A Scoping Review Mapping Research on Green Space and Associated Mental Health Benefits


Abstract
:1. Introduction
2. Materials and Methods
- Identifying the research question(s);
- Identifying relevant studies;
- Study selection;
- Charting the data;
- Collating, summarizing, and reporting the results.
- How do different types of GS (recreational, residential, urban, rural) affect HWB and how much green space is needed for health improvement?
- How can we best define, measure, and quantify GS and mental HWB?
- Do different co-exposures or contextual factors affect the mental HWB outcome?
- Do different age groups and population subgroups benefit differently from exposure to GS?
3. Results
3.1. Numerical Analysis
3.2. Thematic Analysis
3.3. Analysis of Study Design
4. Discussion
- Different types of GS in many contexts and different environments have a positive effect on mental HWB (RQ 1 & 3);
- For a variety of different groups of people (RQ 4), GS does have a positive effect on mental HWB;
- Different types of GS affect the HWB of individuals in different ways (RQ 1 & 4).
- ‘Realise our abilities, live a life with purpose and meaning, and make a positive contribution to our communities;
- Form positive relationships with others, and feel connected and supported;
- Experience peace of mind, contentment, happiness and joy;
- Cope with life’s ups and downs and be confident and resilient;
- Take responsibility for oneself and for others as appropriate.’
- Quantity of greenery or natural elements;
- Type of vegetation (creating shade or not/natural daylight);
- Whether the environment is natural or managed;
- Quantity of built elements;
- Traffic noise and air pollution levels;
- General soundscape;
- Number of people present in the environment;
- Setting and context.
- Description of aim and research question(s);
- Description of the study design;
- Description of participant type (incl. sex, mean age, min/max age, population subgroup characteristics and other relevant socioeconomic characteristics);
- Description of recruitment process;
- Careful description and quantification of the GS investigated (study sites);
- Clear definition of the mental HWB endpoint(s);
- Justification of the choice of tools to assess the health endpoint;
- Measurement of contextual factors and co-exposures.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bang, K.S.; Lee, I.; Kim, S.; Lim, C.S.; Joh, H.K.; Park, B.J.; Song, M.K. The effects of a campus forest-walking program on undergraduate and graduate students’ physical and psychological health. Int. J. Environ. Res. Public Health 2017, 14. [Google Scholar] [CrossRef] [PubMed]
- Oh, B.; Lee, K.J.; Zaslawski, C.; Yeung, A.; Rosenthal, D.; Larkey, L.; Back, M. Health and well-being benefits of spending time in forests: Systematic review. Environ. Health Prev. Med. 2017, 22. [Google Scholar] [CrossRef] [PubMed]
- Elmendorf, W. The importance of trees and nature in community: A review of the relative literature. Arboric. Urban For. 2008, 34, 152–156. [Google Scholar]
- Gascon, M.; Triguero-Mas, M.; Martinez, D.; Dadvand, P.; Forns, J.; Plasencia, A.; Nieuwenhuijsen, M.J. Mental health benefits of long-term exposure to residential green and blue spaces: A systematic review. Int. J. Environ. Res. Public Health 2015, 12, 4354–4379. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, A.; Gobster, P.H. Shades of green: Measuring the ecology of urban green space in the context of human health and well-being. Nat. Cult. 2010, 5, 338–363. [Google Scholar] [CrossRef]
- van den Bosch, M.; Ode Sang, Å. Urban natural environments as nature-based solutions for improved public health—A systematic review of reviews. Environ. Res. 2017, 158, 373–384. [Google Scholar] [CrossRef] [PubMed]
- Kondo, M.C.; Fluehr, J.M.; McKeon, T.; Branas, C.C. Urban green space and its impact on human health. Int. J. Environ. Res. Public Health 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Douglas, O.; Lennon, M.; Scott, M. Green space benefits for health and well-being: A life-course approach for urban planning, design and management. Cities 2017, 66, 53–62. [Google Scholar] [CrossRef] [Green Version]
- Hartig, T.; Mitchell, R.; de Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [PubMed]
- Okvat, H.A.; Zautra, A.J. Community gardening: A parsimonious path to individual, community, and environmental resilience. Am. J. Community Psychol. 2011, 47, 374–387. [Google Scholar] [CrossRef] [PubMed]
- Whear, R.; Coon, J.T.; Bethel, A.; Abbott, R.; Stein, K.; Garside, R. What is the impact of using outdoor spaces such as gardens on the physical and mental well-being of those with dementia? A systematic review of quantitative and qualitative evidence. J. Am. Med. Dir. Assoc. 2014, 15, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Wright, S.D.; Wadsworth, A.M. Gray and green revisited: A multidisciplinary perspective of gardens, gardening, and the aging process. J. Aging Res. 2014, 2014, 13. [Google Scholar] [CrossRef] [PubMed]
- Detweiler, M.B.; Sharma, T.; Detweiler, J.G.; Murphy, P.F.; Lane, S.; Carman, J.; Chudhary, A.S.; Halling, M.H.; Kim, K.Y. What is the evidence to support the use of therapeutic gardens for the elderly? Psychiatry Investig. 2012, 9, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Choi, H.; Bang, K.S.; Kim, S.; Song, M.; Lee, B. Effects of forest therapy on depressive symptoms among adults: A systematic review. Int. J. Environ. Res. Public Health 2017, 14. [Google Scholar] [CrossRef]
- van den Berg, M.; Wendel-Vos, W.; van Poppel, M.; Kemper, H.; van Mechelen, W.; Maas, J. Health benefits of green spaces in the living environment: A systematic review of epidemiological studies. Urban For. Urban Green. 2015, 14, 806–816. [Google Scholar] [CrossRef]
- Tzoulas, K.; Korpela, K.; Venn, S.; Yli-Pelkonen, V.; Kazmierczak, A.; Niemela, J.; James, P. Promoting ecosystem and human health in urban areas using green infrastructure: A literature review. Landsc. Urban Plan. 2007, 81, 167–178. [Google Scholar] [CrossRef]
- Sandifer, P.A.; Sutton-Grier, A.E.; Ward, B.P. Exploring connections among nature, biodiversity, ecosystem services, and human health and well-being: Opportunities to enhance health and biodiversity conservation. Ecosyst. Serv. 2015, 12, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Jennings, V.; Larson, L.; Yun, J. Advancing sustainability through urban green space: Cultural ecosystem services, equity, and social determinants of health. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef]
- Taylor, L.; Hochuli, D.F. Defining greenspace: Multiple uses across multiple disciplines. Landsc. Urban Plan. 2017, 158, 25–38. [Google Scholar] [CrossRef] [Green Version]
- Lederbogen, F.; Kirsch, P.; Haddad, L.; Streit, F.; Tost, H.; Schuch, P.; Wust, S.; Pruessner, J.C.; Rietschel, M.; Deuschle, M.; et al. City living and urban upbringing affect neural social stress processing in humans. Nature 2011, 474, 498–501. [Google Scholar] [CrossRef]
- Wang, J.L. Rural-urban differences in the prevalence of major depression and associated impairment. Soc. Psychiatry Psychiatr. Epidemiol. 2004, 39, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Peen, J.; Schoevers, R.A.; Beekman, A.T.; Dekker, J. The current status of urban-rural differences in psychiatric disorders. Acta Psychiatr. Scand. 2010, 121, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.J.; Richardson, E.A.; Shortt, N.K.; Pearce, J.R. Neighborhood environments and socioeconomic inequalities in mental well-being. Am. J. Prev. Med. 2015, 49, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Triguero-Mas, M.; Dadvand, P.; Cirach, M.; Martínez, D.; Medina, A.; Mompart, A.; Basagaña, X.; Gražulevičienė, R.; Nieuwenhuijsen, M.J. Natural outdoor environments and mental and physical health: Relationships and mechanisms. Environ. Int. 2015, 77, 35–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alcock, I.; White, M.P.; Lovell, R.; Higgins, S.L.; Osborne, N.J.; Husk, K.; Wheeler, B.W. What accounts for ‘england’s green and pleasant land’? A panel data analysis of mental health and land cover types in rural England. Landsc. Urban Plan. 2015, 142, 38–46. [Google Scholar] [CrossRef]
- Butler, S.S.; Cohen, A.L. The importance of nature in the well-being of rural elders. Nat. Cult. 2010, 5, 150–174. [Google Scholar] [CrossRef]
- Hansen-Ketchum, P.A.; Marck, P.; Reutter, L.; Ha’penny, E. Strengthening access to restorative places: Findings from a participatory study on engaging with nature in the promotion of health. Health Place 2011, 17, 558–571. [Google Scholar] [CrossRef] [PubMed]
- Pretty, J.; Peacock, J.; Hine, R.; Sellens, M.; South, N.; Griffin, M. Green exercise in the UK countryside: Effects on health and psychological well-being, and implications for policy and planning. J. Environ. Plan. Manag. 2007, 50, 211–231. [Google Scholar] [CrossRef]
- Gilbert, A.; Colley, K.; Roberts, D. Are rural residents happier? A quantitative analysis of subjective wellbeing in Scotland. J. Rural Stud. 2016, 44, 37–45. [Google Scholar] [CrossRef]
- Weich, S.; Twigg, L.; Lewis, G. Rural/non-rural differences in rates of common mental disorders in Britain —Prospective multilevel cohort study. Br. J. Psychiatry 2006, 188, 51–57. [Google Scholar] [CrossRef]
- Verheij, R.A.; Maas, J.; Groenewegen, P.P. Urban-rural health differences and the availability of green space. Eur. Urban Reg. Stud. 2008, 15, 307–316. [Google Scholar] [CrossRef]
- Kohlleppel, T.; Bradley, J.C.; Jacob, S. A walk through the garden: Can a visit to a botanic garden reduce stress? HortTechnology 2002, 12, 489–492. [Google Scholar] [CrossRef]
- Carrus, G.; Scopelliti, M.; Panno, A.; Lafortezza, R.; Colangelo, G.; Pirchio, S.; Ferrini, F.; Salbitano, F.; Agrimi, M.; Portoghesi, L.; et al. A different way to stay in touch with ‘urban nature’: The perceived restorative qualities of botanical gardens. Front. Psychol. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Kreski, B. Healing and empowering veterans in a botanic garden. J. Mus. Educ. 2016, 41, 110–115. [Google Scholar] [CrossRef]
- Adevi, A.A.; Lieberg, M. Stress rehabilitation through garden therapy a caregiver perspective on factors considered most essential to the recovery process. Urban For. Urban Green. 2012, 11, 51–58. [Google Scholar] [CrossRef]
- Sahlin, E.; Ahlborg, G.; Tenenbaum, A.; Grahn, P. Using nature-based rehabilitation to restart a stalled process of rehabilitation in individuals with stress-related mental illness. Int. J. Environ. Res. Public Health 2015, 12, 1928–1951. [Google Scholar] [CrossRef] [PubMed]
- Sahlin, E.; Ahlborg, G.; Matuszczyk, J.V.; Grahn, P. Nature-based stress management course for individuals at risk of adverse health effects from work-related stress-effects on stress related symptoms, workability and sick leave. Int. J. Environ. Res. Public Health 2014, 11, 6586–6611. [Google Scholar] [CrossRef]
- Adevi, A.A.; Mårtensson, F. Stress rehabilitation through garden therapy: The garden as a place in the recovery from stress. Urban For. Urban Green. 2013, 12, 230–237. [Google Scholar] [CrossRef]
- Gonzalez, M.T.; Hartig, T.; Patil, G.G.; Martinsen, E.W.; Kirkevold, M. Therapeutic horticulture in clinical depression: A prospective study of active components. J. Adv. Nurs. 2010, 66, 2002–2013. [Google Scholar] [CrossRef]
- Grabbe, L.; Ball, J.; Goldstein, A. Gardening for the mental well-being of homeless women. J. Holist. Nurs. 2013, 31, 258–266. [Google Scholar] [CrossRef]
- Parkinson, S.; Lowe, C.; Vecsey, T. The therapeutic benefits of horticulture in a mental health service. Br. J. Occup. Ther. 2011, 74, 525–534. [Google Scholar] [CrossRef]
- Baybutt, M.; Chemlal, K. Health-promoting prisons: Theory to practice. Glob. Health Promot. 2016, 23, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Edwards, C.A.; McDonnell, C.; Merl, H. An evaluation of a therapeutic garden’s influence on the quality of life of aged care residents with dementia. Dementia 2013, 12, 494–510. [Google Scholar] [CrossRef]
- Hawkins, J.L.; Mercer, J.; Thirlaway, K.J.; Clayton, D.A. ‘Doing’ gardening and ‘being’ at the allotment site: Exploring the benefits of allotment gardening for stress reduction and healthy aging. Ecopsychology 2013, 5, 110–125. [Google Scholar] [CrossRef]
- Burton, E.; Mitchell, L.; Stride, C. Bed of roses? The role of garden space in older people’s well-being. Proc. Inst. Civ. Eng.—Urban Des. Plan. 2015, 168, 164–173. [Google Scholar] [CrossRef]
- McMahan, E.A.; Estes, D. The effect of contact with natural environments on positive and negative affect: A meta-analysis. J. Posit. Psychol. 2015, 10, 507–519. [Google Scholar] [CrossRef]
- Wild, C.P. Complementing the genome with an “exposome”: The outstanding challenge of environmental exposure measurement in molecular epidemiology. Cancer Epidemiol. Biomark. 2005, 14, 1847–1850. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Bingley, A. Woodland as working space: Where is the restorative green idyll? Soc. Sci. Med. 2013, 91, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Gatersleben, B.; Andrews, M. When walking in nature is not restorative—The role of prospect and refuge. Health Place 2013, 20, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Wahrborg, P.; Petersson, I.F.; Grahn, P. Nature-assisted rehabilitation for reactions to severe stress and/or depression in a rehabilitation garden: Long-term follow-up including comparisons with a matched population-based reference cohort. J. Rehabil. Med. 2014, 46, 271–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewi, N.S.; Komatsuzaki, M.; Yamakawa, Y.; Takahashi, H.; Shibanuma, S.; Yasue, T.; Okayama, T.; Toyoda, A.; Shimonishi, H.; Sasaki, S. Community gardens as health promoters: Effects on mental and physical stress levels in adults with and without mental disabilities. Sustainability 2017, 9. [Google Scholar] [CrossRef]
