
Physical Activity Behaviors and Barriers in Multifetal Pregnancy: What to Expect When You’re Expecting More


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval and Participant Recruitment
2.2. Questionnaire Content
2.3. Questionnaire Analysis
2.3.1. Quantitative Data Analysis
2.3.2. Qualitative Data Analysis
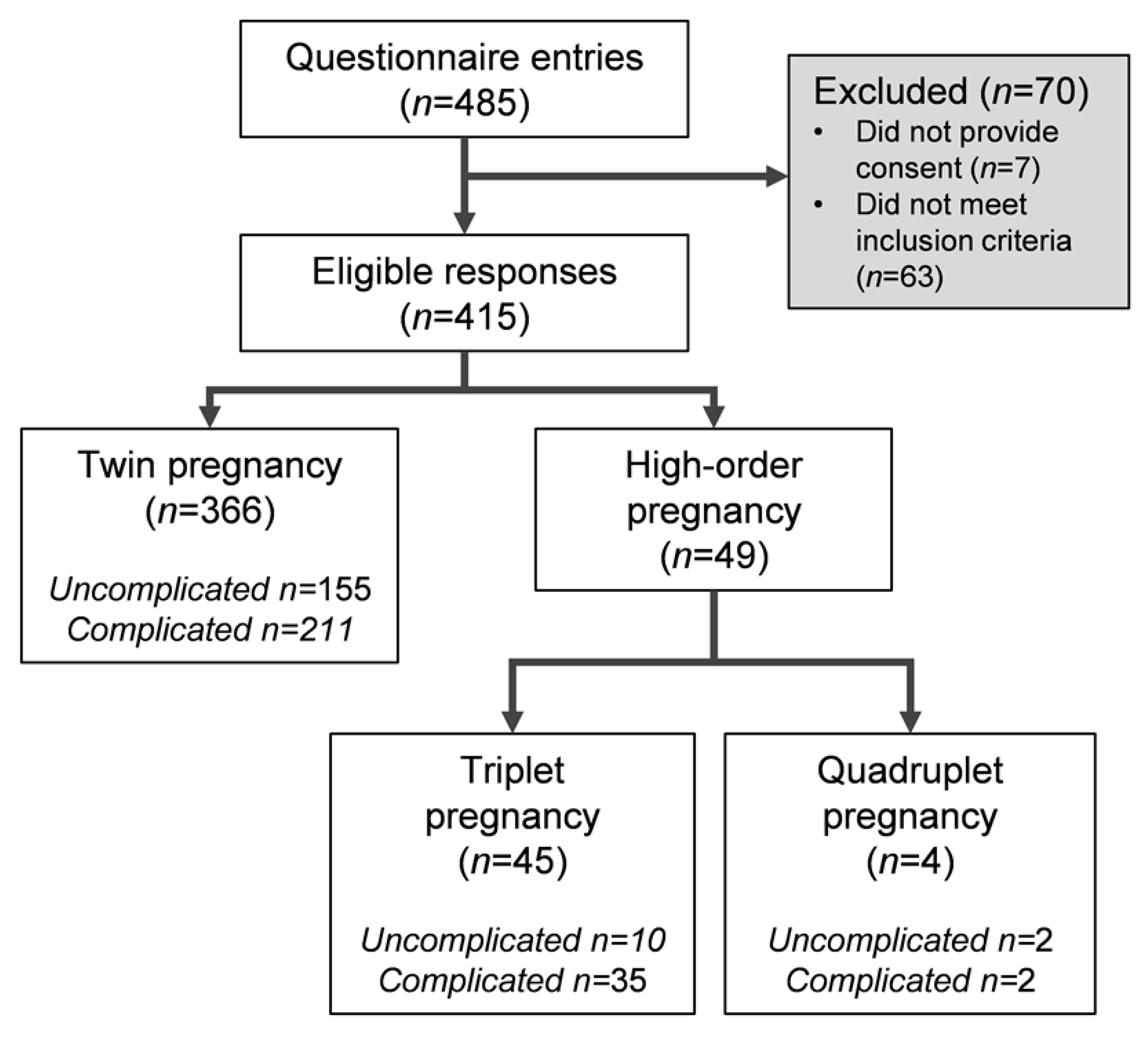
3. Results
3.1. Maternal Demographics
3.2. Birth and Infant Outcomes
3.3. Prenatal Physical Activity Knowledge
