
Female Genital Mutilation/Cutting among Somali Women in the U.S. State of Arizona: Evidence of Treatment Access, Health Service Use and Care Experiences


Abstract
:1. Introduction
2. Materials and Methods
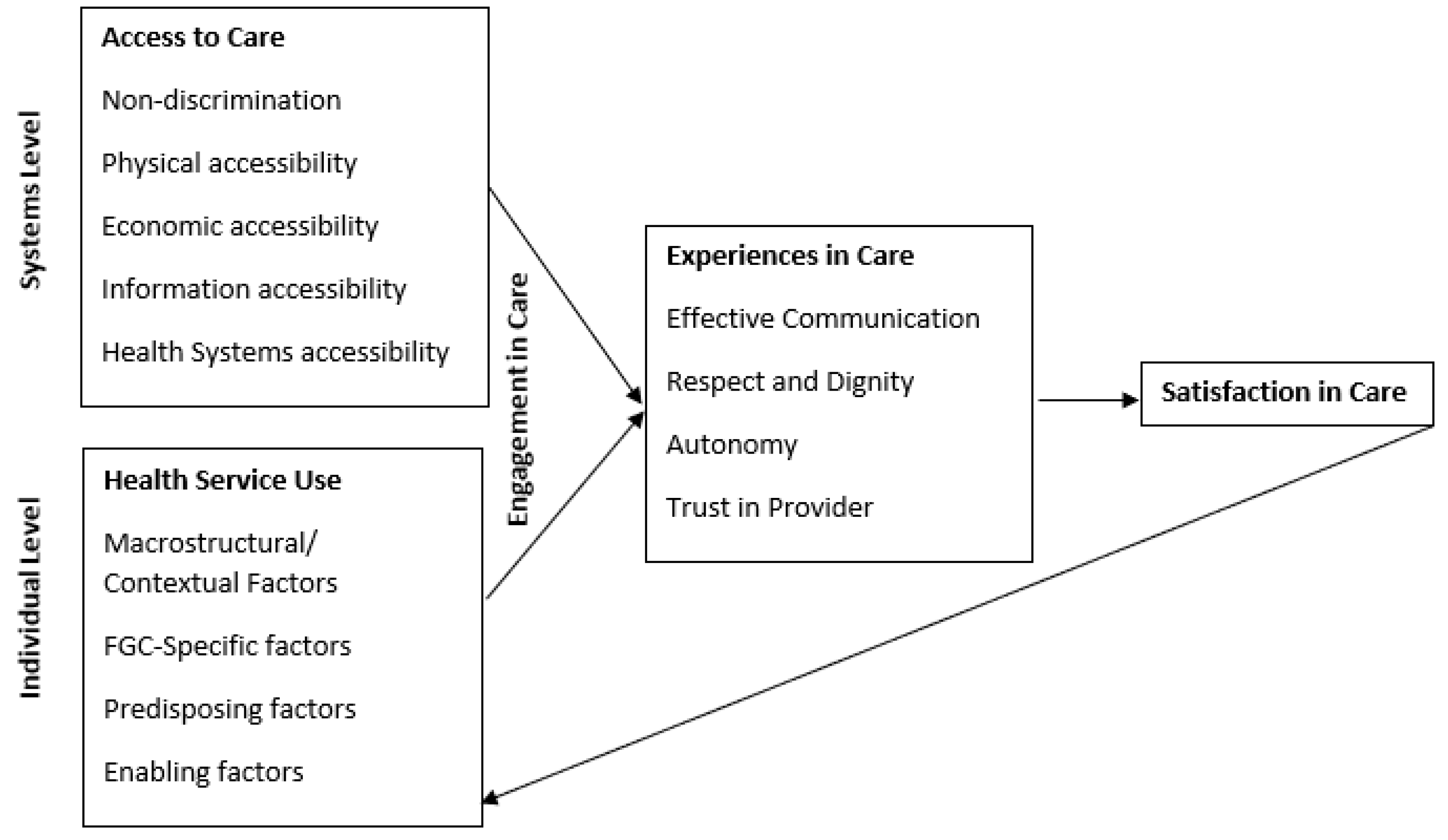
2.1. Conceptual Framework
2.2. Data Collection and Measures
2.3. Data Analysis
3. Results
3.1. Access to Care
3.2. FGM/C-Related Health Service Use
3.3. Care Experiences and Satisfaction in Care
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bureau, U.S.C. American FactFinder-Results. Available online: https://factfinder.census.gov/faces/nav/jsf/pages/index.xhtml (accessed on 4 October 2019).
