Lay People Training in CPR and in the Use of an Automated External Defibrillator, and Its Social Impact: A Community Health Study


 ,
,
Abstract
:1. Introduction
2. Material and Methods
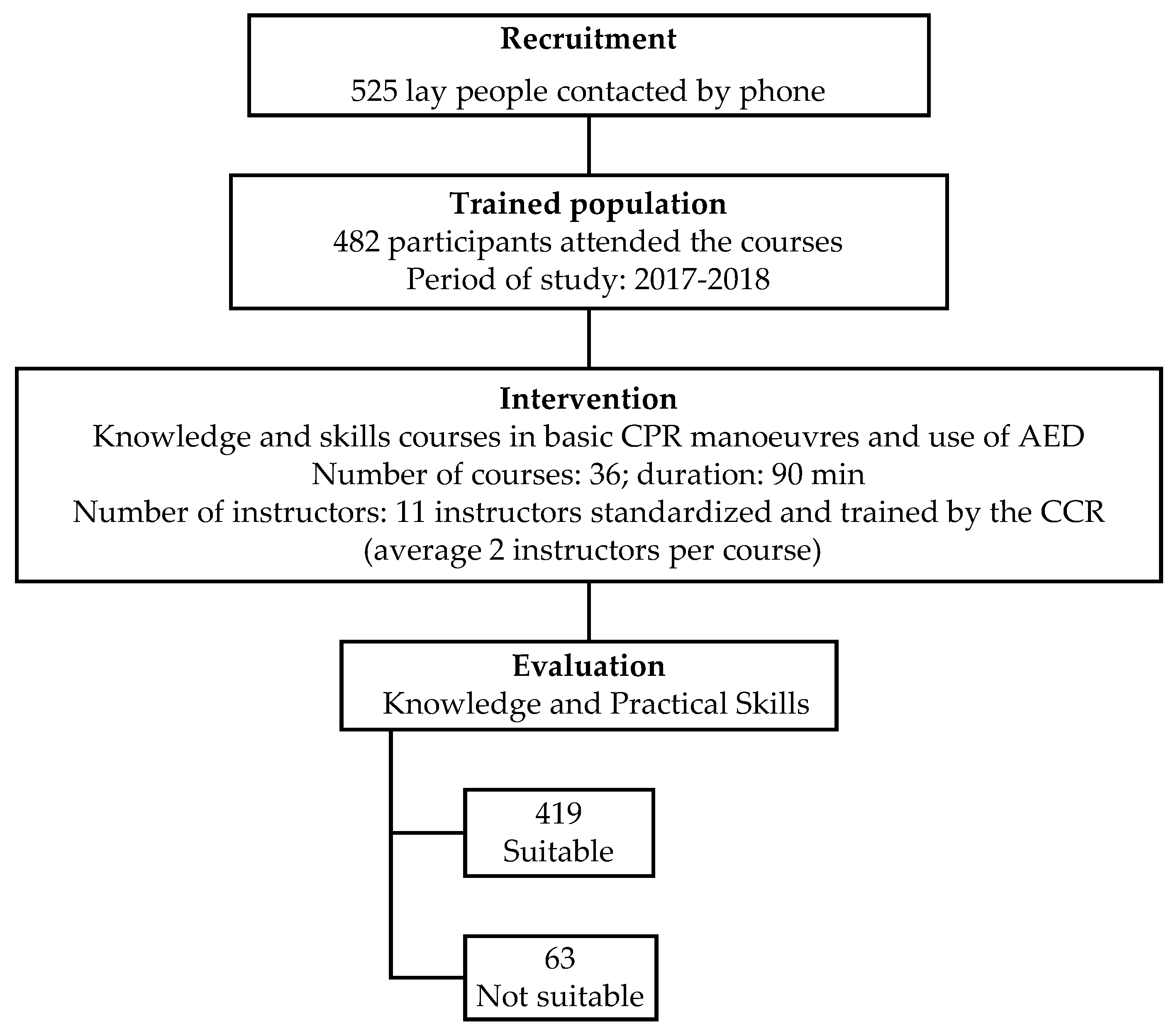
2.1. Study Design
2.2. Participants
2.3. Training
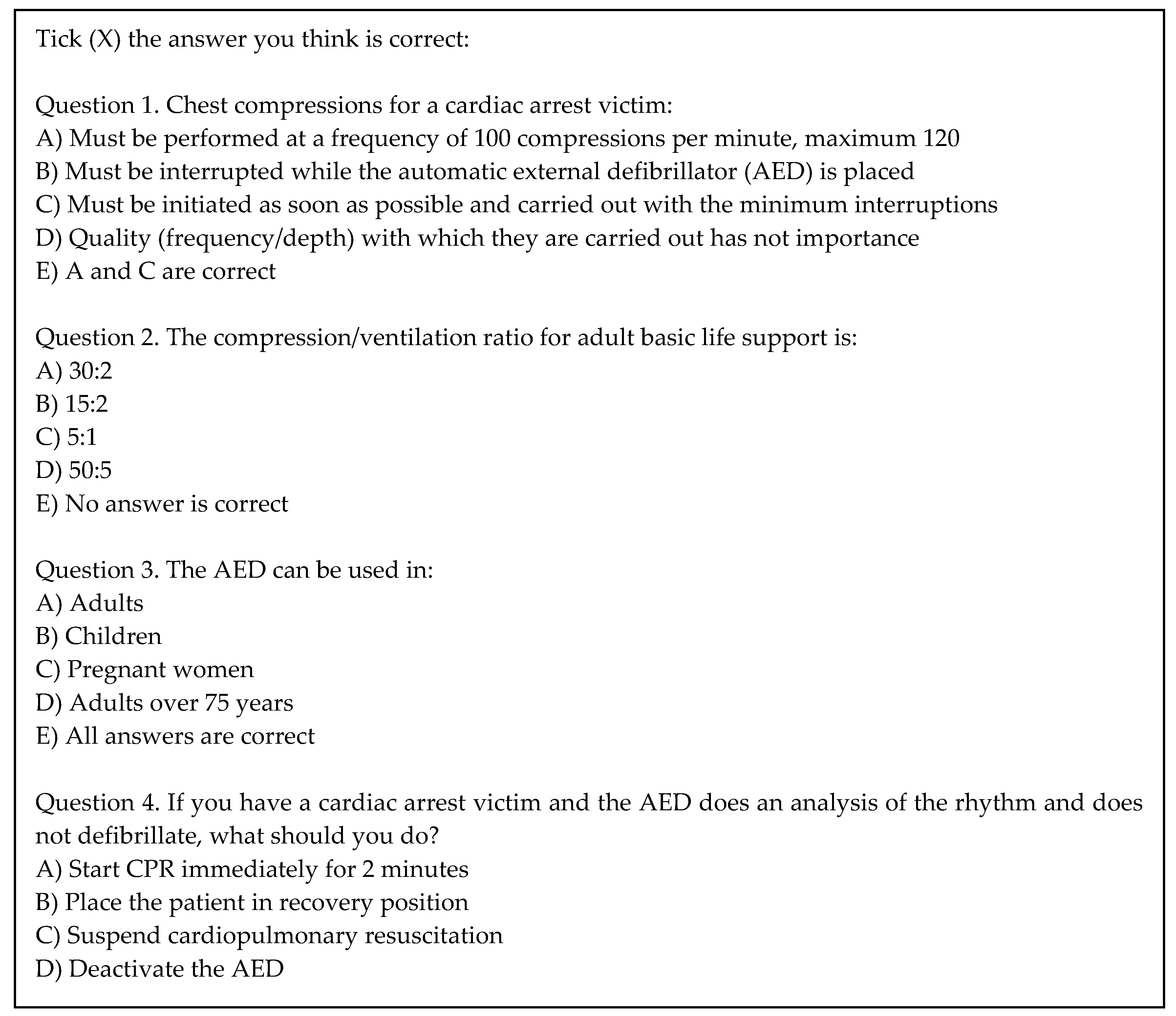
2.4. Variables
2.5. Social Impact
2.6. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics
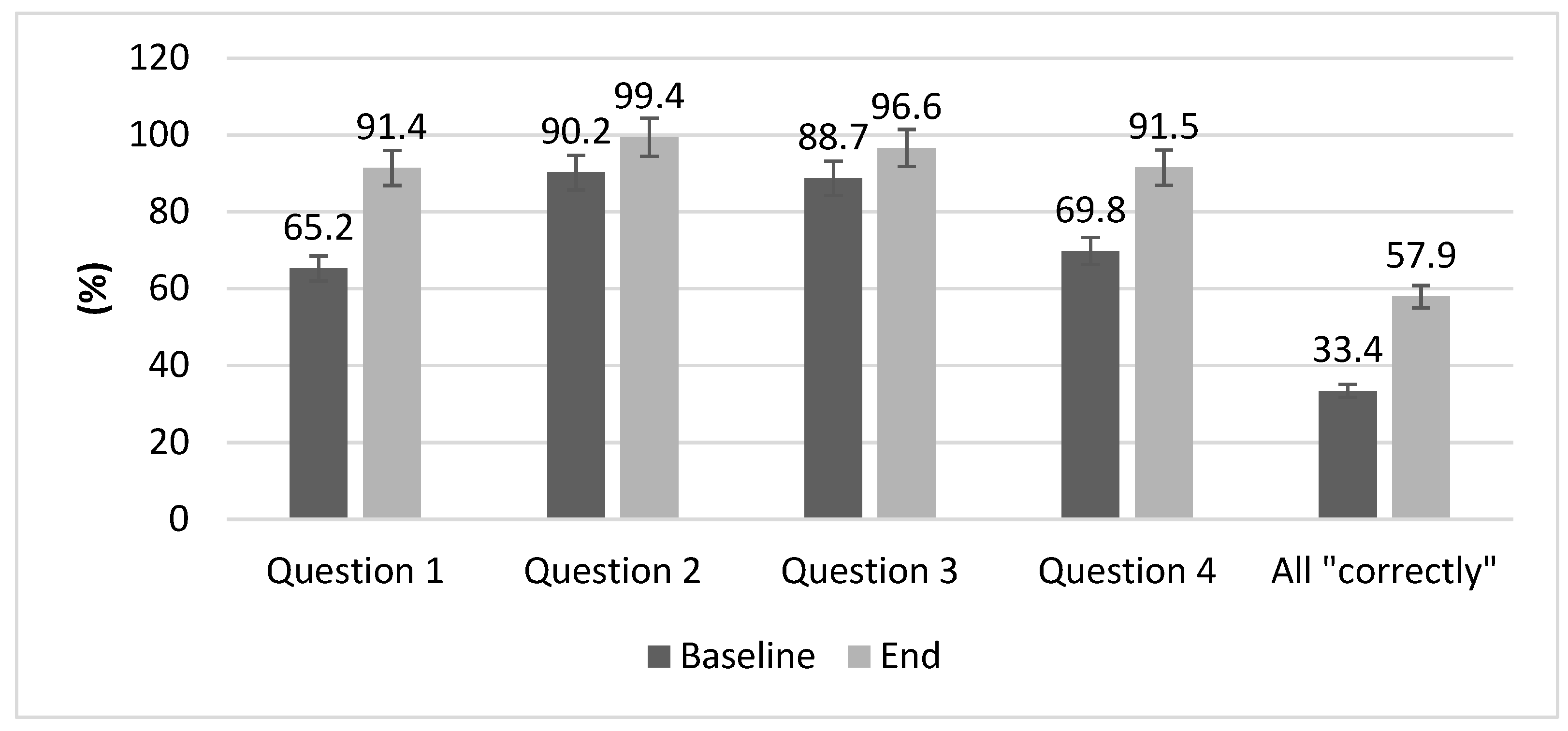
3.2. Training Evaluation
3.3. Social Impact
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Berdowski, J.; Berg, R.A.; Tijssen, J.G.P.; Koster, R.W. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospective studies. Resuscitation 2010, 81, 1479–1487. [Google Scholar] [CrossRef] [PubMed]
- Requena-Morales, R.; Palazón-Bru, A.; Rizo-Baeza, M.M.; Adsuar-Quesada, J.M.; Gil-Guillén, V.F.; Cortés-Castell, E. Mortality after out-of-hospital cardiac arrest in a Spanish Region. PLoS ONE 2017, 12, e0175818. [Google Scholar] [CrossRef] [PubMed]
- Ballesteros-Peña, S.; Abecia-Inchaurregui, L.C.; Echevarría-Orella, E. Factors Associated with Mortality in Out-of-hospital Cardiac Arrests Attended in Basic Life Support Units in the Basque Country (Spain). Rev. Española Cardiol. (Engl. Ed.) 2012, 66, 269–274. [Google Scholar]
- Ballesteros-Peña, S. Supervivencia extrahospitalaria tras una parada cardiorespiratoria en España: Una revisión de la literatura. Emerg. Rev. La Soc. Española Med. Urgenc. Emerg. 2013, 25, 137–142. [Google Scholar]
- Sociedad Española de Medicina Intensiva, Crítica y Unidades Coronarias (SEMICYUC). La cadena de supervivencia. In Plan Nacional RCP-Semicyuc; SEMICYUC: Madrid, Spain, 2012; pp. 1–2. [Google Scholar]
- García Guasch, R.; Cerdà, M. Enseñanza de la reanimación cardiopulmonar a la población: Uno de los pilares para mejorar la supervivencia de los pacientes en paro cardíaco. Med. Clin. (BARC) 2005, 124, 13–15. [Google Scholar] [CrossRef]
- Fordyce, C.B.; Hansen, C.M.; Kragholm, K.; Dupre, M.E.; Jollis, J.G.; Roettig, M.L.; Becker, L.B.; Hansen, S.M.; Hinohara, T.T.; Corbett, C.C.; et al. Association of Public Health Initiatives with Outcomes for Out-of-Hospital Cardiac Arrest at Home and in Public Locations. JAMA Cardiol. 2017, 2, 1226. [Google Scholar] [CrossRef]
