
Nationwide Population-Based Epidemiological Study for Outcomes of Adjunctive Steroid Therapy in Pediatric Patients with Bacterial Meningitis in Taiwan


Abstract
:1. Introduction
2. Patients and Methods
2.1. Data Source
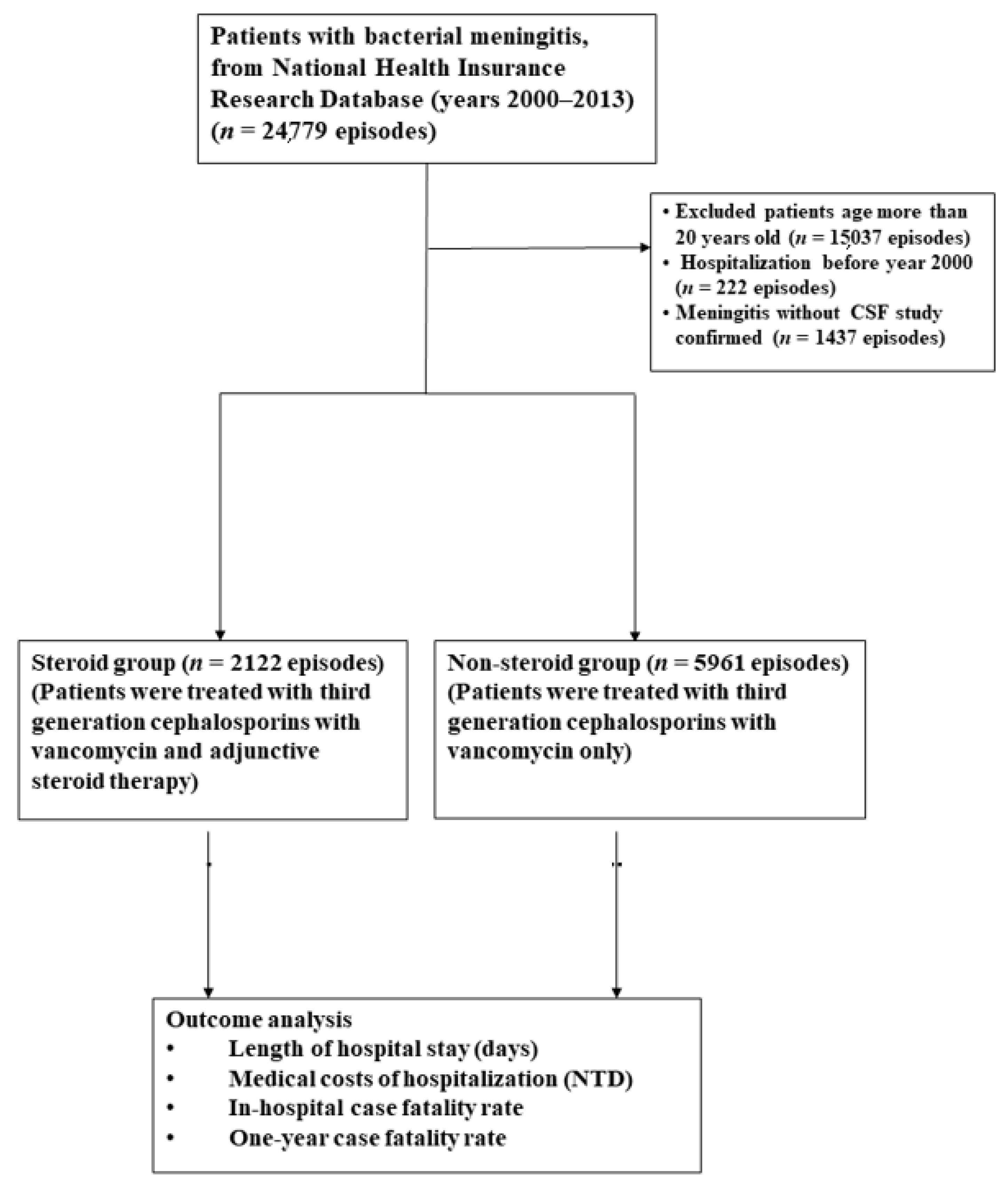
2.2. Study Subjects
2.3. Outcome Assessment
3. Results
3.1. Baseline Characteristics of Study Patients
3.2. Underlying Diseases and Clinical Features
3.3. Duration and Cost of Hospitalization
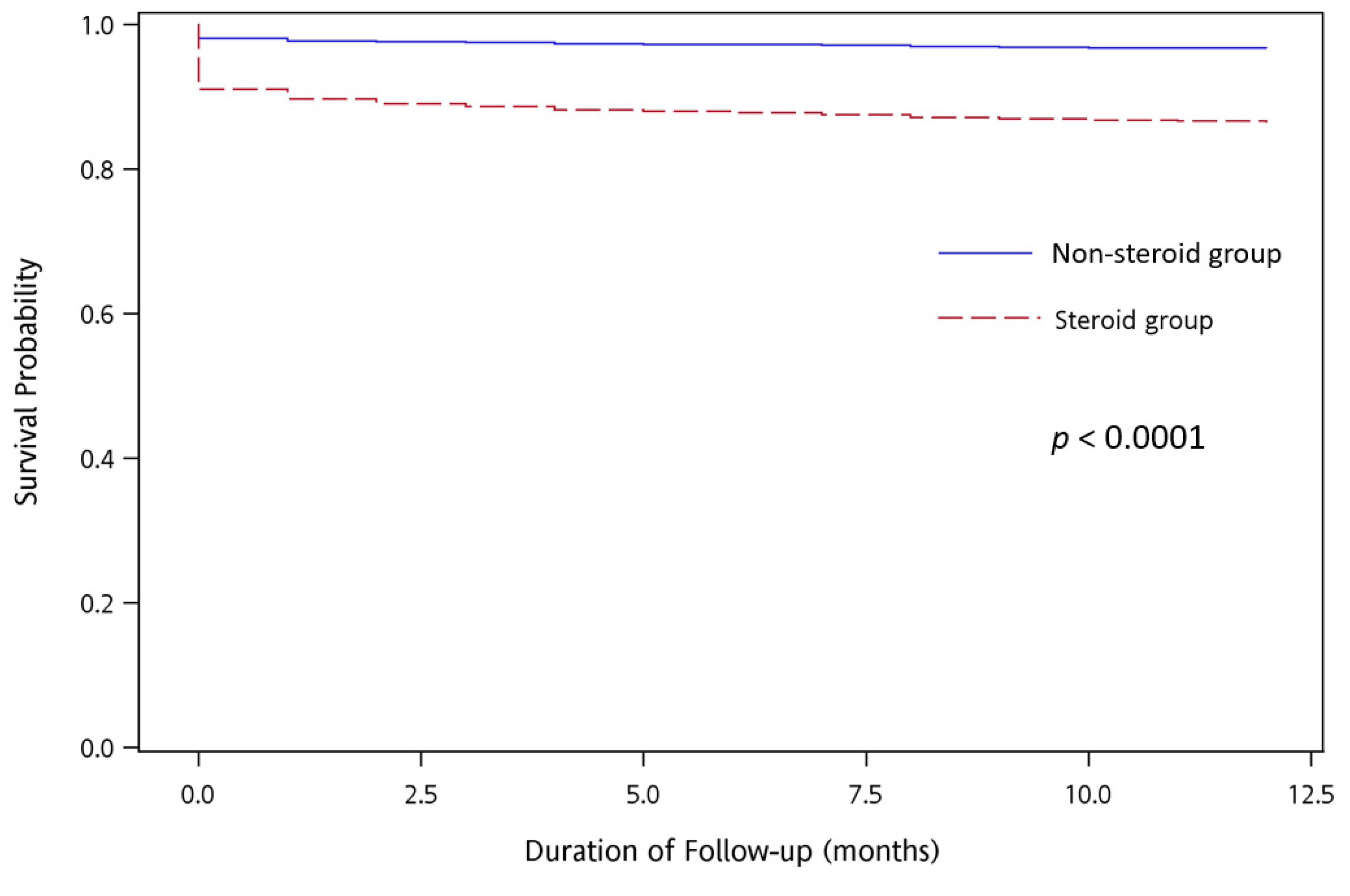
3.4. Therapeutic Outcome of Patients
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baraff, L.J.; Lee, S.I.; Schriger, D.L. Outcomes of bacterial meningitis in children: A meta-analysis. Pediatr. Infect. Dis. J. 1993, 12, 389–394. [Google Scholar] [CrossRef]
- Mongelluzzo, J.; Mohamad, Z.; Ten Have, T.R.; Shah, S.S. Corticosteroids and mortality in children with bacterial meningitis. JAMA 2008, 299, 2048–2055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nigrovic, L.E.; Kuppermann, N.; Malley, R.; Bacterial Meningitis Study Group of the Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics. Children with bacterial meningitis presenting to the emergency department during the pneumococcal conjugate vaccine era. Acad. Emerg. Med. 2008, 15, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Olarte, L.; Barson, W.J.; Barson, R.M.; Lin, P.L.; Romero, J.R.; Tan, T.Q.; Givner, L.B.; Bradley, J.S.; Hoffman, J.A.; Hulten, K.G.; et al. Impact of the 13-Valent Pneumococcal Conjugate Vaccine on Pneumococcal Meningitis in US Children. Clin. Infect. Dis. 2015, 61, 767–775. [Google Scholar] [CrossRef] [Green Version]
- Brouwer, M.C.; McIntyre, P.; Prasad, K.; van de Beek, D. Corticosteroids for acute bacterial meningitis. Cochrane Database Syst. Rev. 2015, CD004405. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, X.; Wang, Y.; Liu, Q.; Kong, C.; Xu, G. Meta-analysis of adjunctive dexamethasone to improve clinical outcome of bacterial meningitis in children. Child’s Nerv. Syst. 2018, 34, 217–223. [Google Scholar] [CrossRef] [PubMed]
- King, S.M.; Law, B.; Langley, J.M.; Heurter, H.; Bremner, D.; Wang, E.E.; Gold, R. Dexamethasone therapy for bacterial meningitis: Better never than late? Can. J. Infect. Dis. 1994, 5, 210–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasbun, R. Update and advances in community acquired bacterial meningitis. Curr. Opin. Infect. Dis. 2019, 32, 233–238. [Google Scholar] [CrossRef]