- Refugee Processing Center. Arrivals by State and Nationality. 2010–2016. Available online: https://www.wrapsnet.org/archives/ (accessed on 10 May 2019).
- Gundel, J. Clans in Somalia; Austrian Red Cross: Vienna, Austria, 2009; Available online: http://www.ecoi.net/file_upload/90_1261130976_accord-report-clans-in-somalia-revised-edition-20091215.pdf (accessed on 31 March 2021).
- Rinehard, B. Clan Structure in Somalia. Comprehensive Information on Complex Crises. 2011. Available online: https://fdocuments.in/document/clan-structure-in-somalia.html (accessed on 31 March 2021).
- US Department of Health and Human Services, Centers for Diseases Control and Prevention, National Center for Emerging and Zoonotic Infectious Diseases, Division of Global Migration and Quarantine. Somali Refugee Health Profile. 15 October 2018. Available online: https://www.cdc.gov/immigrantrefugeehealth/profiles/somali/index.html (accessed on 31 March 2021).
- Lehman, D.V.; Eno, O. The Somali Bantu: Their History and Culture. Culture Profile. 2003. Available online: https://files.eric.ed.gov/fulltext/ED482784.pdf (accessed on 31 March 2021).
- World Health Organization. WHO Guidelines on the Management of Health Complications from Female Genital Mutilation; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- UNICEF. Female Genital Mutilation/Cutting: A Global Concern. 2016. Available online: https://www.unicef.org/media/files/FGMC_2016_brochure_final_UNICEF_SPREAD.pdf (accessed on 31 March 2021).
- Upvall, M.J.; Mohammed, K.; Dodge, P.D. Perspectives of Somali Bantu refugee women living with circumcision in the United States: A focus group approach. Int. J. Nurs. Stud. 2009, 46, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Fried, S.; Warsame, A.M.; Berggren, V.; Isman, E.; Johansson, A. Outpatients’ Perspectives on Problems and Needs Related to Female Genital Mutilation/Cutting: A Qualitative Study from Somaliland. Obstet. Gynecol. Int. 2013, 2013, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Berg, R.C.; Underland, V.; Odgaard-Jensen, J.; Fretheim, A.; Vist, G.E. Effects of female genital cutting on physical health outcomes: A systematic review and meta-analysis. BMJ Open 2014, 4, e006316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulongo, P.; Martin, C.H.; McAndrew, S. The psychological impact of Female Genital Mutilation/Cutting (FGM/C) on girls/women’s mental health: A narrative literature review. J. Reprod. Infant Psychol. 2014, 32, 469–485. [Google Scholar] [CrossRef]
- World Health Organization. Health Risks of Female Genital Mutilation (FGM); World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Olenja, J. Editorial Health seeking behaviour in context. East Afr. Med. J. 2004, 80, 61–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, P.Q.; Hwang, S.H. Explaining Immigrant Health Service Utilization: A Theoretical Framework. SAGE Open 2016, 6. [Google Scholar] [CrossRef] [Green Version]
- Johnsdotter, S. The Impact of Migration on Attitudes to Female Genital Cutting and Experiences of Sexual Dysfunction Among Migrant Women with FGC. Curr. Sex. Health Rep. 2018, 10, 18–24. [Google Scholar] [CrossRef] [Green Version]
