
The Effects of Group Art Therapy on the Primary Family Caregivers of Hospitalized Patients with Brain Injuries in South Korea

 , , , and
, , , and
Abstract
:1. Introduction
1.1. Patients with Brain Injury and Their Families
1.2. Benefits of Art Therapy
1.3. Purpose
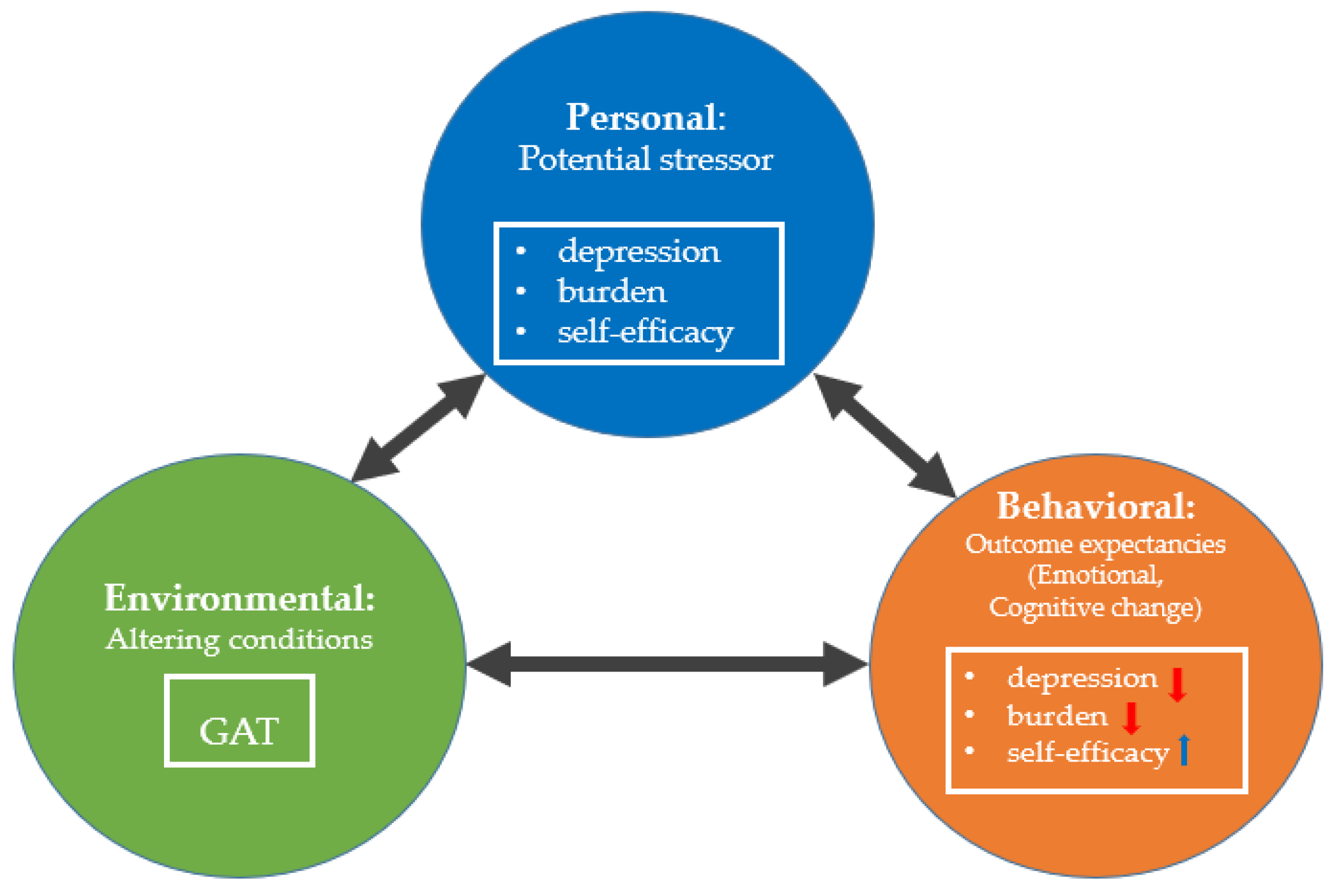
2. Theoretical Framework
3. Materials and Methods