- Stokes, N.A.; Scapigliati, A.; Trammell, A.R.; Parish, D.C. The Effect of the AED and AED Programs on Survival of Individuals, Groups and Populations. Prehosp. Disaster Med. 2012, 27, 419–424. [Google Scholar] [CrossRef]
- Hansen, C.M.; Kragholm, K.; Pearson, D.A.; Tyson, C.; Monk, L.; Myers, B.; Nelson, D.; Dupre, M.E.; Fosbøl, E.L.; Jollis, J.G.; et al. Association of bystander and first-responder intervention with survival after out-of-hospital cardiac arrest in North Carolina, 2010–2013. JAMA J. Am. Med. Assoc. 2015, 314, 255–264. [Google Scholar] [CrossRef]
- Smith, G.B.; Welch, J.; DeVita, M.A.; Hillman, K.M.; Jones, D. Education for cardiac arrest—Treatment or prevention? Resuscitation 2015, 92, 59–62. [Google Scholar] [CrossRef]
- Gräsner, J.-T.; Bossaert, L. Epidemiology and management of cardiac arrest: What registries are revealing. Best Pract. Res. Clin. Anaesthesiol. 2013, 27, 293–306. [Google Scholar] [CrossRef]
- Clark, A.P.; Aldridge, M.D.; Guzzetta, C.E.; Nyquist-Heise, P.; Norris, R.M.; Loper, P.; Meyers, T.A.; Voelmeck, W. Family Presence During Cardiopulmonary Resuscitation. Crit. Care Nurs. Clin. North Am. 2005, 17, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Stiell, I.G.; Nichol, G.; Wells, G.; De Maio, V.; Nesbitt, L.; Blackburn, J.; Spaite, D. Health-Related Quality of Life Is Better for Cardiac Arrest Survivors Who Received Citizen Cardiopulmonary Resuscitation. Circulation 2003, 108, 1939–1944. [Google Scholar] [CrossRef] [PubMed]
- Haydon, G.; van der Riet, P.; Maguire, J. Survivors’ quality of life after cardiopulmonary resuscitation: An integrative review of the literature. Scand. J. Caring Sci. 2017, 31, 6–26. [Google Scholar] [CrossRef] [PubMed]
- Hollenberg, J.; Herlitz, J.; Lindqvist, J.; Riva, G.; Bohm, K.; Rosenqvist, M.; Svensson, L. Improved Survival After Out-of-Hospital Cardiac Arrest Is Associated with an Increase in Proportion of Emergency Crew–Witnessed Cases and Bystander Cardiopulmonary Resuscitation. Circulation 2008, 118, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Out-of-Hospital Cardiac Arrest Surveillance—Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005–December 31, 2010. Surveill. Summ. 2011, 60, 1–19. [Google Scholar]
