
Treatment of Cardiac Rhabdomyomas with mTOR Inhibitors in Children with Tuberous Sclerosis Complex—A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
- (a)
- P (patients)—children (0–18 years) with TSC and CRs
- (b)
- I (intervention)—treatment with mTORi (everolimus or sirolimus)
- (c)
- C (comparator)—At the beginning, we searched for studies comparing the treatment of CRs with mTORi to surgical intervention or non-intervention. We only found one small retrospective study with a historical control group. Therefore, we had modified the criteria and decided to resign from the comparator criterion.
- (d)
- O (outcome)—size/volume of CRs (if possible to determine), influence on the clinical symptoms caused by CRs, and assessment of side effects associated with mTORi.
- (e)
- S (study design)—Only full-text, original studies disregarding of study type. Only studies published in English or Polish.
2.2. Information Sources
2.3. Search Strategy
2.4. Study Selection
2.5. Data Collection Process and Data Items
2.6. Assessing the Risk of Bias in Individual Studies
2.7. Summary Measures
2.8. Data Analysis
3. Results
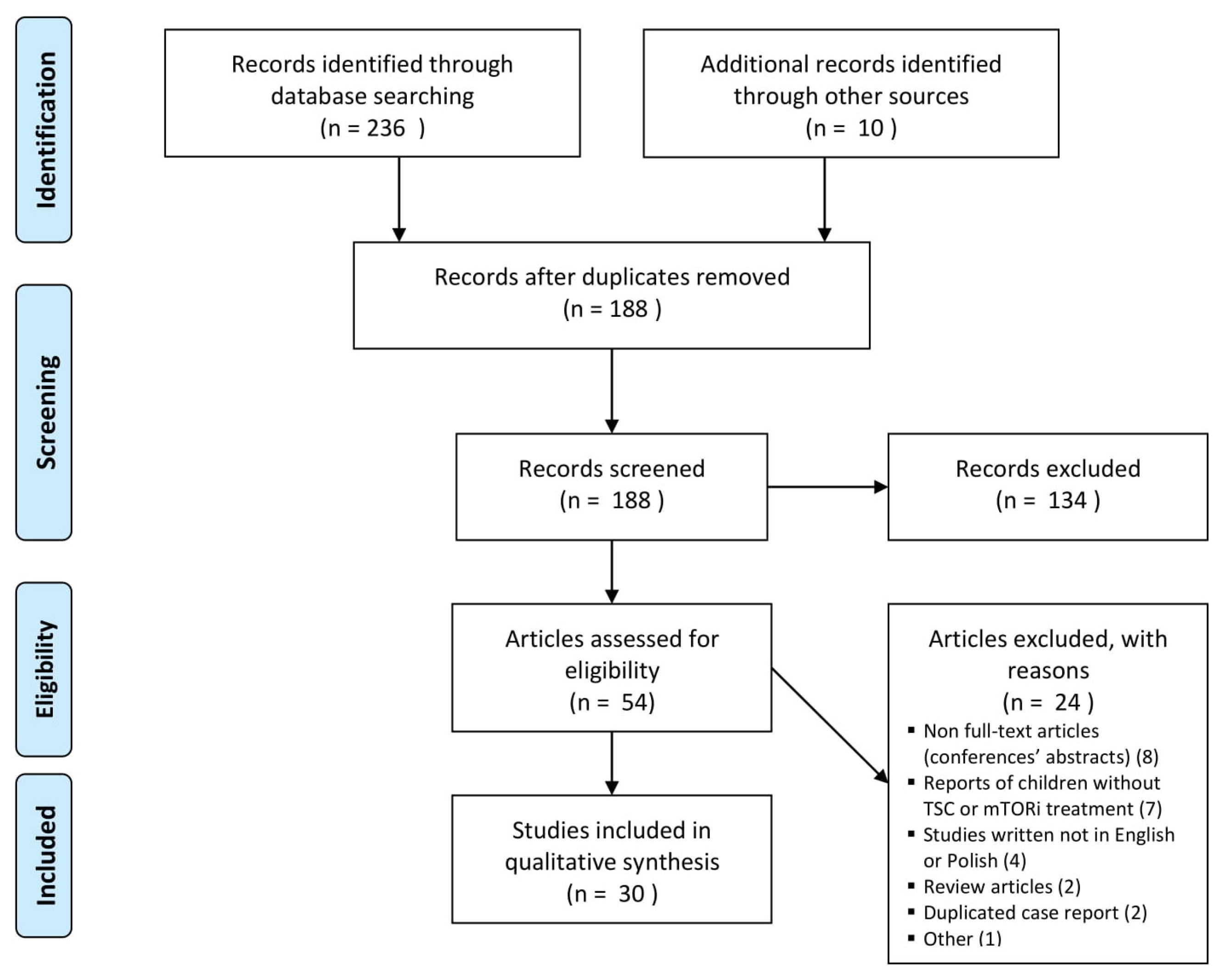
3.1. Study Selection and Available Literature
3.2. Study Characteristics
3.3. Risk of Bias within Studies
3.4. Results of Included Studies
3.4.1. Doses of mTORi
3.4.2. Effect of mTORi on CRs Size
3.4.3. Effect of mTORi on Clinical Symptoms of CRs
3.4.4. CRs Size and Clinical Manifestations after mTORi Discontinuation
3.4.5. Safety Profile of mTORi
3.4.6. Meta-Analysis and Comparison between Everolimus and Sirolimus, and Non-Intervention
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Uzun, O.; Wilson, D.G.; Vujanic, G.M.; Parsons, J.M.; De Giovanni, J.V. Cardiac tumours in children. Orphanetj. Rare Dis. 2007, 2. [Google Scholar] [CrossRef] [Green Version]
- Ebrahimi-Fakhari, D.; Mann, L.L.; Poryo, M.; Graf, N.; von Kries, R.; Heinrich, B.; Ebrahimi-Fakhari, D.; Flotats-Bastardas, M.; Gortner, L.; Zemlin, M.; et al. Incidence of tuberous sclerosis and age at first diagnosis: New data and emerging trends from a national, prospective surveillance study. Orphanetj. Rare Dis. 2018, 13, 117. [Google Scholar] [CrossRef] [PubMed]
- Curatolo, P.; Bombardieri, R.; Jozwiak, S. Tuberous sclerosis. Lancet 2008, 372, 657–668. [Google Scholar] [CrossRef]
- Northrup, H.; Krueger, D.A.; Northrup, H.; Krueger, D.A.; Roberds, S.; Smith, K.; Sampson, J.; Korf, B.; Kwiatkowski, D.J.; Mowat, D.; et al. Tuberous Sclerosis Complex Diagnostic Criteria Update: Recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr. Neurol. 2013, 49, 243–254. [Google Scholar] [CrossRef] [Green Version]
- Tworetzky, W.; McElhinney, D.B.; Margossian, R.; Moon-Grady, A.J.; Sallee, D.; Goldmuntz, E.; Van Der Velde, M.E.; Silverman, N.H.; Allan, L.D. Association between cardiac tumors and tuberous sclerosis in the fetus and neonate. Am. J. Cardiol. 2003, 92, 487–489. [Google Scholar] [CrossRef]
- Sciacca, P.; Giacchi, V.; Mattia, C.; Greco, F.; Smilari, P.; Betta, P.; Distefano, G. Rhabdomyomas and Tuberous sclerosis complex: Our experience in 33 cases. Bmc. Cardiovasc. Disord. 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Słowińska, M.; Kotulska-Jóźwiak, K.; Sadowski, K.; Szymkiewicz-Dangel, J.; Bokiniec, R.; Borszewska-Kornacka, M.; Kawalec, W.; Respondek-Liberska, M.; Werner, B.; Borkowska, J.; et al. Multiple cardiac tumours as a biomarker of tuberous sclerosis complex in children below two years of age. Pediatr. Pol. 2018, 93, 132–138. [Google Scholar] [CrossRef]
- Słowińska, M.; Jóźwiak, S.; Peron, A.; Borkowska, J.; Chmielewski, D.; Sadowski, K.; Jurkiewicz, E.; Vignoli, A.; La Briola, F.; Canevini, M.P.; et al. Early diagnosis of tuberous sclerosis complex: A race against time. How to make the diagnosis before seizures? Orphanetj. Rare Dis. 2018, 13, 25. [Google Scholar] [CrossRef] [Green Version]