- Hawkins, J.L.; Thirlaway, K.J.; Backx, K.; Clayton, D.A. Allotment gardening and other leisure activities for stress reduction and healthy aging. HortTechnology 2011, 21, 577–585. [Google Scholar] [CrossRef]
- Park, S.A.; Lee, A.Y.; Son, K.C.; Lee, W.L.; Kim, D.S. Gardening intervention for physical and psychological health benefits in elderly women at community centers. HortTechnology 2016, 26, 474–483. [Google Scholar] [CrossRef]
- Soga, M.; Cox, D.T.C.; Yamaura, Y.; Gaston, K.J.; Kurisu, K.; Hanaki, K. Health benefits of urban allotment gardening: Improved physical and psychological well-being and social integration. Int. J. Environ. Res. Public Health 2017, 14. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, A.E.; Maas, J.; Verheij, R.A.; Groenewegen, P.P. Green space as a buffer between stressful life events and health. Soc. Sci. Med. 2010, 70, 1203–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Im, S.G.; Choi, H.; Jeon, Y.H.; Song, M.K.; Kim, W.; Woo, J.M. Comparison of effect of two-hour exposure to forest and urban environments on cytokine, anti-oxidant, and stress levels in young adults. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.H.; Woo, J.M.; Ryu, J.S. Effect of a forest therapy program and the forest environment on female workers’ stress. Urban For. Urban Green. 2015, 14, 274–281. [Google Scholar] [CrossRef]
- Lee, J.; Park, B.J.; Tsunetsugu, Y.; Kagawa, T.; Miyazaki, Y. Restorative effects of viewing real forest landscapes, based on a comparison with urban landscapes. Scand. J. For. Res. 2009, 24, 227–234. [Google Scholar] [CrossRef]
- Chun, M.H.; Chang, M.C.; Lee, S.-J. The effects of forest therapy on depression and anxiety in patients with chronic stroke. Int. J. Neurosci. 2017, 127, 199–203. [Google Scholar] [CrossRef]
- Sung, J.; Woo, J.-M.; Kim, W.; Lim, S.-K.; Chung, E.-J. The effect of cognitive behavior therapy-based “forest therapy” program on blood pressure, salivary cortisol level, and quality of life in elderly hypertensive patients. Clin. Exp. Hypertens. 2012, 34, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.M.; Lee, Y.J.; Kim, J.Y.; Yoon, S.B.; Shin, C.S. Effects of forest therapy camp on quality of life and stress in postmenopausal women. For. Sci. Technol. 2016, 12, 125–129. [Google Scholar] [CrossRef]
- Eriksson, T.; Westerberg, Y.; Jonsson, H. Experiences of women with stress-related ill health in a therapeutic gardening program. Can. J. Occup. Ther. 2011, 78, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Korpela, K.; Hartig, T. Restorative qualities of favorite places. J. Environ. Psychol. 1996, 16, 221–233. [Google Scholar] [CrossRef]
- Hartig, T.; Korpela, K.; Evans, G.W.; Gärling, T. A measure of restorative quality in environments. Scand. Hous. Plan. Res. 1997, 14, 175–194. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect—The panas scales. J. Personal. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, D.P.; Hillier, V.F. Scaled version of the general health questionnaire. Psychol. Med. 1979, 9, 139–145. [Google Scholar] [CrossRef]
- Stewart-Brown, S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Weich, S. Internal construct validity of the warwick-edinburgh mental well-being scale (WEMWBS): A Rasch analysis using data from the scottish health education population survey. Health Qual. Life Outcomes 2009, 7. [Google Scholar] [CrossRef]
- Ware, J.E.; Sherbourne, C.D. The mos 36-item short-form health survey (sf-36):1. Conceptual-framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Beck, A.T.; Rial, W.Y.; Rickels, K. Short form of depression inventory: Cross-validation. Psychol. Rep. 1974, 34, 1184–1186. [Google Scholar] [PubMed]
- Beck, A.T.; Steer, R.A. Internal consistencies of the original and revised beck depression inventory. J. Clin. Psychol. 1984, 40, 1365–1367. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Grove, J.R.; Prapavessis, H. Preliminary evidence for the reliability and validity of an abbreviated profile of mood states. Int. J. Sport Psychol. 1992, 23, 93–109. [Google Scholar]
- Mcnair, D.M. Citation classic-manual for the profile of mood states. Curr. Contents/Soc. Behav. Sci. 1984, 27, 20. [Google Scholar]
- McNair, D.M. Profile of mood states (poms) in evaluation of antianxiety and antidepressant drugs. J. Pharmacol. 1974, 5, 10. [Google Scholar]
- Mayer, F.S.; Frantz, C.M. The connectedness to nature scale: A measure of individuals’ feeling in community with nature. J. Environ. Psychol. 2004, 24, 503–515. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. Manual for the State-Trait Anxiety Inventory; Consulting Psychologist Press: Mountain View, CA, USA, 1970. [Google Scholar]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Cimprich, B. Development of an intervention to restore attention in cancer-patients. Cancer Nurs. 1993, 16, 83–92. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.T.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- The Whoqol Group. The World Health Organization quality of life assessment (WHOQOL): Development and general psychometric properties. Soc. Sci. Med. 1998, 46, 1569–1585. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the beck depression and anxiety inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Primary, P.H.Q. Validation and utility of a self-report version of PRIME-MD—The PHQ primary care study. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Melamed, S.; Ugarten, U.; Shirom, A.; Kahana, L.; Lerman, Y.; Froom, P. Chronic burnout, somatic arousal and elevated salivary cortisol levels. J. Psychosom. Res. 1999, 46, 591–598. [Google Scholar] [CrossRef]
- Ryan, R.M.; Frederick, C. On energy, personality, and health: Subjective vitality as a dynamic reflection of well-being. J. Personal. 1997, 65, 529–565. [Google Scholar] [CrossRef]
- Sheikh, J.I.; Yesavage, J.A. Geriatric depression scale (GDS): Recent evidence and development of a shorter version. J. Aging Ment. Health 1986, 5, 165–173. [Google Scholar]
- Jenkinson, C.; Layte, R.; Coulter, A.; Wright, L. Evidence for the sensitivity of the SF-36 health status measure to inequalities in health: Results from the Oxford healthy lifestyles survey. J. Epidemiol. Community Health 1996, 50, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, C.; Layte, R.; Jenkinson, D.; Lawrence, K.; Petersen, S.; Paice, C.; Stradling, J. A shorter form health survey: Can the SF-12 replicate results from the SF-36 in longitudinal studies? J. Public Health Med. 1997, 19, 179–186. [Google Scholar] [CrossRef]
- Williams, A. Euroqol—A new facility for the measurement of health-related quality-of-life. Health Policy 1990, 16, 199–208. [Google Scholar]
- Schultz, P.W. Inclusion with nature: The psychology of human-nature relations. In Psychology of Sustainable Development; Schmuck, P., Schultz, W.P., Eds.; Kluwer Academic Publishers: Norwell, MA, USA, 2002; pp. 61–78. [Google Scholar]
- Ryff, C.D. Happiness is everything, or is it—Explorations on the meaning of psychological well-being. J. Personal. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Elo, A.-L.; Dallner, M.; Gamberale, F.; Hottinen, V.; Knardahl, S.; Lindström, K.; Skogstad, A.; Ørhede, E. Validation of the nordic questionnaire for psychological and social factors at work—QPSNordic. In Innovative Theories, Tools, and Practices in Work and Organizational Psychology; Vartiainen, M., Avallone, F., Anderson, N., Eds.; Hogrefe & Huber Publishers: Ashland, OH, USA, 2000; pp. 47–57. [Google Scholar]
- Beck, A.T.; Brown, G.; Epstein, N.; Steer, R.A. An inventory for measuring clinical anxiety—Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Rumpf, H.J.; Meyer, C.; Hapke, U.; John, U. Screening for mental health: Validity of the MHI-5 using DSM-IV Axis I psychiatric disorders as gold standard. Psychiatry Res. 2001, 105, 243–253. [Google Scholar] [CrossRef]
- Pangman, V.C.; Sloan, J.; Guse, L. An examination of psychometric properties of the mini-mental state examination and the standardized mini-mental state examination: Implications for clinical practice. Appl. Nurs. Res. 2000, 13, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Sonnentag, S.; Fritz, C. The recovery experience questionnaire: Development and validation of a measure for assessing recuperation and unwinding from work. J. Occup. Health Psychol. 2007, 12, 204–221. [Google Scholar] [CrossRef] [PubMed]
- Trapnell, P.D.; Campbell, J.D. Private self-consciousness and the five-factor model of personality: Distinguishing rumination from reflection. J. Personal. Soc. Psychol. 1999, 76, 284–304. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B.; Salanova, M. The measurement of work engagement with a short questionnaire—A cross-national study. Educ. Psychol. Meas. 2006, 66, 701–716. [Google Scholar] [CrossRef]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Personal. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef]
- Hardy, C.J.; Rejeski, W.J. Not what, but how one feels—The measurement of affect during exercise. J. Sport Exerc. Psychol. 1989, 11, 304–317. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Smith, J.A. Beyond the divide between cognition and discourse: Using interpretative phenomenological analysis in health psychology. Psychol. Health 1996, 11, 261–271. [Google Scholar] [CrossRef]
- Eriksen, H.R.; Ihlebaek, C.; Ursin, H. A scoring system for Subjective Health Complaints (SHC). Scand. J. Public Health 1999, 27, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Neugarten, B.L.; Havighurst, R.J.; Tobin, S.S. The measurement of life satisfaction. J. Gerontol. 1961, 16, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Diener, E.; Biswas-Diener, R. Happiness: Unlocking the Mysteries of Psychological Wealth; Blackwell Publishing: Malden, MA, USA, 2008. [Google Scholar]
- Zuckerman, M. Development of a situation-specific trait-state test for prediction and measurement of affective responses. J. Consult. Clin. Psychol. 1977, 45, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.A.; Ward, L.M.; Pratt, G. Affective quality attributed to environments—A factor analytic study. Environ. Behav. 1981, 13, 259–288. [Google Scholar] [CrossRef]
- Kyle, G.; Graefe, A.; Manning, R. Testing the dimensionality of place attachment in recreational settings. Environ. Behav. 2005, 37, 153–177. [Google Scholar] [CrossRef]
- Abele-Brehm, A.; Brehm, W. Zur konzeptualisierung und messung von befindlichkeit. Die entwicklung der “befindlichkeitsskalen” (BFS) [the conceptualization and measurement of mood: The development of the ‘Mood Survey.’]. Diagnostica 1986, 32, 209–228. [Google Scholar]
- Zhang, J.X.; Schwarzer, R. Measuring optimistic self-beliefs—A Chinese adaptation of the general self-efficacy scale. Psychologia 1995, 38, 174–181. [Google Scholar]
- Clifton, R.A.; Etcheverry, E.; Hasinoff, S.; Roberts, L.W. Measuring the cognitive domain of the quality of life of university students. Soc. Indic. Res. 1996, 38, 29–52. [Google Scholar] [CrossRef]
- Roberts, L.W.; Clifton, R.A. Measuring the affective quality-of-life of university-students—The validation of an instrument. Soc. Indic. Res. 1992, 27, 113–137. [Google Scholar] [CrossRef]
- Becker, P. Der Trier Personlichkeitsfragebogen [Trier Personality Questionnaire]; Hogrefe: Göttingen, Germany, 1989. [Google Scholar]
- Bradburn, N.M. Bradburn Scale of Psychological Well-Being; Aldine: Chicago, IL, USA, 1969. [Google Scholar]
- Cimprich, B.; Visovatti, M.; Ronis, D.L. The attentional function index-a self-report cognitive measure. Psychooncology 2011, 20, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Cosco, N.G.; Moore, R.C.; Islam, M.Z. Behavior mapping: A method for linking preschool physical activity and outdoor design. Med. Sci. Sports Exerc. 2010, 42, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Saucier, G. Mini-markers: A brief version of goldberg’s unipolar Big-Five markers. J. Personal. Assess. 1994, 63, 506–516. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R.; Melisaratos, N. The brief symptom inventory: An introductory report. Psychol. Med. 1983, 13, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Treynor, W.; Gonzalez, R.; Nolen-Hoeksema, S. Rumination reconsidered: A psychometric analysis. Cognit. Ther. Res. 2003, 27, 247–259. [Google Scholar] [CrossRef]
- Buss, A.H.; Perry, M. The aggression questionnaire. J. Personal. Soc. Psychol. 1992, 63, 452–459. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Lipson, S.; Werner, P.; Billig, N.; Taylor, L.; Woosley, R. Withdrawal of haloperidol, thioridazine, and lorazepam in the nursing home—A controlled, double-blind study. Arch. Intern. Med. 1999, 159, 1733–1740. [Google Scholar] [CrossRef] [PubMed]
- Cox, R.H.; Martens, M.P.; Russell, W.D. Measuring anxiety in athletics: The revised competitive state anxiety inventory-2. J. Sport Exerc. Psychol. 2003, 25, 519–533. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Alexopoulos, G.S.; Abrams, R.C.; Young, R.C.; Shamoian, C.A. Cornell scale for depression in dementia. Biol. Psychiatry 1988, 23, 271–284. [Google Scholar] [CrossRef]
- Brantley, P.J.; Waggoner, C.D.; Jones, G.N.; Rappaport, N.B. A daily stress inventory—Development, reliability, and validity. J. Behav. Med. 1987, 10, 61–74. [Google Scholar] [CrossRef]
- Brod, M.; Stewart, A.L.; Sands, L.; Walton, P. Conceptualization and measurement of quality of life in dementia: The dementia quality of life instrument (DQOL). Gerontologist 1999, 39, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Steer, R.A. Modal profile analyses of the SCL-90-r for 7 mental-disorders. Multivar. Exp. Clin. Res. 1983, 6, 55–67. [Google Scholar]
