
Ambient Air Pollution and Cardiorespiratory Outcomes amongst Adults Residing in Four Informal Settlements in the Western Province of South Africa

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Population and Sampling
2.2. Questionnaire
2.3. Outcome Characterisation
2.4. Exposure Characterisation
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
3.1. Demographic Characteristics of the Study Participants
3.2. Cardiorespiratory Outcomes of the Study Participants
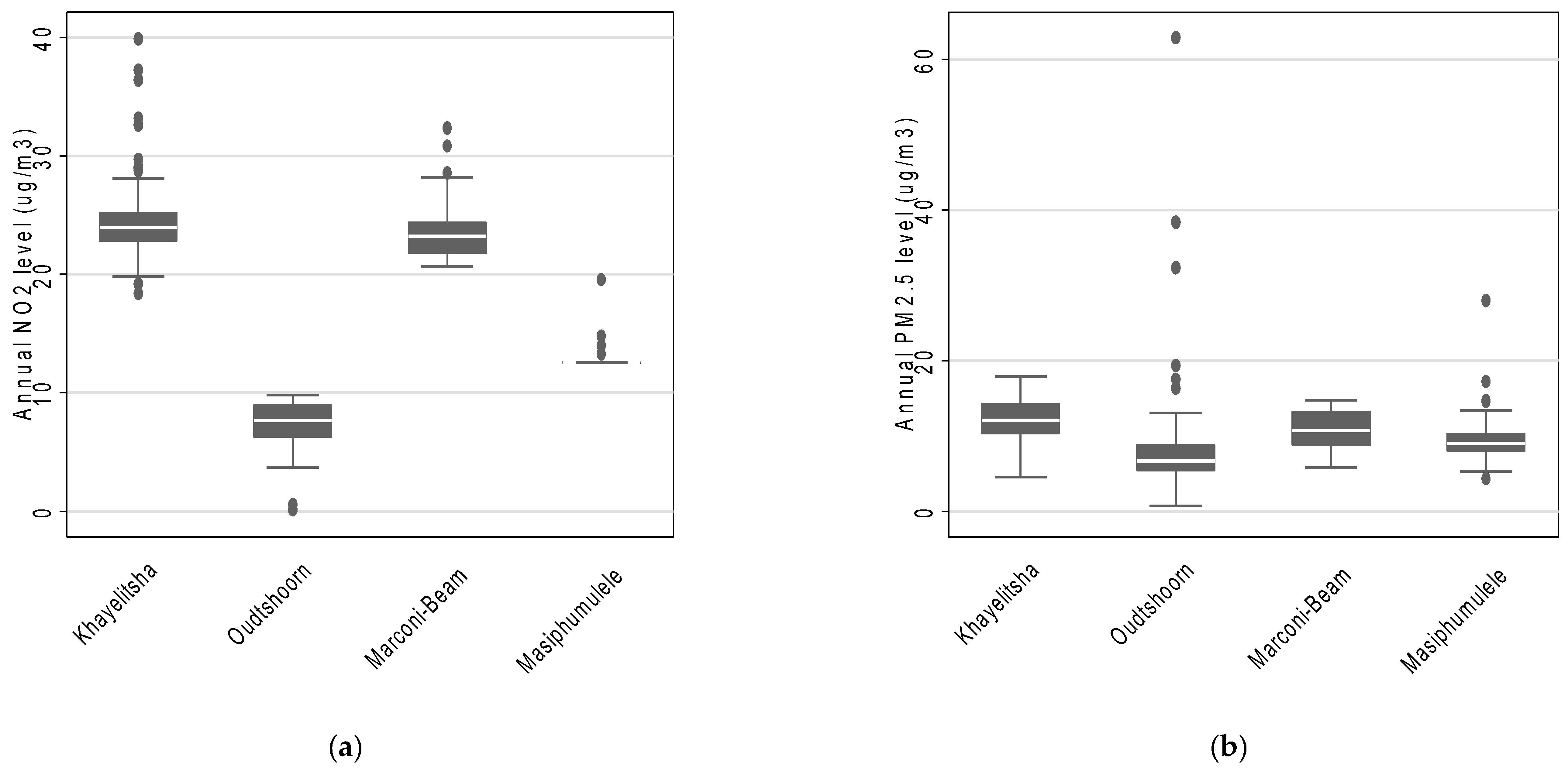
3.3. Air Pollution Characterization Based on LUR Modelling
3.4. Association between NO2 and PM2.5 Levels and Self-Reported Reported Cardiorespiratory Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Global Ambient Air Quality Database (Update 2018). Available online: https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health (accessed on 1 November 2021).