- Jóźwiak, S.; Kotulska, K.; Kasprzyk-Obara, J.; Domańska-Pakieła, D.; Tomyn-Drabik, M.; Roberts, P.; Kwiatkowski, D. Clinical and genotype studies of cardiac tumors in 154 patients with tuberous sclerosis complex. Pediatrics 2006, 118. [Google Scholar] [CrossRef]
- Józwiak, S.; Schwartz, R.A.; Janniger, C.K.; Bielicka-Cymerman, J. Usefulness of Diagnostic Criteria of Tuberous Sclerosis Complex in Pediatric Patients. J. Child. Neurol. 2000, 15, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Curatolo, P.; Bjørnvold, M.; Dill, P.E.; Ferreira, J.C.; Feucht, M.; Hertzberg, C.; Jansen, A.; Jóźwiak, S.; Kingswood, J.C.; Kotulska, K.; et al. The Role of mTOR Inhibitors in the Treatment of Patients with Tuberous Sclerosis Complex: Evidence-based and Expert Opinions. Drugs 2016, 76, 551–565. [Google Scholar] [CrossRef]
- Franz, D.N.; Belousova, E.; Sparagana, S.; Bebin, E.M.; Frost, M.; Kuperman, R.; Witt, O.; Kohrman, M.H.; Flamini, J.R.; Wu, J.Y.; et al. Efficacy and safety of everolimus for subependymal giant cell astrocytomas associated with tuberous sclerosis complex (EXIST-1): A multicentre, randomised, placebo-controlled phase 3 trial. Lancet 2013, 381, 125–132. [Google Scholar] [CrossRef]
- Bissler, J.J.; Kingswood, J.C.; Radzikowska, E.; Zonnenberg, B.A.; Frost, M.; Belousova, E.; Sauter, M.; Nonomura, N.; Brakemeier, S.; de Vries, P.J.; et al. Everolimus for angiomyolipoma associated with tuberous sclerosis complex or sporadic lymphangioleiomyomatosis (EXIST-2): A multicentre, randomised, double-blind, placebo-controlled trial. Lancet 2013, 381, 817–824. [Google Scholar] [CrossRef]
- French, J.A.; Lawson, J.A.; Yapici, Z.; Ikeda, H.; Polster, T.; Nabbout, R.; Curatolo, P.; de Vries, P.J.; Dlugos, D.J.; Berkowitz, N.; et al. Adjunctive everolimus therapy for treatment-resistant focal-onset seizures associated with tuberous sclerosis (EXIST-3): A phase 3, randomised, double-blind, placebo-controlled study. Lancet 2016, 388, 2153–2163. [Google Scholar] [CrossRef] [Green Version]
- Davies, D.M.; de Vries, P.J.; Johnson, S.R.; McCartney, D.L.; Cox, J.A.; Serra, A.L.; Watson, P.C.; Howe, C.J.; Doyle, T.; Pointon, K.; et al. Sirolimus Therapy for Angiomyolipoma in Tuberous Sclerosis and Sporadic Lymphangioleiomyomatosis: A Phase 2 Trial. Clin. Cancer Res. 2011, 17, 4071–4081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCormack, F.X.; Inoue, Y.; Moss, J.; Singer, L.G.; Strange, C.; Nakata, K.; Barker, A.F.; Chapman, J.T.; Brantly, M.L.; Stocks, J.M.; et al. Efficacy and Safety of Sirolimus in Lymphangioleiomyomatosis. N. Engl. J. Med. 2011, 364, 1595–1606. [Google Scholar] [CrossRef] [PubMed]
- Franz, D.N.; Budde, K.; Kingswood, J.C.; Belousova, E.; Sparagana, S.; de Vries, P.J.; Berkowitz, N.; Ridolfi, A.; Bissler, J.J. Effect of everolimus on skin lesions in patients treated for subependymal giant cell astrocytoma and renal angiomyolipoma: Final 4-year results from the randomized EXIST-1 and EXIST-2 studies. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1796–1803. [Google Scholar] [CrossRef]
- Koenig, M.K.; Hebert, A.A.; Roberson, J.; Samuels, J.; Slopis, J.; Woerner, A.; Northrup, H. Topical rapamycin therapy to alleviate the cutaneous manifestations of tuberous sclerosis complex: A double-blind, randomized, controlled trial to evaluate the safety and efficacy of topically applied rapamycin. Drugsr. D. 2012, 12, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Bissler, J.J.; McCormack, F.X.; Young, L.R.; Elwing, J.M.; Chuck, G.; Leonard, J.M.; Schmithorst, V.J.; Laor, T.; Brody, A.S.; Bean, J.; et al. Sirolimus for Angiomyolipoma in Tuberous Sclerosis Complex or Lymphangioleiomyomatosis. N. Engl. J. Med. 2008, 358, 140–151. [Google Scholar] [CrossRef] [Green Version]
- Kotulska, K.; Larysz-Brysz, M.; Grajkowska, W.; Jóźwiak, J.; Włodarski, P.; Sahin, M.; Lewin-Kowalik, J.; Domańska-pakieŁa, D.; Jóźwiak, S. Cardiac rhabdomyomas in tuberous sclerosis complex show apoptosis regulation and mTOR pathway abnormalities. Pediatr. Dev. Pathol. 2009, 12, 89–95. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 December 2020).