- Tunkel, A.R.; Hartman, B.J.; Kaplan, S.L.; Kaufman, B.A.; Roos, K.L.; Scheld, W.M.; Whitley, R.J. Practice guidelines for the management of bacterial meningitis. Clin. Infect. Dis. 2004, 39, 1267–1284. [Google Scholar] [CrossRef] [PubMed]
- Swanson, D. Meningitis. Pediatr. Rev. 2015, 36, 514–524, quiz 516–525. [Google Scholar] [CrossRef]
- Ahmed, A.; Jafri, H.; Lutsar, I.; McCoig, C.C.; Trujillo, M.; Wubbel, L.; Shelton, S.; McCracken, G.H., Jr. Pharmacodynamics of vancomycin for the treatment of experimental penicillin- and cephalosporin-resistant pneumococcal meningitis. Antimicrob. Agents Chemother. 1999, 43, 876–881. [Google Scholar] [CrossRef] [Green Version]
- Cabellos, C.; Martinez-Lacasa, J.; Martos, A.; Tubau, F.; Fernandez, A.; Viladrich, P.F.; Gudiol, F. Influence of dexamethasone on efficacy of ceftriaxone and vancomycin therapy in experimental pneumococcal meningitis. Antimicrob. Agents Chemother. 1995, 39, 2158–2160. [Google Scholar] [CrossRef] [Green Version]
- Paris, M.M.; Hickey, S.M.; Uscher, M.I.; Shelton, S.; Olsen, K.D.; McCracken, G.H., Jr. Effect of dexamethasone on therapy of experimental penicillin- and cephalosporin-resistant pneumococcal meningitis. Antimicrob. Agents Chemother. 1994, 38, 1320–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annane, D.; Bellissant, E.; Bollaert, P.E.; Briegel, J.; Keh, D.; Kupfer, Y.; Pirracchio, R.; Rochwerg, B. Corticosteroids for treating sepsis in children and adults. Cochrane Database Syst. Rev. 2019, 12, CD002243. [Google Scholar] [CrossRef]
- Dias, S.P.; Brouwer, M.C.; Bijlsma, M.W.; van der Ende, A.; van de Beek, D. Sex-based differences in adults with community-acquired bacterial meningitis: A prospective cohort study. Clin. Microbiol. Infect. 2017, 23, 121.e9–121.e15. [Google Scholar] [CrossRef] [Green Version]
- Dharmarajan, L.; Salazar, L.; Hasbun, R. Gender Differences in Community-acquired Meningitis in Adults: Clinical Presentations and Prognostic Factors. J. Meningitis. 2016, 1, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basri, R.; Zueter, A.R.; Mohamed, Z.; Alam, M.K.; Norsa’adah, B.; Hasan, S.A.; Hasan, H.; Ahmad, F. Burden of bacterial meningitis: A retrospective review on laboratory parameters and factors associated with death in meningitis, kelantan malaysia. Nagoya J. Med. Sci. 2015, 77, 59–68. [Google Scholar]