- Maloney, M.P.; Ward, M.P.; Braucht, G.N. Psychology in action—Revised scale for measurement of ecological attitudes and knowledge. Am. Psychol. 1975, 30, 787–790. [Google Scholar] [CrossRef]
- Vincenti, G.E. Edinburgh post-natal depression scale. Br. J. Psychiatry 1987, 151, 865. [Google Scholar] [CrossRef] [PubMed]
- Huta, V.; Ryan, R.M. Pursuing pleasure or virtue: The differential and overlapping well-being benefits of hedonic and eudaimonic motives. J. Happiness Stud. 2010, 11, 735–762. [Google Scholar] [CrossRef]
- Gauvin, L.; Rejeski, W.J. The exercise-induced feeling inventory—Development and initial validation. J. Sport Exerc. Psychol. 1993, 15, 403–423. [Google Scholar] [CrossRef]
- Gauvin, L.; Szabo, A. Application of the experience sampling method to the study of the effects of exercise withdrawal on weil-being. J. Sport Exerc. Psychol. 1992, 14, 361–374. [Google Scholar] [CrossRef]
- Svebak, S.; Murgatroyd, S. Metamotivational dominance: A multimethod validation of reversal theory constructs. J. Personal. Soc. Psychol. 1985, 48, 107–116. [Google Scholar] [CrossRef]
- Gagnon Thompson, S.C.; Barton, M.A. Ecocentric and anthropocentric attitudes toward the environment. J. Environ. Psychol. 1994, 14, 149–157. [Google Scholar] [CrossRef]
- Kaiser, F.G. General measure of ecological behavior. J. Appl. Soc. Psychol. 1998, 28, 395–422. [Google Scholar] [CrossRef]
- Kozma, A.; Stones, M.J. The measurement of happiness—Development of the memorial-university-of-newfoundland scale of happiness (munsh). J. Gerontol. 1980, 35, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Seo, H.M.; Hah, Y.S. A study of factors influencing on health promiting lifestyle in the elderly-application of pender’s health promotion model. J. Korean Acad. Nurs. 2004, 34, 1288–1297. [Google Scholar] [CrossRef]
- Thake, C.L.; Bambling, M.; Edirippulige, S.; Marx, E. A psychoevolutionary approach to identifying preferred nature scenes with potential to provide restoration from stress. HERD—Health Environ. Res. Des. J. 2017, 10, 111–124. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Mermelstein, R.; Kamarck, T.; Hoberman, H. Measuring the functional components of social support. In Social Support: Theory, Research and Applications; Sarason, I.G., Sarason, B.R., Eds.; Martinus Nijhoff Publishers: Dordrecht, The Netherlands, 1985; pp. 73–94. [Google Scholar]
- Vagg, P.R.; Spielberger, C.D. The job stress survey: Assessing perceived severity and frequency of occurrence of generic sources of stress in the workplace. J. Occup. Health Psychol. 1999, 4, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Olsen, L.R.; Mortensen, E.L.; Bech, P. The SCL-90 and SCL-90R versions validated by item response models in a Danish community sample. Acta Psychiatr. Scand. 2004, 110, 225–229. [Google Scholar] [CrossRef]
- Forsell, Y. The major depression inventory versus schedules for clinical assessment in neuropsychiatry in a population sample. Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 209–213. [Google Scholar] [CrossRef]
- Priebe, S.; Huxley, P.; Knight, S.; Evans, S. Application and results of the Manchester Short Assessment of Quality of Life (MANSA). Int. J. Soc. Psychiatry 1999, 45, 7–12. [Google Scholar] [CrossRef]
- Crowne, D.P.; Marlowe, D. A new scale of social desirability independent of psychopathology. J. Consult. Psychol. 1960, 24, 349–354. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach burnout inventory. In Evaluating Stress: A Book of Resources, 3rd ed.; Zalaquett, C.P., Wood, R.J., Eds.; Scarecrow Press: Lanham, MD, USA, 1997; pp. 191–218. [Google Scholar]
- Sheehan, D.V.; Janavs, J.; Baker, R.; Harnett-Sheehan, K.; Knapp, E.; Sheehan, M.; Lecrubier, Y.; Weiller, E.; Hergueta, T.; Amorim, P.; et al. MINI—Mini international neuropsychiatric interview—English version 5.0.0—DSM-IV. J. Clin. Psychiatry 1998, 59, 34–57. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The mini-international neuropsychiatric interview (MINI): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar]
- Steyer, R.; Schwenkmezger, P.; Notz, P.; Eid, M. Der Mehrdimensionale Befindlichkeitsfragebogen (MDBF) [the Multidimensional Comfort Questionnaire (MDBF)]; Hogrefe: Göttingen, Germany, 1997. [Google Scholar]
- Terasaki, M.; Kishimoto, Y.; Koga, A. Construction of a multiple mood scale. Jpn. J. Psychol. 1992, 62, 350–356. [Google Scholar] [CrossRef]
- Largo-Wight, E.; Chen, W.W.; Dodd, V.; Weiler, R. The nature contact questionnaire: A measure of healthy workplace exposure. Work 2011, 40, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Scott, B.; Brandberg, M.; Ohman, A. Measuring the negative mood component of stress experiences: Description and psychometric properties of a short adjective check-list of stress responses. Scand. J. Psychol. 2001, 42, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Francis, L.J.; Brown, L.B.; Lester, D.; Philipchalk, R. Happiness as stable extraversion: A cross-cultural examination of the reliability and validity of the Oxford happiness inventory among students in the UK, USA, Australia, and Canada. Personal. Individ. Differ. 1998, 24, 167–171. [Google Scholar] [CrossRef]
- Campbell, A.; Converse, P.E.; Rodgers, W.L. The Quality of American Life: Perceptions, Evaluations, and Satisfactions; Russell Sage Foundation: New York, NY, USA, 1976. [Google Scholar]
- Robitschek, C. Personal growth initiative: The construct and its measure. Meas. Eval. Couns. Dev. 1998, 30, 183–198. [Google Scholar]
- Lafortezza, R.; Carrus, G.; Sanesi, G.; Davies, C. Benefits and well-being perceived by people visiting green spaces in periods of heat stress. Urban For. Urban Green. 2009, 8, 97–108. [Google Scholar] [CrossRef]
- Dupuy, H. The psychological general wellbeing (PGWB) index. In Assessment of Quality of Life in Clinical Trials of Cardiovascular Therapies; Wenger, N.K., Mattson, M.E., Furberg, C.D., Elinson, J., Eds.; Le Jacq Publishing: New York, NY, USA, 1984; pp. 170–183. [Google Scholar]
- Andereck, K.L.; Nyaupane, G. Development of a tourism and quality-of-life instrument. Soc. Indic. Res. Ser. 2011, 43, 95–113. [Google Scholar] [CrossRef]
- Andereck, K.L.; Nyaupane, G.P. Exploring the nature of tourism and quality of life perceptions among residents. J. Travel Res. 2011, 50, 248–260. [Google Scholar] [CrossRef]
- Pang, S.M.C.; Chan, K.S.; Chung, B.P.M.; Lau, K.S.; Leung, E.M.F.; Leung, A.W.K.; Chan, H.Y.L.; Chan, T.M.F. Assessing quality of life of patients with advanced chronic obstructive pulmonary disease in the end of life. J. Palliat. Care 2005, 21, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Pang, S.M.C.; Tse, C.; Chan, K.; Chung, B.P.M.; Leung, A.K.A.; Leung, E.M.F.; Ko, S.K.K. An empirical analysis of the decision-making of limiting life-sustaining treatment for patients with advanced chronic obstructive pulmonary disease in Hong Kong, China. J. Crit. Care 2004, 19, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Burckhardt, C.S.; Woods, S.L.; Schultz, A.A.; Ziebarth, D.M. Quality of life of adults with chronic illness—A psychometric study. Res. Nurs. Health 1989, 12, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Dunbar, G.C.; Stoker, M.J.; Hodges, T.C.P.; Beaumont, G. The development of SBQUL: A unique scale for measuring quality of life. Br. J. Med. Econ. 1992, 2, 65–74. [Google Scholar]
- Kim, K.Y.; Chun, B.Y.; Kam, S.; Lee, S.W.; Park, K.S.; Chae, S.C. Development of measurement scale for the quality of life in hypertensive patients. J. Prev. Med. Public Health 2005, 38, 61–70. [Google Scholar]
- Waterman, A.S.; Schwartz, S.J.; Zamboanga, B.L.; Ravert, R.D.; Williams, M.K.; Agocha, V.B.; Kim, S.Y.; Donnellan, M.B. The questionnaire for eudaimonic well-being: Psychometric properties, demographic comparisons, and evidence of validity. J. Posit. Psychol. 2010, 5, 41–61. [Google Scholar] [CrossRef]
- Hays, R.D.; Sherbourne, C.D.; Mazel, R.M. User’s Manual for the Medical Outcomes Study (MOS) Core Measures of Health-Related Quality of Life; RAND Corporation: Santa Monica, CA, USA, 1995. [Google Scholar]
- McDowell, I.; Newell, C. Measuring Health: A Guide to Rating Scales and Questionnaires, 2nd ed.; Oxford University Press: Oxford, UK, 1996. [Google Scholar]
- Crompton, J.L. Motivations for pleasure vacation. Ann. Tour. Res. 1979, 6, 408–424. [Google Scholar] [CrossRef]
- Mill, R.C.M.; Morrison, A.M. The Tourism System: An Introductory Text; Prentice-Hall: Englewood Cliffs, NJ, USA, 1985. [Google Scholar]
- Pearce, P.L.; Lee, U.-I. Developing the travel career approach to tourist motivation. J. Travel Res. 2005, 43, 226–237. [Google Scholar] [CrossRef]
- Tinsley, H.E.A.; Kass, R.A.; Driver, B.L. Reliability and concurrent validity of the recreation experience preference scales. Educ. Psychol. Meas. 1981, 41, 897–907. [Google Scholar] [CrossRef]
- Korpela, K.M.; Ylen, M.; Tyrvainen, L.; Silvennoinen, H. Determinants of restorative experiences in everyday favorite places. Health Place 2008, 14, 636–652. [Google Scholar] [CrossRef] [Green Version]
- Korpela, K.M.; Ylen, M.P. Effectiveness of favorite-place prescriptions a field experiment. Am. J. Prev. Med. 2009, 36, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, J.R.; House, R.J.; Lirtzman, S.I. Role conflict and ambiguity in complex organizations. Adm. Sci. Q. 1970, 15, 150–162. [Google Scholar] [CrossRef]
- Ryan, R.M.; Weinstein, N.; Bernstein, J.; Brown, K.W.; Mistretta, L.; Gagne, M. Vitalizing effects of being outdoors and in nature. J. Environ. Psychol. 2010, 30, 159–168. [Google Scholar] [CrossRef]
- Ericsson, A.; Nystrom, C.; Mannerkorpi, K. Psychometric properties of the stress and crisis inventory (SCI-93) in females with fibromyalgia and chronic widespread pain. Nord. J. Psychiatry 2015, 69, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Nyström, C.; Nyström, O. Skattad stress verifierar autonom dysfunktion [estimated stress verifies autonomic dysfunction]. Lakartidningen 1996, 93, 2583–2584. [Google Scholar] [PubMed]
- Mcauley, E.; Courneya, K.S. The Subjective Exercise Experiences Scale (sees)—Development and preliminary validation. J. Sport Exerc. Psychol. 1994, 16, 163–177. [Google Scholar]
- Tangney, J.P.; Baumeister, R.F.; Boone, A.L. High self-control predicts good adjustment, less pathology, better grades, and interpersonal success. J. Personal. 2004, 72, 271–324. [Google Scholar] [CrossRef]
- Han, K.T. A reliable and valid self-rating measure of the restorative quality of natural environments. Landsc. Urban Plan. 2003, 64, 209–232. [Google Scholar] [CrossRef]
- Mackay, C.; Cox, T.; Burrows, G.; Lazzerini, T. Inventory for measurement of self-reported stress and arousal. Br. J. Soc. Clin. Psychol. 1978, 17, 283–284. [Google Scholar] [CrossRef]
- Lundberg, O.; Peck, N.M. A simplified way of measuring sense of coherence experiences from a population survey in Sweden. Eur. J. Public Health 1995, 5, 56–59. [Google Scholar] [CrossRef]
- Salkovskis, P.M.; Rimes, K.A.; Warwick, H.M.C.; Clark, D.M. The health anxiety inventory: Development and validation of scales for the measurement of health anxiety and hypochondriasis. Psychol. Med. 2002, 32, 843–853. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Khalek, A.M. Measuring happiness with a single-item scale. Soc. Behav. Personal. 2006, 34, 139–149. [Google Scholar] [CrossRef]
- Sampson, R.J.; Raudenbush, S.W.; Earls, F. Neighborhoods and violent crime: A multilevel study of collective efficacy. Science 1997, 277, 918–924. [Google Scholar] [CrossRef] [PubMed]
- Cutrona, C.E.; Russell, D.W. The provisions of social relationships and adaptation to stress. In Advances in Personal Relationships; JAI Press: Greenwich, CT, USA, 1987; pp. 37–67. [Google Scholar]
- Koh, K.B.; Park, J.K.; Kim, C.H.; Cho, S. Development of the stress response inventory and its application in clinical practice. Psychosom. Med. 2001, 63, 668–678. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.-I.; Shimada, H.; Miura, M.; Katayanagi, K.; Umano, R.; Sakano, Y. Development of a new psychological Stress Response Scale (SRS-18) and investigation of the reliability and the validity. Jpn. J. Behav. Med. 1997, 4, 22–29. [Google Scholar] [CrossRef]
- Taylor, S.P. Aggressive behavior and physiological arousal as a function of provocation and tendency to inhibit aggression. J. Personal. 1967, 35, 297. [Google Scholar] [CrossRef]
- Thayer, R.E. The Biopsychology of Mood and Arousal; Oxford University Press: New York, NY, USA, 1989. [Google Scholar]
- Sherman, G.D.; Haidt, J.; Coan, J.A. Viewing cute images increases behavioral carefulness. Emotion 2009, 9, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Lese, K.P.; MacNair-Semands, R.R. The therapeutic factors inventory: Development of a scale. Group 2000, 24, 303–317. [Google Scholar] [CrossRef]
- Chern, J.S.; Kielhofner, G.; delasHeras, C.G.; Magalhaes, L.C. The volitional questionnaire: Psychometric development and practical use. Am. J. Occup. Ther. 1996, 50, 516–525. [Google Scholar] [CrossRef]
- Choi, S.M.; Kang, T.Y.; Woo, J.M. Development and validation of a modifiedform of the stress response inventory for workers. J. Korean Neuropsychiatr. Assoc. 2006, 45, 541–553. [Google Scholar]
- Ferris, D.L.; Brown, D.J.; Berry, J.W.; Lian, H.W. The development and validation of the workplace ostracism scale. J. Appl. Psychol. 2008, 93, 1348–1366. [Google Scholar] [CrossRef] [PubMed]
- Hendee, J.C.; Catton, W.R.; Marlow, L.D.; Brockman, C.F. Wilderness Users in the Pacific Northwest—Their Characteristics, Values, and Management Preferences; USDA Forest Service research paper PNW-61; Pacific Northwest Forest and Range Experiment Station: Portland, OR, USA, 1968.