- Doucerain, M.M.; Segalowitz, N.; Ryder, A.G. Acculturation measurement: From simple proxies to sophisticated toolkit. In Oxford Handbook of Acculturation and Health; Oxford University Press: New York, NY, USA, 2017. [Google Scholar]
- Bourhis, R.Y.; Moise, L.C.; Perreault, S.; Senecal, S. Towards an Interactive Acculturation Model: A Social Psychological Approach. Int. J. Psychol. 1997, 32, 369–386. [Google Scholar] [CrossRef]
- Hagi Salaad, M.F.; Lahr, B.D.; Flynn, P.M.; Wieland, M.L. Provider and interpreter preferences among Somali women in a primary care setting. J. Prim. Care Community Health 2015, 6, 105–110. [Google Scholar]
- Pavlish, C.L.; Noor, S.; Brandt, J. Somali immigrant women and the American health care system: Discordant beliefs, divergent expectations, and silent worries. Soc. Sci. Med. 2010, 71, 353–361. [Google Scholar] [CrossRef] [Green Version]
- Jacoby, S.D.; Lucarelli, M.; Musse, F.; Krishnamurthy, A.; Salyers, V. A mixed-methods study of immigrant Somali women’s health literacy and perinatal experiences in Maine. J. Midwifery Womens Health 2015, 60, 593–603. [Google Scholar] [CrossRef]
- Windau-Melmer, T. A Guide for Advocating for Respectful Maternity Care. Washington, DC: Futures Group, Health Policy Project. 2013. Available online: https://www.healthpolicyproject.com/pubs/189_RMCGuideFINAL.pdf (accessed on 31 March 2021).
- UN Committee on Economic, Social and Cultural Rights (CESCR). General Comment No. 14: The Right to the Highest At-tainable Standard of Health (Art 12 of the Covenant). 11 August 2000. Available online: http://docstore.ohchr.org/SelfServices/FilesHandler.ashx?enc=4slQ6QSmlBEDzFEovLCuW1AVC1NkPsgUedPlF1vfPMJ2c7ey6PAz2qaojTzDJmC0y%2B9t%2BsAtGDNzdEqA6SuP2r0w%2F6sVBGTpvTSCbiOr4XVFTqhQY65auTFbQRPWNDxL (accessed on 31 March 2021).
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1. [Google Scholar] [CrossRef] [PubMed]
- Tunçalp, Ö.; Were, W.M.; MacLennan, C.; Oladapo, O.T.; Gülmezoglu, A.M.; Bahl, R.; Daelmans, B.; Mathai, M.; Say, L.; Kristensen, F.; et al. Quality of care for pregnant women and newborns—the WHO vision. BJOG 2015, 122, 1045–1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohren, M.A.; Vogel, J.P.; Hunter, E.C.; Lutsiv, O.; Makh, S.K.; Souza, J.P.; Aguiar, C.; Coneglian, F.S.; Diniz, A.L.A.; Tunçalp, Ö.; et al. The Mistreatment of Women during Childbirth in Health Facilities Globally: A Mixed-Methods Systematic Review. PLoS Med. 2015, 12, e1001847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, K.A.; Johnson-Agbakwu, C. Crime Victimization, Health, and Female Genital Mutilation or Cutting Among Somali Women and Adolescent Girls in the United States, 2017. Am. J. Public Health 2020, 110, 112–118. [Google Scholar] [CrossRef]
- Johnson, C.E.; Ali, S.A.; Shipp, M.P.-L. Building Community-Based Participatory Research Partnerships with a Somali Refugee Community. Am. J. Prev. Med. 2009, 37, S230–S236. [Google Scholar] [CrossRef]
- Johnson-Agbakwu, C.E.; Helm, T.; Killawi, A.; Padela, A.I. Perceptions of obstetrical interventions and female genital cutting: Insights of men in a Somali refugee community. Ethn. Health 2013, 19, 440–457. [Google Scholar] [CrossRef]
