Epidemiological Analysis of the 2019 Dengue Epidemic in Bhutan

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Data Sources
2.3. Descriptive Analysis
2.4. Growth Rate
2.5. Effective Reproduction Number
3. Results
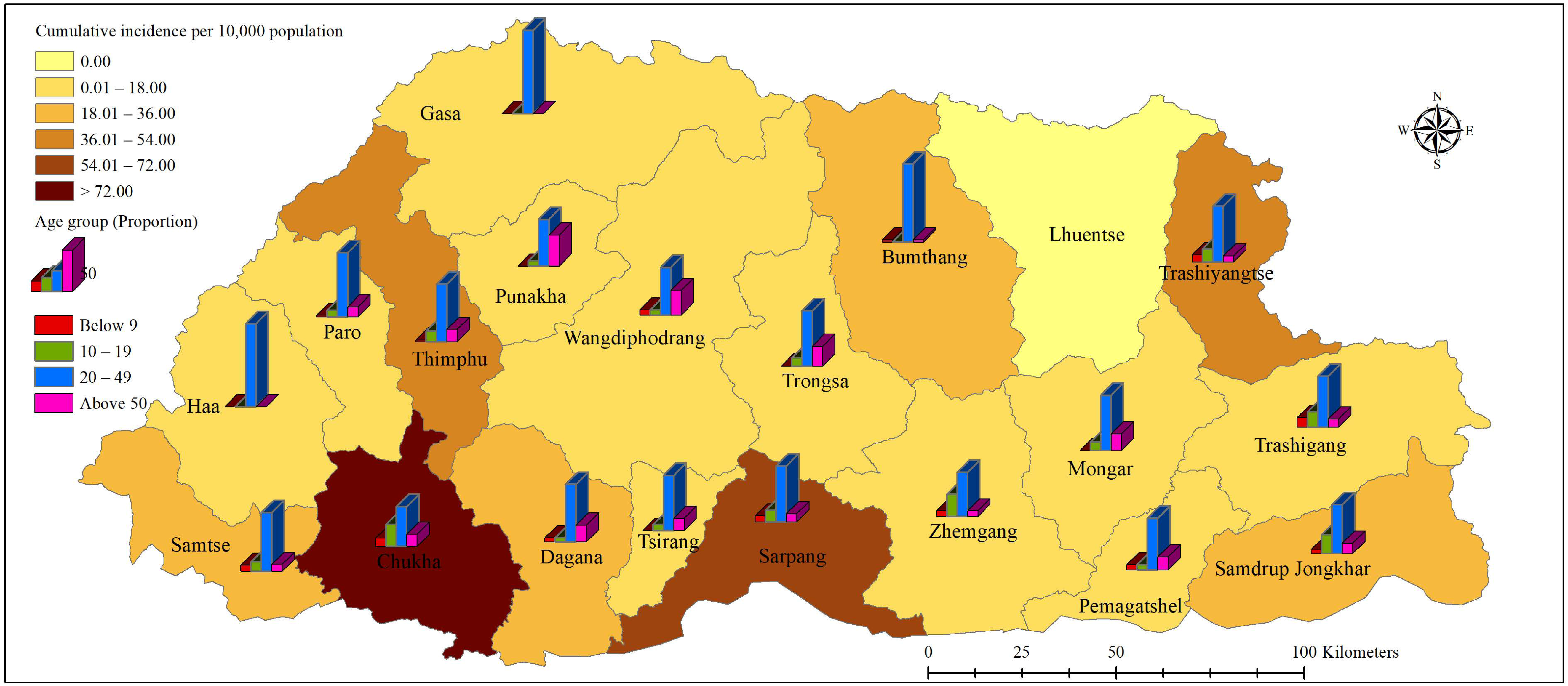
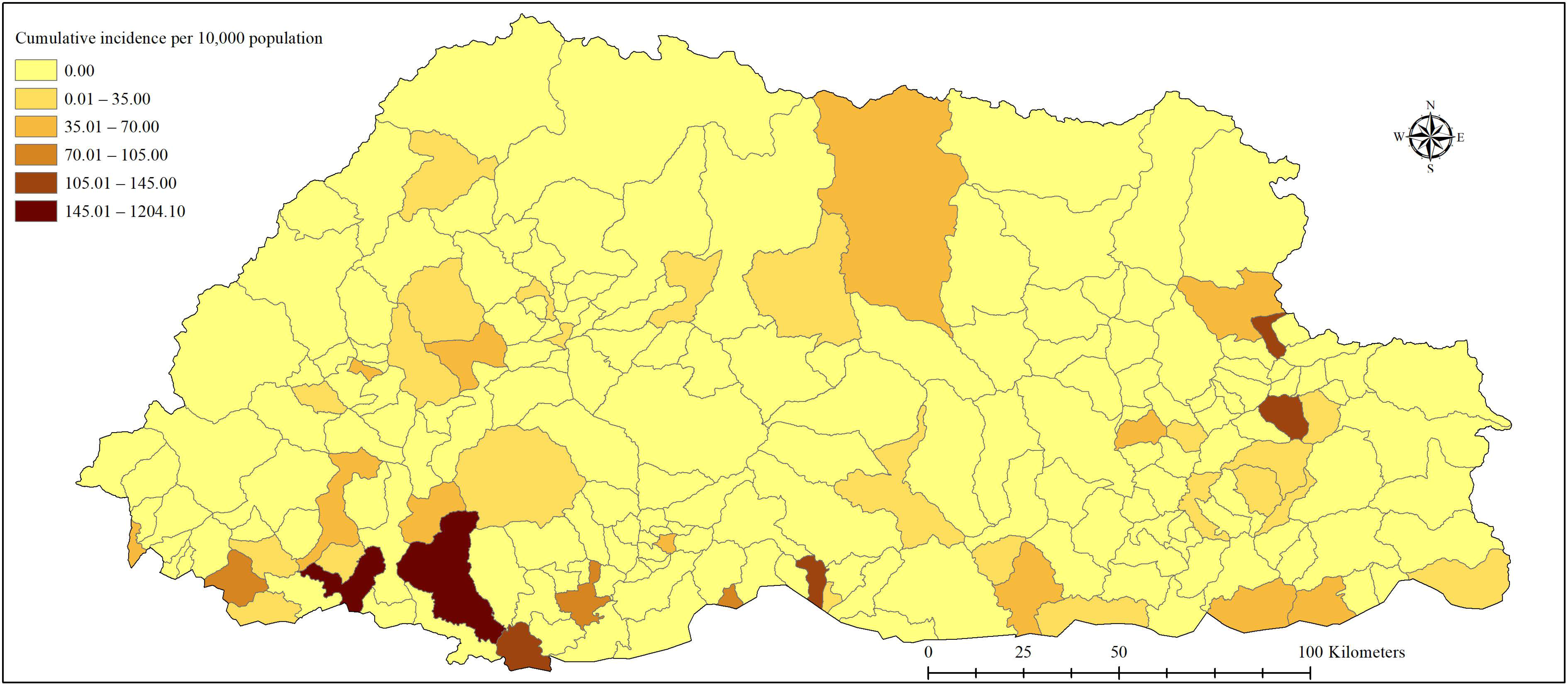
3.1. Descriptive Analysis
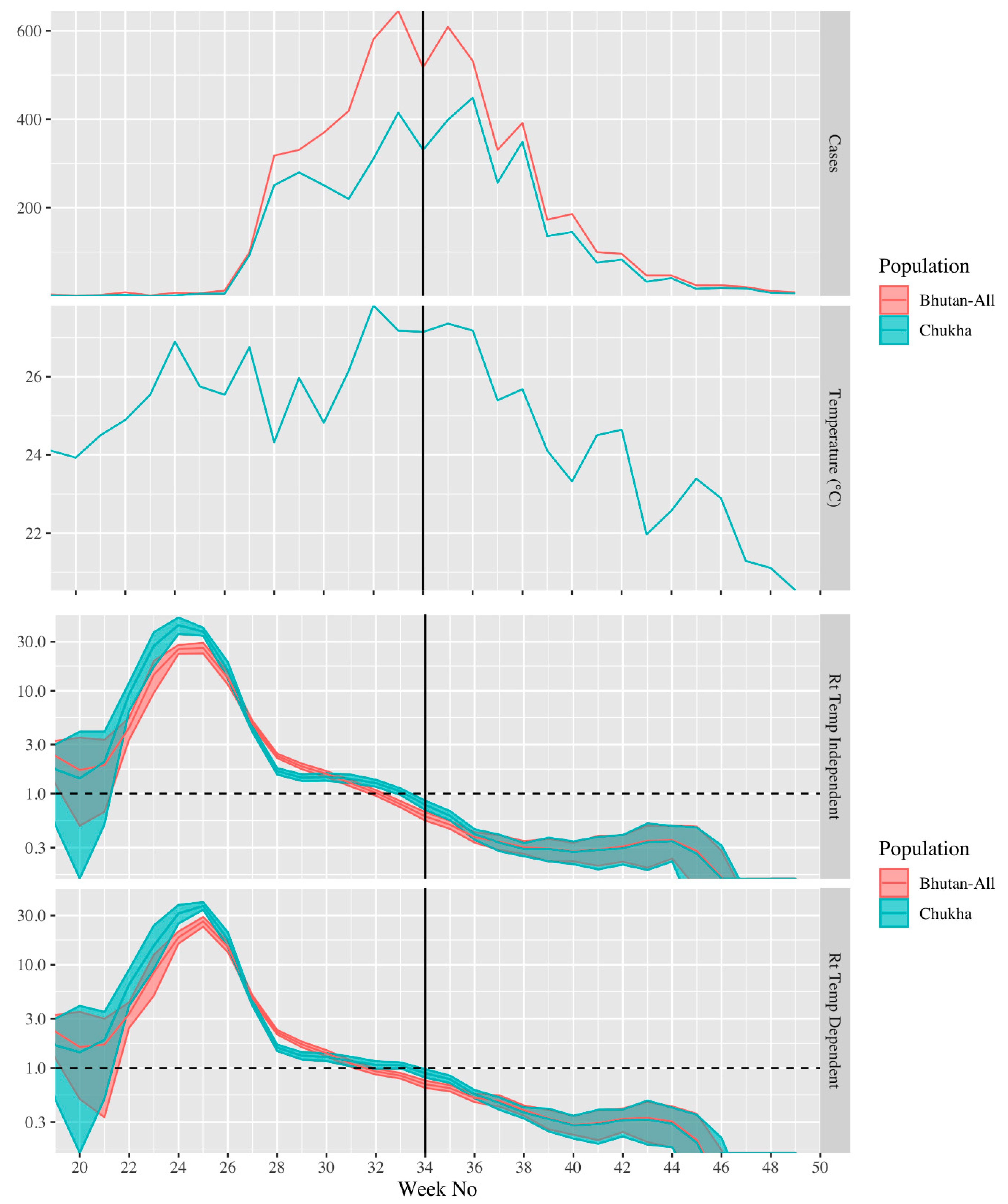
3.2. Growth Rate
3.3. Effective Reproduction Number
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gubler, D.J. Dengue and dengue hemorrhagic fever. Clin. Microbiol. Rev. 1998, 11, 480–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brady, O.J.; Gething, P.W.; Bhatt, S.; Messina, J.P.; Brownstein, J.S.; Hoen, A.G.; Moyes, C.L.; Farlow, A.W.; Scott, T.W.; Hay, S.I. Refining the Global Spatial Limits of Dengue Virus Transmission by Evidence-Based Consensus. PLoS Neglected Trop. Dis. 2012, 6, e1760. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The global distribution and burden of dengue. Nat. Cell Biol. 2013, 496, 504–507. [Google Scholar] [CrossRef] [PubMed]
- Guzman, M.G.; Kourí, G. Dengue and dengue hemorrhagic fever in the Americas: Lessons and challenges. J. Clin. Virol. 2003, 27, 1–13. [Google Scholar] [CrossRef]
- Kyle, J.L.; Harris, E. Global Spread and Persistence of Dengue. Annu. Rev. Microbiol. 2008, 62, 71–92. [Google Scholar] [CrossRef] [Green Version]
- Wilder-Smith, A.; Gubler, D.J. Geographic Expansion of Dengue: The Impact of International Travel. Med. Clin. N. Am. 2008, 92, 1377–1390. [Google Scholar] [CrossRef]
- Jaenisch, T.; Junghanss, T.; Wills, B.; Brady, O.J.; Eckerle, I.; Farlow, A.; Hay, S.I.; McCall, P.J.; Messina, J.P.; Ofula, V.; et al. Dengue Expansion in Africa—Not Recognized or Not Happening? Emerg. Infect. Dis. 2014, 20, e140487. [Google Scholar] [CrossRef]