- Zung, W.W.K. A self-rating depression scale. Arch. Gen. Psychiatry 1965, 12, 63–70. [Google Scholar] [CrossRef]
- Beute, F.; de Kort, Y.A.W. The natural context of wellbeing: Ecological momentary assessment of the influence of nature and daylight on affect and stress for individuals with depression levels varying from none to clinical. Health Place 2018, 49, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Bratman, G.N.; Daily, G.C.; Levy, B.J.; Gross, J.J. The benefits of nature experience: Improved affect and cognition. Landsc. Urban Plan. 2015, 138, 41–50. [Google Scholar] [CrossRef]
- Hinds, J.; Sparks, P. The affective quality of human-natural environment relationships. Evol. Psychol. 2011, 9, 147470491100900314. [Google Scholar] [CrossRef]
- Poon, K.T.; Teng, F.; Wong, W.Y.; Chen, Z.S. When nature heals: Nature exposure moderates the relationship between ostracism and aggression. J. Environ. Psychol. 2016, 48, 159–168. [Google Scholar] [CrossRef]
- Wang, Y.; She, Y.; Colarelli, S.M.; Fang, Y.; Meng, H.; Chen, Q.; Zhang, X.; Zhu, H. Exposure to nature counteracts aggression after depletion. Aggress. Behav. 2018, 44, 89–97. [Google Scholar] [CrossRef]
- DeWolfe, J.; Waliczek, T.M.; Zajicek, J.M. The relationship between levels of greenery and landscaping at track and field sites, anxiety, and sports performance of collegiate track and field athletes. HortTechnology 2011, 21, 329–335. [Google Scholar] [CrossRef]
- Mackay, G.J.; Neill, J.T. The effect of “green exercise” on state anxiety and the role of exercise duration, intensity, and greenness: A quasi-experimental study. Psychol. Sport Exerc. 2010, 11, 238–245. [Google Scholar] [CrossRef]
- Gidlow, C.J.; Randall, J.; Gillman, J.; Smith, G.R.; Jones, M.V. Natural environments and chronic stress measured by hair cortisol. Landsc. Urban Plan. 2016, 148, 61–67. [Google Scholar] [CrossRef]
- Berman, M.G.; Kross, E.; Krpan, K.M.; Askren, M.K.; Burson, A.; Deldin, P.J.; Kaplan, S.; Sherdell, L.; Gotlib, I.H.; Jonides, J. Interacting with nature improves cognition and affect for individuals with depression. J. Affect. Disord. 2012, 140, 300–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beyer, K.M.M.; Szabo, A.; Nattinger, A.B. Time spent outdoors, depressive symptoms, and variation by race and ethnicity. Am. J. Prev. Med. 2016, 51, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Christensen, K.M.; Holt, J.M.; Wilson, J.F. The relationship between outdoor recreation and depression among older adults. World Leisure J. 2013, 55, 72–82. [Google Scholar] [CrossRef]
- Farber, M.E.; Hall, T.E. Emotion and environment: Visitors’ extraordinary experiences along the dalton highway in Alaska. J. Leisure Res. 2007, 39, 248–270. [Google Scholar] [CrossRef]
- Gonzalez, M.T.; Hartig, T.; Patil, G.G.; Martinsen, E.W.; Kirkevold, M. A prospective study of group cohesiveness in therapeutic horticulture for clinical depression. Int. J. Ment. Health Nurs. 2011, 20, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Korpela, K.M.; Stenggård, E.; Jussila, P. Nature walks as a part of therapeutic intervention for depression. Ecopsychology 2016, 8, 8–15. [Google Scholar] [CrossRef]
- McCaffrey, R. The effect of healing gardens and art therapy on older adults with mild to moderate depression. Holist. Nurs. Pract. 2007, 21, 79–84. [Google Scholar] [CrossRef]
- McCaffrey, R.; Hanson, C.; McCaffrey, W. Garden walking for depression: A research report. Holist. Nurs. Pract. 2010, 24, 252–259. [Google Scholar] [CrossRef]
- McCaffrey, R.; Liehr, P.; Gregersen, T.; Nishioka, R. Garden walking and art therapy for depression in older adults: A pilot study. Res. Gerontol. Nurs. 2011, 4, 237–242. [Google Scholar] [CrossRef]
- McEachan, R.R.C.; Prady, S.L.; Smith, G.; Fairley, L.; Cabieses, B.; Gidlow, C.; Wright, J.; Dadvand, P.; van Gent, D.; Nieuwenhuijsen, M.J. The association between green space and depressive symptoms in pregnant women: Moderating roles of socioeconomic status and physical activity. J. Epidemiol. Community Health 2016, 70, 253–259. [Google Scholar] [CrossRef]
- Min, K.B.; Kim, H.J.; Kim, H.J.; Min, J.Y. Parks and green areas and the risk for depression and suicidal indicators. Int. J. Public Health 2017, 62, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, D.; Safraj, S.; Tayyab, M.; Shivashankar, R.; Patel, S.A.; Narayanan, G.; Ajay, V.S.; Ali, M.K.; Narayan, K.M.V.; Tandon, N.; et al. Park availability and major depression in individuals with chronic conditions: Is there an association in urban India? Health Place 2017, 47, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Nichani, V.; Dirks, K.; Burns, B.; Bird, A.; Grant, C. Green space and depression during pregnancy: Results from the growing up in New Zealand study. Int. J. Environ. Res. Public Health 2017, 14. [Google Scholar] [CrossRef] [PubMed]
- Rappe, E.; Kivelä, S.-L. Effects of garden visits on long-term care residents as related to depression. HortTechnology 2005, 15, 298–303. [Google Scholar] [CrossRef]
- Reklaitiene, R.; Grazuleviciene, R.; Dedele, A.; Virviciute, D.; Vensloviene, J.; Tamosiunas, A.; Baceviciene, M.; Luksiene, D.; Sapranaviciute-Zabazlajeva, L.; Radisauskas, R.; et al. The relationship of green space, depressive symptoms and perceived general health in urban population. Scand. J. Public Health 2014, 42, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Shin, W.; Shin, C.; Yeoun, P. The influence of forest therapy camp on depression in alcoholics. Environ. Health Prev. Med. 2012, 17, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Torres, E.R.; Sampselle, C.M.; Ronis, D.L.; Neighbors, H.W.; Gretebeck, K.A. Gardening/yard work and depressive symptoms in African Americans. Arch. Psychiatr. Nurs. 2016, 30, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.F.; Christensen, K.M. The relationship between outdoor recreation and depression among individuals with disabilities. J. Leisure Res. 2012, 44, 486–506. [Google Scholar] [CrossRef]
- Han, K.-T. The effect of nature and physical activity on emotions and attention while engaging in green exercise. Urban For. Urban Green. 2017, 24, 5–13. [Google Scholar] [CrossRef]
- Marselle, M.R.; Irvine, K.N.; Lorenzo-Arribas, A.; Warber, S.L. Moving beyond green: Exploring the relationship of environment type and indicators of perceived environmental quality on emotional well-being following group walks. Int. J. Environ. Res. Public Health 2015, 12, 106–130. [Google Scholar] [CrossRef]
- Ambrey, C.L.; Shahni, T.J. Greenspace and wellbeing in Tehran: A relationship conditional on a neighbourhood’s crime rate? Urban For. Urban Green. 2017, 27, 155–161. [Google Scholar] [CrossRef]
- Dadvand, P.; Bartoll, X.; Basagaña, X.; Dalmau-Bueno, A.; Martinez, D.; Ambros, A.; Cirach, M.; Triguero-Mas, M.; Gascon, M.; Borrell, C.; et al. Green spaces and general health: Roles of mental health status, social support, and physical activity. Environ. Int. 2016, 91, 161–167. [Google Scholar] [CrossRef] [PubMed]
- de Vries, S.; van Dillen, S.M.E.; Groenewegen, P.P.; Spreeuwenberg, P. Streetscape greenery and health: Stress, social cohesion and physical activity as mediators. Soc. Sci. Med. 2013, 94, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Stigsdotter, U.K.; Ekholm, O.; Schipperijn, J.; Toftager, M.; Kamper-Jørgensen, F.; Randrup, T.B. Health promoting outdoor environments—Associations between green space, and health, health-related quality of life and stress based on a Danish national representative survey. Scand. J. Public Health 2010, 38, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Takayama, N.; Korpela, K.; Lee, J.; Morikawa, T.; Tsunetsugu, Y.; Park, B.J.; Li, Q.; Tyrvainen, L.; Miyazaki, Y.; Kagawa, T. Emotional, restorative and vitalizing effects of forest and urban environments at four sites in Japan. Int. J. Environ. Res. Public Health 2014, 11, 7207–7230. [Google Scholar] [CrossRef] [PubMed]
- Weimann, H.; Rylander, L.; Albin, M.; Skärbäck, E.; Grahn, P.; Östergren, P.-O.; Björk, J. Effects of changing exposure to neighbourhood greenness on general and mental health: A longitudinal study. Health Place 2015, 33, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Willis, K.; Crabtree, B.; Osman, L.M.; Cathrine, K. Green space and health benefits: A QALY and CEA of a mental health programme. J. Environ. Econ. Policy 2016, 5, 163–180. [Google Scholar] [CrossRef]
- Cini, F.; Kruger, S.; Ellis, S. A model of intrinsic and extrinsic motivations on subjective well-being: The experience of overnight visitors to a national park. Appl. Res. Qual. Life 2013, 8, 45–61. [Google Scholar] [CrossRef]
- Frash, R.E., Jr.; Blose, J.E.; Norman, W.C.; Patience, M. Healthy parks, happy people: An exploratory study of a county park system. J. Park Recreat. Adm. 2016, 34, 84–102. [Google Scholar]
- Saw, L.E.; Lim, F.K.S.; Carrasco, L.R. The relationship between natural park usage and happiness does not hold in a tropical city-state. PLoS ONE 2015, 10, e0133781. [Google Scholar] [CrossRef]
- Dzhambov, A.M.; Dimitrova, D.D. Elderly visitors of an urban park, health anxiety and individual awareness of nature experiences. Urban For. Urban Green. 2014, 13, 806–813. [Google Scholar] [CrossRef]
- Shin, W.S. The influence of forest view through a window on job satisfaction and job stress. Scand. J. For. Res. 2007, 22, 248–253. [Google Scholar] [CrossRef]
- Ambrey, C.; Fleming, C. Public greenspace and life satisfaction in urban Australia. Urban Stud. 2014, 51, 1290–1321. [Google Scholar] [CrossRef]
- Biedenweg, K.; Scott, R.P.; Scott, T.A. How does engaging with nature relate to life satisfaction? Demonstrating the link between environment-specific social experiences and life satisfaction. J. Environ. Psychol. 2017, 50, 112–124. [Google Scholar] [CrossRef]
- Fleming, C.M.; Manning, M.; Ambrey, C.L. Crime, greenspace and life satisfaction: An evaluation of the New Zealand experience. Landsc. Urban Plan. 2016, 149, 1–10. [Google Scholar] [CrossRef]
- Waliczek, T.M.; Zajicek, J.M.; Lineberger, R.D. The influence of gardening activities on consumer perceptions of life satisfaction. Hortscience 2005, 40, 1360–1365. [Google Scholar] [CrossRef]
- Alcock, I.; White, M.P.; Wheeler, B.W.; Fleming, L.E.; Depledge, M.H. Longitudinal effects on mental health of moving to greener and less green urban areas. Environ. Sci. Technol. 2014, 48, 1247–1255. [Google Scholar] [CrossRef]
- Ambrey, C.L. Urban greenspace, physical activity and wellbeing: The moderating role of perceptions of neighbourhood affability and incivility. Land Use Policy 2016, 57, 638–644. [Google Scholar] [CrossRef]
- An, M.; Colarelli, S.M.; O’Brien, K.; Boyajian, M.E. Why we need more nature at work: Effects of natural elements and sunlight on employee mental health and work attitudes. PLoS ONE 2016, 11. [Google Scholar] [CrossRef]