3.4. Prenatal Physical Activity Bevahiours
Subgroup Analyses
3.5. Barriers to Physical Activity
Subgroup Analyses
3.6. Activity Restriction and Experience
Subgroup Analyses
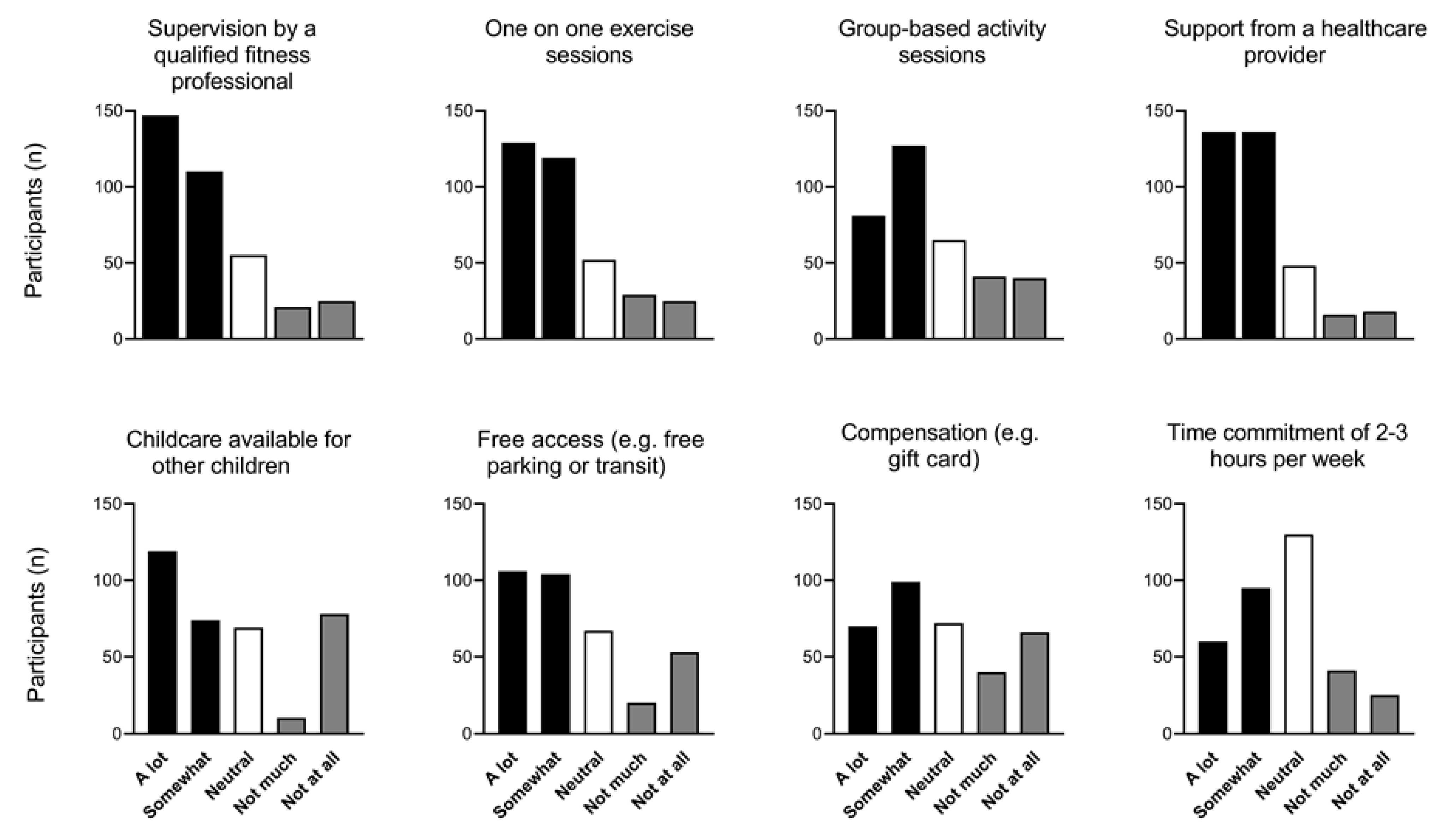
3.7. Research Participation
4. Discussion
Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.; Driscoll, A.K. Births: Final Data for 2018; National Vital Statistics Reports; National Center for Health Statistics: Hyattsville, MD, USA, 2019; pp. 1–47.