- Altieri, K.; Keen, S. The Cost of Air Pollution in South Africa. International Growth Centre Blog. 22 November. Available online: http://eprints.lse.ac.uk/id/eprint/81698 (accessed on 1 November 2021).
- World Health Organisation. Ambient Air Pollution Attributable DALYs. 2018. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/mbd-aap-ambient-air-pollution-attributable-dalys (accessed on 30 November 2021).
- Dockery, D.W.; Pope, C.A.; Xu, X.; Spengler, J.D.; Ware, J.H.; Fay, M.E.; Ferris, B.G.; Speizer, F.E. An Association between Air Pollution and Mortality in Six U.S. Cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pope, C.A.; Thun, M.J.; Namboodiri, M.M.; Dockery, D.W.; Evans, J.S.; Speizer, F.E.; Heath, C.W. Particulate air pollution as a predictor of mortality in a prospective study of U.S. adults. Am. J. Respir. Crit. Care Med. 1995, 151, 669–674. [Google Scholar] [CrossRef]
- Kim, H.; Kim, J.; Kim, S.; Kang, S.H.; Kim, H.J.; Kim, H.; Heo, J.; Yi, S.-M.; Kim, K.; Youn, T.-J. Cardiovascular Effects of Long-Term Exposure to Air Pollution: A population Based Study With 900 845 Person-Years of Follow up. J. Am. Heart Assoc. 2017, 6, e007170. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Guo, C.; Lau, A.K.; Chan, T.-C.; Chuang, Y.C.; Lin, C.; Jiang, W.K.; Yeoh, E.-K.; Tam, T.; Woo, K.S.; et al. Long-Term Exposure to Fine Particulate Matter, Blood Pressure, and Incident Hypertension in Taiwanese Adults. Environ. Health Perspect. 2018, 126, 017008. [Google Scholar] [CrossRef]
- Le Tertre, A.; Medina, S.; Samoli, E.; Forsberg, B.; Michelozzi, P.; Boumghar, A.; Vonk, J.M.; Bellini, A.; Atkinson, R.; Ayres, J.G.; et al. Short-term effects of particulate air pollution on cardiovascular diseases in eight European cities. J. Epidemiol. Community Health 2002, 56, 773–779. [Google Scholar] [CrossRef]
- Adam, M.; Schikowski, T.; Carsin, A.E.; Cai, Y.; Jacquemin, B.; Sanchez, M.; Vierkötter, A.; Marcon, A.; Keidel, D.; Sugiri, D.; et al. Adult lung function and long-term air pollution exposure. ESCAPE: A multicentre cohort study and meta-analysis. Eur. Respir. J. 2015, 45, 38–50. [Google Scholar] [CrossRef] [Green Version]
- Ackermann-Liebrich, U.; Leuenberger, P.; Schwartz, J.; Schindler, C.; Monn, C.; Bolognini, G.; Bongard, J.P.; Brändli, O.; Domenighetti, G.; Elsasser, S.; et al. Lung function and long term exposure to air pollutants in Switzerland. Study on Air Pollution and Lung Diseases in Adults (SAPALDIA) Team. Am. J. Respir. Crit. Care Med. 1997, 155, 122–129. [Google Scholar] [CrossRef] [PubMed]
- McCreanor, J.; Cullinan, P.; Nieuwenhuijsen, M.J.; Stewart-Evans, J.; Malliarou, E.; Jarup, L.; Harrington, R.; Svartengren, M.; Han, I.-K.; Ohman-Strickland, P.; et al. Respiratory Effects of Exposure to Diesel Traffic in Persons with Asthma. N. Engl. J. Med. 2007, 357, 2348–2358. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.; Guo, Y.; Di, Q.; Zheng, Y.; Kowal, P.; Xiao, J.; Tao, L.; Xing, L.; Wenlin, Z.; Steven, W.H.; et al. Ambient PM2.5 and Stroke: Effect Modifiers and Population Attributable Risk in Six Low- and Middle- Income Countries. Stroke 2017, 48, 1191–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wichmann, J.; Voyi, K. Ambient air pollution exposure and respiratory, cardiovascular and cerebrovascular mortality in Cape Town, South Africa: 2001–2006. Int. J. Environ. Res. Public Health 2012, 9, 3978–4016. [Google Scholar] [CrossRef]