- Stelmaszewski, E.V.; Parente, D.B.; Farina, A.; Stein, A.; Gutierrez, A.; Raquelo-Menegassio, A.F.; Manterola, C.; De Sousa, C.F.; Victor, C.; Maki, D.; et al. Everolimus for cardiac rhabdomyomas in children with tuberous sclerosis. the ORACLE study protocol (everOlimus for caRdiac rhAbdomyomas in tuberous sCLErosis): A randomised, multicentre, placebo-controlled, double-blind phase II trial. Cardiol. Young 2020, 30, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Aw, F.; Goyer, I.; Raboisson, M.J.; Boutin, C.; Major, P.; Dahdah, N. Accelerated Cardiac Rhabdomyoma Regression with Everolimus in Infants with Tuberous Sclerosis Complex. Pediatr. Cardiol. 2017, 38, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Bornaun, H.; Öztarhan, K.; Erener-Ercan, T.; Dedeoğlu, R.; Tugcu, D.; Aydoğmuş, Ç.; Cetinkaya, M.; Kavuncuoglu, S. Regression of Cardiac Rhabdomyomas in a Neonate after Everolimus Treatment. Case Rep. Pediatr. 2016, 2016, 1–3. [Google Scholar] [CrossRef]
- Hoshal, S.G.; Samuel, B.P.; Schneider, J.R.; Mammen, L.; Vettukattil, J.J. Regression of massive cardiac rhabdomyoma on everolimus therapy. Pediatr. Int. 2016, 58, 397–399. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Lee, N.; Ko, H.; Byun, J.H.; Lee, H.D.; Sung, S.C.; Kim, H.; Choi, K.H. Clinical Manifestations and Outcomes of Cardiac Tumours in Children. HK J. Paediatr. 2019, 24, 140–146. [Google Scholar]
- Knadler, J.J.; Lawrence, E.; Iacobas, I.; Justino, H.; Sheth, S. Combination percutaneous and medical management of cardiac rhabdomyomas obstructing tricuspid valve inflow: Case report. J. Neonatal. Perinatal. Med. 2020, 14, 143–148. [Google Scholar] [CrossRef]
- Lawley, C.; Popat, H.; Wong, M.; Badawi, N.; Ayer, J. A Dramatic Response to Sirolimus Therapy in a Premature Infant With Massive Cardiac Rhabdomyoma. Jacc Case Rep. 2019, 1, 327–331. [Google Scholar] [CrossRef]
- Lee, S.J.; Song, E.S.; Cho, H.J.; Choi, Y.Y.; Ma, J.S.; Cho, Y.K. Rapid Regression of Obstructive Cardiac Rhabdomyoma in a Preterm Neonate after Sirolimus Therapy. Biomed. Hub. 2017, 2, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Lucchesi, M.; Chiappa, E.; Giordano, F.; Mari, F.; Genitori, L.; Sardi, I. Sirolimus in Infants with Multiple Cardiac Rhabdomyomas Associated with Tuberous Sclerosis Complex. Case Rep. Oncol. 2018, 11, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Mao, S.; Long, Q.; Lin, H.; Liu, J. Rapamycin therapy for neonatal tuberous sclerosis complex with cardiac rhabdomyomas: A case report and review. Exp. Ther. Med. 2017, 14, 6159–6163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-García, A.; Michel-Macías, C.; Cordero-González, G.; Escamilla-Sánchez, K.I.; Aguinaga-Ríos, M.; Coronado-Zarco, A.; Cardona-Pérez, J.A. Giant left ventricular rhabdomyoma treated successfully with everolimus: Case report and review of literature. Cardiol. Young 2018, 28, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Mlczoch, E.; Hanslik, A.; Luckner, D.; Kitzmüller, E.; Prayer, D.; Michel-Behnke, I. Prenatal diagnosis of giant cardiac rhabdomyoma in tuberous sclerosis complex: A new therapeutic option with everolimus. Ultrasound Obstet. Gynecol. 2015, 45, 618–621. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, I.; Ethier, G.; Goyer, I.; Major, P.; Dahdah, N. Oral everolimus treatment in a preterm infant with multifocal inoperable cardiac rhabdomyoma associated with tuberous sclerosis complex and a structural heart defect. Bmj Case Rep. 2014, 2014. [Google Scholar] [CrossRef] [Green Version]
- Breathnach, C.; Pears, J.; Franklin, O.; Webb, D.; McMahon, C.J. Rapid regression of left ventricular outflow tract rhabdomyoma after sirolimus therapy. Pediatrics 2014, 134, e1199–e1202. [Google Scholar] [CrossRef] [Green Version]
- Ninic, S.; Kalaba, M.; Jovicic, B.; Vukomanovic, V.; Prijic, S.; Vucetic, B.; Kravljanac, R.; Vujic, A.; Kosutic, J. Successful use of sirolimus for refractory atrial ectopic tachycardia in a child with cardiac rhabdomyoma. Ann. Noninvasive Electrocardiol. 2017, 22, e12435. [Google Scholar] [CrossRef]