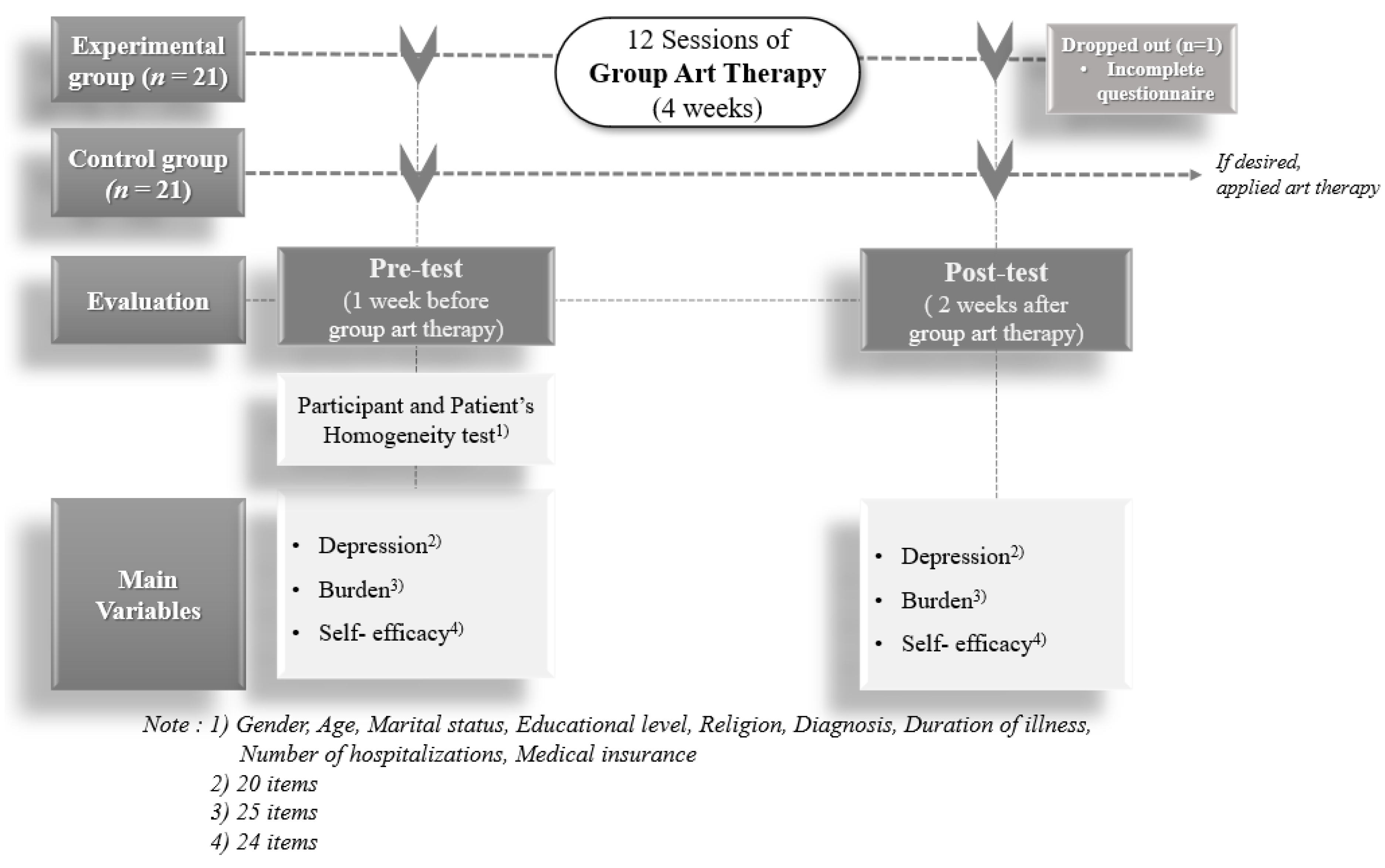
3.1. Design
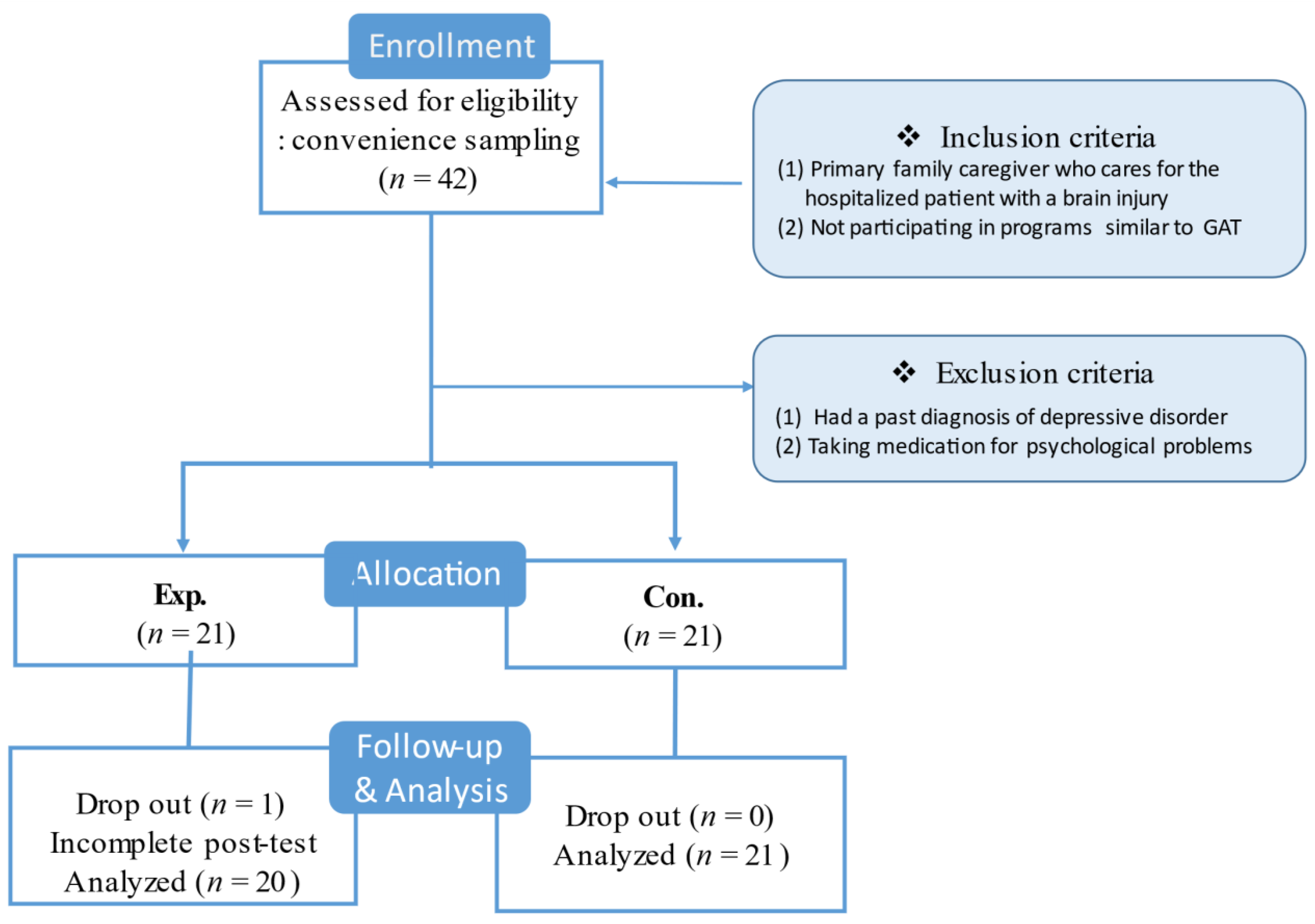
3.2. Setting and Participants
3.3. Measurements
3.3.1. Depression
3.3.2. Burden
3.3.3. Self-Efficacy
3.3.4. Content Validity
3.4. Training of the Research Assistant
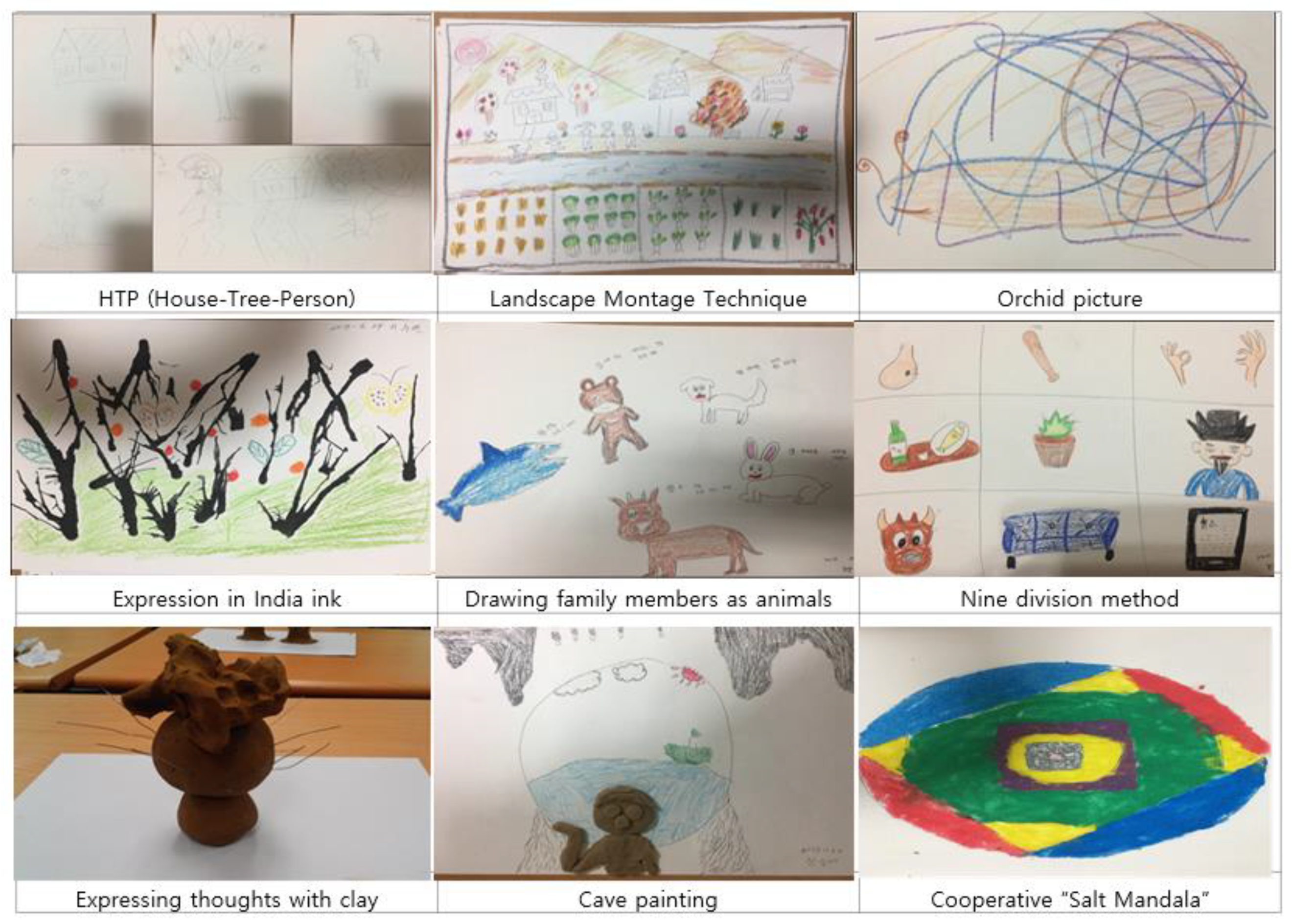
3.5. Group Art Therapy Intervention
- Group formation phase (Sessions 1–5): Builds trust and intimacy among the group members, reduces their burden, and adapts them to and induces interest in GAT.
- Ego search phase (Sessions 6–9): Explores and recognizes an individual’s inner feelings and promotes self-efficacy through interactions among group members. It also reduces stress and anxiety, promotes understanding of oneself and others, and facilitates group interaction.
- Self-acceptance phase (Sessions 10–11): Enables an individual’s recognition of the changes in themselves, makes them confident through emotional stability, and establishes a positive self-image.
- Closing phase (Session 12): Organizes and closes the process through the group activity of “Salt Mandala”.