- Annerstedt, M.; Ostergren, P.-O.; Björk, J.; Grahn, P.; Skärbäck, E.; Währborg, P. Green qualities in the neighbourhood and mental health—Results from a longitudinal cohort study in Southern Sweden. BMC Public Health 2012, 12, 337. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Mitchell, R.; Hartig, T. The association between green space and mental health varies across the lifecourse. A longitudinal study. J. Epidemiol. Community Health 2014, 68, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Beyer, K.M.M.; Kaltenbach, A.; Szabo, A.; Bogar, S.; Nieto, F.J.; Malecki, K.M. Exposure to neighborhood green space and mental health: Evidence from the survey of the health of wisconsin. Int. J. Environ. Res. Public Health 2014, 11, 3453–3472. [Google Scholar] [CrossRef] [PubMed]
- Bos, E.H.; van der Meulen, L.; Wichers, M.; Jeronimus, B.F. A primrose path? Moderating effects of age and gender in the association between green space and mental health. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Cline, H.; Turkheimer, E.; Duncan, G.E. Access to green space, physical activity and mental health: A twin study. J. Epidemiol. Community Health 2015, 69, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.T.C.; Shanahan, D.F.; Hudson, H.L.; Plummer, K.E.; Siriwardena, G.M.; Fuller, R.A.; Anderson, K.; Hancock, S.; Gaston, K.J. Doses of neighborhood nature: The benefits for mental health of living with nature. BioScience 2017, 67, 147–155. [Google Scholar] [CrossRef]
- Crust, L.; Henderson, H.; Middleton, G. The acute effects of urban green and countryside walking on psychological health: A field-based study of green exercise. Int. J. Sport Psychol. 2013, 44, 160–177. [Google Scholar] [CrossRef]
- Dzhambov, A.; Hartig, T.; Markevych, I.; Tilov, B.; Dimitrova, D. Urban residential greenspace and mental health in youth: Different approaches to testing multiple pathways yield different conclusions. Environ. Res. 2018, 160, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Gubbels, J.S.; Kremers, S.P.J.; Droomers, M.; Hoefnagels, C.; Stronks, K.; Hosman, C.; de Vries, S. The impact of greenery on physical activity and mental health of adolescent and adult residents of deprived neighborhoods: A longitudinal study. Health Place 2016, 40, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Iwata, Y.; Dhubháin, Á.N.; Brophy, J.; Roddy, D.; Burke, C.; Murphy, B. Benefits of group walking in forests for people with significant mental ill-health. Ecopsychology 2016, 8, 16–26. [Google Scholar] [CrossRef]
- Liu, H.; Li, F.; Li, J.; Zhang, Y. The relationships between urban parks, residents’ physical activity, and mental health benefits: A case study from beijing, China. J. Environ. Manag. 2017, 190, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R. Is physical activity in natural environments better for mental health than physical activity in other environments? Soc. Sci. Med. 2013, 91, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Mutz, M.; Mueller, J. Mental health benefits of outdoor adventures: Results from two pilot studies. J. Adolesc. 2016, 49, 105–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nutsford, D.; Pearson, A.L.; Kingham, S. An ecological study investigating the association between access to urban green space and mental health. Public Health 2013, 127, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Pálsdóttir, A.M.; Persson, D.; Persson, B.; Grahn, P. The journey of recovery and empowerment embraced by nature—Clients’ perspectives on nature-based rehabilitation in relation to the role of the natural environment. Int. J. Environ. Res. Public Health 2014, 11, 7094–7115. [Google Scholar] [CrossRef] [PubMed]
- Rogerson, M.; Brown, D.K.; Sandercock, G.; Wooller, J.J.; Barton, J. A comparison of four typical green exercise environments and prediction of psychological health outcomes. Perspect. Public Health 2016, 136, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Ruijsbroek, A.; Mohnen, S.M.; Droomers, M.; Kruize, H.; Gidlow, C.; Grazuleviciene, R.; Andrusaityte, S.; Maas, J.; Nieuwenhuijsen, M.J.; Triguero-Mas, M.; et al. Neighbourhood green space, social environment and mental health: An examination in four european cities. Int. J. Public Health 2017, 62, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Sturm, R.; Cohen, D. Proximity to urban parks and mental health. J. Ment. Health Policy Econ. 2014, 17, 19–24. [Google Scholar]
- Sugiyama, T.; Leslie, E.; Giles-Corti, B.; Owen, N. Associations of neighbourhood greenness with physical and mental health: Do walking, social coherence and local social interaction explain the relationships? J. Epidemiol. Community Health 2008, 62, e9. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Villanueva, K.; Knuiman, M.; Francis, J.; Foster, S.; Wood, L.; Giles-Corti, B. Can neighborhood green space mitigate health inequalities? A study of socio-economic status and mental health. Health Place 2016, 38, 16–21. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, M.; van Poppel, M.; Smith, G.; Triguero-Mas, M.; Andrusaityte, S.; van Kamp, I.; van Mechelen, W.; Gidlow, C.; Gražulevičiene, R.; Nieuwenhuijsen, M.J.; et al. Does time spent on visits to green space mediate the associations between the level of residential greenness and mental health? Urban For. Urban Green. 2017, 25, 94–102. [Google Scholar] [CrossRef]
- van den Berg, M.; van Poppel, M.; van Kamp, I.; Andrusaityte, S.; Balseviciene, B.; Cirach, M.; Danileviciute, A.; Ellis, N.; Hurst, G.; Masterson, D.; et al. Visiting green space is associated with mental health and vitality: A cross-sectional study in four european cities. Health Place 2016, 38, 8–15. [Google Scholar] [CrossRef] [PubMed]
- van den Bosch, M.A.; Östergren, P.-O.; Grahn, P.; Skärbäck, E.; Währborg, P. Moving to serene nature may prevent poor mental health-results from a Swedish longitudinal cohort study. Int. J. Environ. Res. Public Health 2015, 12, 7974–7989. [Google Scholar] [CrossRef] [PubMed]
- Vujcic, M.; Tomicevic-Dubljevic, J.; Grbic, M.; Lecic-Tosevski, D.; Vukovic, O.; Toskovic, O. Nature based solution for improving mental health and well-being in urban areas. Environ. Res. 2017, 158, 385–392. [Google Scholar] [CrossRef] [PubMed]
- White, M.P.; Alcock, I.; Wheeler, B.W.; Depledge, M.H. Would you be happier living in a greener urban area? A fixed-effects analysis of panel data. Psychol. Sci. 2013, 24, 920–928. [Google Scholar] [CrossRef]
- Wilson, N.W.; Jones, R.; Fleming, S.; Lafferty, K.; Knifton, L.; Cathrine, K.; McNish, H. Branching out: The impact of a mental health ecotherapy program. Ecopsychology 2011, 3, 1–7. [Google Scholar] [CrossRef]
- Wilson, N.W.; Fleming, S.; Jones, R.; Lafferty, K.; Cathrine, K.; Seaman, P.; Knifton, L. Green shoots of recovery: The impact of a mental health ecotherapy programme. Ment. Health Rev. J. 2010, 15, 4–14. [Google Scholar] [CrossRef]
- Wood, L.; Hooper, P.; Foster, S.; Bull, F. Public green spaces and positive mental health—Investigating the relationship between access, quantity and types of parks and mental wellbeing. Health Place 2017, 48, 63–71. [Google Scholar] [CrossRef]
- Ambrey, C.L.; Cartlidge, N. Do the psychological benefits of greenspace depend on one’s personality? Personal. Individ. Differ. 2017, 116, 233–239. [Google Scholar] [CrossRef]
- Budruk, M.; Lee, W. Importance of managing for personal benefits, hedonic and utilitarian motivations, and place attachment at an urban natural setting. Environ. Manag. 2016, 58, 504–517. [Google Scholar] [CrossRef]
- Gilchrist, K.; Brown, C.; Montarzino, A. Workplace settings and wellbeing: Greenspace use and views contribute to employee wellbeing at pen-urban business sites. Landsc. Urban Plan. 2015, 138, 32–40. [Google Scholar] [CrossRef]
- Henderson-Wilson, C.; Sia, K.L.; Veitch, J.; Staiger, P.K.; Davidson, P.; Nicholls, P. Perceived health benefits and willingness to pay for parks by park users: Quantitative and qualitative research. Int. J. Environ. Res. Public Health 2017, 14. [Google Scholar] [CrossRef]
- Houlden, V.; Weich, S.; Jarvis, S. A cross-sectional analysis of green space prevalence and mental wellbeing in England. BMC Public Health 2017, 17. [Google Scholar] [CrossRef]
- Jakubec, S.L.; Den Hoed, D.C.; Ray, H.; Krishnamurthy, A. Mental well-being and quality-of-life benefits of inclusion in nature for adults with disabilities and their caregivers. Landsc. Res. 2016, 41, 616–627. [Google Scholar] [CrossRef]
- Barton, J.; Griffin, M.; Pretty, J. Exercise-, nature- and socially interactive-based initiatives improve mood and self-esteem in the clinical population. Perspect. Public Health 2012, 132, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Joye, Y.; Bolderdijk, J.W. An exploratory study into the effects of extraordinary nature on emotions, mood, and prosociality. Front. Psychol. 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- McCaffrey, R.; Liehr, P. The effect of reflective garden walking on adults with increased levels of psychological stress. J. Holist. Nurs. 2016, 34, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Mental health benefits of neighbourhood green space are stronger among physically active adults in middle-to-older age: Evidence from 260,061 australians. Prev. Med. 2013, 57, 601–606. [Google Scholar] [CrossRef]
- Hansmann, R.; Hug, S.-M.; Seeland, K. Restoration and stress relief through physical activities in forests and parks. Urban For. Urban Green. 2007, 6, 213–225. [Google Scholar] [CrossRef]
- Hartig, T.; Kaiser, F.G.; Strumse, E. Psychological restoration in nature as a source of motivation for ecological behaviour. Environ. Conserv. 2007, 34, 291–299. [Google Scholar] [CrossRef]
- Calogiuri, G.; Evensen, K.; Weydahl, A.; Andersson, K.; Patil, G.; Ihlebæk, C.; Raanaas, R.K. Green exercise as a workplace intervention to reduce job stress. Results from a pilot study. Work 2016, 53, 99–111. [Google Scholar] [CrossRef]
- Barnicle, T.; Midden, K.S. The effects of a horticulture activity program on the psychological well-being of older people in a long-term care facility. HortTechnology 2003, 13, 81–85. [Google Scholar] [CrossRef]
- Fruhauf, A.; Niedermeier, M.; Elliott, L.R.; Ledochowski, L.; Marksteiner, J.; Kopp, M. Acute effects of outdoor physical activity on affect and psychological well-being in depressed patients—A preliminary study. Ment. Health Phys. Act. 2016, 10, 4–9. [Google Scholar] [CrossRef]
- Herzog, T.R.; Strevey, S.J. Contact with nature, sense of humor, and psychological well-being. Environ. Behav. 2008, 40, 747–776. [Google Scholar] [CrossRef]