- Öztunç, F.; Atik, S.U.; Güneş, A.O. Everolimus treatment of a newborn with rhabdomyoma causing severe arrhythmia. Cardiol Young. 2014, 25, 1411–1414. [Google Scholar] [CrossRef]
- Patel, C.; Abraham, S.; Ferdman, D. Rapid Regression of Prenatally Identified Intrapericardial Giant Rhabdomyomas with Sirolimus. CASE 2018, 2, 258–261. [Google Scholar] [CrossRef] [Green Version]
- Prabhu, N.; Osifodunrin, N.; Murphy, D.; Butler, S.; Hunter, L. Innovative Strategies for the Management of a Massive Neonatal Rhabdomyoma. J. Pediatr. Intensive Care 2017, 7. [Google Scholar] [CrossRef]
- Prasad, K.; Barwad, P.; Santosh, K.; Vijay, J.; Naganur, S. Accelerated regression of cardiac rhabdomyoma by mTOR inhibitors in a neonate with heart failure: A case report. Ihj Cardiovasc. Case Rep. 2020, 4, 142–145. [Google Scholar] [CrossRef]
- Saffari, A.; Brösse, I.; Wiemer-Kruel, A.; Wilken, B.; Kreuzaler, P.; Hahn, A.; Bernhard, M.K.; van Tilburg, C.M.; Hoffmann, G.F.; Gorenflo, M.; et al. Safety and efficacy of mTOR inhibitor treatment in patients with tuberous sclerosis complex under 2 years of age–a multicenter retrospective study. Orphanetj. Rare Dis. 2019, 14, 96. [Google Scholar] [CrossRef] [PubMed]
- Shibata, Y.; Maruyama, H.; Hayashi, T.; Ono, H.; Wada, Y.; Fujinaga, H.; Fujino, S.; Nagasawa, J.; Amari, S.; Tsukamoto, K.; et al. Effect and Complications of Everolimus Use for Giant Cardiac Rhabdomyomas with Neonatal Tuberous Sclerosis. Ajp Rep. 2019, 9, e213–e217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiberio, D.; Franz, D.N.; Phillips, J.R. Regression of a cardiac rhabdomyoma in a patient receiving everolimus. Pediatrics 2011, 127. [Google Scholar] [CrossRef] [PubMed]
- Wagner, R.; Riede, F.T.; Seki, H.; Hornemann, F.; Syrbe, S.; Daehnert, I.; Weidenbach, M. Oral Everolimus for Treatment of a Giant Left Ventricular Rhabdomyoma in a Neonate–Rapid Tumor Regression Documented by Real Time 3D Echocardiography. Echocardiography 2015, 32, 1876–1879. [Google Scholar] [CrossRef] [PubMed]
- Weiland, M.D.; Bonello, K.; Hill, K.D. Rapid regression of large cardiac rhabdomyomas in neonates after sirolimus therapy. Cardiol. Young 2018, 28, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Castro-Monsalve, J.; Alvarado-Socarras, J.L.; Mantilla, K.A.; Forero, L.; Moreno, A.; Prada, C.E. Cardiac Rhabdomyomas in Tuberous Sclerosis Complex. J. Pediatr. 2018, 192, 264–264.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choudhry, S.; Nguyen, H.H.; Anwar, S. Rapid resolution of cardiac rhabdomyomas following everolimus therapy. Bmj Case Rep. 2015, 2015. [Google Scholar] [CrossRef]
- Colaneri, M.; Quarti, A.; Pozzi, M. Everolimus-induced near-resolution of giant cardiac rhabdomyomas and large renal angiomyolipoma in a newborn with tuberous sclerosis complex. Cardiol. Young 2016, 26, 1025–1028. [Google Scholar] [CrossRef]
- Demir, H.A.; Ekici, F.; Erdem, A.Y.; Emir, S.; Tunç, B. Everolimus: A challenging drug in the treatment of multifocal inoperable cardiac rhabdomyoma. Pediatrics 2012, 130. [Google Scholar] [CrossRef] [Green Version]
- Doğan, V.; Yeşi, Ş.; Kayali, Ş.; Beken, S.; Özgür, S.; Ertuğrul, I.; Bozkurt, C.; Örün, U.A.; Karademir, S. Regression of symptomatic multiple cardiac rhabdomyomas associated with tuberous sclerosis complex in a newborn receiving everolimus. J. Trop. Pediatr. 2015, 61, 74–77. [Google Scholar] [CrossRef] [Green Version]
- Garg, A.; Gorla, S.R.; Kardon, R.E.; Swaminathan, S. Rapid Involution of Large Cardiac Rhabdomyomas With Everolimus Therapy. World J. Pediatr. Congenit. Hear. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Goyer, I.; Dahdah, N.; Major, P. Use of mTOR inhibitor everolimus in three neonates for treatment of tumors associated with tuberous sclerosis complex. Pediatr. Neurol. 2015, 52, 450–453. [Google Scholar] [CrossRef]
- Common Terminology Criteria of Adverse Events (CTCAE). Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm (accessed on 13 February 2021).