- Benaissa, F.; Alkama, R.; Annesi-Maesano, I. Assessment of air pollution impacts on population health in Bejaia city, Northern Algeria. Iran. J. Public Health 2014, 43, 1221–1228. [Google Scholar] [PubMed]
- Ana, G.; Odeshi, T.; Sridhar, M.; Ige, M. Outdoor respirable particulate matter and the lung function status of residents of selected communities in Ibadan, Nigeria. Perspect. Public Health 2014, 134, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Hamatui, N.; Beynon, C. Particulate Matter and Respiratory Symptoms among Adults Living in Windhoek, Namibia: A Cross Sectional Descriptive Study. Int. J. Environ. Res. Public Health 2017, 14, 110. [Google Scholar] [CrossRef] [Green Version]
- Olaniyan, T.; Jeebhay, M.; Röösli, M.; Naidoo, R.; Baatjies, R.; Künzil, N.; Tsai, M.; Davey, M.; De Hoogh, K.; Berman, D.; et al. A prospective cohort study on ambient air pollution and respiratory morbidities including childhood asthma in adolescents from the western Cape Province: Study protocol. BMC Public Health 2017, 17, 712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarvis, D.; Knox, J.; Burney, P.; Chinn, S.; Luczynska, C.; Anto, J.M.; Cerveri, I.; de Marco, R.; Gislasson, T.; Heinrich, J.; et al. The European Community Respiratory Health Survey II. Steer. Comm. Eur. Respir. J. 2002, 20, 1071–1079. [Google Scholar]
- Curtin, L.R.; Mohadjer, L.K.; Dohrmann, S.M.; Kruszon-Moran, D.; Mirel, L.B.; Carroll, M.D.; Hirsch, R.; Burt, V.L.; Johnson, C.L. National Health and Nutrition Examination Survey: Sample design, 2007–2010. Vital Health Stat. 2013, 2, 1–23. [Google Scholar]
- Calciano, L.; Corsico, A.G.; Pirina, P.; Trucco, G.; Jarvis, D.; Janson, C.; Accordini, S. Assessment of asthma severity in adults with ever asthma: A continuous score. PLoS ONE 2017, 12, e0177538. [Google Scholar] [CrossRef]
- Saucy, A.; Röösli, M.; Künzli, N.; Tsai, M.-Y.; Sieber, C.; Olaniyan, T.; Baatjies, R.; Jeebhay, M.; Davey, M.; Flückiger, B.; et al. Land Use Regression Modelling of Outdoor NO2 and PM2.5 Concentrations in Three Low Income Areas in the Western Cape Province, South Africa. Int. J. Environ. Res. Public Health 2018, 15, 1452. [Google Scholar] [CrossRef] [Green Version]
- Suid-Afrika RVAN. National Ambient Air Quality Standards [Internet]. Government Gazette; 2009; p. 4. Available online: https://www.gov.za/sites/default/files/gcis_document/201409/35463gon486.pdf (accessed on 1 February 2019).
- DEA. Ambient Air Quality Standards. Republic of South Africa, GN 35072, 2 March 2012. Available online: https://www.gov.za/sites/default/files/gcis_document/201409/35072144.pdf (accessed on 1 November 2021).