- Guo, C.; Zhou, Z.; Wen, Z.; Liu, Y.; Zeng, C.; Xiao, D.; Ou, M.; Han, Y.; Huang, S.; Liu, D.; et al. Global Epidemiology of Dengue Outbreaks in 1990–2015: A Systematic Review and Meta-Analysis. Front. Cell. Infect. Microbiol. 2017, 7, 317. [Google Scholar] [CrossRef]
- Hermann, L.L.; Gupta, S.B.; Manoff, S.B.; Kalayanarooj, S.; Gibbons, R.V.; Coller, B.-A.G. Advances in the understanding, management, and prevention of dengue. J. Clin. Virol. 2015, 64, 153–159. [Google Scholar] [CrossRef]
- Dash, A.P.; Bhatia, R.; Sunyoto, T.; Mourya, D.T. Emerging and re-emerging arboviral diseases in Southeast Asia. J. Vector Borne Dis. 2013, 50, 77–84. [Google Scholar]
- World Health Organization. Epidemic, & Pandemic Alert. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Huang, Y.-J.S.; Higgs, S.; Horne, K.M.; VanLandingham, D.L. Flavivirus-Mosquito Interactions. Viruses 2014, 6, 4703–4730. [Google Scholar] [CrossRef] [Green Version]
- Higa, Y. Dengue Vectors and their Spatial Distribution. Trop. Med. Health 2011, 39, S17–S27. [Google Scholar] [CrossRef] [Green Version]
- Ebi, K.L.; Nealon, J. Dengue in a changing climate. Environ. Res. 2016, 151, 115–123. [Google Scholar] [CrossRef] [Green Version]
- Zangmo, S.; Klungthong, C.; Chinnawirotpisan, P.; Tantimavanich, S.; Kosoltanapiwat, N.; Thaisomboonsuk, B.; Phuntsho, K.; Wangchuk, S.; Yoon, I.-K.; Fernandez, S. Epidemiological and Molecular Characterization of Dengue Virus Circulating in Bhutan, 2013–2014. PLoS Neglected Trop. Dis. 2015, 9, e0004010. [Google Scholar] [CrossRef]
- Dorji, T.; Yoon, I.-K.; Holmes, E.C.; Wangchuk, S.; Tobgay, T.; Nisalak, A.; Chinnawirotpisan, P.; Sangkachantaranon, K.; Gibbons, R.V.; Jarman, R.G. Diversity and Origin of Dengue Virus Serotypes 1, 2, and 3, Bhutan. Emerg. Infect. Dis. 2009, 15, 1630–1632. [Google Scholar] [CrossRef]