- FDA Approves Everolimus for Tuberous Sclerosis Complex-Associated Partial-Onset Seizures. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-everolimus-tuberous-sclerosis-complex-associated-partial-onset-seizures (accessed on 20 December 2020).
- EMA: Votubia. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/votubia (accessed on 20 December 2020).
- MacKeigan, J.P.; Krueger, D.A. Differentiating the mTOR inhibitors everolimus and sirolimus in the treatment of tuberous sclerosis complex. Neuro Oncol. 2015, 17, 1550–1559. [Google Scholar] [CrossRef] [PubMed]
- Emoto, C.; Fukuda, T.; Mizuno, T.; Schniedewind, B.; Christians, U.; Adams, D.M.; Vinks, A.A. Characterizing the developmental trajectory of sirolimus clearance in neonates and infants. Cpt Pharmacomet. Syst. Pharmacol. 2016, 5, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Strolin Benedetti, M.; Whomsley, R.; Baltes, E.L. Differences in absorption, distribution, metabolism and excretion of xenobiotics between the paediatric and adult populations. Expert Opin. Drug Metab. Toxicol. 2005, 1, 447–471. [Google Scholar] [CrossRef]
- Sadowski, K.; Kotulska, K.; Jóźwiak, S. Management of side effects of mTOR inhibitors in tuberous sclerosis patients. Pharmacol. Rep. 2016, 68, 536–542. [Google Scholar] [CrossRef]
- Jóźwiak, S.; Kotulska, K.; Berkowitz, N.; Brechenmacher, T.; Franz, D.N. Safety of Everolimus in Patients Younger than 3 Years of Age: Results from EXIST-1, a Randomized, Controlled Clinical Trial. J. Pediatr. 2016, 172, 151–155.e1. [Google Scholar] [CrossRef]
- Bissler, J.J.; Kingswood, J.C.; Radzikowska, E.; Zonnenberg, B.A.; Belousova, E.; Frost, M.D.; Sauter, M.; Brakemeier, S.; de Vries, P.J.; Berkowitz, N.; et al. Everolimus long-term use in patients with tuberous sclerosis complex: Four-year update of the EXIST-2 study. PLoS ONE 2017, 12, e0180939. [Google Scholar] [CrossRef]
- Kotulska, K.; Borkowska, J.; Jóźwiak, S. Possible prevention of tuberous sclerosis complex lesions. Pediatrics 2013, 132, 239–242. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Author, Year | Localization of the Largest or Symptomatic CR | initial Size of the Largest or Symptomatic CR | CR Clinical Symptoms/Reason to Start mTORi | Age at mTORi Introduction | Treatment Duration | Initial mTORi Dose | Follow-Up of mTORi Serum Level | Effect of mTORi on CRs Volume | Effect of mTORi on Clinical Symptoms | Follow-Up Period after mTORi Withdrawal | CRs Volume at the End of Follow-Up | CR Clinical Manifestations at the End of Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aw et al., 2017 [24]; Goyer et al., 2015 [53]; Mlczoch et al., 2015 [34] | ||||||||||||
| 1 | LV | 8 × 7 mm | significant pressure gradient in the LV outflow tract | 1 day | 36 days | 0.1 mg/day (4.5 mg/m2/week), targeted level 5–15 ng/mL | after 10 days; drug level—10.2 ng/mL | After 36 days; 50% reduction of the largest CR, other 3 disappeared | no cardiological symptoms | at least 18 months | progressive increase in CR size: on day 112: CR size was 3.2 × 2.7 mm on day 576: CR size was 6.6 × 4.1 mm | no clinical symptoms |
| 2 | LV | 15 × 9 mm | no clinical symptoms, multiple tumors occupying LV and concern about possible outflow tract obstruction | 4 days | 46 day | 0.1 mg/day (4.5 mg/m2/week); targeted level 5–15 ng/mL | after 6 days; drug level—11 ng/mL | After 22 days; 50% reduction of CR size | remained asymptomatic | at least 7 months | progressive increase in CR size On the 48th day of life—12.4 × 7.8 mm On the 268th day of life–17.5 × 13.2 mm | remained asymptomatic |
| 3 | RV | 11 × 6 mm | SEGA, CR were asymptomatic | 9 days | no data | 0.1 mg/day (4.5 mg/m2/week); targeted level 5–15 ng/mL | after 13 days; drug level −5.4 ng/mL | After 11 days; CR size was 6.5 × 3.1 mm (30–50% reduction) After 1 month; CR was undetectable | remained asymptomatic | still treated with everolimus | - | - |
| 4 | RV | no data | duct dependent RVOT obstruction, heart failure | 21 days | planned for 1 year | 3 mg/m2; targeted level of 4–5 ng/mL | no data | after 28 days; CR regression (no detailed data) | after 3 months; a significant improvement, no obstruction in RVOT | 2 weeks | CR dramatically increased in size (everolimus was re-introduced) | do data |
| Bornaun et al., 2016 [25] | LV, RV | 1.3 cm2 | cyanosis, hypotonia, LV hypertrophy, obstruction of LVOT, mild obstruction of RVOT, inoperable CR | 7 days | overall 6 months | 2 × 0.25 mg twice a week; targeted level 2.6–6.1 ng/mL | drug level varied from 0.4 to 2.6 ng/mL | (1) after 28 days; significant reduction of CR (everolimus was ceased) (2) after 180 days of everolimus reintroduction; marked decrease of CR size | after 4 weeks; resolution of LV outflow tract obstruction | (1) 10 days (after 1st drug withdrawal) (2) 12 months (after 2nd drug withdrawal) | (1) significant regrowth of all CR (2) stable CR size | no data |