- Hasselqvist-Ax, I.; Riva, G.; Herlitz, J.; Rosenqvist, M.; Hollenberg, J.; Nordberg, P.; Ringh, M.; Jonsson, M.; Axelsson, C.; Lindqvist, J.; et al. Early Cardiopulmonary Resuscitation in Out-of-Hospital Cardiac Arrest. N. Engl. J. Med. 2015, 372, 2307–2315. [Google Scholar] [CrossRef] [PubMed]
- Del Pozo, A.; Villalobos, F.; Rey-Reñones, C.; Granado, E.; Sabaté, D.; Poblet, C.; Calvet, A.; Basora, J.; Castro, A.; Flores, G. Effectiveness of a network of automatically activated trained volunteers on the reduction of cardiopulmonary resuscitation manoueuvers initiation time: Study protocol. BMC Public Health 2019, 19, 572. [Google Scholar] [CrossRef]
- Consell Català de Resusscitació. Ressuscitació Cardiopulmonar. In Manual de l’alumne; CCR: Barcelona, Spain, 2010. [Google Scholar]
- Monsieurs, K.G.; Nolan, J.P.; Bossaert, L.L.; Greif, R.; Maconochie, I.K.; Nikolaou, N.I.; Perkins, G.D.; Soar, J.; Truhlář, A.; Wyllie, J.; et al. European Resuscitation Council Guidelines for Resuscitation 2015. Resuscitation 2015, 95, 1–80. [Google Scholar] [CrossRef]
- Domingo, A.; Marcos, J. Propuesta de un indicador de la «clase social» basado en la ocupación. Gac. Sanit. 1989, 3, 320–326. [Google Scholar] [CrossRef]
- Consell Català de Resusscitació. Test avaluació Suport Vital Bàsic i Desfibrilació Automàtica (SVB-DEA); CCR: Barcelona, Spain, 2010. [Google Scholar]
- Consell Català de Resusscitació. Avaluació pràctica. Seqüència SVB + DEA; CCR: Barcelona, Spain, 2010. [Google Scholar]
- Ballesteros-Peña, S.; Fernández-Aedo, I.; Pérez-Urdiales, I.; García-Azpiazu, Z.; Unanue-Arza, S. Conocimientos y actitudes de los ciudadanos del País Vasco sobre la resucitación cardiopulmonar y los desfibriladores externos automatizados. Med. Intensiva 2016, 40, 75–83. [Google Scholar] [CrossRef]