- Toan, D.T.T.; Hu, W.; Thai, P.Q.; Hoat, L.N.; Wright, P.; Martens, P. Hot spot detection and spatio-temporal dispersion of dengue fever in Hanoi, Vietnam. Glob. Health Action 2013, 6, 18632. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, R.F. Thinking about GIS: Geographic Information System Planning for Managers; ESRI, Inc.: Redlands, CA, USA, 2007. [Google Scholar]
- Heffernan, J.M.; Smith, R.J.; Wahl, L.M. Perspectives on the basic reproductive ratio. J. R. Soc. Interface 2005, 2, 281–293. [Google Scholar] [CrossRef]
- De Serres, G.; Gay, N.J.; Farrington, C.P. Epidemiology of Transmissible Diseases after Elimination. Am. J. Epidemiol. 2000, 151, 1039–1048; discussion 49–52. [Google Scholar] [CrossRef]
- Chowell, G.; Diaz-Dueñas, P.; Miller, J.; Alcazar-Velazco, A.; Hyman, J.; Fenimore, P.; Castillo-Chavez, C. Estimation of the reproduction number of dengue fever from spatial epidemic data. Math. Biosci. 2007, 208, 571–589. [Google Scholar] [CrossRef]
- National Statistical Bureau. Statistical Yearbook of Bhutan; Royal Government of Bhutan: Thimphu, Bhutan, 2018. [Google Scholar]
- National Statistical Bureau. Dzongkhag Population Projections 2017–2027; Royal Government of Bhutan: Thimphu, Bhutan, 2017. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Codeço, C.T.; Villela, D.A.M.; Coelho, F.C. Estimating the effective reproduction number of dengue considering temperature-dependent generation intervals. Epidemics 2018, 25, 101–111. [Google Scholar] [CrossRef]
- Wallinga, J. Different Epidemic Curves for Severe Acute Respiratory Syndrome Reveal Similar Impacts of Control Measures. Am. J. Epidemiol. 2004, 160, 509–516. [Google Scholar] [CrossRef] [Green Version]