- Namani, S.; Milenkovic, Z.; Kuchar, E.; Koci, R.; Mehmeti, M. Mortality from bacterial meningitis in children in Kosovo. J. Child Neurol. 2012, 27, 46–50. [Google Scholar] [CrossRef]
- Eshima, N.; Tokumaru, O.; Hara, S.; Bacal, K.; Korematsu, S.; Karukaya, S.; Uruma, K.; Okabe, N.; Matsuishi, T. Age-specific sex-related differences in infections: A statistical analysis of national surveillance data in Japan. PLoS ONE 2012, 7, e42261. [Google Scholar] [CrossRef]
- Alamarat, Z.; Hasbun, R. Management of Acute Bacterial Meningitis in Children. Infect. Drug Resist. 2020, 13, 4077–4089. [Google Scholar] [CrossRef] [PubMed]
- Saez-Llorens, X.; McCracken, G.H., Jr. Bacterial meningitis in children. Lancet 2003, 361, 2139–2148. [Google Scholar] [CrossRef]
- Thigpen, M.C.; Whitney, C.G.; Messonnier, N.E.; Zell, E.R.; Lynfield, R.; Hadler, J.L.; Harrison, L.H.; Farley, M.M.; Reingold, A.; Bennett, N.M.; et al. Bacterial meningitis in the United States, 1998–2007. N. Engl. J. Med. 2011, 364, 2016–2025. [Google Scholar] [CrossRef]
- Whitney, C.G.; Farley, M.M.; Hadler, J.; Harrison, L.H.; Bennett, N.M.; Lynfield, R.; Reingold, A.; Cieslak, P.R.; Pilishvili, T.; Jackson, D.; et al. Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine. N. Engl. J. Med. 2003, 348, 1737–1746. [Google Scholar] [CrossRef] [Green Version]
- Wenger, J.D.; Hightower, A.W.; Facklam, R.R.; Gaventa, S.; Broome, C.V. Bacterial meningitis in the United States, 1986: Report of a multistate surveillance study. The Bacterial Meningitis Study Group. J. Infect. Dis. 1990, 162, 1316–1323. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.C.; Chiu, N.C.; Chi, H.; Ho, C.S.; Huang, F.Y. Evolving trends of neonatal and childhood bacterial meningitis in northern Taiwan. J. Microbiol. Immunol. Infect. 2015, 48, 296–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, P.L.; Chie, W.C.; Wang, C.Y.; Yang, C.Y.; Lu, C.Y.; Chang, L.Y.; Huang, L.M.; Lee, C.Y. Epidemiology of Haemophilus influenzae type b meningitis in Taiwan, 1997 and 2000. J. Microbiol. Immunol. Infect. 2004, 37, 164–168. [Google Scholar]
- Dunbar, M.; Shah, H.; Shinde, S.; Vayalumkal, J.; Vanderkooi, O.G.; Wei, X.-C.; Kirton, A. Stroke in Pediatric Bacterial Meningitis: Population-Based Epidemiology. Pediatr. Neurol. 2018, 89, 11–18. [Google Scholar] [CrossRef]