- Committee on Practice Bulletins–Obstetrics; Society for Maternal–Fetal Medicine. Practice Bulletin No. 169: Multifetal Gestations: Twin, Triplet, and Higher-Order Multifetal Pregnancies. Obstet. Gynecol. 2016, 128, e131–e146. [Google Scholar] [CrossRef]
- Rabi, D.M.; McBrien, K.A.; Sapir-Pichhadze, R.; Nakhla, M.; Ahmed, S.B.; Dumanski, S.M.; Butalia, S.; Leung, A.A.; Harris, K.C.; Cloutier, L.; et al. Hypertension Canada’s 2020 Comprehensive Guidelines for the Prevention, Diagnosis, Risk Assessment, and Treatment of Hypertension in Adults and Children. Can. J. Cardiol. 2020, 36, 596–624. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Meah, V.L.; Ruchat, S.M.; Davies, G.A.; Skow, R.J.; Barrowman, N.; Adamo, K.B.; Poitras, V.J.; Gray, C.E.; Garcia, A.J.; et al. Impact of prenatal exercise on neonatal and childhood outcomes: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1386–1396. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; McCurdy, A.P.; Mottola, M.F.; Skow, R.J.; Meah, V.L.; Poitras, V.J.; Garcia, A.J.; Gray, C.E.; Barrowman, N.; Riske, L.; et al. Impact of prenatal exercise on both prenatal and postnatal anxiety and depressive symptoms: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1376–1385. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Ruchat, S.M.; Poitras, V.J.; Garcia, A.J.; Gray, C.E.; Barrowman, N.; Skow, R.J.; Meah, V.L.; Riske, L.; Sobierajski, F.; et al. Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1367–1375. [Google Scholar] [CrossRef]
- Ruchat, S.M.; Mottola, M.F.; Skow, R.J.; Nagpal, T.S.; Meah, V.L.; James, M.; Riske, L.; Sobierajski, F.; Kathol, A.J.; Marchand, A.A.; et al. Effectiveness of exercise interventions in the prevention of excessive gestational weight gain and postpartum weight retention: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1347–1356. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Kathol, A.J.; Mottola, M.F.; Skow, R.J.; Meah, V.L.; Poitras, V.J.; Garcia, A.J.; Gray, C.E.; Barrowman, N.; Riske, L.; et al. Prenatal exercise is not associated with fetal mortality: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 108–115. [Google Scholar] [CrossRef]
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.M.; Davies, G.A.; Poitras, V.; Gray, C.; Garcia, A.J.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. No. 367-2019 Canadian Guideline for Physical Activity throughout Pregnancy. J. Obstet. Gynaecol. Can. 2018, 40, 1528–1537. [Google Scholar] [CrossRef]
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.M.; Davies, G.A.; Poitras, V.; Gray, C.; Garcia, A.J.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. N degrees 367-2019 Lignes Directrices Canadiennes Sur L’activite Physique Durant La Grossesse. J. Obstet. Gynaecol. Can. 2018, 40, 1538–1548. [Google Scholar] [CrossRef] [PubMed]
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.M.; Davies, G.A.; Poitras, V.J.; Gray, C.E.; Garcia, A.J.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. 2019 Canadian guideline for physical activity throughout pregnancy. Br. J. Sports Med. 2018, 52, 1339–1346. [Google Scholar] [CrossRef] [Green Version]
- Meah, V.L.; Davies, G.A.; Davenport, M.H. Why can’t I exercise during pregnancy? Time to revisit medical ‘absolute’ and ‘relative’ contraindications: Systematic review of evidence of harm and a call to action. Br. J. Sports Med. 2020, 54, 1395–1404. [Google Scholar] [CrossRef] [PubMed]
- da Silva Lopes, K.; Takemoto, Y.; Ota, E.; Tanigaki, S.; Mori, R. Bed rest with and without hospitalisation in multiple pregnancy for improving perinatal outcomes. Cochrane Database Syst. Rev. 2017, 3, CD012031. [Google Scholar] [CrossRef] [PubMed]
- Fox, N.S.; Gelber, S.E.; Kalish, R.B.; Chasen, S.T. The recommendation for bed rest in the setting of arrested preterm labor and premature rupture of membranes. Am. J. Obstet. Gynecol. 2009, 200, 165.e1–165.e6. [Google Scholar] [CrossRef] [PubMed]
