
Effectiveness of Integrated Education to Reduce Postoperative Nausea, Vomiting, and Dizziness after Abdominal Surgery under General Anesthesia

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
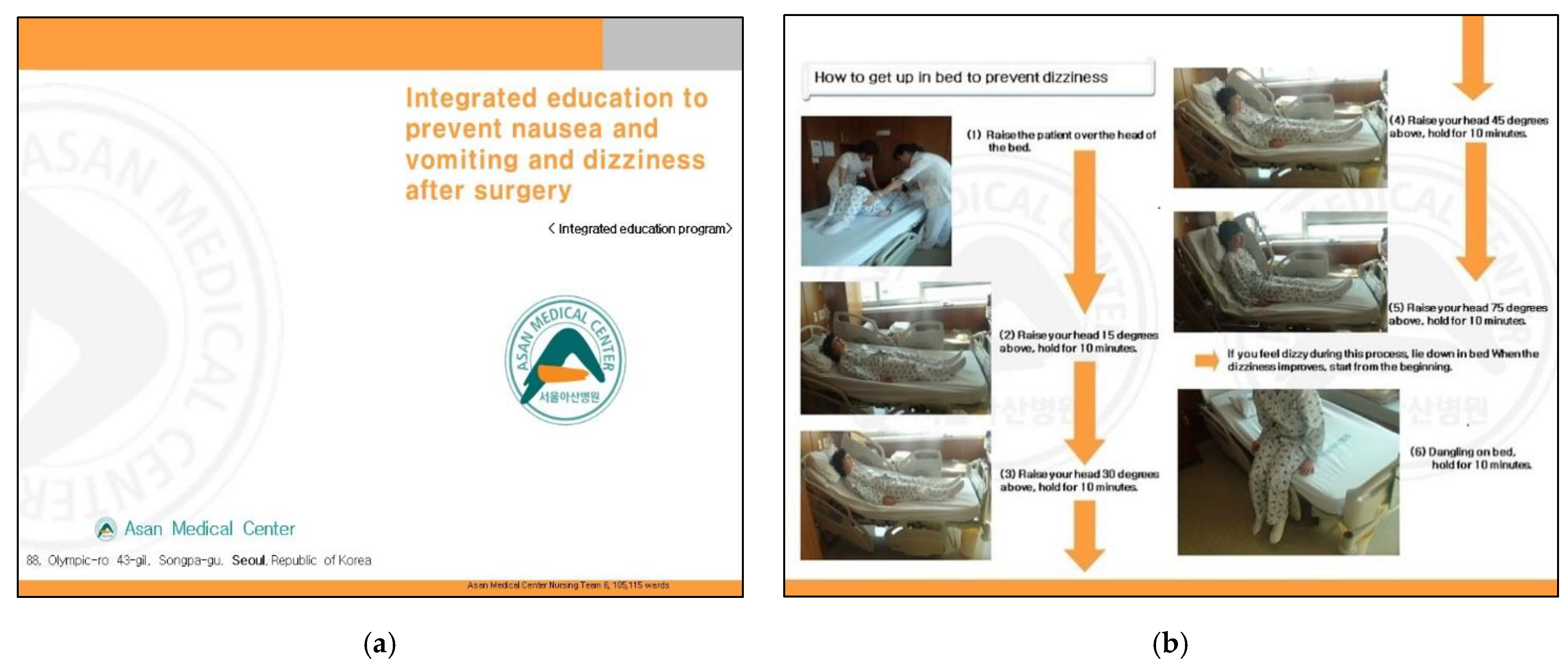
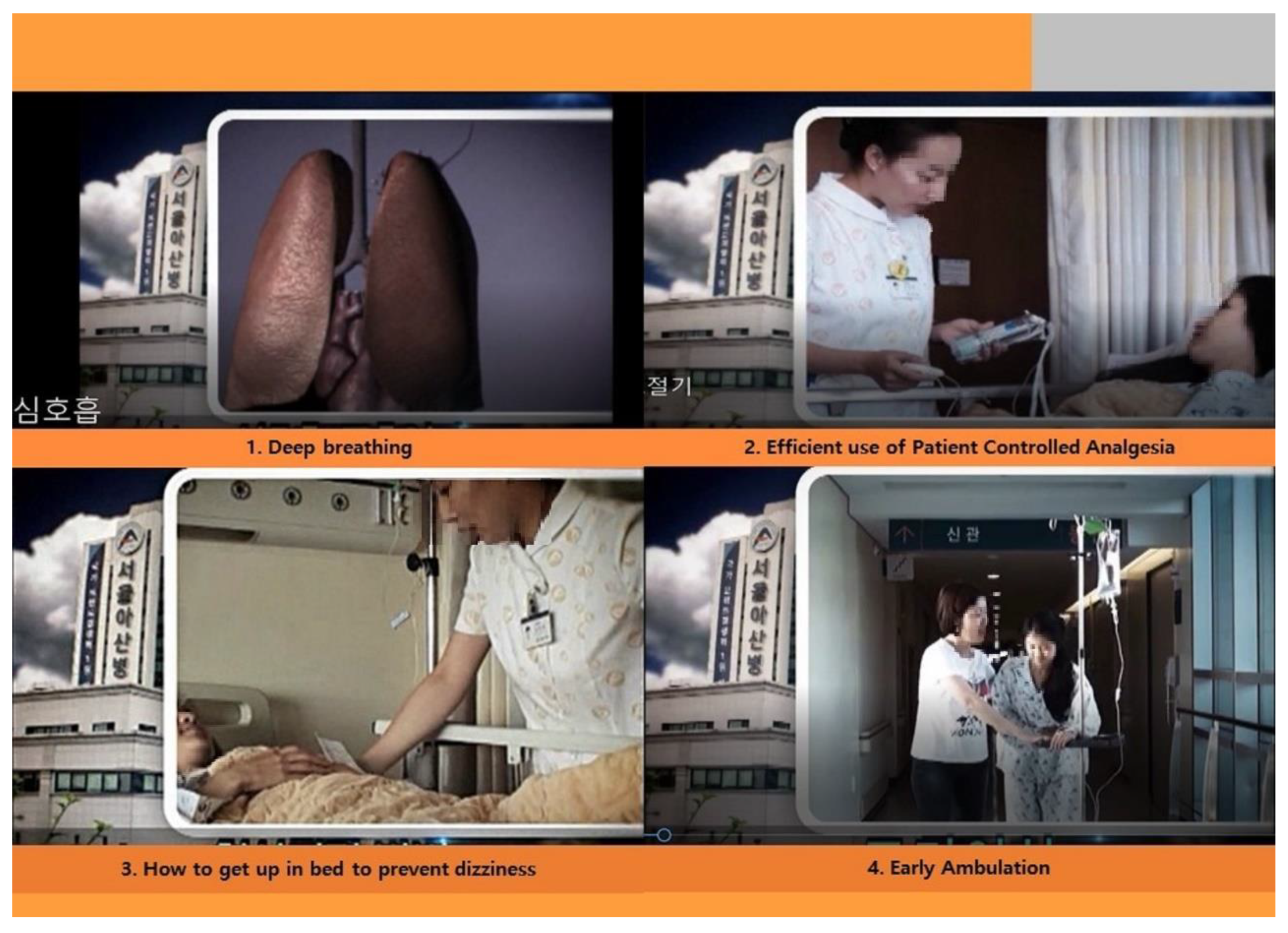
2.3. Process of Developing the Anticipatory Integrated Education Program
2.4. Study Protocol
2.5. Measurements
2.5.1. Nausea and Dizziness
2.5.2. Vomiting and Frequency of Antiemetic Use
2.6. Data Collection
2.7. Ethics
2.8. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Noh, S.H. Conventional open surgery in early gastric cancer. J. Korean Med. Assoc. 2010, 53, 306–310. [Google Scholar] [CrossRef] [Green Version]
- National Health Insurance Service. Statistics of Surgical Operations Covered by NIH. Available online: https://www.nhis.or.kr/nhis/together/wbhaec06800m01.do?mode=view&articleNo=135135&article.offset=0&articleLimit=10 (accessed on 20 April 2021).
- National Cancer Center. 2018 National Cancer Registration Statistics. 2020. Available online: https://ncc.re.kr/cancerStatsView.ncc?bbsnum=538&searchKey=total&searchValue=&pageNum=1 (accessed on 20 April 2021).