- Namani, S.; Milenkovic, Z.; Koci, B. A prospective study of risk factors for neurological complications in childhood bacterial meningitis. J. Pediatr. 2013, 89, 256–262. [Google Scholar] [CrossRef] [Green Version]
- Hsu, M.H.; Hsu, J.F.; Kuo, H.C.; Lai, M.Y.; Chiang, M.C.; Lin, Y.J.; Huang, H.R.; Chu, S.M.; Tsai, M.H. Neurological Complications in Young Infants With Acute Bacterial Meningitis. Front. Neurol. 2018, 9, 903. [Google Scholar] [CrossRef]
- Anderson, V.; Anderson, P.; Grimwood, K.; Nolan, T. Cognitive and executive function 12 years after childhood bacterial meningitis: Effect of acute neurologic complications and age of onset. J. Pediatr. Psychol. 2004, 29, 67–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, Y.R.; Lin, J.R.; Chang, W.N.; Tsai, N.W.; Huang, C.C.; Wang, H.C.; Su, Y.J.; Lin, W.C.; Cheng, B.C.; Su, C.M.; et al. Outcomes of adjunctive steroid therapy in adult patients with bacterial meningitis in Taiwan: A nationwide population-based epidemiologic study. J. Clin. Neurosci. 2019, 61, 54–58. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Enrollment | Steroid Group (n = 2122) | Non-Steroid Group (n = 5961) | p-Value |
|---|---|---|---|
| n (%) | n (%) | ||
| Age at infection (mean ± SD, years) | 5.5 ± 4.0 | 4.4 ± 3.6 | |
| Sex | 0.63 | ||
| Male | 1275(60.08%) | 3617 (60.68%) | |
| Female | 847 (39.92%) | 2344(39.32%) | |
| Distribution of years § | <0.0001 | ||
| 2000 | 313 (14.75%) | 724 (12.15%) | |
| 2001 | 353 (16.64%) | 1254 (21.04%) | |
| 2002 | 227 (10.70%) | 668 (11.21%) | |
| 2003 | 159 (7.49%) | 393 (6.59%) | |
| 2004 | 163 (7.68%) | 390 (6.54%) | |
| 2005 | 162 (7.63%) | 540 (9.06%) | |
| 2006 | 151 (7.12%) | 409 (6.86%) | |
| 2007 | 93 (4.38%) | 333 (5.59%) | |
| 2008 | 95 (4.48%) | 242 (4.06%) | |
| 2009 | 84 (3.96%) | 231 (3.88%) | |
| 2010 | 93 (4.38%) | 186 (3.12%) | |
| 2011 | 93 (4.38%) | 207 (3.47%) | |
| 2012 | 76 (3.58%) | 194 (3.25%) | |
| 2013 | 60 (2.83%) | 190 (3.19%) |
| Causative Pathogens § | Steroid Group (n = 2122) n (%) | Non-Steroid Group (n = 5961) n (%) |
|---|---|---|
| Streptococcus Species (n = 569) | ||
| Streptococcus Pneumoniae | 152 (7.2%) | 110 (1.9%) |
| Other streptococci | 127 (6.0%) | 180 (3.0%) |
| Haemophilus influenzae(n= 119) | 85 (4.0%) | 34 (0.6%) |