- Riggs, M.; Franklin, R.; Saylany, L. Associations between cardiopulmonary resuscitation (CPR) knowledge, self-efficacy, training history and willingness to perform CPR and CPR psychomotor skills: A systematic review. Resuscitation 2019, 138, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Carrera, M.J.S.; García, L.M.G.; Nieto, F.B.; Cid, J.L.; Álvarez, A.C. Enseñanza de la reanimación cardiopulmonar básica en población general. Atención Primaria 2004, 34, 408–413. [Google Scholar] [CrossRef]
- Cartledge, S.; Bray, J.E.; Leary, M.; Stub, D.; Finn, J. A systematic review of basic life support training targeted to family members of high-risk cardiac patients. Resuscitation 2016, 105, 70–78. [Google Scholar] [CrossRef]
- García-Suárez, M.; Méndez-Martínez, C.; Martínez-Isasi, S.; Gómez-Salgado, J.; Fernández-García, D. Basic life support training methods for health science students: A systematic review. Int. J. Environ. Res. Public Health 2019, 16, 768. [Google Scholar] [CrossRef] [PubMed]
- Messa, J.B.L. Is the Spanish population aware and capable of acting in response to cardiac arrest? Med. Intensiva 2016, 40, 73–74. [Google Scholar]
- Miró, Ò.; Jiménez-Fábrega, X.; Díaz, N.; Coll-Vinent, B.; Bragulat, E.; Jiménez, S.; Espinosa, G.; Hernández-Rodríguez, J.; García-Alfranca, F.; Álvarez, M.T.; et al. Programa de Reanimación cardiopulmonar Orientado a Centros de Enseñanza Secundaria (PROCES): Análisis de los resultados del estudio piloto. Med. Clin. (BARC) 2005, 124, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.; Ryoo, H.W.; Ahn, J.Y.; Park, J.B.; Lee, D.E.; Kim, J.H.; Jin, S.; Lee, K.W. A 5-year change of knowledge and willingness by sampled respondents to perform bystander cardiopulmonary resuscitation in a metropolitan city. PLoS ONE 2019, 14, e0211804. [Google Scholar] [CrossRef]
- Nishiyama, C.; Kitamura, T.; Sakai, T.; Murakami, Y.; Shimamoto, T.; Kawamura, T.; Yonezawa, T.; Nakai, S.; Marukawa, S.; Sakamoto, T.; et al. Community-wide dissemination of bystander cardiopulmonary resuscitation and automated external defibrillator use using a 45-min chest compression–only cardiopulmonary resuscitation training. J. Am. Heart Assoc. 2019, 8, 1–10. [Google Scholar] [CrossRef]