3.6. Data Collection
3.7. Ethical Considerations
3.8. Data Analysis
4. Results
4.1. Descriptive Results and Homogeneity Test of Demographic Characteristics and Outcome Variables
4.2. Mean Differences in the Dependent Variables between the Two Groups
5. Discussion
5.1. Implications for Nursing Practice
5.2. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, K.S.; Yoon, E.J.; Kim, S.Y.; Kim, O.S.; Soo, H.S.; Lee, M.S.; Seo, Y.O.; Lee, M.S.; Lee, D.N.; Lee, E.J.; et al. Adult Health Nursing; Soomonsa Publishing Co.: Paju, Korea, 2015; pp. 1219–1252. [Google Scholar]
- Korean Ministry of Health and Welfare. Korean Disability Welfare Act. 2017. Available online: http://www.law.go.kr/lsInfoP.do?lsiSeq=198604&efYd=20171230#0000 (accessed on 24 June 2020).
- Li, M.; Zhao, Z.; Yu, G.; Zhang, J. Epidemiology of traumatic brain injury over the world: A systematic review. Austin Neurol. Neurosci. 2016, 1, 1–14. [Google Scholar] [CrossRef]
- Statistics Korea. Cause of Death Statistics. 2016. Available online: http://kostat.go.kr/portal/korea/kor_nw/2/6/1/index.board?bmode=read&aSeq=363268 (accessed on 24 June 2020).
- Kim, Y.; Choi, E.Y. An analysis of family function and burden of family caregivers of the patient with brain injury. Korean J. Stress Res. 2012, 20, 61–68. [Google Scholar]
- Seok, J.H.; Yang, Y.A. A study on the relationship between guardian burden and quality of life according to activities of daily living of brain lesion patients. OTAD 2019, 13, 89–95. [Google Scholar]
- Yu, H.Y.; Shin, J.I. Correlation between depression of stroke caregivers and their life quality. Korea Aging Friendly Ind. Assoc. (KAFA) 2011, 3, 59–66. [Google Scholar]
- Sohn, J.H. Burden and Intention to Use the Long-Term Care Hospital among Family Caregivers of Elderly with Stroke. Master’s Thesis, Hanyang University, Seoul, Korea, 2016. [Google Scholar]
- Denno, M.S.; Gillard, P.J.; Graham, G.D.; DiBonaventure, M.D.; Goren, A.; Varon, S.F.; Zorowitz, R. Anxiety and depression associated with caregiver burden in caregivers of stroke survivors with spasticity. Arch. Phys. Med. Rehabil. 2013, 94, 1731–1736. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psych. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Han, H.J. Effects of Self Assertiveness training on the Development of Children’s Self-Efficacy. Master’s Thesis, Seoul National University of Education, Seoul, Korea, 2002. [Google Scholar]
- Han, E.S. The Effects of Group Art Therapy on Psychological Well-Being and Self-Efficacy of Working Mothers. Master’s Thesis, Seoul Women’s University, Seoul, Korea, 2014. [Google Scholar]
- Kim, J.H. The Effects of Group Art Therapy on Self-Efficacy and Stress Coping Ability of Adolescents. Master’s Thesis, Wonkwang University, Iksan, Korea, 2016. [Google Scholar]
- Bandura, A. Social Foundation of thought and Action: A Social Cognitive Theory; Englewood Cliff, N.J., Ed.; Prentice-Hall: New York, NY, USA, 1986; pp. 117–164. [Google Scholar]
- Suh, M.H.; Oh, K.S. A study of well-being in caregivers caring for chronically ill family members. J. Korean Acad. Nurs. 1993, 23, 467–486. [Google Scholar] [CrossRef] [Green Version]
- Choi, E.M. Art Therapy Techniques and Applications; Sigma Press: Seoul, Korea, 2011; pp. 193–209. [Google Scholar]
- Korean Art Therapy Association. Theory and Practice of Art Therapy; Dong-A Publishing Co.: Seoul, Korea, 2000; pp. 69–128. [Google Scholar]