| Gram-negative bacilli (n = 175) | ||
| Escherichia coli | 14 (0.7%) | 18 (0.3%) |
| Pseudomonas species | 2 (0.09%) | 5 (0.08%) |
| Salmonella species | 3 (0.1%) | 1 (0.02%) |
| Other Gram-negative Bacilli | 54 (2.5%) | 78 (1.3%) |
| Staphylococcus Species (n = 20) | ||
| Staphylococcus aureus | 10 (0.5%) | 9 (0.2%) |
| Other Staphylococci | 1 (0.05%) | 0 |
| Neisseria meningitidis(n = 1) | 0 | 1 (0.02%) |
| Listeria monocytogenes(n = 10) | 7 (0.3%) | 3 (0.05%) |
| Anaerobes pathogens (n = 10) | 7 (0.3%) | 3 (0.05%) |
| Others (n = 7179) | 1660 (78.2%) | 5519 (92.6%) |
| Characteristics | Steroid Group (n = 2122) | Non-Steroid Group (n = 5961) | p-Value |
|---|---|---|---|
| n (%) | n (%) | ||
| Underlying diseases | |||
| Chronic epilepsy | 45 (2.1%) | 116 (2.0%) | 0.62 |
| Hypertension | 46 (2.2%) | 28 (0.5%) | <0.0001 |
| Type 1 diabetes mellitus | 40 (1.9%) | 23 (0.4%) | <0.0001 |
| Status post neurosurgical procedure | 25 (1.2%) | 26 (0.4%) | 0.0002 |
| Systemic lupus erythematosus | 14 (0.7%) | 3 (0.05%) | <0.0001 |
| Chronic kidney diseases | 8 (0.4%) | 10 (0.2%) | 0.08 |
| Non-alcoholic liver cirrhosis | 6 (0.3%) | 6 (0.1%) | 0.06 |
| Atrial fibrillation | 6 (0.3%) | 4 (0.07%) | 0.0152 |
| Clinical features | |||
| Hydrocephalus | 234 (11.0%) | 157 (2.6%) | <0.0001 |
| Acute respiratory failure | 216 (10.2%) | 67 (1.1%) | <0.0001 |
| Pneumonia | 198 (9.3%) | 240 (4.0%) | <0.0001 |
| Urinary tract infection | 184 (8.7%) | 630 (10.6%) | 0.0126 |
| Brain edema | 90 (4.2%) | 71 (1.2%) | <0.0001 |
| Brain abscesses | 84 (4.0%) | 46 (0.8%) | <0.0001 |
| Fever | 73 (3.4%) | 398 (6.7%) | <0.0001 |
| Headache | 40 (1.9%) | 205 (3.4%) | 0.0003 |
| Shunt infection | 38 (1.8%) | 61 (1.0%) | 0.0058 |
| Acute symptomatic seizure | 30 (1.4%) | 40 (0.7%) | 0.0015 |
| CSF rhinorrhea | 17 (0.8%) | 21 (0.4%) | 0.0094 |
| Bacterial endocarditis | 6 (0.3%) | 2 (0.03%) | 0.0017 |
| Cerebral infarctions | 4 (0.2%) | 9 (0.2%) | 0.71 |
| Hospitalization | Steroid Group | Non-Steroid Group | p-Value |
|---|---|---|---|
| Length of hospital stay (days) (Median (IQR)) | 13 (6–27) | 6 (4–10) | p < 0.0001 |
| Medical costs of hospitalization (NTD) (Median (IQR)) | 77,941 (26,647–237,540) | 26,653 (14,287–53,421) | p < 0.0001 |
| Fatality | Survival n (%) | Death n (%) | Univariate Cox Model | Multivariate Cox Model | ||