- Wallinga, J.; Lipsitch, M. How generation intervals shape the relationship between growth rates and reproductive numbers. Proc. Biol. Sci. 2006, 274, 599–604. [Google Scholar] [CrossRef] [Green Version]
- Wangdi, K.; Clements, A.C.A.; Du, T.; Nery, S.V. Spatial and temporal patterns of dengue infections in Timor-Leste, 2005–2013. Parasites Vectors 2018, 11, 9. [Google Scholar] [CrossRef] [Green Version]
- Tosepu, R.; Tantrakarnapa, K.; Nakhapakorn, K.; Worakhunpiset, S. Climate variability and dengue hemorrhagic fever in Southeast Sulawesi Province, Indonesia. Environ. Sci. Pollut. Res. 2018, 25, 14944–14952. [Google Scholar] [CrossRef]
- Ehelepola, N.D.B.; Ariyaratne, K.; Buddhadasa, W.M.N.P.; Ratnayake, S.; Wickramasinghe, M. A study of the correlation between dengue and weather in Kandy City, Sri Lanka (2003–2012) and lessons learned. Infect. Dis. Poverty 2015, 4, 42. [Google Scholar] [CrossRef] [Green Version]
- Teurlai, M.; Menkès, C.E.; Cavarero, V.; Degallier, N.; Descloux, E.; Grangeon, J.-P.; Guillaumot, L.; Libourel, T.; Lucio, P.S.; Mathieu-Daudé, F.; et al. Socio-economic and Climate Factors Associated with Dengue Fever Spatial Heterogeneity: A Worked Example in New Caledonia. PLoS Neglected Trop. Dis. 2015, 9, e0004211. [Google Scholar] [CrossRef] [Green Version]
- Kraemer, M.U.G.; Reiner, R.C.; Brady, O.J.; Messina, J.P.; Gilbert, M.; Pigott, D.M.; Yi, D.; Johnson, K.; Earl, L.; Marczak, L.B.; et al. Past and future spread of the arbovirus vectors Aedes aegypti and Aedes albopictus. Nat. Microbiol. 2019, 4, 854–863. [Google Scholar] [CrossRef]
- Scott, T.W.; Morrison, A.C. Vector dynamics and transmission of dengue virus: Implications for dengue surveillance and pre-vention strategies: Vector dynamics and dengue prevention. Curr. Top. Microbiol. Immunol. 2010, 338, 115–128. [Google Scholar] [PubMed]