- Maloni, J.A.; Cohen, A.W.; Kane, J.H. Prescription of activity restriction to treat high-risk pregnancies. J. Womens Health 1998, 7, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Matenchuk, B.; Khurana, R.; Cai, C.; Boule, N.G.; Slater, L.; Davenport, M.H. Prenatal bed rest in developed and developing regions: A systematic review and meta-analysis. CMAJ Open 2019, 7, E435–E445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neilson, J.P.; Verkuyl, D.A.; Bannerman, C. Tape measurement of symphysis-fundal height in twin pregnancies. Br. J. Obstet. Gynaecol. 1988, 95, 1054–1059. [Google Scholar] [CrossRef]
- Benute, G.R.; Nozzella, D.C.; Prohaska, C.; Liao, A.; de Lucia, M.C.; Zugaib, M. Twin pregnancies: Evaluation of major depression, stress, and social support. Twin Res. Hum. Genet. 2013, 16, 629–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, A.L.; Taylor, N.F.; Shields, N.; Frawley, H.C. Attitudes, barriers and enablers to physical activity in pregnant women: A systematic review. J. Physiother. 2018, 64, 24–32. [Google Scholar] [CrossRef]
- Hayman, M.; Reaburn, P.; Alley, S.; Cannon, S.; Short, C. What exercise advice are women receiving from their healthcare practitioners during pregnancy? Women Birth 2020, 33, e357–e362. [Google Scholar] [CrossRef]
- De Vivo, M.; Mills, H. “They turn to you first for everything”: Insights into midwives’ perspectives of providing physical activity advice and guidance to pregnant women. BMC Pregnancy Childbirth 2019, 19, 462. [Google Scholar] [CrossRef]
- Whitaker, K.M.; Baruth, M.; Schlaff, R.A.; Talbot, H.; Connolly, C.P.; Liu, J.; Wilcox, S. Provider advice on physical activity and nutrition in twin pregnancies: A cross-sectional electronic survey. BMC Pregnancy Childbirth 2019, 19, 418. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [Green Version]
- Davenport, M.H.; Meyer, S.; Meah, V.L.; Strynadka, M.C.; Khurana, R. Moms Are Not OK: COVID-19 and Maternal Mental Health. Front. Glob. Women’s Health 2020, 1, 1. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Young, B.C.; Wylie, B.J. Effects of twin gestation on maternal morbidity. Semin. Perinatol. 2012, 36, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Wen, S.W.; Demissie, K.; Yang, Q.; Walker, M.C. Maternal morbidity and obstetric complications in triplet pregnancies and quadruplet and higher-order multiple pregnancies. Am. J. Obstet. Gynecol. 2004, 191, 254–258. [Google Scholar] [CrossRef]
- Bryan, E. The impact of multiple preterm births on the family. BJOG 2003, 110 (Suppl. 20), 24–28. [Google Scholar] [CrossRef]
- Sechrist, D.M.; Tiongco, C.G.; Whisner, S.M.; Geddie, M.D. Physiological Effects of Aquatic Exercise in Pregnant Women on Bed Rest. Occup. Ther. Health Care 2015, 29, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Zemet, R.; Schiff, E.; Manovitch, Z.; Cahan, T.; Yoeli-Ullman, R.; Brandt, B.; Hendler, I.; Dorfman-Margolis, L.; Yinon, Y.; Sivan, E.; et al. Quantitative assessment of physical activity in pregnant women with sonographic short cervix and the risk for preterm delivery: A prospective pilot study. PLoS ONE 2018, 13, e0198949. [Google Scholar] [CrossRef]
- Bailey, D.M.; Davies, B.; Budgett, R.; Sanderson, D.C.; Griffin, D. Endurance training during a twin pregnancy in a marathon runner. Lancet 1998, 351, 1182. [Google Scholar] [CrossRef]
- Gao, L.; Lyu, S.P.; Zhao, X.R.; Wu, Y.; Hua, R.Y.; Wang, S.; Zhang, Y.; Wang, Y.L. Systematic management of twin pregnancies to reduce pregnancy complications. Chin. Med. J. 2020, 133, 1355–1357. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, P.J.; Poudevigne, M.S.; Johnson, K.E.; Brito de Araujo, J.; Ward-Ritacco, C.L. Effects of Resistance Training on Fatigue-Related Domains of Quality of Life and Mood During Pregnancy: A Randomized Trial in Pregnant Women with Increased Risk of Back Pain. Psychosom. Med. 2018, 80, 327–332. [Google Scholar] [CrossRef]