| Castro-Monsalve et al., 2018 [47] | IVS | no data | cardiac arrest, severe hemodynamic instability, cardiac failure | neonate | no data | 0.1 mg/day | drug level between 5–8 ng/mL | After 31 days; 60% reduction of CR size After 60 days; resolution of CR | no data | no data | no data | no data |
| Choudhry et al., 2015 [48] | RV, LV | from 3 to 12 mm | SEGA; CR were asymptomatic | neonate | no data | no data | no data | after 30 days; the apparent resolution of all CR (no detailed data) | remained asymptomatic | no data | no data | remained asymptomatic |
| Colaneri et al., 2016 [49] | LV | 40 × 35 × 40 mm (transverse diameter in thorax MRI—35 × 25 mm) | severe reduction of LV volume resulting in duct dependent heart disease, sporadic ventricular extrasystoles, large renal angiomyolipoma; surgery was contraindicated | 7 days | 10 weeks | 0.25 mg/day (0.11 mg/kg; 1.5 mg/m2), targeted level 5–15 ng/mL | after 5 days; drug level—9.1 ng/mL; | After 70 days; CR size—23 × 9 mm in thorax MRI (30–50 % reduction) | after 10 days; extrasystoles disappeared after 3 weeks; normal ventricular function | 9 months | Stable | no clinical symptoms |
| Demir et al., 2012 [50]; | RV, IVS, LV | CR sizes ranged from 5 to 25 mm | cyanosis, RV heart failure, obstruction of RV inflow, CR ineligible for surgery | neonate | 2.5 months | 0.25 mg every 6 h 2 days per week; targeted level 5–15 ng/mL | after 4 doses drug level was 83.5 ng/mL | After 70–75 days; CR remarkably decreased in size (no detailed data) | after 2.5 months; hemodynamic instability improved | 2 months | no data | no clinical symptoms |
| Dogan et al., 2015 [51] | LV | 24 × 21 mm and 22 × 20 mm | cyanosis, LV obstruction, inoperable tumors | neonate | 3 months | 0.25 mg two times per day, 2 days per week; targeted level of 5–15 ng/mL | drug level ranged from 3.6 to 7.8 ng/mL | After 60 days; significant CR reduction | After 2 months; no hemodynamic instability, relief of LV obstruction | 15 months | no data | severe mitral insufficiency, moderate LV dilatation, WPW in ECG |
| Garg et al., 2018 [52] | RV | 40 × 37 × 30 mm | ventricular tachycardia, hypotension, mild/moderate tricuspid insufficiency; high risk of surgery | neonate (around 4–5th day of life) | no data | 0.08 mg/day (0.3 mg/m2/day) | no data | After 14 days; a slight decrease of CR size After 30 days rapid involution of the CR | Significant clinical improvement after a few days of treatment | still treated, but the dose was not weight-adjusted | - | - |
| Hoshal et, 2015 [26] | LV, intrapericardial tumor extending along the aortic root | no data | circulatory collapse, RVOT obstruction, cardiac enlargement, disqualification from the surgery | neonate or infant | more than 10 months | 0.5 mg/day | no data | After 60 days; regression of CR After 300 days; CR almost disappeared | after 2 months; improvement after 10 months; normal LV ejection fraction | no data | no data | no data |
| Kim et al., 2019 [27] | no data | 45 mm | hemodynamically unstable arrhythmia and SEGA | older than 15 months | no data | no data | no data | After 150 days; complete regression of CR | no data | no data | no data | no data |
| Martínez-García et al., 2018 [33] | LV | 47 × 40 mm | Giant CR occupying almost whole LV resulting in duct dependent heart disease, cardiomegaly, incomplete left bundle branch block with severe repolarization disorder | 36 days | no data | 0.25 mg two times per day only 2 days a week | no data | After 90 days; CR size 22 × 29 mm (30–50% reduction) | after 3 months; normal ejection fraction | no data | no data | no data |
| Mohamed et al. 2014 [35] | IVS, RV | 16 × 11 mm | RVOT obstruction with heart failure; high risk of surgery, additional duct dependent heart defect | 20 days | 34 days | 0.1 mg/day (about 4.5 mg/m2/week) targeted level of 5–15 ng/mL | after 11 days; drug level 11 ng/mL | After 34 days; significant reduction of CR | after 34 days; no obstruction of RV outflow tract (the child underwent surgical intervention on the 88th day of life due to a structural heart defect) | 12 months | stable | no clinical symptoms |
| Öztunç et al., 2015 [38] | LV, RV, IVS | no data | pharmacoresistant supraventricular tachycardia | neonate | 4 weeks | 0.25 mg 2 times per day twice a week | no data | After 15 days; CR started to shrink | after 8 days; the frequency and duration of tachycardia diminished | 6 months | stable | no clinical symptoms |