- Vaillancourt, C.; Charette, M.; Kasaboski, A.; Brehaut, J.C.; Osmond, M.; Wells, G.A.; Stiell, I.G.; Grimshaw, J. Barriers and facilitators to CPR knowledge transfer in an older population most likely to witness cardiac arrest: A theory-informed interview approach. Emerg. Med. J. 2014, 31, 700–705. [Google Scholar] [CrossRef]
- Méndez-Martínez, C.; Martínez-Isasi, S.; García-Suárez, M.; Peña-Rodríguez, M.A.D.L.; Gómez-Salgado, J.; Fernández-García, D. Acquisition of Knowledge and Practical Skills after a Brief Course of BLS-AED in First-Year Students in Nursing and Physiotherapy at a Spanish University. Int. J. Environ. Res. Public Health 2019, 16, 766. [Google Scholar] [CrossRef]
- Basanta Camiño, S.; Navarro Patón, R.; Freire Tellado, M.; Barcala Furelos, R.; Pavón Prieto, M.P.; Fernández López, M.; Neira Pájaro, M.A. Evaluación del conocimiento y de las habilidades para el uso de un Desfibrilador Externo Automatizado (DEA) por estudiantes universitarios. Un diseño cuasiexperimental. Med. Intensiva 2017, 41, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Nordberg, P.; Jonsson, M.; Forsberg, S.; Ringh, M.; Fredman, D.; Riva, G.; Hasselqvist-Ax, I.; Hollenberg, J. The survival benefit of dual dispatch of EMS and fire-fighters in out-of-hospital cardiac arrest may differ depending on population density—A prospective cohort study. Resuscitation 2015, 90, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Myerburg, R.J.; Fenster, J.; Velez, M.; Rosenberg, D.; Lai, S.; Kurlansky, P.; Newton, S.; Knox, M.; Castellanos, A. Impact of community-wide police car deployment of automated external defibrillators on survival from out-of-hospital cardiac arrest. Circulation 2002, 106, 1058–1064. [Google Scholar] [CrossRef] [PubMed]
- Saner, H.; Morger, C.; Eser, P.; von Planta, M. Dual dispatch early defibrillation in out-of-hospital cardiac arrest in a mixed urban-rural population. Resuscitation 2013, 84, 1197–1202. [Google Scholar] [CrossRef] [PubMed]
- Strömsöe, A.; Andersson, B.; Ekström, L.; Herlitz, J.; Axelsson, Å.; Göransson, K.E.; Svensson, L.; Holmberg, S. Education in cardiopulmonary resuscitation in Sweden and its clinical consequences. Resuscitation 2010, 81, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Böttiger, B.W.; Bossaert, L.L.; Castrén, M.; Cimpoesu, D.; Georgiou, M.; Greif, R.; Grünfeld, M.; Lockey, A.; Lott, C.; Maconochie, I.; et al. Kids Save Lives—ERC position statement on school children education in CPR.: “Hands that help—Training children is training for life”. Resuscitation 2016, 105, A1–A3. [Google Scholar]