- Nkhama, E.; Ndhlovu, M.; Dvonch, J.T.; Lynam, M.; Mentz, G.; Siziya, S.; Voyi, K. Effects of airborne particulate matter on respiratory health in a community near a cement factory in Chilanga, Zambia results from a panel study. Int. J. Environ. Res. Public Health 2017, 14, 1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuvarega, A.T.; Taru, P. Ambiental dust speciation and metal content variation in TSP, PM10 and PM2.5 in urban atmospheric air of Harare (Zimbabwe). Environ. Monit. Assess. 2008, 144, 1–14. [Google Scholar] [CrossRef]
- Worobiec, A.; Potgieter-Vermaak, S.S.; Berghmans, P.; Winkler, H.; Burger, R.; Van Grieken, R. Air Particulate Emissions in Developing Countries: A Case Study in South Africa. Anal. Lett. 2011, 44, 1907–1924. [Google Scholar] [CrossRef]
- Nkosi, V.; Wichmann, J.; Voyi, K. Comorbidity of respiratory and cardiovascular diseases among the elderly residing close to mine dumps in South Africa: A cross-sectional study. S. Afr. Med. J. 2016, 106, 290–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cesaroni, G.; Forastiere, F.; Stafoggia, M.; Andersen, Z.J.; Badaloni, C.; Beelen, R.; Caracciolo, B.; De Faire, U.; Erbel, R.; Eriksen, K.T.; et al. Long term exposure to ambient air pollution and incidence of acute coronary events: Prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project. BMJ 2013, 348, f7412. [Google Scholar] [CrossRef] [Green Version]
- Young, M.T.; Sandler, D.P.; DeRoo, L.A.; Vedal, S.; Kaufman, J.; London, S.J. Ambient Air Pollution Exposure and Incident Adult Asthma in a Nationwide Cohort of U.S. Women. Am. J. Respir. Crit. Care Med. 2014, 190, 914–921. [Google Scholar] [CrossRef] [Green Version]
- Jacquemin, B.; Siroux, V.; Sanchez, M.; Carsin, A.-E.; Schikowski, T.; Adam, M.; Bellisario, V.; Buschka, A.; Bono, R.; Brunekreef, B.; et al. Ambient Air Pollution and Adult Asthma Incidence in Six European Cohorts (ESCAPE). Environ. Health Perspect. 2015, 123, 613–621. [Google Scholar] [CrossRef]
- Zheng, X.-Y.; Ding, H.; Jiang, L.-N.; Chen, S.-W.; Zheng, J.-P.; Qiu, M.; Zhou, Y.-X.; Chen, Q.; Guan, W.-J. Association between Air Pollutants and Asthma Emergency Room Visits and Hospital Admissions in Time Series Studies: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0138146. [Google Scholar] [CrossRef]
- Xu, A.; Mu, Z.; Jiang, B.; Wang, W.; Yu, H.; Zhang, L.; Li, J. Acute Effects of Particulate Air Pollution on Ischemic Heart Disease Hospitalizations in Shanghai, China. Int. J. Environ. Res. Public Health 2017, 14, 168. [Google Scholar] [CrossRef]
- Bai, L.; Shin, S.; Burnett, R.T.; Kwong, J.C.; Hystad, P.; Van Donkelaar, A.; Goldberg, M.S.; Lavigne, E.; Copes, R.; Martin, R.V.; et al. Exposure to ambient air pollution and the incidence of congestive heart failure and acute myocardial infarction: A population-based study of 5.1 million Canadian adults living in Ontario. Environ. Int. 2019, 132, 105004. [Google Scholar] [CrossRef] [PubMed]