| Prasad et al. 2020 [41] | LV | 31 × 41 mm | congestive heart failure, respiratory dysfunction, LV dysfunction | neonate | 16 weeks | 4.5 mg/kg/m2 weekly | no data | After 70 days; CR size was 9 × 11 mm (>50% reduction) | improvement of respiratory function | no data | no data | no clinical symptoms |
| Saffari et al., 2016 [42] (study reported 8 patients with CR treated with mTORi) | no data | no data | (6 children) symptomatic CR—obstruction of cardiac outflow or arrhythmia; (1 child) SEGA and symptomatic CR; (1 child) SEGA and asymptomatic CR | median age 10.5 days (2 days—5 months); neonates—5 children; infants— 3 children | no data | Infants up to 3 months—doses ranging from 0.05–0.3 mg; infants > 5 months—doses ranging from 1 to 5 mg/day | In 1 patient toxic drug level of around 100 ng/mL after initial dose of 0.4–0.45 mg (1.5–2 mg/m2) | In all patients CR decreased in size | clinical improvement | no data | no data | In one patient recurrence of potentially life-threatening arrhythmia after everolimus cessation. The reintroduction of the drug controlled the arrhythmia |
| Shibata et al., 2019 [43] | RV | 35 × 21 mm | duct dependent obstruction of the LVOT | 4 days | less than 35 days | 0.2 mg/kg/day; targeted level 5–15 ng/mL | on 4th day; drug level: 76.1 ng/mL, drug was transiently withdrawn | After 16 days; CR size—28 × 15 mm (<30% reduction) After 38 days; CR size—24 × 11 mm (30–50% reduction) | after 4 days; resolution of duct dependent heart disease | no data | no data | no data |
| Tibero et al., 2011 [44] | LV | no detailed data | SEGA, CR were asymptomatic | 5 years | 13 months | no data | drug level between 2.3 and 7.1 ng/mL | After13 months; near-resolution of CR | remained asymptomatic | no data | no data | remained asymptomatic |
| Wagner et al., 2015 [45] | LV | 21 × 37 × 21 mm | LVOT obstruction (partially duct dependent) | 2 days | 19 days | 1.5–2 mg/m2; targeted level 5–15 ng/mL | after 4 days; drug level of 108 ng/mL; the drug was stopped for 4 days | After 21 days; CR size—10 × 28 × 13 mm (30–50% reduction) | improvement—prostaglandin infusion was ceased after 2 days of therapy | 5 months | stable | no clinical symptoms |
| Author, Year | Localization of the largest or Symptomatic CR | Initial Size of the Largest or Symptomatic CR | CR Clinical Symptoms/Reason to Start mTORi | Age at mTORi Introduction | Treatment Duration | Initial mTORi Dose | Follow-Up of mTORi Serum Level | Effect of mTORi on CR Volume | Effect of mTORi on Clinical Symptoms | Follow-Up Period after mTORi Withdrawal | CR Volume at the End of Follow-Up | CR Clinical Manifestations at the End of Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Breathnach et al., 2014 [36] | LV | 15 × 12 mm | obstruction of LVOT resulting in temporary duct dependent heart disease; high risk of surgery | 10 days | 24 days | 0.5 mg/once daily; targeted level 20 ng/mL | After 7 days; drug level—26 ng/mL | After 5 days; CR size—7 × 8 mm (30–50% reduction) After 24 days; CR size—5 × 4 mm (>50% reduction) | no cardiological symptoms | 7 months | CR slightly increased in size | no clinical symptoms |
| Knadler J et al., 2020 [28] | RA | (a) 51 mm (b) 8.5 × 8 mm | Duct dependent heart disease due to limited tricuspid valve inflow caused by CR and additional atrial septal defect with right to left shunt | 3 days | until at least 6 months of age | targeted drug level 8–12 ng/mL | initially slightly supratherapeutic drug level (no detailed data) | After 90 days; remarkable reduction of CR size | after 3 months; no cardiological symptoms | no data | no data | no data |
| Lawley et al., 2019 [29] | IVS encroaching on both ventricles | no data | LVOT obstruction, cardiomegaly | 3 days | 2 months | 0.25 mg daily; targeted drug level 5–15 ng/mL | after 8 days; drug level was 69.7 ng/mL (the drug was transiently withdrawn) | After 11 days; significant regression of CR | clinical improvement | (1) 1 month (2) 9 months after sirolimus reintroduction | (1) substantial increase in CR size; (2) sustained reduction of CR size | no data |
| Lee et al., 2017 [30] | LV | 5.2 × 3.6 mm | severe LVOT obstruction, high risk of surgery | 18 days | 10 weeks | 0.25 mg daily | after 14 days; drug level of 42.1 ng/mL; | After 43 days; CR size—2.3 × 1.9 mm (>50% reduction) | after 43 days; no cardiological symptoms | 7 months | no data | no clinical symptoms |