- Cave, D.M.; Aufderheide, T.P.; Beeson, J.; Ellison, A.; Gregory, A.; Hazinski, M.F.; Hiratzka, L.F.; Lurie, K.G.; Morrison, L.J.; Mosesso, V.N.; et al. Importance and Implementation of Training in Cardiopulmonary Resuscitation and Automated External Defibrillation in Schools. Circulation 2011, 123, 691–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitamura, T.; Kiyohara, K.; Sakai, T.; Matsuyama, T.; Hatakeyama, T.; Shimamoto, T.; Izawa, J.; Fujii, T.; Nishiyama, C.; Kawamura, T.; et al. Public-Access Defibrillation and Out-of-Hospital Cardiac Arrest in Japan. N. Engl. J. Med. 2016, 375, 1649–1659. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Participants (n = 482) % | |
|---|---|
| Age (years) * | 45.7 (2.8) |
| Women | 50.8 |
| Employment status | |
| Currently working | 73.5 |
| Unemployed | 5.8 |
| Retired | 9.5 |
| Housewife | 3.4 |
| Student | 5.8 |
| Disability | 1.3 |
| Social class | |
| Lower class (IV–VI) | 14.1 |
| Middle class (IIIN–IIIM) | 48.7 |
| Upper class (I–II) | 37.2 |
| Group | |
| General population | 60.8 |
| Catalan Police | 13.9 |
| Firefighters | 9.8 |
| National Police | 5.4 |
| Gym instructors | 6.4 |
| Teaching staff | 3.1 |
| University students | 0.6 |
| Group | Question 1 | Question 2 | Question 3 | Question 4 | ||||
|---|---|---|---|---|---|---|---|---|
| Baseline | End | Baseline | End | Baseline | End | Baseline | End | |
| General population * | 60.6 | 93.5 | 88 | 99 | 88.9 | 97.5 | 67.7 | 92.1 |
| Catalan police * | 51.1 | 85.7 | 95.3 | 100 | 90.5 | 100 | 69.4 | 78.8 |
| Firefighters * | 93.3 | 100 | 100 | 100 | 91.5 | 97.6 | 88.9 | 100 |
| National police * | 56.5 | 56.2 | 78.3 | 100 | 73.9 | 60 | 65 | 93.3 |
| Gym instructors * | 74.1 | 91.7 | 93.5 | 100 | 90 | 100 | 63.3 | 92.3 |
| Teaching staff * | 78.6 | 93.3 | 75 | 100 | 93.3 | 100 | 68.3 | 100 |
| University students * | 66.7 | 100 | 100 | 100 | 66.7 | 100 | 66.7 | 100 |