- William, E.; Cayley, J.R. Diagnosing the Cause of Chest Pain. Am. Fam. Physician 2005, 72, 1. [Google Scholar]
- Hystad, P.; Larkin, A.; Rangarajan, S.; AlHabib, K.F.; Avezum, Á.; Calik, K.B.T.; Chifamba, J.; Dans, A.; Diaz, R.; du Plessis, J.L.; et al. Associations of outdoor fine particulate air pollution and cardiovascular disease in 157 436 individuals from 21 high-income, middle-income, and low-income countries (PURE): A prospective cohort study. Lancet Planet. Health 2020, 4, e235–e245. [Google Scholar] [CrossRef]
- Sheppard, L.; Burnett, R.T.; Szpiro, A.A.; Kim, S.-Y.; Jerrett, M.; Pope, C.A.; Brunekreef, B. Confounding and exposure measurement error in air pollution epidemiology. Air Qual. Atmos. Health 2012, 5, 203–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Asthma-Related Questions |
| Wheezing in the last 12 months |
| Shortness of breath in the last 12 months |
| Woken up by feeling of tight chest in the last 12 months |
| Attack of shortness of breath at rest in the last 12 months |
| Woken up by attack of shortness of breath in the last 12 months |
| Attack of shortness of breath after exercise in the last 12 months |
| Self- reported asthma |
| Medication for asthma control |
| Additional Cardiorespiratory Questions |
| Self-reported doctor diagnosis of asthma |
| Self-reported chest-pain |
| Self-reported hypertension |
| Self-reported high cholesterol |
| Khayelitsha (N = 172) | Marconi-Beam (N = 132) | Oudtshoorn (N = 156) | Masiphumelele (N = 112) | All (N = 572) | |
|---|---|---|---|---|---|
| Age | 40.8 (35.4; 47.5) | 38.8 (32.7; 43.6) | 43.0 (36.3; 51.5) | 38.2 (33.8; 45.2) | 40.7 (34.6; 47.2) |
| Sex (female) | 151 (87.8) | 121 (91.7) | 142 (91.0) | 92 (82.1) | 506 (88.5) |
Home language
| 148 (86.0) 38 (22.1) | 110 (83.3) 33 (25.0) | 32 (20.5) 124 (79.5) | 108 (96.4) 9 (8.0) | 398 (69.6) 204 (35.7) |
Education
| 2 (1.2) 169 (98.3) 124 (72.1) | 2 (1.5) 130 (98.5) 94 (71.2) | 0 (0) 156 (100) 119 (76.5) | 0 (0) 112 (100) 93 (83.0) | 4 (0.7) 567 (99.1) 429 (75.0) |
| Employed | 77 (44.8) | 57 (43.2) | 50 (32.1) | 58 (51.8) | 242 (42.3) |
Fuel used to heat home or cooking
| 3 (1.7) 0 (0) 16 (9.3) 140 (81.4) 0 (0) 0 (0) 82 (47.7) | 0 (0) 0 (0) 4 (3.0) 108 (81.8) 0 (0) 0 (0) 52 (39.4) | 6 (3.9) 0 (0) 9 (5.8) 33 (21.2) 0 (0) 0 (0) 131 (84.0) | 0 (0) 1 (0.9) 3 (2.7) 70 (62.5) 0 (0) 0 (0) 54 (48.2) | 9 (1.6) 1 (0.2) 32 (5.6) 351 (61.4) 0 (0) 0 (0) 319 (55.8) |
| Physical active in last month | 54 (31.4) | 36 (27.3) | 31 (19.9) | 22 (19.6) | 143 (25.0) |
| Smoke cigarettes | 16 (9.3) | 3 (2.3) | 50 (32.1) | 7 (6.3) | 76 (13.3) |
| Khayelitsha (N = 172) N (%) | Marconi-Beam (N = 132) N (%) | Oudtshoorn (N = 156) N (%) | Masiphumelele (N = 112) N (%) | All areas (N = 572) N (%) | |