- Hsieh, Y.-H.; Ma, S. Intervention measures, turning point, and reproduction number for dengue, Singapore, 2005. Am. J. Trop. Med. Hyg. 2009, 80, 66–71. [Google Scholar] [CrossRef]
- Hsieh, Y.-H.; Chen, C.W.S. Turning points, reproduction number, and impact of climatological events for multi-wave dengue outbreaks. Trop. Med. Int. Health 2009, 14, 628–638. [Google Scholar] [CrossRef]
- Hyman, J.M.; Nesse, H.; Aguilera, X.; Olea, A.; Fuentes, R.; Chowell, G. The Basic Reproduction Number R0 and Effectiveness of Reactive Interventions during Dengue Epidemics: The 2002 Dengue Outbreak in Easter Island, Chile. Math. Biosci. Eng. 2013, 10, 1455–1474. [Google Scholar] [CrossRef]
- Favier, C.; Degallier, N.; Rosa-Freitas, M.G.; Boulanger, J.-P.; Lima, J.R.C.; Luitgards-Moura, J.F.; Menkes, C.E.; Mondet, B.; Oliveira, C.; Weimann, E.T.S.; et al. Early determination of the reproductive number for vector-borne diseases: The case of dengue in Brazil. Trop. Med. Int. Health 2006, 11, 332–340. [Google Scholar] [CrossRef]
- Supriatna, A.K. Estimating the Basic Reproduction Number of Dengue Transmission during 2002–2007 outbreaks in Bandung, Indonesia. WHO Reg. Off. South-East Asia 2009, 33, 21–33. [Google Scholar]
- Zangmo, S.; Darnal, J.B.; Gyeltshen, S.; Thapa, B.T.; Rodpradit, P.; Chinnawirotpisan, P.; Manasatienkij, W.; Macareo, L.R.; Fernandez, S.; Wangchuk, S.; et al. Molecular epidemiology of dengue fever outbreaks in Bhutan, 2016–2017. PLoS Neglected Trop. Dis. 2020, 14, e0008165. [Google Scholar] [CrossRef] [Green Version]
- Dash, P.K.; Parida, M.; Saxena, P.; Abhyankar, A.; Singh, C.P.; Tewari, K.N.; Jana, A.M.; Sekhar, K.; Rao, P.L. Reemergence of dengue virus type-3 (subtype-III) in India: Implications for increased incidence of DHF & DSS. Virol. J. 2006, 3, 55. [Google Scholar] [CrossRef] [Green Version]