- Hug, S.-M.; Hansmann, R.; Monn, C.; Krütli, P.; Seeland, K. Restorative effects of physical activity in forests and indoor settings. Int. J. Fit. 2008, 4, 25–37. [Google Scholar]
- Kamitsis, I.; Francis, A.J.P. Spirituality mediates the relationship between engagement with nature and psychological wellbeing. J. Environ. Psychol. 2013, 36, 136–143. [Google Scholar] [CrossRef]
- Lawton, E.; Brymer, E.; Clough, P.; Denovan, A. The relationship between the physical activity environment, nature relatedness, anxiety, and the psychological well-being benefits of regular exercisers. Front. Psychol. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Martens, D.; Gutscher, H.; Bauer, N. Walking in “wild” and “tended” urban forests: The impact on psychological well-being. J. Environ. Psychol. 2011, 31, 36–44. [Google Scholar] [CrossRef]
- Wolsko, C.; Lindberg, K. Experiencing connection with nature: The matrix of psychological well-being, mindfulness, and outdoor recreation. Ecopsychology 2013, 5, 80–91. [Google Scholar] [CrossRef]
- Bricker, K.S.; Hendricks, W.W.; Aschenbrenner, C.A. Californians’ perceptions of the influence of parks and recreation on quality of life. J. Park Recreat. Adm. 2016, 34, 64–82. [Google Scholar] [CrossRef]
- Camargo, D.M.; Ramirez, P.C.; Fermino, R.C. Individual and environmental correlates to quality of life in park users in Colombia. Int. J. Environ. Res. Public Health 2017, 14. [Google Scholar] [CrossRef]
- Lai, C.K.Y.; Lau, C.K.Y.; Kan, W.Y.; Lam, W.M.; Fung, C.Y.Y. The effect of horticultural therapy on the quality of life of palliative care patients. J. Psychosoc. Oncol. 2017, 35, 278–291. [Google Scholar] [CrossRef] [PubMed]
- McFarland, A.L.; Waliczek, T.M.; Zajicek, J.M. The relationship between student use of campus green spaces and perceptions of quality of life. HortTechnology 2008, 18, 232–238. [Google Scholar] [CrossRef]
- Shafer, C.S.; Lee, B.K.; Turner, S. A tale of three greenway trails: User perceptions related to quality of life. Landsc. Urban Plan. 2000, 49, 163–178. [Google Scholar] [CrossRef]
- Sommerfeld, A.J.; Waliczek, T.M.; Zajicek, J.M. Growing minds: Evaluating the effect of gardening on quality of life and physical activity level of older adults. HortTechnology 2010, 20, 705–710. [Google Scholar] [CrossRef]
- Tiyarattanachai, R.; Hollmann, N.M. Green campus initiative and its impacts on quality of life of stakeholders in green and non-green campus universities. SpringerPlus 2016, 5, 84. [Google Scholar] [CrossRef] [PubMed]
- de Bloom, J.; Sianoja, M.; Korpela, K.; Tuomisto, M.; Lilja, A.; Geurts, S.; Kinnunen, U. Effects of park walks and relaxation exercises during lunch breaks on recovery from job stress: Two randomized controlled trials. J. Environ. Psychol. 2017, 51, 14–30. [Google Scholar] [CrossRef] [Green Version]
- Bodin, M.; Hartig, T. Does the outdoor environment matter for psychological restoration gained through running? Psychol. Sport Exerc. 2003, 4, 141–153. [Google Scholar] [CrossRef]
- Chen, Z.; He, Y.; Yu, Y. Enhanced functional connectivity properties of human brains during in-situ nature experience. PeerJ 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Hartig, T.; Mang, M.; Evans, G.W. Restorative effects of natural environment experiences. Environ. Behav. 1991, 23, 3–26. [Google Scholar] [CrossRef]
- Korpela, K.M.; Hartig, T.; Kaiser, F.G.; Fuhrer, U. Restorative experience and self-regulation in favorite places. Environ. Behav. 2001, 33, 572–589. [Google Scholar] [CrossRef]
- Weng, P.-Y.; Chiang, Y.-C. Psychological restoration through indoor and outdoor leisure activities. J. Leisure Res. 2014, 46, 203–217. [Google Scholar] [CrossRef]
- Sonntag-Ostrom, E.; Nordin, M.; Lundell, Y.; Dolling, A.; Wiklund, U.; Karlsson, M.; Carlberg, B.; Jarvholm, L.S. Restorative effects of visits to urban and forest environments in patients with exhaustion disorder. Urban For. Urban Green. 2014, 13, 344–354. [Google Scholar] [CrossRef]
- von Lindern, E.; Bauer, N.; Frick, J.; Hunziker, M.; Hartig, T. Occupational engagement as a constraint on restoration during leisure time in forest settings. Landsc. Urban Plan. 2013, 118, 90–97. [Google Scholar] [CrossRef]
- Cervinka, R.; Schwab, M.; Schönbauer, R.; Hämmerle, I.; Pirgie, L.; Sudkamp, J. My garden—My mate? Perceived restorativeness of private gardens and its predictors. Urban For. Urban Green. 2016, 16, 182–187. [Google Scholar] [CrossRef]
- Hartig, T.; Kaiser, F.G.; Bowler, P.A. Psychological restoration in nature as a positive motivation for ecological behavior. Environ. Behav. 2001, 33, 590–607. [Google Scholar] [CrossRef]
- Hipp, J.A.; Gulwadi, G.B.; Alves, S.; Sequeira, S. The relationship between perceived greenness and perceived restorativeness of university campuses and student-reported quality of life. Environ. Behav. 2016, 48, 1292–1308. [Google Scholar] [CrossRef]
- Twedt, E.; Rainey, R.M.; Proffitt, D.R. Designed natural spaces: Informal gardens are perceived to be more restorative than formal gardens. Front. Psychol. 2016, 7. [Google Scholar] [CrossRef]
- Abkar, M.; Kamal, M.S.M.; Maulan, S.; Mariapan, M.; Davoodi, S.R. Relationship between the preference and perceived restorative potential of urban landscapes. HortTechnology 2011, 21, 514–519. [Google Scholar] [CrossRef]
- Nordh, H.; Alalouch, C.; Hartig, T. Assessing restorative components of small urban parks using conjoint methodology. Urban For. Urban Green. 2011, 10, 95–103. [Google Scholar] [CrossRef]
- Tenngart Ivarsson, C.; Hagerhall, C.M. The perceived restorativeness of gardens—Assessing the restorativeness of a mixed built and natural scene type. Urban For. Urban Green. 2008, 7, 107–118. [Google Scholar] [CrossRef]
- Bratman, G.N.; Hamilton, J.P.; Hahn, K.S.; Daily, G.C.; Gross, J.J. Nature experience reduces rumination and subgenual prefrontal cortex activation. Proc. Natl. Acad. Sci. USA 2015, 112, 8567–8572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, A.J.; Knight, L.F.M.; Wallach, J. Gardening activities, education, and self-esteem—Learning outside the classroom. Urban Educ. 2007, 42, 403–411. [Google Scholar] [CrossRef]
- Wood, C.J.; Pretty, J.; Griffin, M. A case-control study of the health and well-being benefits of allotment gardening. J. Public Health 2016, 38, E336–E344. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Das, K.V.; Chen, Q. Neighborhood green, social support, physical activity, and stress: Assessing the cumulative impact. Health Place 2011, 17, 1202–1211. [Google Scholar] [CrossRef] [PubMed]
- Grahn, P.; Stigsdotter, U.A. Landscape planning and stress. Urban For. Urban Green. 2003, 2, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Largo-Wight, E.; Wlyudka, P.S.; Merten, J.W.; Cuvelier, E.A. Effectiveness and feasibility of a 10-minute employee stress intervention: Outdoor booster break. J. Workplace Behav. Health 2017, 32, 159–171. [Google Scholar] [CrossRef]
- Lottrup, L.; Grahn, P.; Stigsdotter, U.K. Workplace greenery and perceived level of stress: Benefits of access to a green outdoor environment at the workplace. Landsc. Urban Plan. 2013, 110, 5–11. [Google Scholar] [CrossRef]
- Morita, E.; Fukuda, S.; Nagano, J.; Hamajima, N.; Yamamoto, H.; Iwai, Y.; Nakashima, T.; Ohira, H.; Shirakawa, T. Psychological effects of forest environments on healthy adults: Shinrin-yoku (forest-air bathing, walking) as a possible method of stress reduction. Public Health 2007, 121, 54–63. [Google Scholar] [CrossRef] [Green Version]
- Orsega-Smith, E.; Mowen, A.J.; Payne, L.L.; Godbey, G. The interaction of stress and park use on psycho-physiological health in older adults. J. Leisure Res. 2004, 36, 232–256. [Google Scholar] [CrossRef]
- Roe, J.J.; Aspinall, P.A.; Thompson, C.W. Coping with stress in deprived urban neighborhoods: What is the role of green space according to life stage? Front. Psychol. 2017, 8. [Google Scholar] [CrossRef]
- Roe, J.J.; Thompson, C.W.; Aspinall, P.A.; Brewer, M.J.; Duff, E.I.; Miller, D.; Mitchell, R.; Clow, A. Green space and stress: Evidence from cortisol measures in deprived urban communities. Int. J. Environ. Res. Public Health 2013, 10, 4086–4103. [Google Scholar] [CrossRef] [PubMed]
- Sidenius, U.; Stigsdotter, U.K.; Poulsen, D.V.; Bondas, T. “I look at my own forest and fields in a different way”: The lived experience of nature-based therapy in a therapy garden when suffering from stress-related illness. Int. J. Qual. Stud. Health Well-Being 2017, 12. [Google Scholar] [CrossRef] [PubMed]
- Stigsdotter, U.K.; Grahn, P. Stressed individuals’ preferences for activities and environmental characteristics in green spaces. Urban For. Urban Green. 2011, 10, 295–304. [Google Scholar] [CrossRef]
- Thompson, C.W.; Roe, J.; Aspinall, P.; Mitchell, R.; Clow, A.; Miller, D. More green space is linked to less stress in deprived communities: Evidence from salivary cortisol patterns. Landsc. Urban Plan. 2012, 105, 221–229. [Google Scholar] [CrossRef] [Green Version]
- Thompson, C.W.; Aspinall, P.; Roe, J.; Robertson, L.; Miller, D. Mitigating stress and supporting health in deprived urban communities: The importance of green space and the social environment. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Tyrvainen, L.; Ojala, A.; Korpela, K.; Lanki, T.; Tsunetsugu, Y.; Kagawa, T. The influence of urban green environments on stress relief measures: A field experiment. J. Environ. Psychol. 2014, 38, 1–9. [Google Scholar] [CrossRef]
- Van Den Berg, A.E.; Custers, M.H.G. Gardening promotes neuroendocrine and affective restoration from stress. J. Health Psychol. 2010, 16, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Olafsdottir, G.; Cloke, P.; Vogele, C. Place, green exercise and stress: An exploration of lived experience and restorative effects. Health Place 2017, 46, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Bjornstad, S.; Patil, G.G.; Raanaas, R.K. Nature contact and organizational support during office working hours: Benefits relating to stress reduction, subjective health complaints, and sick leave. Work—J. Prev. Assess. Rehabilit. 2016, 53, 9–20. [Google Scholar] [CrossRef]
- Hull, R.B.; Michael, S.E. Nature-based recreation, mood change, and stress restoration. Leisure Sci. 1995, 17, 1–14. [Google Scholar] [CrossRef]
- Ambrey, C.L. An investigation into the synergistic wellbeing benefits of greenspace and physical activity: Moving beyond the mean. Urban For. Urban Green. 2016, 19, 7–12. [Google Scholar] [CrossRef]
- Bertram, C.; Rehdanz, K. The role of urban green space for human well-being. Ecol. Econ. 2015, 120, 139–152. [Google Scholar] [CrossRef] [Green Version]