|---|---|---|---|---|---|
| Doctor diagnosed asthma | 14 (8.1) | 7 (5.3) | 11 (7.1) | 6 (5.4) | 38 (6.6) |
| Wheezing in the last 12 months | 23 (13.4) | 8 (6.1) | 13 (8.3) | 11 (9.8) | 55 (9.6) |
| Shortness of breath in last 12 months | 18 (10.5) | 7 (5.3) | 14 (9.0) | 7 (6.3) | 46 (8.1) |
| Woken up by feeling of tight chest in the last 12 months | 21 (12.2) | 9 (6.8) | 14 (9.0) | 9 (8.0) | 53 (9.3) |
| Woken up by attack of shortness of breath at rest in the last 12 months | 18 (10.5) | 7 (5.3) | 14 (9.0) | 9 (8.0) | 48 (8.4) |
| Attack of shortness of breath after exercise in the last 12 months | 35 (20.3) | 14 (10.6) | 26 (16.7) | 29 (25.9) | 104 (18.2) |
| Bring up phlegm from chest at any time of day in the winter | 20 (11.6) | 3 (2.3) | 19 (12.2) | 10 (8.9) | 52 (9.1) |
| Woken up by heavy coughing at any time in the last 12 months | 29 (16.9) | 6 (4.5) | 22 (14.1) | 16 (14.3) | 73 (12.8) |
| Self-reported asthmatic | 16 (9.3) | 11 (8.3) | 11 (7.1) | 6 (5.4) | 44 (7.7) |
| Medication for asthma control | 7 (4.1) | 2 (1.5) | 10 (6.4) | 1 (0.9) | 20 (3.5) |
Asthma symptom score #
| 0 (0) 108 (62.8) 78 (45.3) | 0 (0) 108 (81.8) 35 (26.5) | 0 (0) 123 (78.8) 33 (21.2) | 0 (0) 72 (64.3) 45 (40.2) | 0 (0) 411 (71.9) 191(33.4) |
| Self-reported experience chest pain | 25 (14.5) | 5 (3.8) | 17 (10.9) | 4 (3.6) | 51 (8.9) |
| Self-reported hypertension | 42 (24.4) | 14 (10.6) | 38 (24.4) | 21 (18.8) | 115 (20.1) |
| Self-reported cholesterol | 15 (8.7) | 8 (6.1) | 5 (3.2) | 5 (4.5) | 33 (5.8) |
| NO2 | PM2.5 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Doctor Diagnosed Asthma | Asthma Symptom Score > 2 | Chest-Pain | Hypertension | High Cholesterol | Doctor Diagnosed Asthma | Asthma Symptom Score > 2 | Chest-Pain | Hypertension | High Cholesterol | |
| A | 0.92 (0.48–1.75) | 1.31 (0.92–1.85) | 1.06 (0.61–1.83) | 0.75 (0.50–1.11) | 1.90 (0.94–3.83) | 1.21 (0.90–1.62) | 1.14 (0.93–1.41) | 1.38 (1.06–1.80) | 0.90 (0.69–1.18) | 1.15 (0.83–1.60) |
| B | 1.13 (0.58–2.19) | 1.40 (0.98–1.99) | 1.15 (0.66–2.02) | 0.93 (0.61–1.42) | 2.29 (1.11–4.72) | 1.26 (0.95–1.69) | 1.16 (0.94–1.43) | 1.41 (1.08–1.85) | 0.95 (0.73–1.25) | 1.20 (0.86–1.66) |
| C | 1.61 (0.76–3.41) | 1.23 (0.81–1.87) | 1.23 (0.65–2.35) | 0.83 (0.50–1.39) | 1.98 (0.84–4.64) | 1.28 (0.97–1.69) | 1.14 (0.92–1.41) | 1.42 (1.08–1.86) | 0.94 (0.70–1.25) | 1.16 (0.79–1.69) |
| D | 1.67 (0.78–3.55) | 1.34 (0.88–2.05) | 1.42 (0.74–2.74) | 0.87 (0.52–1.45) | 2.17 (0.93–5.11) | 1.28 (0.97–1.69) | 1.15 (0.93–1.42) | 1.42 (1.09–1.86) | 0.95 (0.71–1.26) | 1.18 (0.82–1.72) |
| E | 1.66 (0.78–3.55) | 1.43 (0.93–2.20) | 1.45 (0.75–2.79) | 0.89 (0.53–1.49) | 2.24 (0.96–5.22) | 1.28 (0.97–1.69) | 1.17 (0.95–1.46) | 1.43 (1.09–1.87) | 0.96 (0.73–1.27) | 1.20 (0.84–1.71) |