| Participants (n = 361) | |
|---|---|
| Contents | |
| The topics were addressed correctly | 4.60 (0.49) |
| Methodology/Organization | |
| The duration of the training course was appropriate | 4.64 (0.49) |
| Course instructors | |
| The environmental conditions (classroom, furniture, resources used) were adequate to facilitate the training process | 4.63 (0.51) |
| The instructor handled the topics well | 4.73 (0.45) |
| Appreciation | |
| The instructor motivated the participants | 4.75 (0.43) |
| The training course has been useful | 4.77 (0.42) |
| Participants (n = 207) % | |
|---|---|
| Do you know the meaning of OHCA? | 89.9 |
| Would you know how to identify a victim of OHCA? | 86.6 |
| Would you be able to recognize a public access AED device? | 82.1 |
| Have you ever witnessed an OHCA? | 28.5 |
| Have you ever tried to perform basic CPR? | 15.9 |
| Considers important knowledge in basic CPR | 100 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villalobos, F.; Del Pozo, A.; Rey-Reñones, C.; Granado-Font, E.; Sabaté-Lissner, D.; Poblet-Calaf, C.; Basora, J.; Castro, A.; Flores-Mateo, G. Lay People Training in CPR and in the Use of an Automated External Defibrillator, and Its Social Impact: A Community Health Study. Int. J. Environ. Res. Public Health 2019, 16, 2870. https://doi.org/10.3390/ijerph16162870
Villalobos F, Del Pozo A, Rey-Reñones C, Granado-Font E, Sabaté-Lissner D, Poblet-Calaf C, Basora J, Castro A, Flores-Mateo G. Lay People Training in CPR and in the Use of an Automated External Defibrillator, and Its Social Impact: A Community Health Study. International Journal of Environmental Research and Public Health. 2019; 16(16):2870. https://doi.org/10.3390/ijerph16162870
Chicago/Turabian StyleVillalobos, Felipe, Albert Del Pozo, Cristina Rey-Reñones, Ester Granado-Font, David Sabaté-Lissner, Carme Poblet-Calaf, Josep Basora, Antoni Castro, and Gemma Flores-Mateo. 2019. "Lay People Training in CPR and in the Use of an Automated External Defibrillator, and Its Social Impact: A Community Health Study" International Journal of Environmental Research and Public Health 16, no. 16: 2870. https://doi.org/10.3390/ijerph16162870