- Carrus, G.; Scopelliti, M.; Lafortezza, R.; Colangelo, G.; Ferrini, F.; Salbitano, F.; Agrimi, M.; Portoghesi, L.; Sernenzato, P.; Sanesi, G. Go greener, feel better? The positive effects of biodiversity on the well-being of individuals visiting, urban and peri-urban green areas. Landsc. Urban Plan. 2015, 134, 221–228. [Google Scholar] [CrossRef]
- Cervinka, R.; Röderer, K.; Hefler, E. Are nature lovers happy? On various indicators of well-being and connectedness with nature. J. Health Psychol. 2011, 17, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Korpela, K.; De Bloom, J.; Sianoja, M.; Pasanen, T.; Kinnunen, U. Nature at home and at work: Naturally good? Links between window views, indoor plants, outdoor activities and employee well-being over one year. Landsc. Urban Plan. 2017, 160, 38–47. [Google Scholar] [CrossRef]
- Korpela, K.; Nummi, T.; Lipiainen, L.; De Bloom, J.; Sianoja, M.; Pasanen, T.; Kinnunen, U. Nature exposure predicts well-being trajectory groups among employees across two years. J. Environ. Psychol. 2017, 52, 81–91. [Google Scholar] [CrossRef]
- Kothencz, G.; Kolcsar, R.; Cabrera-Barona, P.; Szilassi, P. Urban green space perception and its contribution to well-being. Int. J. Environ. Res. Public Health 2017, 14. [Google Scholar] [CrossRef] [PubMed]
- Krekel, C.; Kolbe, J.; Wuestemann, H. The greener, the happier? The effect of urban land use on residential well-being. Ecol. Econ. 2016, 121, 117–127. [Google Scholar] [CrossRef] [Green Version]
- Leck, C.; Upton, D.; Evans, N. Growing well-beings: The positive experience of care farms. Br. J. Health Psychol. 2015, 20, 745–762. [Google Scholar] [CrossRef]
- Loureiro, A.; Veloso, S. Outdoor exercise, well-being and connectedness to nature. PSICO 2014, 45, 299–304. [Google Scholar] [CrossRef]
- Luck, G.W.; Davidson, P.; Boxall, D.; Smallbone, L. Relations between urban bird and plant communities and human well-being and connection to nature. Conserv. Biol. 2011, 25, 816–826. [Google Scholar] [CrossRef] [PubMed]
- Marselle, M.R.; Irvine, K.N.; Warber, S.L. Examining group walks in nature and multiple aspects of well-being: A large-scale study. Ecopsychology 2014, 6, 134–147. [Google Scholar] [CrossRef]
- Nisbet, E.K.; Zelenski, J.M.; Murphy, S.A. Happiness is in our nature: Exploring nature relatedness as a contributor to subjective well-being. J. Happiness Stud. 2011, 12, 303–322. [Google Scholar] [CrossRef]
- Holli-Anne, P.; Andrew, J.H. Nature involvement increases hedonic and eudaimonic well-being: A two-week experimental study. Ecopsychology 2014, 6, 148–154. [Google Scholar] [CrossRef]
- Richardson, M.; Cormack, A.; McRobert, L.; Underhill, R. 30 days wild: Development and evaluation of a large-scale nature engagement campaign to improve well-being. PLoS ONE 2016, 11. [Google Scholar] [CrossRef]
- Scopelliti, M.; Carrus, G.; Adinolfi, C.; Suarez, G.; Colangelo, G.; Lafortezza, R.; Panno, A.; Sanesi, G. Staying in touch with nature and well-being in different income groups: The experience of urban parks in bogota. Landsc. Urban Plan. 2016, 148, 139–148. [Google Scholar] [CrossRef]
- Wang, X.; Rodiek, S.; Wu, C.; Chen, Y.; Li, Y. Stress recovery and restorative effects of viewing different urban park scenes in Shanghai, China. Urban For. Urban Green. 2016, 15, 112–122. [Google Scholar] [CrossRef]
- Webber, J.; Hinds, J.; Camic, P.M. The well-being of allotment gardeners: A mixed methodological study. Ecopsychology 2015, 7, 20–28. [Google Scholar] [CrossRef]
- McClimens, A.; Doel, M.; Ibbotson, R.; Partridge, N.; Muscroft, E.; Lockwood, L. How do the ‘peace gardens’ make you feel? Public space and personal wellbeing in city centre Sheffield. J. Urban Des. 2012, 17, 117–133. [Google Scholar] [CrossRef]
- Nisbet, E.K.; Zelenski, J.M. Underestimating nearby nature: Affective forecasting errors obscure the happy path to sustainability. Psychol. Sci. 2011, 22, 1101–1106. [Google Scholar] [CrossRef]
- Akobeng, A.K. Understanding randomised controlled trials. Arch. Dis. Child. 2005, 90, 840–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoney, C.M.; Johnson, L.L. Design of clinical studies and trials. In Principles and Practice of Clinical Research, 3rd ed.; Gallin, J.I., Ognibene, F.P., Eds.; Academic Press: London, UK, 2012; pp. 225–242. [Google Scholar]
- South, E.C.; Kondo, M.C.; Cheney, R.A.; Branas, C.C. Neighborhood blight, stress, and health: A walking trial of urban greening and ambulatory heart rate. Am. J. Public Health 2015, 105, 909–913. [Google Scholar] [CrossRef] [PubMed]
- Tilley, S.; Neale, C.; Patuano, A.; Cinderby, S. Older people’s experiences of mobility and mood in an urban environment: A mixed methods approach using electroencephalography (EEG) and interviews. Int. J. Environ. Res. Public Health 2017, 14. [Google Scholar] [CrossRef] [PubMed]
- Fleuret, S.; Atkinson, S. Wellbeing, health and geography: A critical review and research agenda. N. Z. Geogr. 2007, 63, 106–118. [Google Scholar] [CrossRef]
- Gesler, W.M.; Kearns, R.A. Culture/Place/Health; Routledge: New York, NY, USA, 2002. [Google Scholar]
- Heslop, P.; Blair, P.; Flemming, P.; Hoghton, M.; Marriot, A.; Russ, L. Confidential Inquiry into Premature Deaths for People with Learning Disabilities (CIPOLD); Final Report; Norah Fry Research Centre, University of Bristol: Bristol, UK, 2013. [Google Scholar]
- Honold, J.; Lakes, T.; Beyer, R.; van der Meer, E. Restoration in urban spaces: Nature views from home, greenways, and public parks. Environ. Behav. 2016, 48, 796–825. [Google Scholar] [CrossRef]
- Ng, K.S.T.; Sia, A.; Ng, M.K.W.; Tan, C.T.Y.; Chan, H.Y.; Tan, C.H.; Rawtaer, I.; Feng, L.; Mahendran, R.; Larbi, A.; et al. Effects of horticultural therapy on asian older adults: A randomized controlled trial. Int. J. Environ. Res. Public Health 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Ho, R.C.-M.; Mak, A. Interleukin (il)-6, tumour necrosis factor alpha (tnf-α) and soluble interleukin-2 receptors (sil-2r) are elevated in patients with major depressive disorder: A meta-analysis and meta-regression. J. Affect. Disord. 2012, 139, 230–239. [Google Scholar] [CrossRef] [PubMed]


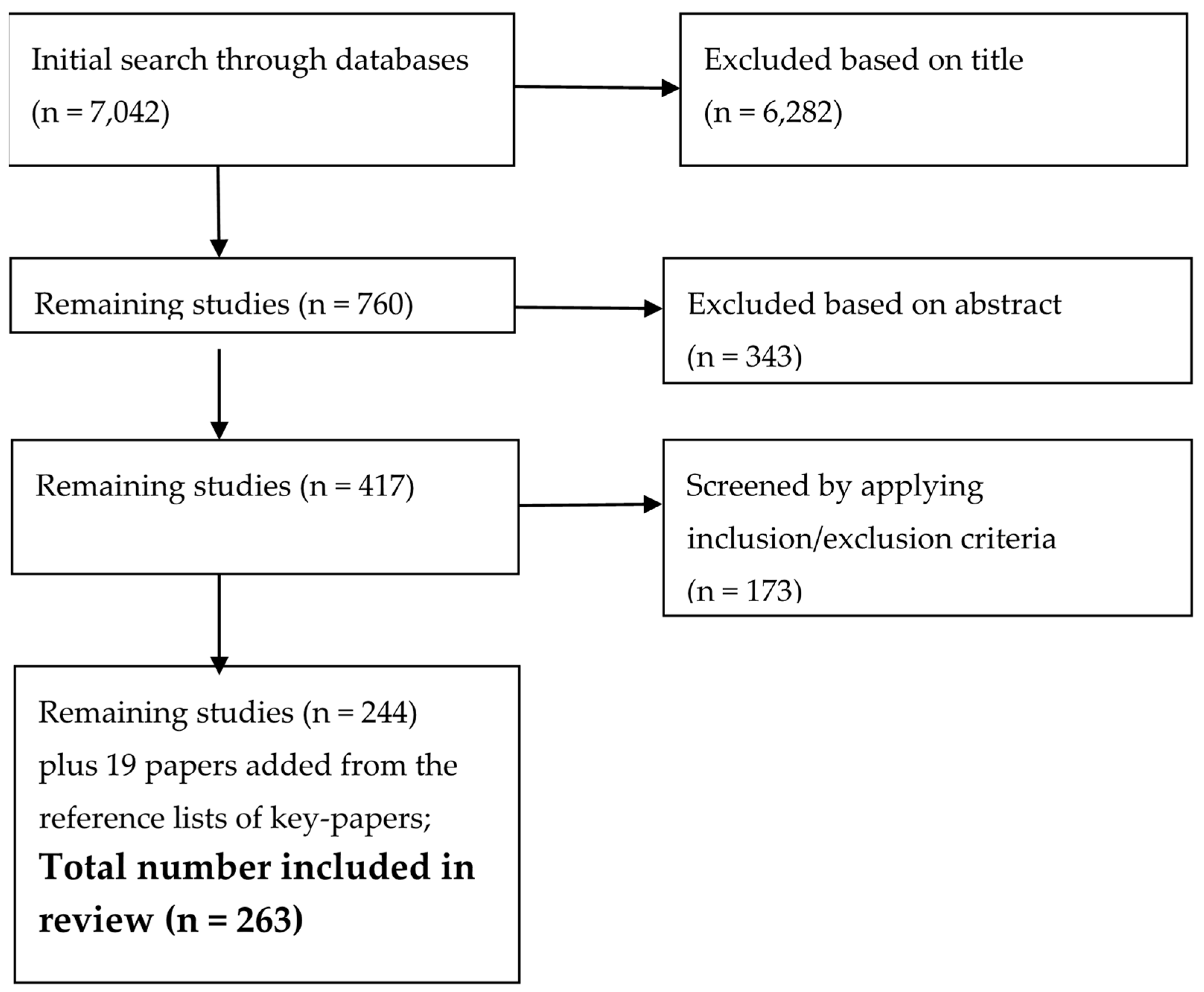{kind=link}
| Concept 1 | |
| Alternative Terms/Synonyms (combined with OR) | “green space*”, green*, “green environ*”, “green infrastruct*”, outdoor*, “outdoor experience*”, “nature experience*”, “natural space*”, “natural infrastruct*” “green health*” |
| Broader terms (combined with OR) | “wilderness experience*”, “adventure therapy”, “outdoor therapy”, “nature therapy”, “nature connect*”, “near nature*”, ecotherap*, eco-therap*, “eco therap”, “green therap*”, “green-therap*”, “green exercis*”, “green-exercis*” |
| Narrower terms (combined with OR) | ecopsychology, eco-psychology, “eco psychology”, “environmental psychology”, park, parks, forest*, horticultur*, “horticulture therap*”, garden*, allotment*, landscap*, highland*, wasteland* |
| Concept 2 | |
| Alternative Terms/Synonyms (combined with OR) | “mental wellbeing”, “mental well-being”, “mental well being”, “mental health”, “emotional wellbeing”, “emotional well-being”, “emotional well being”, “emotional health”, “psychological wellbeing”, “psychological well-being”, “psychological well being”, “psychological health” |
| Broader terms (combined with OR) | “self-concept”, “self concept”, “self-esteem”, “self esteem”, “self-image”, “self image”, “sense of coherence”, “sense of personal control”, “social wellbeing”, “social well-being”, “social well being”, “psychological issue*”, ruminat*, restorative |
| Narrower terms (combined with OR) | “well-being”, wellbeing, “well being” “quality of life”, “life satisfaction”, emotion, depress*, anxi*, stress*, fear*, frustrate*, agress*, lonely, loneliness, isolation, happy, happiness, resilien*, optimis*, hope*, empower* |
| Type of Green Space | |
|---|---|
| Group 1 | Horticulture, garden, allotment (n = 43) |
| Group 2 | Urban and mixed green space (n = 140) |
| Group 3 | Wild, natural or rural green space (n = 34) |
| Group 4 | Virtual or indoor green space (n = 24) |
| Type of Study | # of Studies |
|---|---|
| Cross-sectional | 227 |
| Longitudinal | 13 |
| Review | 22 |
| Historic, secondary narrative analysis | 1 |
| Total | 263 |
| RCT with crossover | 9 |
| RCT, no crossover | 21 |
| Non-randomized CT, cross over | 2 |
| Non-randomized CT, no crossover | 6 |
| Continent | # of Studies |
|---|---|
| North America | 64 |
| South America | 3 |
| Asia | 29 |
| South Africa | 1 |
| New Zealand | 3 |
| Australia | 18 |
| Europe | 123 |
| -east | 5 |
| -west | 56 |
| -north | 38 |
| -south | 6 |
| -central | 14 |
| -across regions | 4 |
| Total | 241 |
| Participant Type | # of Studies |
|---|---|
| General public, parents, twins | 79 |
| University students, undergraduates, college students, students, graduate students, university students, healthy and physically inactive, male university students, pupils | 37 |
| Psychiatric patients, individuals with clinical depression, mental health patients, stress-related mental health patients, adults with depression, adults with increased psychological stress, adults with mental health issues, individuals with burnout, exhaustion disorder, individual with stress, patients with depression, individuals with burnout, diagnosed with depression/anxiety/stress, females diagnosed with exhaustion disorder, mental disorder clients, individuals with stress injuries, people with mental health problems, people with significant mental ill-health, people diagnosed with chronic mental illness | 32 |
| Older adults, over 65’s, elderly women | 15 |
| Office workers, science park employees, university office staff, employees, workers | 11 |
| Park users, allotment gardeners, recreational walkers, botanical garden visitors, forest users, GS users, greenway trail users, forest users/volunteers | 18 |
| Female healthcare workers, health care workers, caregivers, rehabilitation team members, practitioners/decision-makers, public sector employees | 6 |
| Athletes, physically active, active runners, experienced runners | 6 |
| Dementia sufferers, cancer patients, palliative care patients, individuals with hypertension, chronic stroke patients | 7 |
| Deprived communities, vulnerable, homeless women, female prisoners, deprived urban neighborhoods | 9 |
| Rural elders, rural population, local residents (predominantly farmers), local residents (farmers and visitors) | 4 |
| Adults with disabilities, individuals with disabilities, individuals with learning difficulties, people with disability | 4 |
| Postmenopausal women, pregnant women, women | 4 |
| Tourists, experienced physically fit backpackers | 3 |
| Forest workers, woodland workers | 3 |
| African Americans | 1 |
| People building houses | 1 |
| Alcoholics | 1 |
| Primary Mental HWB Outcome | # of Times Used |
|---|---|
| Mental health | 37 |
| Wellbeing | 35 |