- Keikhaie, K.R.; Amirshahi, M.; Behnamfar, N.; Badakhsh, M.; Rafiemanesh, H.; Sheyback, M.; Sari, M. Prevalence of postoperative nausea and vomiting: A systematic review and meta-analysis. Saudi J. Anaesth. 2020, 14, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.-J.; Lee, E. Cost analysis of post operative pain management for surgical patients using PCA. J. Korean Acad. Fundam. Nurs. 2013, 20, 137–146. [Google Scholar] [CrossRef] [Green Version]
- Bulut, M.; Alemdar, D.K.; Bulut, A.; Şalcı, G. The effect of music therapy, hand massage, and kaleidoscope usage on postoperative nausea and vomiting, pain, fear, and stress in children: A randomized controlled trial. J. PeriAnesth. Nurs. 2020, 35, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wei, X.; Zhang, S.; Zhou, L.; Zhang, J. A meta-analysis of palonosetron for the prevention of postoperative nausea and vomiting in adults. J. PeriAnesth. Nurs. 2015, 30, 398–405. [Google Scholar] [CrossRef]
- Kim, N.C.; Yoo, J.B.; Cho, M.S.; Shin, E.J.; Hahm, T.S. Effects of Nei-Guan acupressure on nausea, vomiting and level of satisfaction for gynecological surgery patients who are using a patient-controlled analgesia. J. Korean Acad. Nurs. 2010, 40, 423–432. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.D.; Lee, H.K.; Park, Y.G.; Lee, W.S. Quality of life after acoustic tumor surgery. J. Korean Skull Base Soc. 2007, 2, 18–22. [Google Scholar]
- Mattila, K.; Toivonen, J.; Janhunen, L.; Rosenberg, P.H.; Hynynen, M. Postdischarge Symptoms after ambulatory surgery: First-week incidence, intensity, and risk factors. Anesth. Analg. 2005, 101, 1643–1650. [Google Scholar] [CrossRef]
- De Almeida, E.; De Almeida, J.; Landoni, G.; Galas, F.R.B.G.; Fukushima, J.; Fominskiy, E.; De Brito, C.; Cavichio, L.; De Almeida, L.; Ribeiro, U., Jr.; et al. Early mobilization programme improves functional capacity after major abdominal cancer surgery: A randomized controlled trial. Br. J. Anaesth. 2017, 119, 900–907. [Google Scholar] [CrossRef]
- Radtke, A.; Lempert, T.; Von Brevern, M.; Feldmann, M.; Lezius, F.; Neuhauser, H. Prevalence and complications of orthostatic dizziness in the general population. Clin. Auton. Res. 2011, 21, 161–168. [Google Scholar] [CrossRef]
- Thomson, P.; Fletcher, I.; Briggs, S.; Barthram, D.; Cato, G. Patient morbidity following oral day surgery—use of a post-operative telephone questionnaire. Ambul. Surg. 2003, 10, 122–127. [Google Scholar] [CrossRef]
- Rosén, H.; Lauzon Clabo, L.M.; Mårtensson, L. Symptoms following day surgery: A review of the literature. J. Adv. Perioper. Care 2009, 4, 7–18. [Google Scholar]
- Kim, T.S.; Choi, S.E.; Won, R.S. Undesirable symptoms of patients in the postanesthesia recovery situation. Korean J. Anesthesiol. 2001, 40, 619. [Google Scholar] [CrossRef]
- Huang, J.; Lin, J.; Xiong, Y.; Wang, Z.; Zhu, Y.; Ye, H.; Guo, W. Risk factors associated with postoperative discomfort after ambulatory strabismus surgery under general anesthesia. J. Pain Res. 2020, 13, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.U. Orthostatic dizziness. Res. Vestib. Sci. 2011, 10, S150–S154. [Google Scholar]
- Smiler, B.G.; Srock, M. Isopropyl alcohol for transport-related nausea. Anesth. Analg. 1998, 87, 1214. [Google Scholar] [CrossRef]
- Kovac, A.L. Prevention and treatment of postoperative nausea and vomiting. Drugs 2000, 59, 213–243. [Google Scholar] [CrossRef] [PubMed]
- Abraham, J. Acupressure and acupuncture in preventing and managing postoperative nausea and vomiting in adults. J. Perioper. Pract. 2008, 18, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Park, Y.H.; Lee, S.E.; Kwak, C.; Kim, H.H. Oncological and surgical outcomes of pure laparoscopic radical nephrectomy and hand-assisted laparoscopic radical nephrectomy for pT1 renal cell carcinoma: Comparison with open radical nephrectomy. Korean J. Urol. 2009, 50, 457–462. [Google Scholar] [CrossRef]