- Stuckey, H.L.; Nobel, J. The connection between art, healing, and public health: A review of current literature. Am. J. Public Health 2010, 100, 254–263. [Google Scholar] [CrossRef]
- Goetze, H.; Geue, K.; Buttstaedt, M.; Singe, S.; Schwarz, R. Art therapy for cancer patients in outpatient care. Psychological distress and coping of the participants. Forschende Komplementarmedizin 2009, 16, 28–33. [Google Scholar] [CrossRef]
- Nigmatullina, I.; Gerasimenko, J.A. Correction of school disadaptation of teenagers by art therapy methods. Int. J. Environ. Sci. 2016, 11, 2037–2045. [Google Scholar]
- Riley, S. Contemporary Art Therapy with Adolescents; Jessica Kingsley: Philadelphia, PA, USA, 1999; p. 237. [Google Scholar]
- Kim, Y.R.; Kim, Y.J. The effects of group art therapy on relieving depression of the elderly stroke patients. J. Fam. Relat. 2009, 14, 213–237. [Google Scholar]
- Kim, J.Y.; Park, H.J.; Lee, I.S. The effects of group art therapy with Hanji, Korean paper, to improve the quality of life of elderly stroke patients. Korean Geron. Soc. 2012, 32, 87–102. [Google Scholar]
- Lee, H.Y. The Effects of Group Art Therapy on the Happiness of Mothers of Children with Handicapped. Master’s Thesis, Daegu University, Daegu, Korea, 2015. [Google Scholar]
- Rubin, J.A. Approaches to Art Therapy; Brunner Mazzel Publishers: New York, NY, USA, 2001; pp. 251–274. [Google Scholar]
- Polit, D.F.; Beck, C.T. Nursing Research: Generating and Assessing Evidence for Nursing Practice, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2017; pp. 200–201. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Chon, K.K.; Rhee, M.K. Development of Korean version of CES-D: A preliminary study. Korean Psychol. Assoc. 1992, 11, 437–445. [Google Scholar]
- Cha, J.E. Study for the General Self-Efficacy Scale Development. Master’s Thesis, Ewha Women’s University, Seoul, Korea, 1997. [Google Scholar]
- Sherer, M.; Maddux, J.E.; Prentice-Dunn, B.M.S.; Jacobs, B.; Rogers, R.W. The self-efficacy scale: Construction and validation. Psychol. Rep. 1982, 51, 663–671. [Google Scholar] [CrossRef]
- Morrison, G.R. Designing Effective Instruction, 6th ed.; John Wiley & Sons: New York, NY, USA, 2010; pp. 230–287. [Google Scholar]
- Orr, P.P. Art therapy with children after a disaster: A content analysis. Arts Psychother. 2007, 34, 350–361. [Google Scholar] [CrossRef]
- Monti, D.A.; Peterson, C.; Kunkel, E.J.S.; Hauck, W.W.; Pequignot, E.; Rhodes, L.; Brainard, G.C. A randomized, controlled trial of mindfulness-based art therapy (MBAT) for women with cancer. Psychooncology 2006, 15, 363–373. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, M.W.; Nabors, L.; Quinlan, A. The effectiveness of art therapy: Does it work? Art Ther. 2000, 17, 207–213. [Google Scholar] [CrossRef]
- Puig, A.; Min Lee, S.; Goodwin, L.; Sherrard, P. The efficacy of creative arts therapies to enhance emotional expression, spirituality, and psychological well-being of newly diagnosed stage I and stage II breast cancer patients: A preliminary study. Arts Psychother. 2006, 33, 218–228. [Google Scholar] [CrossRef]
- Nobel, J.; Kazis, L.E.; Cabral, H.; Soley-Bori, M.; Allen, H. Artfully advancing treatment of diabetes. Physician Leadersh. J. 2017, 4, 46–52. [Google Scholar]
- Waller, D.; Sibbett, C. Art Therapy and Cancer Care; Open University Press: London, UK, 2005; pp. 69–95. [Google Scholar]