- Johnson-Agbakwu, C. Female Genital Mutilation/Cutting: Healthcare Experiences and Prevention Efforts from the U.S. Context. Abstract in: Female genital mutilation/cutting: Sharing data and experiences to accel-erate eradication and improve care: Part 2. Reprod. Health 2017, 14 (Suppl. 2), 115. [Google Scholar] [CrossRef] [Green Version]
- Johnson-Agbakwu, C.E.; Allen, J.; Nizigiyimana, J.F.; Ramirez, G.; Hollifield, M. Mental health screening among newly arrived refugees seeking routine obstetric and gynecologic care. Psychol. Serv. 2014, 11, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Hollifield, M.; Toolson, E.C.; Verbillis-Kolp, S.; Farmer, B.; Yamazaki, J.; Woldehaimanot, T.; Holland, A. Effective screening for emotional distress in refugees: The refugee health screener. J. Nerv. Ment. Dis. 2016, 204, 247–253. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toubia, N. FC/FGM Full Color Quick Reference Chart; Research Action and Information Network for Bodily Integrity of Women: New York, NY, USA, 1999; ISBN 1-893136-02-7. [Google Scholar]
- Johnson-Agbakwu, C.E.; Flynn, P.; Asiedu, G.B.; Hedberg, E.; Breitkopf, C.R. Adaptation of an Acculturation Scale for African Refugee Women. J. Immigr. Minority Health 2014, 18, 252–262. [Google Scholar] [CrossRef] [Green Version]
- Szapocznik, J.; Kurtines, W.M.; Fernandez, T. Bicultural involvement and adjustment in Hispanic-American youths. Int. J. Intercult. Relat. 1980, 4, 353–365. [Google Scholar] [CrossRef]
- Berry, J.W. Immigration, acculturation, and adaptation. Appl. Psychol. 1997, 46, 5–34. [Google Scholar] [CrossRef]
- Gordon, M.M. Assimilation in American Life: The Role of Race, Religion, and National Origins; Oxford University Press on Demand: Oxford, UK, 1964. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 14; StataCorp LP: College Station, TX, USA, 2015. [Google Scholar]
- National Center for Health Statistics. FastStats—Access to Health Care. 2018. Available online: https://www.cdc.gov/nchs/fastats/access-to-health-care.htm (accessed on 4 October 2019).
- Lien, I.-L.; Schultz, J.-H. Internalizing Knowledge and Changing Attitudes to Female Genital Cutting/Mutilation. Obstet. Gynecol. Int. 2013, 2013, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Banks, E.; Meirik, O.; Farley, T.M.M.; Akande, O.O.; Bathija, H.; Ali, M.M.; Fahmy, A. Female genital mutilation and obstetric outcome: WHO collaborative prospective study in six African countries. Lancet 2006, 367, 1835–1841. [Google Scholar] [CrossRef]
- World Health Organization. Care of Women and Girls Living with Female Genital Mutilation: A Clinical Handbook; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Johnson-Agbakwu, C.E.; Manin, E. Sculptors of African Women’s Bodies: Forces Reshaping the Embodiment of Female Genital Cutting in the West. Arch. Sex. Behav. 2020, 2020, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, S.; LaLonde, A. The global epidemic of abuse and disrespect during childbirth: History, evidence, interventions, and FIGO’s mother-baby friendly birthing facilities initiative. Int. J. Gynecol. Obstet. 2015, 131, S49–S52. [Google Scholar] [CrossRef] [Green Version]
- Alliance for Innovation on Maternal Health, Council on Patient Safety in Women’s Health Care. AIM Program. 2019. Available online: https://safehealthcareforeverywoman.org/aim/ (accessed on 4 October 2019).