- Tan, L.; Zou, J.; Zhang, Y.; Yang, Q.; Shi, H. A Longitudinal Study of Physical Activity to Improve Sleep Quality During Pregnancy. Nat. Sci. Sleep 2020, 12, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Marchand, A.A.; Mottola, M.F.; Poitras, V.J.; Gray, C.E.; Garcia, A.J.; Barrowman, N.; Sobierajski, F.; James, M.; Meah, V.L.; et al. Exercise for the prevention and treatment of low back, pelvic girdle and lumbopelvic pain during pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 90–98. [Google Scholar] [CrossRef] [Green Version]
- Connolly, C.P.; Mudd, L.M.; Pivarnik, J.M. Associations among Work-Related and Leisure-Time Physical Activity with Level of Nausea during Pregnancy. Am. J. Lifestyle Med. 2019, 13, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Owe, K.M.; Stoer, N.; Wold, B.H.; Magnus, M.C.; Nystad, W.; Vikanes, A.V. Leisure-time physical activity before pregnancy and risk of hyperemesis gravidarum: A population-based cohort study. Prev. Med. 2019, 125, 49–54. [Google Scholar] [CrossRef]
- Rubarth, L.B.; Schoening, A.M.; Cosimano, A.; Sandhurst, H. Women’s Experience of Hospitalized Bed Rest During High-Risk Pregnancy. J. Obstet. Gynecol. Neonatal Nurs. 2012, 41, 398–407. [Google Scholar] [CrossRef]
- Grigoriadis, S.; VonderPorten, E.H.; Mamisashvili, L.; Tomlinson, G.; Dennis, C.L.; Koren, G.; Steiner, M.; Mousmanis, P.; Cheung, A.; Radford, K. The impact of maternal depression during pregnancy on perinatal outcomes: A systematic review and meta-analysis. J. Clin. Psychiatry 2013, 74, e321–e341. [Google Scholar] [CrossRef]
- Nagpal, T.S.; Souza, S.C.; da Silva, D.F.; Adamo, K.B. Taking a patient-oriented approach in exercise interventions for pregnant women: A commentary. Can. J. Public Health 2020. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Maternal age at delivery (years) | 32.5 ± 4.6 |
| Gravidity | 2 ± 1 |
| Pre-pregnancy BMI (kg/m2) | 26.2 ± 6.2 |
| Underweight (<18.5 kg/m2) | 7 (2%) |
| Normal weight (18.5–24.9 kg/m2) | 174 (49%) |
| Overweight (25–29.9 kg/m2) | 100 (28%) |
| Obese (>30 kg/m2) | 75 (21%) |
| Gestational weight gain (kg) | 16.5 ± 10.1 |
| Ethnicity (n = 397) † | |
| Asian | 12 (3%) |
| Black or African American | 2 (1%) |
| Caucasian | 361 (91%) |
| First Nations, Inuit, Métis, American Indian, or Alaska Native | 9 (2%) |
| Hispanic of Latinx | 9 (2%) |
| Native Hawaiian or Other Pacific Islander | 2 (1%) |
| Mixed Heritage | 9 (2%) |
| Prefer not to say | 3 (1%) |
| Gender (n = 415) | |
| Female | 408 (98%) |
| Male | 5 (1%) |
| Nonbinary | 1 (<1%) |
| Prefer not to say | 1 (<1%) |
| Education (n = 413) | |
| High school | 26 (6%) |
| College | 2 (0%) |
| Trade, technical, or vocational training | 35 (8%) |
| University certificate/diploma | 52 (13%) |
| Undergraduate degree | 169 (41%) |
| Postgraduate degree | 89 (22%) |
| Professional degree | 38 (9%) |
| Pregnancy type | |
| Zygosity (n = 415) | |
| Monozygotic | 113 (27%) |
| Dizygotic | 276 (67%) |
| Combination (high-order pregnancies only) | 14 (3%) |
| Unsure | 12 (3%) |
| Chorionicity (n = 414) | |
| Monochorionic | 91 (22%) |
| Dichorionic | 299 (72%) |
| Combination (high-order pregnancies only) | 12 (3%) |
| Unsure | 12 (3%) |
| Pregnancy complications (n = 401) † | |
| No complications | 165 (41%) |
| Preterm labor | 71 (18%) |
| Preeclampsia | 60 (15%) |
| Gestational hypertension | 43 (11%) |
| Gestational diabetes mellitus | 45 (11%) |
| Short cervix (with and without cervical cerclage) | 29 (7%) |
| n (%) | MET Minutes Per Week Mean ± SD | |
|---|---|---|
| Prepregnancy physical activity (n = 406) | ||
| “In the year prior to pregnancy, would you describe yourself as physically active?” † | ||
