0.012) | (0.010) | |
| Control variable | control | control |
| Constant | −1.205 *** | |
| (0.073) | ||
| Pseudo R2/R-squared | 0.045 | 0.013 |
| LR chi2/wald chi2 | 4125.03 *** | 1757.83 *** |
| Log likelihood | −43,385.808 | −66,148.823 |
| Observations | 96,792 | 96,792 |
| Variables | Mode1 | Model 2 | Model 3 | Model 4 |
|---|---|---|---|---|
| Men | Women | Han Nationality | Ethnic Minority | |
| Self-employment | 0.264 *** | 0.183 *** | 0.258 *** | −0.072 |
| (0.051) | (0.054) | (0.039) | (0.118) | |
| Control variable | control | control | control | control |
| Wald chi2 | 30,391.51 *** | 24,105.80 *** | 49,129.56 *** | 4680.29 *** |
| Log likelihood | −54,638.587 | −37,477.517 | −83,939.327 | −8366.088 |
| Observations | 57,176 | 39,616 | 88,177 | 8615 |
| Variables | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Manual Labor | Flexible Time | Working Stability | |
| Self-employment | −0.458 *** | 0.111 *** | 0.241 *** |
| (0.032) | (0.017) | (0.011) | |
| Constant | 1.504 *** | 2.496 *** | −1.872 *** |
| (0.239) | (0.141) | (0.085) | |
| Control variable | control | control | control |
| Constant | 1.504 *** | 2.496 *** | −1.872 *** |
| (0.239) | (0.141) | (0.085) | |
| Pseudo R2 | 0.640 | 0.014 | 0.055 |
| LR chi2 | 18,043.75 *** | 398.73 *** | 5531.79 *** |
| Log likelihood | −5085.095 | −14,069.308 | −47,295.463 |
| Control variable | control | control | control |
| Observations | 96,792 | 96,792 | 96,792 |
| Variables | Financial Return | Social Integration | ||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model3 | Model 4 | |||||
| OLS | Oprobit | Probit | Oprobit | Probit | Oprobit | Oprobit | Oprobit | |
| Wage | Health | Medical Payment Ability | Health | Social Capital | Health | Psychological Identity | Health | |
| Self-employment | 0.071 *** | 0.079 *** | 0.181 *** | 0.056 *** | 0.109 *** | 0.060 *** | 0.077 *** | 0.097 *** |
| (0.007) | (0.011) | (0.026) | (0.012) | (0.010) | (0.012) | (0.008) | (0.007) | |
| Wage | 0.058 *** | |||||||
| (0.004) | ||||||||
| Medical payment ability | 0.705 *** | |||||||
| (0.033) | ||||||||
| Social capital | 0.081 *** | |||||||
| (0.012) | ||||||||
| Psychological identity | 0.058 *** | |||||||
| (0.012) | ||||||||
| Constant | 7.824 *** | 0.254 *** | −1.652 *** | |||||
| (0.025) | (0.200) | (0.078) | ||||||
| Control variable | control | control | control | control | control | control | control | control |
| Adj R2/Pseudo R2 | 0.058 | 0.0460 | 0.057 | 0.050 | 0.067 | 0.046 | 0.038 | 0.048 |
| Observations | 96,792 | 96,792 | 96,792 | 96,792 | 96,792 | 96,792 | 96,792 | 96,792 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, W.; He, L.; Lan, H. The Impact of Self-Employment on the Health of Migrant Workers: Evidence from China Migrants Dynamic Survey. Int. J. Environ. Res. Public Health 2022, 19, 5868. https://doi.org/10.3390/ijerph19105868
Huang W, He L, Lan H. The Impact of Self-Employment on the Health of Migrant Workers: Evidence from China Migrants Dynamic Survey. International Journal of Environmental Research and Public Health. 2022; 19(10):5868. https://doi.org/10.3390/ijerph19105868
Chicago/Turabian StyleHuang, Wanting, Lei He, and Hongxing Lan. 2022. "The Impact of Self-Employment on the Health of Migrant Workers: Evidence from China Migrants Dynamic Survey" International Journal of Environmental Research and Public Health 19, no. 10: 5868. https://doi.org/10.3390/ijerph19105868