- Evans, C.; Tweheyo, R.; McGarry, J.; Eldridge, J.; Albert, J.; Nkoyo, V.; Higginbottom, G. Improving care for women and girls who have undergone female genital mutilation/cutting: Qualitative systematic reviews. Health Serv. Deliv. Res. 2019, 7, 1–216. [Google Scholar] [CrossRef]
- Hamid, A.; Grace, K.T.; Warren, N. A Meta-Synthesis of the Birth Experiences of African Immigrant Women Affected by Female Genital Cutting. J. Midwifery Women’s Health 2018, 63, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Abdulcadir, J.; Botsikas, D.; Bolmont, M.; Bilancioni, A.; Djema, D.A.; Demicheli, F.B.; Yaron, M.; Petignat, P. Sexual Anatomy and Function in Women with and Without Genital Mutilation: A Cross-Sectional Study. J. Sex. Med. 2016, 13, 226–237. [Google Scholar] [CrossRef]
- Childbirth Connection. How do Childbearing Experiences Differ across Racial and Ethnic Groups in the United States. A Lis-tening to Mothers III Data Brief. [Blog Post]. Transforming Maternity Care. Available online: https://www.nationalpartnership.org/our-work/health/maternity/listening-to-mothers.html (accessed on 31 March 2021).


{kind=link}
| % | n | M | SD | Range | |
|---|---|---|---|---|---|
| Age (years) | 31.15 | 13.8 | 15–90 | ||
| Ethnicity | |||||
| Ethnic Somali | 73.7 | 631 | |||
| Somali Bantu | 26.3 | 225 | |||
| Context of Emigration | |||||
| Involuntary migration (refugee) | 78.3 | 611 | |||
| Voluntary migration | 16 | 125 | |||
| U.S. Born | 5.6 | 44 | |||
| Years in the U.S. | 8.67 | 6.85 | 0–47 | ||
| Education | |||||
| None | 25.3 | 217 | |||
| Any | 74.7 | 641 | |||
| Primary | 16.1 | 138 | |||
| High School | 42.2 | 362 | |||
| College | 16.4 | 141 | |||
| Acculturation | |||||
| Bicultural | 12.1 | 106 | |||
| Acculturated | 36.1 | 316 | |||
| Traditional | 33.3 | 291 | |||
| Hypocultural | 18.5 | 162 | |||
| Household size | |||||
| 1 | 8.3 | 71 | |||
| 2 | 13.6 | 116 | |||
| 3–5 | 39.3 | 335 | |||
| 6+ | 38.8 | 331 | |||
| Annual Household Income | |||||
| <10,000 USD | 41.4 | 247 | |||
| 10–24,999 USD | 38.8 | 231 | |||
| >25,000 USD | 19.8 | 106 | |||
| Self-rated health | |||||
| Excellent | 53.4 | 463 | |||
| Very Good | 24.1 | 209 | |||
| Good | 16.8 | 146 | |||
| Fair | 4.9 | 43 | |||
| Poor | 0.1 | 6 | |||
| Sought medical care for FGM/C-related health ever | |||||
| Yes | 14.4 | 98 | |||
| No | 85.6 | 589 | |||
| Insurance | |||||
| None | 9.2 | 78 | |||
| Public | 82.6 | 703 | |||
| Private | 8.2 | 70 | |||
| FGM/C Status | |||||
| Uncircumcised | 22.6 | 199 | |||
| Circumcised | 77.4 | 680 | |||
| FGM/C Type * | |||||
| Type I | 36.9 | 223 | |||
| Type II | 23 | 139 | |||
| Type III | 40.1 | 243 | |||
| Age of circumcision | 7.09 | 2.27 | 0–15 | ||
| Recall experiencing health problems at the time of circumcision | |||||
| Yes | 26.7 | 143 | |||
| No | 73.3 | 393 | |||
| Regret being circumcised | |||||
| Yes | 25.7 | 173 | |||
| No | 74.3 | 500 | |||
| Had choice whether to be circumcised | |||||
| Yes | 10.1 | 69 | |||
| No | 89.9 | 613 |