| Yes, most, if not all, of the time | 174 (43%) | |
| Yes, sometimes | 144 (35%) | |
| Yes, but rarely | 46 (11%) | |
| Yes, but never meeting recommendations | 24 (6%) | |
| No | 18 (4%) | |
| Prenatal physical activity (n = 388) | ||
| “During your multiple pregnancy, would you describe yourself as physically active?” ‡ | ||
| Yes, most, if not all, of the time | 64 (16%) | |
| Yes, sometimes | 95 (24%) | |
| Yes, but rarely | 63 (16%) | |
| Yes, but never meeting recommendations | 62 (16%) | |
| No | 104 (27%) | |
| Self-reported prenatal physical activity characteristics | n = 300 | |
| Intensity of activity (METs) | 4.5 ± 2.3 | |
| Frequency of activity (per week) | 3.2 ± 1.9 | |
| Duration of activity (minutes) | 43 ± 34 | |
| Volume of activity (MET·mins·week−1) | 577 ± 758 | |
| Gestational age at cessation (weeks) | 30 ± 9 | |
| Intensity of self-reported prenatal physical activity (n = 677 responses from 300 participants) | ||
| Light (light effort:, e.g., yoga, easy walking, bowling, stretching) | 411 (61%) | 387 ± 402 |
| Moderate (not exhausting, medium effort:, e.g., fast walking, tennis, easy bicycling, breaststroke swimming) | 230 (34%) | 733 ± 646 |
| Strenuous (high effort:, e.g., running, jogging, front crawl swimming, cycling uphill) | 35 (5%) | 1774 ± 2125 |
| Location of prenatal physical activity (n = 490) | ||
| In a facility (e.g., gym, recreation center, yoga studio) | 167 (34%) | |
| At home | 129 (26%) | |
| In local neighborhood | 85 (17%) | |
| At swimming pool | 67 (14%) | |
| In a public park or green space | 31 (6%) | |
| At a sporting facility (e.g., golf course, soccer field) | 11 (2%) |
| n (%) | ||
|---|---|---|
| Barriers (n = 363) † | ||
| I did not experience any barriers | 49 (13%) | |
| Pregnancy symptoms limited motivation | 204 (56%) | |
| Worried about potential risks | 128 (35%) | |
| Lack of time | 86 (24%) | |
| Healthcare provider advised against certain forms of activity | 83 (23%) | |
| Stress, anxiety, and/or low mood | 45 (12%) | |
| Weather | 44 (12%) | |
| Lack of childcare | 38 (10%) | |
| Lack of information about physical activity | 35 (10%) | |
| Lack of access to a gym or equipment | 28 (8%) | |
| Healthcare provider was unsure about physical activity | 16 (4%) | |
| Lack of support from others in life | 5 (1%) | |
| Physical symptoms affecting physical activity levels (n = 383) † | ||
| No symptoms affected my physical activity levels | 20 (5%) | |
| Fatigue | 274 (72%) | |
| Exhaustion/being over-tired | 219 (57%) | |
| Lower back pain | 199 (52%) | |
| Pelvic pain | 185 (48%) | |
| Pregnancy-induced sickness (nausea, vomiting) | 167 (44%) | |
| Shortness of breath | 159 (42%) | |
| General body aches or pains (not specific to lower back or pelvis) | 143 (37%) | |
| Dizziness/light-headedness | 96 (25%) | |
| Stress incontinence | 24 (6%) | |
| Contractions | 10 (3%) | |
| Swelling of lower limbs | 6 (2%) | |
| Overcoming barriers (n = 153) ‡ | ||
| Theme | Example quotes | |
| Social | • People being more understanding of the effects of exercise on multiple pregnancy and stop assuming that multiple pregnancy will be complicated-makes it so much more stressful. • A group of moms to be who were also experiencing twin pregnancy would have been nice. | 28 (18%) |
| Information | • More consistent advice on how much and what types of exercise were beneficial and also which would increase risks (in multifetal pregnancy). • Clearer and more conclusive information on physical activity during a multiple pregnancy. | 28 (18%) |
| Environmental/Access | • (There was) a lack of pools that encouraged prenatal swimming or had classes. I found it difficult (in …) to find a pool that had public swimming at an early time that also encouraged preggos (pregnant individuals) to come on down. • Exercise classes specific to multiple pregnancy. | 28 (18%) |