|---|---|---|---|---|---|---|
| Hazard Ratio § (95% CI) | p-Value | Hazard Ratio § (95% CI) | p-Value | |||
| Study groups | ||||||
| Non-steroid group | 5861 (98.3%) | 100 (1.7%) | 2.531 (1.9–3.3) | <0.0001 | 2.551 (2.0–3.3) | <0.0001 |
| Steroid group | 1955 (92.1%) | 167 (7.9%) | ||||
| Age at infection (mean, years) | 4.6 | 5.3 | 0.996 (1.0–1.1) | 0.75 | 0.992 (0.9–1.0) | 0.50 |
| Sex | ||||||
| Male | 4754 (97.2%) | 138 (2.8%) | 1.441 (1.1–1.8) | 0.0029 | 1.436(1.1–1.8) | 0.0032 |
| Females | 3062 (96.0%) | 129 (4.0%) | ||||
| Fatality | Survival n (%) | Death n (%) | Univariate Cox Model | Multivariate Cox Model | ||
|---|---|---|---|---|---|---|
| Hazard Ratio § (95% CI) | p-Value | Hazard Ratio § (95% CI) | p-Value | |||
| Study groups | ||||||
| Non-steroid group | 5763 (96.7%) | 198 (3.3%) | 4.26 (3.56–5.1) | <0.0001 | 4.13 (3.443–4.953) | <0.0001 |
| Steroid group | 1832 (86.3%) | 290 (13.7%) | ||||
| Age at infection (mean, years) | 4.6 | 5.7 | 1.04 (1.02–1.06) | <0.0001 | 1.026 (1.009–1.042) | 0.0021 |
| Sex | ||||||
| Male | 4622 (94.5%) | 270 (5.5%) | 1.25 (1.04–1.49) | 0.016 | 1.255 (1.05–1.501) | 0.0127 |
| Females | 2973 (93.2%) | 218 (6.8%) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, D.-Y.; Lai, Y.-R.; Lien, C.-Y.; Chang, W.-N.; Huang, C.-C.; Cheng, B.-C.; Kung, C.-T.; Lu, C.-H. Nationwide Population-Based Epidemiological Study for Outcomes of Adjunctive Steroid Therapy in Pediatric Patients with Bacterial Meningitis in Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 6386. https://doi.org/10.3390/ijerph18126386
Hsieh D-Y, Lai Y-R, Lien C-Y, Chang W-N, Huang C-C, Cheng B-C, Kung C-T, Lu C-H. Nationwide Population-Based Epidemiological Study for Outcomes of Adjunctive Steroid Therapy in Pediatric Patients with Bacterial Meningitis in Taiwan. International Journal of Environmental Research and Public Health. 2021; 18(12):6386. https://doi.org/10.3390/ijerph18126386
Chicago/Turabian StyleHsieh, Dong-Yi, Yun-Ru Lai, Chia-Yi Lien, Wen-Neng Chang, Chih-Cheng Huang, Ben-Chung Cheng, Chia-Te Kung, and Cheng-Hsien Lu. 2021. "Nationwide Population-Based Epidemiological Study for Outcomes of Adjunctive Steroid Therapy in Pediatric Patients with Bacterial Meningitis in Taiwan" International Journal of Environmental Research and Public Health 18, no. 12: 6386. https://doi.org/10.3390/ijerph18126386