| Dimension of Access | N (%) | FGM/C Health Service Use | Satisfaction in Care |
|---|---|---|---|
| Unadjusted OR (95% CI) | Unadjusted OR (95% CI) | ||
| Non-discrimination | |||
| Believe women with FGM/C discriminated against | 136 (16.1) | 1.89 (1.10–3.26) * | 0.22 (0.13–0.37) * |
| Physical Access | |||
| Did not have transportation | 5 (0.7) | ** | ** |
| Economic Access | |||
| Could not afford FGM/C care | 6 (0.9) | ** | ** |
| Insurance would not approve | 16 (2.4) | 0.84 (0.19–3.78) | 0.14 (0.05–0.41) * |
| Informational Access | |||
| Know where to access health care for FGM/C concerns | 490 (75.2) | 1.79 (1.01–3.16) * | 6.32 (3.82–10.45) * |
| Health System Accessibility | |||
| Could not receive referral | 24 (3.5) | 1.59 (0.58–4.37) | 0.10 (0.04–0.23) * |
| Could not find specialist | 39 (5.7) | 1.32 (0.57–3.09) | 0.08 (0.04–0.15) * |
| Could not get appointment | 2 (0.3) | ** | ** |
| Model A | Model B | Model C | Model D | ||
|---|---|---|---|---|---|
| Macrostructural | FGM/C–Specific | Predisposing | Final | ||
| Unadjusted | Adjusted (n = 649) | Adjusted (n = 553) | Adjusted (n = 636) | Adjusted (n = 564) | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Age (covariate) | 1.02 (1.00–1.03) * | 1.02 (1.00–1.03) * | 1.01 (0.99–1.03) | 1.00 (0.98–1.02) | 1.00 (0.98–1.02) |
| Macrostructural/Contextual Factors | |||||
| Perceived discrimination | 1.71 (1.02–2.88) * | 1.89 (1.10–3.26) * | 1.67 (0.79–3.55) | ||
| Involuntary migration | 5.26 (2.09–13.21) * | 5.58 (2.19–14.2) * | 1.48 (0.54–4.03) | ||
| FGM/C Specific Factors | |||||
| FGM/C Type | |||||
| Type I | Ref | Ref | |||
| Type II | 0.78 (0.39–1.58) | 0.53 (0.25–1.16) | |||
| Type III | 2.11 (1.27–3.52) * | 1.20 (0.66–2.20) | |||
| Recall physical/mental sequela | 4.42 (2.80–6.96) * | 3.47 (2.01–5.99) * | 3.09 (1.67–5.68) * | ||
| Regret being circumcised | 2.18 (1.39–3.41) * | 1.15 (0.66–1.99) | |||
| Had choice whether or not circumcised | 0.25 (0.08–0.80) * | 0.26 (0.06–1.12) | |||
| Predisposing Factors | |||||
| Education | |||||
| None | Ref | ||||
| Any | 1.57 (0.92–2.68) | ||||
| Ethnicity | |||||
| Ethnic Somali | Ref | Ref | Ref | ||
| Somali Bantu | 0.14 (0.06–0.36) * | 0.15 (0.06–0.39) * | 0.10 (0.02–0.44) * | ||
| Acculturation | |||||
| Traditional | Ref | Ref | Ref | ||
| Acculturated | 0.31 (0.17–0.59) * | 0.28 (0.15–0.54) * | 0.39 (0.17–0.86) * | ||
| Bicultural | 0.64 (0.33–1.24) | 0.61 (0.31–1.20) | 0.61 (0.25–1.47) | ||
| Hypocultural | 0.29 (0.13–0.66) * | 0.28 (0.12–0.65) * | 0.27 (0.10–0.70) * | ||
| Cannot get preferred physician gender | 5.84 (0.78–43.87) | ||||
| Years in US | 0.98 (0.94–1.01) | ||||
| Enabling Factors | |||||
| Income | |||||
| <10,000 USD | Ref | ||||
| 10–24,999 USD | 1.57 (0.92–2.66) | ||||
| >25,000 USD | 1.20 (0.61–2.36) | ||||
| Insurance (y/n) | 2.37 (0.84–6.69) | ||||
| Household size | |||||
| 1 | Ref | Ref | |||
| 2 | 1.16 (0.51–2.63) | 1.25 (0.44–3.53) | |||
| 3–5 | 0.66 (0.32–1.39) | 0.69 (0.27–1.78) | |||
| 6+ | 0.40 (0.20–0.88) * | 0.48 (0.18–1.31) | |||
| N (%) | Unadjusted | |
|---|---|---|