| F | 1.13 (0.11–12.05) | 1.23 (0.34–4.46) | 0.65 (0.10–4.33) | 0.78 (0.18–3.49) | 0.40 (0.03–5.83) | 1.27 (0.95–1.71) | 1.12 (0.89–1.41) | 1.36 (1.05–1.78) | 0.96 (0.72–1.29) | 1.13 (0.68–1.86) |
| NO2 | PM2.5 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Doctor Diagnosed Asthma | Asthma Symptom Score > 2 | Chest-Pain | Hypertension | High Cholesterol | Doctor Diagnosed Asthma | Asthma Symptom Score > 2 | Chest-Pain | Hypertension | High Cholesterol | |
| A | 0.84 (0.44–1.62) | 1.24 (0.86–1.78) | 0.93 (0.53–1.63) | 0.76 (0.50–1.15) | 1.83 (0.88–3.79) | 1.23 (0.92–1.64) | 1.11 (0.90–1.39) | 1.40 (1.06–1.84) | 0.97 (0.75–1.27) | 1.08 (0.71–1.66) |
| B | 1.03 (0.53–2.00) | 1.32 (0.92–1.92) | 1.00 (0.57–1.79) | 0.94 (0.60–1.47) | 2.19 (1.03–4.64) | 1.27 (0.95–1.70) | 1.12 (0.90–1.39) | 1.42 (1.08–1.88) | 0.98 (0.74–1.30) | 1.10 (0.70–1.74) |
| C | 1.47 (0.69–3.14) | 1.16 (0.75–1.79) | 1.07 (0.55–2.08) | 0.84 (0.50–1.43) | 1.90 (0.79–4.57) | 1.27 (0.95–1.69) | 1.13 (0.91–1.41) | 1.42 (1.08–1.88) | 0.98 (0.74–1.30) | 1.09 (0.68–1.74) |
| D | 1.53 (0.71–3.29) | 1.26 (0.82–1.96) | 1.26 (0.64–2.46) | 0.88 (0.52–1.49) | 2.07 (0.87–4.97) | 1.27 (0.95–1.69) | 1.13 (0.91–1.41) | 1.42 (1.09–1.86) | 0.98 (0.74–1.30) | 1.12 (0.71–1.77) |
| E | 1.53 (0.71–3.30) | 1.34 (0.86–2.09) | 1.29 (0.66–2.52) | 0.89 (0.53–1.52) | 2.13 (0.90–5.03) | 1.27 (0.95–1.69) | 1.15 (0.92–1.44) | 1.42 (1.09–1.87) | 0.99 (0.75–1.31) | 1.15 (0.76–1.75) |
| F | 1.10 (0.10–12.49) | 1.21 (0.33–4.41) | 0.58 (0.08–4.21) | 0.78 (0.18–3.48) | 0.39 (0.03–5.91) | 1.28 (0.95–1.72) | 1.13 (0.90–1.42) | 1.38 (1.06–1.80) | 0.97 (0.73–1.30) | 1.14 (0.69–1.87) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bagula, H.; Olaniyan, T.; de Hoogh, K.; Saucy, A.; Parker, B.; Leaner, J.; Röösli, M.; Dalvie, M.A. Ambient Air Pollution and Cardiorespiratory Outcomes amongst Adults Residing in Four Informal Settlements in the Western Province of South Africa. Int. J. Environ. Res. Public Health 2021, 18, 13306. https://doi.org/10.3390/ijerph182413306
Bagula H, Olaniyan T, de Hoogh K, Saucy A, Parker B, Leaner J, Röösli M, Dalvie MA. Ambient Air Pollution and Cardiorespiratory Outcomes amongst Adults Residing in Four Informal Settlements in the Western Province of South Africa. International Journal of Environmental Research and Public Health. 2021; 18(24):13306. https://doi.org/10.3390/ijerph182413306
Chicago/Turabian StyleBagula, Herman, Toyib Olaniyan, Kees de Hoogh, Apolline Saucy, Bhawoodien Parker, Joy Leaner, Martin Röösli, and Mohamed Aqiel Dalvie. 2021. "Ambient Air Pollution and Cardiorespiratory Outcomes amongst Adults Residing in Four Informal Settlements in the Western Province of South Africa" International Journal of Environmental Research and Public Health 18, no. 24: 13306. https://doi.org/10.3390/ijerph182413306