| Lucchesi et al., 2018 [31](the study of 3 consecutive cases) | no data | no data | SEGA in all patients; 1 patient also had a paroxysmal supraventricular tachycardia | less than 12 months—(mean age 7 months) | at least 6 months | 1 mg/m2/day; targeted level 4–10 ng/L | no data | Median time 1.9 months (57 days) (ranged from 0.8 to 4.7 months) In 2 patients complete regression; In 1 patient more than 50% size reduction | no cardiological symptoms | no data | no data | no data |
| Mao et al., 2017 [32] | LA and RV | 1 × 0.89 mm and 1.8 × 1.7 mm | drug-resistant seizures, CR were asymptomatic | 90 days | no data | no data | targeted level of 5–10 ug/l | After 90 days; regression of CR | remained asymptomatic | no data | no data | no data |
| Ninic et al., 2016 [37] | IVS | no data | pharmacoresistant cardiac arrhythmia, slightly diminished LV contractility | 3 years | no data | 1 mg/m2 twice a day | after 5 days; sirolimus level 6.6 ng/mL (within therapeutic range) | no data | after 14 days; normalization of the heart rhythm | no data | no data | no data |
| Patel et al., 2018 [39] | LV pericardium | 30 × 45 mm | small pericardial effusion after birth, decreased LV systolic function, high risk of surgery | neonate | 4 weeks | no data | no data | Significant regression of CR | after 1 week; notable improvement of cardiac function after 4 weeks; LV function normalized | 1 month | stable | no clinical symptoms |
| Prabhu et al., 2018 [40] | originated from LV and extended to RV and RA | no data | respiratory distress, cardiac failure, the patient required ongoing cardiovascular support; ST depression in ECG | neonate | no data | no data | no data | no data | After 48 h, fulminant ventricular ectopy with associated systemic hypotension occured (antiarrhythmic drugs and extracorporeal life support were required) | no data | no data | patient died due to fulminant sepsis and necrotizing enterocolitis |
| Weiland et al., 2018 [46] | ||||||||||||
| 1 | LV, RV—apex (encroaching on the LV and RV) | 25 × 25 × 33 mm | no symptoms, but CR was massive—concern of possible impairment of ventricular function; high risk of surgery | neonate | 4 weeks | initial dose 0.1 mg/kg daily; targeted level of 5–15 ng/mL | at 4th week drug level—22.5 ng/mL drug was ceased | After 28 days; CR size—9 × 9 × 9 mm (>50% reduction) | remained asymptomatic | 9 months | CR size increased to 16 × 12 × 10 mm | remained asymptomatic |
| 2 | LV | (a) 22.1 × 14.5 × 8 mm (b) 10.6 × 9.6 × 9.7 mm | Mild obstruction of the LVOT | neonate | no data | initial dose 0.1 mg/kg every 12 h; targeted level of 5–15 ng/mL | at 12th day; drug level—24.3 ng/mL | After 12 days: (a) CR size—16 × 7 × 10 mm (<30% reduction) (b) CR size—8 × 6 × 5 mm (30–50% reduction) After 6 weeks; (a) 10 × 9 × 7 mm (>50% reduction); (b) 6 × 5 × 5 mm (>50% reduction) | after 12 days; improvement—no evidence of outflow tract obstruction | no data | no data | remained asymptomatic |
| Side Effect | Number of Particular Adverse Events | |
|---|---|---|
| Everolimus | Sirolimus | |
| dyslipidemia (mostly hypertriglicerydemia) | 6 | 3 |
| transient lymphopenia | 3 | 0 |
| infections | 3 | 1 (sepsis) |
| mouth ulcers/mucositis | 2 | 1 |
| acne | 2 | 0 |
| changes in phosphate levels | 2 | 0 |
| increased cholinesterase | 2 | 0 |
| transient neutropenia | 2 | 1 |
| diarrhea/constipation | 1 | 1 |
| transient hypokalemia | 1 | 0 |
| transient anemia | 1 | 0 |
| pulmonary hemorrhage | 1 | 0 |
| elevated liver enzymes | 1 | 0 |
| decreased CD4/CD8 ratio | 1 | 0 |
| hyponatremia | 1 (association with everolimus is doubtful because the patient also received diuretics) | 0 |
| fever without evidence of infection | 0 | 1 |
| none reported (no. of patients) | 7 | 4 |
| no data (no. of studies) | 7 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sugalska, M.; Tomik, A.; Jóźwiak, S.; Werner, B. Treatment of Cardiac Rhabdomyomas with mTOR Inhibitors in Children with Tuberous Sclerosis Complex—A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4907. https://doi.org/10.3390/ijerph18094907
Sugalska M, Tomik A, Jóźwiak S, Werner B. Treatment of Cardiac Rhabdomyomas with mTOR Inhibitors in Children with Tuberous Sclerosis Complex—A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(9):4907. https://doi.org/10.3390/ijerph18094907
Chicago/Turabian StyleSugalska, Monika, Anna Tomik, Sergiusz Jóźwiak, and Bożena Werner. 2021. "Treatment of Cardiac Rhabdomyomas with mTOR Inhibitors in Children with Tuberous Sclerosis Complex—A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 9: 4907. https://doi.org/10.3390/ijerph18094907