| OR (95%CI) | ||
| Effective Communication | ||
| Confidence in ability to advocate for the FGM/C–care desired | ||
| A great deal of confidence | 475 (59.4) | Ref |
| Some confidence | 192 (24.0) | 0.33 (0.15–0.70) * |
| Very little confidence | 70 (8.8) | 0.06 (0.03–0.14) * |
| No confidence | 63 (7.9) | 0.02 (0.01–0.04) * |
| Comfortable discussing FGM/C–related problems with provider | ||
| No | 137 (20.9) | Ref |
| Yes | 518 (79.1) | 6.94 (4.17–11.56) * |
| Respect and Dignity | ||
| How much respect and dignity did your provider treat you with related to your circumcision | ||
| A great deal | 490 (62.9) | Ref |
| A fair amount | 200 (25.7) | 0.26 (0.13–0.50) * |
| Not too much | 37 (4.8) | 0.05 (0.02–0.11) * |
| None at all | 52 (6.7) | 0.02 (0.01–0.04) * |
| In your opinion, are women with FGM/C looked down on/ discriminated against by providers | ||
| No | 709 (83.9) | Ref |
| Yes | 136 (16.1) | 0.22 (0.13–0.37) * |
| Autonomy | ||
| Have choice in where to receive care | ||
| A great deal of choice | 546 (65.2) | Ref |
| Some choice | 170 (20.3) | 0.25 (0.14–0.45) * |
| Very little choice | 65 (7.8) | 0.13 (0.06–0.28) * |
| No choice | 57 (6.8) | 0.11 (0.05–0.23) * |
| Have choice in provider | ||
| A great deal of choice | 499 (59.8) | Ref |
| Some choice | 185 (22.2) | 0.17 (0.09–0.31) * |
| Very little choice | 89 (10.7) | 0.08 (0.04–0.17) * |
| No choice | 62 (7.4) | 0.12 (0.05–0.27) * |
| Have choice in type of services receive | ||
| A great deal of choice | 512 (61.1) | Ref |
| Some choice | 186 (22.2) | 0.20 (0.11–0.37) * |
| Very little choice | 81 (9.7) | 0.08 (0.04–0.17) * |
| No choice | 59 (7.0) | 0.12 (0.05–0.28) * |
| Feel able to freely express desires regarding circumcision management with provider | ||
| No | 194 (29.4) | Ref |
| Yes | 467 (70.6) | 6.18 (3.69–10.35) * |
| Trust in Provider | ||
| Trust provider to give good quality care in addressing FGM/C concerns | ||
| No | 211 (26.4) | Ref |
| Yes | 589 (73.6) | 10.50 (6.28–17.55) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michlig, G.; Warren, N.; Berhe, M.; Johnson-Agbakwu, C. Female Genital Mutilation/Cutting among Somali Women in the U.S. State of Arizona: Evidence of Treatment Access, Health Service Use and Care Experiences. Int. J. Environ. Res. Public Health 2021, 18, 3733. https://doi.org/10.3390/ijerph18073733
Michlig G, Warren N, Berhe M, Johnson-Agbakwu C. Female Genital Mutilation/Cutting among Somali Women in the U.S. State of Arizona: Evidence of Treatment Access, Health Service Use and Care Experiences. International Journal of Environmental Research and Public Health. 2021; 18(7):3733. https://doi.org/10.3390/ijerph18073733
Chicago/Turabian StyleMichlig, Georgia, Nicole Warren, Merry Berhe, and Crista Johnson-Agbakwu. 2021. "Female Genital Mutilation/Cutting among Somali Women in the U.S. State of Arizona: Evidence of Treatment Access, Health Service Use and Care Experiences" International Journal of Environmental Research and Public Health 18, no. 7: 3733. https://doi.org/10.3390/ijerph18073733