- Gupta, E.; Dar, L.; Kapoor, G.; Broor, S. The changing epidemiology of dengue in Delhi, India. Virol. J. 2006, 3, 92. [Google Scholar] [CrossRef] [Green Version]
- Richards, A.L.; Bagus, R.; Baso, S.M.; Graham, R.R.; Punjabi, N.; Corwin, A.L.; Sandjaja, B.; Tan, R.; Follows, G.A. The first reported outbreak of dengue hemorrhagic fever in Irian Jaya, Indonesia. Am. J. Trop. Med. Hyg. 1997, 57, 49–55. [Google Scholar] [CrossRef]
- Pinho, S.T.R.; Ferreira, C.P.; Esteva, L.; Barreto, F.R.; Silva, V.C.M.; Teixeira, M.G.L. Modelling the dynamics of dengue real epidemics. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2010, 368, 5679–5693. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Categories (Years) | Number of Cases (n) | Proportion (%) |
|---|---|---|
| 0–9 | 434 | 8.27 |
| 10–19 | 1170 | 22.30 |
| 20–49 | 2886 | 55.00 |
| ≥50 | 757 | 14.43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsheten, T.; Mclure, A.; Clements, A.C.A.; Gray, D.J.; Wangdi, T.; Wangchuk, S.; Wangdi, K. Epidemiological Analysis of the 2019 Dengue Epidemic in Bhutan. Int. J. Environ. Res. Public Health 2021, 18, 354. https://doi.org/10.3390/ijerph18010354
Tsheten T, Mclure A, Clements ACA, Gray DJ, Wangdi T, Wangchuk S, Wangdi K. Epidemiological Analysis of the 2019 Dengue Epidemic in Bhutan. International Journal of Environmental Research and Public Health. 2021; 18(1):354. https://doi.org/10.3390/ijerph18010354
Chicago/Turabian StyleTsheten, Tsheten, Angus Mclure, Archie C. A. Clements, Darren J. Gray, Tenzin Wangdi, Sonam Wangchuk, and Kinley Wangdi. 2021. "Epidemiological Analysis of the 2019 Dengue Epidemic in Bhutan" International Journal of Environmental Research and Public Health 18, no. 1: 354. https://doi.org/10.3390/ijerph18010354