- Gilmartin, J.; Wright, K. The nurse’s role in day surgery: A literature review. Int. Nurs. Rev. 2007, 54, 183–190. [Google Scholar] [CrossRef]
- Williams, S.A.; Schreier, A.M. The effect of education in managing side effects in women receiving chemotherapy for treatment of breast cancer. Oncol. Nurs. Forum 2004, 31, E16–E23. [Google Scholar] [CrossRef]
- Park, J.S.; Lee, H.S. Actual condition, knowledge and attitude of patient controlled analgesics (PCA) in postoperative patients. J. Korean Acad. Fundam. Nurs. 2007, 14, 18–28. [Google Scholar]
- Pridham, K.F.; Hansen, M.F.; Conrad, H.H. Anticipatory care as problem solving in family medicine and nursing. J. Fam. Pract. 1977, 4, 1077–1081. [Google Scholar] [PubMed]
- Cumming, S.; Steel, S.; Barrie, J. Anticipatory care planning in Scotland. Int. J. Integr. Care 2017, 17, 130. [Google Scholar] [CrossRef] [Green Version]
- Galland, B.C.; Sayers, R.M.; Cameron, S.L.; Gray, A.R.; Heath, A.M.; Lawrence, J.A.; Newlands, A.; Taylor, B.J.; Taylor, R.W. Anticipatory guidance to prevent infant sleep problems within a randomised controlled trial: Infant, maternal and partner outcomes at 6 months of age. BMJ Open 2017, 7, e014908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, H.W.; Kim, B.H.; Lee, S.W. Effect of patient controlled analgesia (PCA) education for postoperative patients. J. East West Nurs. Res. 2010, 16, 44–52. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Lee, J.H.; Jo, H.S. Effects of a structured patient controlled analgesia (PCA) education on knowledge and attitude regarding PCA usage, pain, and consumption of analgesics in colorectal surgery patients. J. Korean Clin. Nurs. Res. 2011, 17, 455–466. [Google Scholar]
- Kim, J.H.; Kwon, S.J.; Lee, H.W.; Yoo, H.K. Effectiveness and side effects of postoperative pain control methods in stomach and colorectal cancer patients. J. Korean Surg. Soc. 2004, 67, 41–46. [Google Scholar]
- Chia, Y.-Y.; Kuo, M.-C.; Liu, K.; Sun, G.-C.; Hsieh, S.-W.; Chow, L.-H. Does postoperative pain induce emesis? Clin. J. Pain 2002, 18, 317–323. [Google Scholar] [CrossRef]
- Dingle, M. Role of dangling when moving from supine to standing position. Br. J. Nurs. 2003, 12, 346–350. [Google Scholar] [CrossRef]
- Jin, G.-S.; Li, X.-L.; Jin, Y.-Z.; Kim, M.S.; Park, B.R. Role of peripheral vestibular receptors in the control of blood pressure following hypotension. Korean J. Physiol. Pharmacol. 2018, 22, 363–368. [Google Scholar] [CrossRef]
- Suh, Y.S.; Hong, M.S. A study on distress and state anxiety level in gynecological postoperative patients under PCA management. Korean J. Women Health Nurs. 2004, 10, 351–359. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.; Kim, Y. Factors associated with discontinuation of postoperative intravenous patient controlled analgesia. J. Korean Biol. Nurs. Sci. 2017, 20, 236–243. [Google Scholar] [CrossRef] [Green Version]
- Shin, C. Effect of PCA Education and P6 Acupressure on Postoperative Pain, Nausea and Vomiting of Hysterectomy Patient. Master’s Thesis, Gyeongsang National University, Jinju, Korea, 2004. [Google Scholar]



{kind=link}
{kind=link}
| Item | Experimental Group | Control Group |
|---|---|---|
| Content | Factors causing postoperative nausea, dizziness, and vomiting Deep breathing Effectively using the IV-PCA How to get up in bed to prevent dizziness The need for early ambulation to prevent paralytic ileus | Deep breathing Effectively using the IV-PCA |
| Method | Booklet Tablet PC (video) 1:1 Face-to-face education | Brochure 1:1 Face-to-face education |