- Spier, E.; Bend, N. Group art therapy with eighth-grade students transitioning to high school. Art Ther. 2010, 27, 75–83. [Google Scholar] [CrossRef]
- Cira, F.; Michelle, K. The effect of a creative art program on self-esteem, hope, perceived social support, and self-efficacy in individuals with multiple sclerosis: A pilot study. J. Neurosci. Nurs. 2014, 46, 330–336. [Google Scholar]
- Mueller, J.; Alie, C.; Jonas, B.; Brown, E.; Sherr, L. A quasi-experimental evaluation of a community-based art therapy intervention exploring the psychosocial health of children affected by HIV in South Africa. Trop. Med. Int. Health 2011, 16, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Elkis-Abuhoff, D.L.; Goldblatt, R.B.; Gaydos, M.; Corrato, S. The effects of clay manipulation on somatic dysfunction and emotional distress in patients with Parkinson’s disease. Art Ther. 2008, 25, 122–128. [Google Scholar] [CrossRef]
- Gerasimenko, Y.A.; Karpova, G.A. Interpersonal Relationships of Students with Hearing Impairment; Ural State University: Ekaterinburg, Russia, 2004; p. 196. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Session (Duration) | Theme | Contents | Method |
|---|---|---|---|
| I (1 h) | HTP (House-Tree-Person) | Introduction
| Lecture PPT |
Activities
| A4 paper Pencil Eraser | ||
Wrap-up
| Presentation Discussion | ||
| II (1 h) | LMT (Landscape Montage Technique) | Introduction
| PPT |
Activities
| A3 paper Black marker Colored pencil Crayon | ||
Wrap-up
| Presentation Discussion | ||
| III (1 h) | Orchid picture | Introduction
| PPT |
Activities
| A3 paper Watercolor Colored pencil Marker pen | ||
Wrap-up
| Presentation Discussion | ||
| IV (1 h) | Figure drawing from the frontal perspective | Introduction
| PPT |
Activities
| A2 paper Crayon WatercolorColored pencil Marker pen | ||
Wrap-up
| Presentation Discussion | ||
| V (1 h) | Expression in India ink | Introduction
| PPT |
Activities
| A3 paperIndia ink Colored Pencil Crayon Watercolor | ||
Wrap-up
| Presentation Discussion | ||
| VI (1 h) | Drawing family members as animals | Introduction
| PPT |
Activities
| A3 paper Crayon WatercolorColored pencil Marker | ||
Wrap-up
| Presentation Discussion | ||
| VII (1 h) | 9 division method | Introduction
| PPT |
Activities
| A4 paper 4B pencil Eraser Crayon WatercolorColored pencil Marker pen | ||
Wrap-up
| Presentation Discussion | ||
| VIII (1 h) | Expressing thoughts with clay | Introduction
| PPT |
Activities
| Oil-based clay Wire Decorative items | ||
Wrap-up
| Presentation Discussion | ||
| IX (1 h) | Cave painting | Introduction
| PPT |
Activities
| Oil-based clay A3 paper Crayon Watercolor Colored pencil Marker | ||
Wrap-up
| Presentation Discussion | ||
| X (1 h) | Self-portrait &others’ portraits | Introduction
| PPT |
Activities
| A4 paper MagazinesGlue & scissors WatercolorCrayon Marker | ||
Wrap-up
| Presentation Discussion | ||
| XI (1 h) | Gift I want to receive, Gift I want to give to my family members | Introduction
| PPT |
Activities
| A4 paper MagazinesGlue WatercolorCrayon Marker | ||
Wrap-up
| Presentation Discussion | ||
| XII (1 h) | Cooperative Salt “Mandala” | Introduction
| PPT |
Activities
| Pastel Salt A2 paper Glue | ||
Wrap-up
| Presentation Discussion |
| Characteristics | Experimental (n = 20) | Control (n = 21) | χ2/t | p | ||
|---|---|---|---|---|---|---|