| Healthcare provider support | • Connection with others having the same experience, more specific information re benefits and risks, more complete advice from doctor. • More discussion with my OB (obstetrician) would have helped. | 19 (12%) |
| Top Themes | n (%) | Example Quotes | |
|---|---|---|---|
| Participant expressed a negative experience | 144 (61%) | ||
| Psychological | 139 (97%) | • It was very difficult. Limited activities lead to depression and feelings of inadequacy. (I had) too much time to focus on pregnancy complications. • I knew that moving my body was a way that I regulated my mood, but I didn’t realize how much it mattered. | |
| Physical | 96 (67%) | • When I went on medical leave, I felt physically worse (…). I just wanted the pregnancy to be over at that point. • Frustrating because I didn’t want to gain excess weight or lose muscle mass because I knew I would be physically restricted postpartum (prolapse, diastasis recti and time issues). | |
| Previous experience | 24 (17%) | • I had been very active prior to getting pregnant. It was hard to go from essentially working out every day to not being able to even walk down my stairs. My mental health took a hit as I used exercise as a stress relief. • Struggled with the emotional and mental aspect of my body not being able to do what it previously could and the need (to) try and keep some time for me. | |
| Participant expressed a positive experience | 62 (26%) | ||
| Psychological | 57 (92%) | • I emotionally felt better because I was “allowed” to take it easy. • I was fine with it. I knew it was temporary and for a good reason. It actually gave me some peace of mind. | |
| Physical | 45 (73%) | • I was physically more at ease • It felt like my body was telling me to slow down and take care of my babies, so I rested and listened. | |
| Work | 6 (10%) | • I was relieved. I was able to take maternity leave a few weeks earlier and not worry about being on my feet all day and possibly jeopardizing the pregnancy we had worked so hard for. | |
| Participant both positive and negative aspects to their experience | 32 (13%) | ||
| Psychological | 32 (100%) | • Initially hard, but I knew what was at stake. I knew I could get my fitness back, but if anything happened to these sweet babies, I wouldn’t be able to cope. • It was hard but I remember thinking I would do anything to keep my babies safe and in as long as possible. | |
| Physical | 27 (84%) | • Felt guilty for not exercising but knew it felt too hard on my body at the time. • I felt useless and restless, but it felt safer for my babies because I was not having so many contractions anymore. | |
| Social | 6 (19%) | • I was able to spend time with family and friends which helped keep my mood positive. • I was okay with it but concerned about caring for my toddler. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meah, V.L.; Strynadka, M.C.; Khurana, R.; Davenport, M.H. Physical Activity Behaviors and Barriers in Multifetal Pregnancy: What to Expect When You’re Expecting More. Int. J. Environ. Res. Public Health 2021, 18, 3907. https://doi.org/10.3390/ijerph18083907
Meah VL, Strynadka MC, Khurana R, Davenport MH. Physical Activity Behaviors and Barriers in Multifetal Pregnancy: What to Expect When You’re Expecting More. International Journal of Environmental Research and Public Health. 2021; 18(8):3907. https://doi.org/10.3390/ijerph18083907
Chicago/Turabian StyleMeah, Victoria L., Morgan C. Strynadka, Rshmi Khurana, and Margie H. Davenport. 2021. "Physical Activity Behaviors and Barriers in Multifetal Pregnancy: What to Expect When You’re Expecting More" International Journal of Environmental Research and Public Health 18, no. 8: 3907. https://doi.org/10.3390/ijerph18083907