| No. and timing of education sessions | 3 times Evening on the day before surgery (30 min) Operative day: upon arrival at the ward (20 min) The next day (before standing up; 15 min) | 2 times Evening on the day before surgery (15 min) Operative day: upon arrival at the ward (15 min) |
| Variable | Category | Experimental (n = 40) No. (%) or Mean ± SD | Control (n = 39) No. (%) or Mean ± SD | t/X2 | p |
|---|---|---|---|---|---|
| Sex | Male | 30 (75.0) | 24 (61.5) | 1.654 | 0.20 |
| Female | 10 (25.0) | 15 (38.5) | |||
| Age (yr) | 48.28 ± 13.64 | 49.00 ± 14.56 | 0.228 | 0.82 | |
| BMI (kg/m2) | 24.83 ± 2.73 | 24.53 ± 3.31 | −0.436 | 0.67 | |
| Eduction | High school | 21 (52.5) | 20 (51.3) | 6.504 | 0.26 |
| Above college | 19 (47.5) | 19 (48.7) | |||
| Religion | Yes | 19 (47.5) | 22 (56.4) | 0.628 | 0.42 |
| No | 21 (52.5) | 17 (43.6) | |||
| Married | Yes | 33 (82.5) | 35 (89.7) | 1.821 | 0.40 |
| No | 7 (17.5) | 4 (10.3) | |||
| Smoking | Yes | 13 (32.5) | 11 (28.2) | 1.154 | 0.56 |
| No | 27 (67.5) | 28 (71.8) | |||
| Menopause | Yes | 3 (30.0) | 7 (46.7) | 0.694 1 | 0.40 |
| No | 7 (70.0) | 8 (53.3) | |||
| Carsickness | Yes No | 2 (5.0) 38 (95.0) | 7 (17.9) 32 (82.1) | 3.524 1 | 0.26 |
| Hyperemesis | Yes No | 4 (50.0) 4 (50.0) | 11 (73.3) 4 (26.7) | 1.252 1 | 0.37 |
| Operation | Open | 3 (7.5) | 5 (12.8) | 0.614 1 | 0.48 |
| Laparotomy | 37 (92.5) | 34 (87.2) | |||
| Anesthesia time (min) | 198.20 ± 44.50 | 212.28 ± 43.97 | 1.353 | 0.18 | |
| Interval from anesthesia start to standing (min) | 1180.85 ± 193.74 | 1144.64 ± 206.95 | −0.803 | 0.42 | |
| IV-PCA (mixed ondansetron) | Yes | 17 (42.5) | 13 (33.3) | 0.704 | 0.40 |
| No | 23 (57.5) | 26 (66.7) | |||
| ASA class | Class 1 | 18 (45.0) | 23 (59.0) | 1.545 | 0.21 |
| Class 2 | 22 (55.0) | 16 (41.0) | |||
| Previous nausea experience | Yes | 3 (5.0) | 2 (5.1) | 0.001 1 | 1.00 |
| No | 38 (95.0) | 37 (94.9) | |||
| Previous anesthesia experience | Yes | 14 (35.0) | 20 (51.3) | 2.135 | 0.14 |
| No | 26 (65.0) | 19 (48.7) | |||
| Nausea | 10 (25.0), 0.90 ± 1.91 | 11 (28.2), 1.21 ± 2.36 | 0.632 | 0.53 | |
| Dizziness | 6 (15.0), 0.60 ± 1.70 | 9 (23.0), 0.77 ± 1.81 | 0.427 | 0.67 | |
| Vomiting | 0 | 0 | / |
| Group | N (%) | Mean ± SD | t, OR | p |
|---|---|---|---|---|
| Nausea | 2.564 | 0.013 | ||
| Experimental (n = 40) | 7 (17.5) | 0.68 ± 1.61 | ||
| Control (n = 39) | 19 (48.7) | 1.95 ± 2.67 | ||
| Vomiting | 0 | 0.900 | ||
| Experimental (n = 40) | 0 | - | ||
| Control (n = 39) | 2 (5.0) | 0.05 ± 0.22 | ||
| Dizziness | 3.689 | <0.001 | ||
| Experimental (n = 40) | 15 (38.0) | 1.45 ± 2.06 | ||
| Control (n = 39) | 30 (77.0) | 3.51 ± 2.84 | ||
| Antiemetic use (from arrival at the ward until 48 hr) | 2.238 | 0.030 | ||
| Experimental (n = 40) | - | 0.42 ± 0.93 | ||
| Control (n = 39) | - | 1.49 ± 2.81 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seok, Y.; Suh, E.E.; Yu, S.-Y.; Park, J.; Park, H.; Lee, E. Effectiveness of Integrated Education to Reduce Postoperative Nausea, Vomiting, and Dizziness after Abdominal Surgery under General Anesthesia. Int. J. Environ. Res. Public Health 2021, 18, 6124. https://doi.org/10.3390/ijerph18116124
Seok Y, Suh EE, Yu S-Y, Park J, Park H, Lee E. Effectiveness of Integrated Education to Reduce Postoperative Nausea, Vomiting, and Dizziness after Abdominal Surgery under General Anesthesia. International Journal of Environmental Research and Public Health. 2021; 18(11):6124. https://doi.org/10.3390/ijerph18116124
Chicago/Turabian StyleSeok, Yoonhee, Eunyoung E. Suh, Soo-Young Yu, JeongYun Park, Hyunjin Park, and Eunsil Lee. 2021. "Effectiveness of Integrated Education to Reduce Postoperative Nausea, Vomiting, and Dizziness after Abdominal Surgery under General Anesthesia" International Journal of Environmental Research and Public Health 18, no. 11: 6124. https://doi.org/10.3390/ijerph18116124