| N | % | N | % | |||
| Caregivers | ||||||
| Gender | ||||||
| Male | 6 | 30 | 6 | 28.6 | 0.010 | 0.92 |
| Female | 14 | 70 | 15 | 71.4 | ||
| Age | ||||||
| 20–29 | 0 | 0 | 2 | 9.5 | 11.679 | 0.07 |
| 30–39 | 3 | 15.0 | 0 | 0.0 | ||
| 40–49 | 0 | 0 | 5 | 23.8 | ||
| 50–59 | 7 | 35.0 | 6 | 28.6 | ||
| 60–69 | 8 | 40.0 | 6 | 28.6 | ||
| 70–79 | 1 | 5.0 | 2 | 9.5 | ||
| 80–89 | 1 | 5.0 | 0 | 0 | ||
| Religion | ||||||
| Religious | 13 | 65.0 | 14 | 66.7 | 1.178 | 0.882 |
| Nonreligious | 7 | 35.0 | 7 | 33.3 | ||
| Relation | ||||||
| Spouse | 11 | 55 | 8 | 38.1 | 4.785 | 0.31 |
| Son | 5 | 25 | 7 | 33.3 | ||
| Daughter | 1 | 5 | 3 | 14.3 | ||
| Other | 3 | 15 | 3 | 14.3 | ||
| Patient | ||||||
| Gender | ||||||
| Male | 5 | 25.0 | 15 | 71.4 | 0.067 | 0.796 |
| Female | 15 | 75.0 | 6 | 28.6 | ||
| Age | ||||||
| 20–29 | 1 | 5 | 1 | 4.8 | 6.046 | 0.418 |
| 30–39 | 2 | 10.0 | ||||
| 40–49 | 1 | 5.0 | 3 | 14.3 | ||
| 50–59 | 6 | 30.0 | 2 | 9.5 | ||
| 60–69 | 4 | 20.0 | 6 | 28.6 | ||
| 70–79 | 5 | 25.0 | 7 | 33.3 | ||
| 80–89 | 1 | 5 | 2 | 9.5 | ||
| Diagnosis | ||||||
| Injury by accident | 2 | 10.0 | 3 | 14.3 | 1.253 | 0.74 |
| Cerebral hemorrhage | 7 | 35.0 | 6 | 28.6 | ||
| Cerebral infarction | 11 | 55.0 | 12 | 57.1 | ||
| Duration | ||||||
| <6 months | 7 | 35.0 | 12 | 57.1 | 2.02 | 0.155 |
| >6 months | 13 | 65.0 | 9 | 42.9 | ||
| Number of hospitalizations | ||||||
| 1 time | 5 | 25.0 | 2 | 9.5 | 3.949 | 0.413 |
| 2 times | 6 | 30.0 | 8 | 38.1 | ||
| 3 times | 3 | 15.0 | 6 | 28.6 | ||
| 4 times | 1 | 4.8 | ||||
| More than 5 times | 6 | 30.0 | 4 | 19.0 | ||
| Main variables | ||||||
| Depression | 16.90 ± 10.13 | 18.71 ± 8.42 | 0.625 | 0.536 | ||
| Burden | 78.55 ± 9.67 | 73.24 ± 11.58 | −1.579 | 0.119 | ||
| Self-efficacy | 74.95 ± 10.84 | 76.57 ± 8.26 | 5.041 | 0.592 | ||
| Variables | Groups | Pre-Test | Post-Test | Paired-t (p) | t | d | p |
|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | ||||||
| Depression | Exp. | 16.90 (10.13) | 11.80 (7.35) | 3.296 (0.004) | 0.861 | 1.62 | 0.395 |
| Con. | 18.71 (8.42) | 16.14 (9.77) | 1.046 (0.308) | ||||
| Burden | Exp. | 78.55 (9.67) | 71.15 (11.60) | 4.564 (<0.001) | 2.462 | 1.19 | 0.020 |
| Con. | 73.24 (11.58) | 74.81 (11.03) | −0.481 (0.635) | ||||
| Self-efficacy | Exp. | 74.95 (10.84) | 80.95 (8.86) | −5.395 (<0.001) | −6.270 | 1.38 | <0.001 |
| Con. | 76.57 (8.26) | 74.19 (8.52) | 3.211 (0.004) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, N.; Kim, S.-J.; Jeong, G.-H.; Oh, Y.; Jang, H.; Kim, A.-L. The Effects of Group Art Therapy on the Primary Family Caregivers of Hospitalized Patients with Brain Injuries in South Korea. Int. J. Environ. Res. Public Health 2021, 18, 5000. https://doi.org/10.3390/ijerph18095000
Kim N, Kim S-J, Jeong G-H, Oh Y, Jang H, Kim A-L. The Effects of Group Art Therapy on the Primary Family Caregivers of Hospitalized Patients with Brain Injuries in South Korea. International Journal of Environmental Research and Public Health. 2021; 18(9):5000. https://doi.org/10.3390/ijerph18095000
Chicago/Turabian StyleKim, Nayoung, Shin-Jeong Kim, Geum-Hee Jeong, Younjae Oh, Heejung Jang, and Aee-Lee Kim. 2021. "The Effects of Group Art Therapy on the Primary Family Caregivers of Hospitalized Patients with Brain Injuries in South Korea" International Journal of Environmental Research and Public Health 18, no. 9: 5000. https://doi.org/10.3390/ijerph18095000