| Stress | 34 |
| Restorativeness | 20 |
| Depression | 19 |
| Quality of life | 13 |
| Psychological wellbeing | 12 |
| General health | 11 |
| Mental wellbeing | 8 |
| Life satisfaction | 6 |
| Aggression | 4 |
| Affect | 3 |
| General wellbeing | 3 |
| Anxiety, cognition, emotion, happiness, mood, psychological distress, self-esteem, stress reduction | 16 (2 papers for each of the health endpoints) |
| Chronic stress, clinical depression, emotional wellbeing, general preference for GS, health anxiety, job stress, mental stress, personal development, psychological health, psychological restoration, psychological stress, rumination, severe stress, social integration, stress-related mental illness, stress restoration, stressful life events | 17 (1 paper for each of the health endpoints) |
| Abbreviation | Health Outcome Measure | # of Times Used |
|---|---|---|
| DOQ | Developed own questions and questionnaires | 38 |
| PRS | Perceived Restoration Scale [64,65] | 19 |
| PANAS | Positive and Negative Affect Schedule [66] | 17 |
| PSS | Perceived Stress Scale [67] | 16 |
| GHQ | General Health Questionnaire [68] | 15 |
| PS | Population survey with incorporated health and wellbeing assessments | 14 |
| WEMWBS | Warwick-Edinburgh Mental Well-being Scale [69] | 13 |
| HS SF-36 | Health Survey (SF-36) [70] | 10 |
| BDI | Beck Depression Inventory [71,72,73]. | 9 |
| POMS | Profile of Mood States [74,75,76] | 8 |
| CN | Connected to nature [77] | 8 |
| STAI | State-Trait Anxiety Inventory [78] | 8 |
| CES-D | Centre for Epidemiologic Studies Depression Scale for Research in the general population [79] | 7 |
| NCPC | Necker Cube Pattern Control [80] | 6 |
| RSE | Rosenberg self-esteem scale [81] | 5 |
| K10 | Kessler Psychological Distress Scale [82] | 5 |
| SWLS | Satisfaction with Life Scale [83] | 4 |
| WHOQOL | WHO Quality of Life Questionnaire [84] | 4 |
| DASS | Depression Anxiety Stress Scale [85] | 4 |
| PHQ | Patient Health Questionnaire [86] | 4 |
| SMBQ | Shirom-Melmed Burnout Questionnaire [87] | 4 |
| SVS | Subjective Vitality Scale [88] | 4 |
| GDS | Geriatric Depression Scale [89] | 4 |
| HS SF-12 | Health Survey (SF-12) [90,91] | 3 |
| EQ-5D | EuroQol-5Dimensions [92] | 3 |
| INS | Inclusion of Nature in Self scale [93] | 3 |
| ICD | The International Classification of Diseases (WHO) | 3 |
| PWB | Psychological Wellbeing Scale [94] | 2 |
| QPS | QPSNordic-ADW; Nordic Questionnaire for Monitoring the Age Diverse Workforce [95] | 3 |
| BAI | Beck Anxiety Inventory [96] | 2 |
| MHI-5 | Mental Health Inventory [70,97] | 2 |
| MMSE | Mini-Mental state examination (Folstein test) [98] | 2 |
| REQ | Recovery Experience Questionnaire [99] | 2 |
| RRQ | Rumination-Reflection Questionnaire [100] | 2 |
| UWES | Utrecht Work Engagement Scale [101] | 2 |
| MAAS | Mindful Attention and Awareness Scale [102] | 2 |
| FS | Feeling Scale, affective valence assessed by the FS [103] | 2 |
| HAM-17 | Hamilton Depression Rating Scale [104] | 2 |
| IPA | Interpretative Phenomenological Analysis [105] | 2 |
| SHCI | Subjective Health Complaints Inventory [106] | 2 |
| LSIA | Life satisfaction inventory A [107] | 2 |
| SPNE | Scale of Positive and Negative Experience [108] | 2 |
| ZIPERS | Inventory of Personal Reactions, measuring affect [109] | 2 |
| PAQ | Place attachment questionnaire [110,111] | 2 |
| MSS | Mood Survey Scale [112] | 1 |
| GSES | General Self-efficacy Scale [113] | 1 |
| CRC-QOL | Instrument developed by [114,115] to measure quality of life | 1 |
| TPI | Trier Personality Inventory [116] | 1 |
| ABS | Affect Balance Scale [117] | 1 |
| AFI | Attentional function index [118] | 1 |
| BM | Behaviour mapping [119] | 1 |
| BRFSS | Behavioural Risk Factor Surveillance System. (A United States health survey that looks at behavioural risk factors. It is run by Centre for Disease Control and Prevention and conducted by the individual state health departments and is the world’s largest such survey). | 1 |
| BF | Big Five [120] | 1 |
| BSI | Brief Symptom Inventory (anxiety) [121] | 1 |
| BS | Brooding Scale (Rumination) [122] | 1 |
| BPAQ | Buss-Perry Aggression Questionnaire [123] | 1 |
| CMAI | Cohen-Mansfield agitation inventory [124] | 1 |
| CSAI-2 | Competitive state anxiety inventory-2 [125] | 1 |
| CD-RS | Connor-Davidson resilience scale [126] | 1 |
| CS-DD | Cornell scale for depression in Dementia [127] | 1 |
| DSI | Daily Stress Inventory [128] | 1 |
| DEMQOL | Dementia quality of life instrument [129] | 1 |
| SCL-90-R | Symptom Check List [130] | 1 |
| ES-SF | Ecology Scale, Short-Form [131] | 1 |
| EPDS | Edinburgh postnatal Depression Scale [132] | 1 |
| EES | Elevating Experience Scale [133] | 1 |
| EFI | Exercise-Induced Feeling Inventory [134,135] | 1 |
| FAS | Felt Arousal Scale [136] | 1 |
| ES | Ecocentrism scale. Use of natural environments for psychological restoration [137] | 1 |
| GEBS | General Ecological Behaviour Scale [138] | 1 |
| MUNSH | Happiness Scale based on Memorial University of Newfoundland Scale of happiness [139] | 1 |
| Urban HEART-2 | Health Equity Assessment and Response Tool-2 (Urban HEART-2) (http://sdh.umin.jp/heart/) | 1 |
| HAD | Hospital Anxiety and Depression Scale [140] | 1 |
| HPLP-II | Health promoting Lifestyle Profile II [141] | 1 |
| ISS | Importance for Survival Scale [142] | 1 |
| IWG-2006 | International Wellbeing Group 2006. Used to evaluate self-reported, subjective well-being | 1 |
| ISEL | Interpersonal Support Evaluation List [143] | 1 |
| JSS-N | Job Stress Survey [144] | 1 |
| MDI | Major Depression inventory [145,146] | 1 |
| MANSA | Manchester Short Assessment of Quality of life [147] | 1 |
| MC-SDS | Marlow-Crowne Social Desirability Scale [148] | 1 |
| MBI-GS | Korean version of Maslach Burnout Inventory-General Survey [149] | 1 |
| MINI | Mini International Neuropsychiatric Interview [150,151] | 1 |
| MDBF | Multidimensional Comfort Questionnaire [152] | 1 |
| MMS-SF | Multiple Mood Scale-Short form [153] | 1 |
| NCQ | Nature Contact Questionnaire [154] | 1 |
| NMS | Negative Mood Scale [155] | 1 |
| OHI | Oxford Happiness Inventory [156] | 1 |
| OHS | Overall Happiness scale [157] | 1 |
| PGIS | Personal Growth Initiative Scale [158] | 1 |
| PPWB | Physical and Psychological Wellbeing questionnaire [159] | 1 |
| PGWB | Psychological General Well-Being Index [160] | 1 |
| PRQOL | Influence of parks and recreation on quality of life [161,162] | 1 |
| QLCELQ | Quality of Life Concern in End of Life Questionnaire [163,164] | 1 |
| QOLI | Quality of Life Inventory (Frisch, 2009). [165] | 1 |
| QLS | Quality of Life Scale [166] | 1 |
| QLS-ACI | Quality of Life Scale in adults with chronic illness [165] | 1 |
| QOLT | Quality of Life tool [167] | 1 |
| QEWB | Questionnaire for Eudaimonic Well-Being [168] | 1 |
| QEACL | Questionnaires measuring Eudemonia, Apprehension, childhood location. Environments and experiential states. Eliciting participants feelings about place [65] | 1 |
| MOS SF-20 | Rand medical Outcomes Study Health survey (MOS SF-20) [169,170] | 1 |
| RVP | Reason for Visiting the Park, 23-item scale [171,172,173] | 1 |
| REP | Recreation Experience Preference scales [174] | 1 |
| ROS | Restorative Outcome Scale [175,176] | 1 |
| RQE | Restorative quality in environments [65] | 1 |
| RCAS | Role conflict and ambiguity scales [177] | 1 |
| SMS | Sense of Meaning Scale [178] | 1 |
| SCI-93 | Stress and crisis inventory [179,180] | 1 |
| SEES | Subjective Exercise Experiences Scale [181] | 1 |
| BSCS | Self-Control Scale [182] | 1 |
| SRRS | Self-rating restoration scale [183] | 1 |
| SRSA | Self-reported stress and arousal [184] | 1 |
| SOC | Sense of coherence [185] | 1 |
| SHAI | Short Health Anxiety Inventory [186] | 1 |
| SI-happy | Measuring happiness with a single-item scale [187] | 1 |
| SCTS | Social Cohesion and Trust Scale [188] | 1 |
| SPS | Social Provisions Scale [189] | 1 |
| SWS | Stress at Work Scale by the Behavioural Science Institute, Korea university (1999), occupational stress | 1 |
| SRI-MF | Stress response inventory-modified form [190] | 1 |
| SRS-18 | Stress Response Scale [191] | 1 |
| TAP | Taylor Aggression Paradigm [192] | 1 |
| TMM | Model of mood [193] | 1 |
| CMMS | Current mood measurement scale (The best/worst ever; scale taken from [194] | 1 |
| TFI-CS | Therapeutic Factors Inventory–Cohesiveness Scale [195] | 1 |
| VQ | Volitional Questionnaire [196] | 1 |
| WSRI | Workers Stress Response Inventory; an extended version of the Stress Response Inventory-Modified from [190,197] | 1 |
| WOS | Workplace Ostracism Scale [198] | 1 |
| WUS | Wildernism-Urbanism Scale [199] | 1 |
| ZSDS | Zung self-rating depression scale [200] | 1 |
| Paper Number | Primary Health Outcome | Health Outcome Measure | |
|---|---|---|---|
| 1 | [201] | Affect | BDI, SCL-90-R, |
| 2 | [202] | Affect | STAI, RRQ, PANAS |
| 3 | [203] | Affect | QEACL |
| 4 | [204] | Aggression | WOS |
| 5 | [205] | Aggression | TAP, BPAQ, BSCS, PRS; PANAS |
| 6 | [206] | Anxiety | CSAI-2, |
| 7 | [207] | Anxiety | STAI |
| 8 | [208] | Chronic stress | PSS |
| 9 | [209] | Depression | BDI |
| 10 | [210] | Depression | PHQ |
| 11 | [211] | Depression | BRFSS, PHQ |
| 12 | [60] | Depression | BDI, HAM-17, STAI |
| 13 | [212] | Depression | DOQ |
| 14 | [39] | Depression | BDI, AFI, BS, PRS |
| 15 | [213] | Depression | BDI, STAI, PANAS, PSS, TFI-CS |
| 16 | [214] | Depression | IBD, ROS, WEMWBS |
| 17 | [215] | Depression | GDS |
| 18 | [216] | Depression | GDS |
| 19 | [217] | Depression | GDS |
| 20 | [218] | Depression | GHQ |
| 21 | [219] | Depression | CES-D, DOQ |
| 22 | [220] | Depression | MINI, ICD, PSS, WHOQOL |
| 23 | [221] | Depression | EPDS |
| 24 | [222] | Depression | ZSDS |
| 25 | [223] | Depression | CES-D |
| 26 | [224] | Depression | BDI |
| 27 | [225] | Depression | CES-D |
| 28 | [226] | Depression | PHQ |
| 29 | [227] | Emotion | POMS |
| 30 | [228] | Emotional wellbeing | Urban HEART-2 |
| 31 | [229] | General health | GHQ |
| 32 | [230] | General health | GHQ, POPS |
| 33 | [231] | General health | HS SF-36, PSS, DOQ |
| 34 | [232] | General health | HS SF-36, PSS |
| 35 | [233] | General health | POMS, PANAS, ROS, SVS |
| 36 | [24] | General health | POPS, HS SF-36, GHQ, |
| 37 | [234] | General health | POPS |
| 38 | [235] | General health | HS SF-12, |
| 39 | [236] | General wellbeing | RVP, RQE, SWLS, SPNE |
| 40 | [237] | General wellbeing | OHI |
| 41 | [28] | General wellbeing | EQ-5D, GHQ, DOQ, RSE, POMS |
| 42 | [238] | Happiness | SWLS, PANAS |
| 43 | [239] | Health anxiety | SHAI |
| 44 | [240] | Job stress | SWS |
| 45 | [241] | Life satisfaction | DOQ |
| 46 | [242] | Life satisfaction | DOQ |
| 47 | [243] | Life satisfaction | DOQ |
| 48 | [244] | Life Satisfaction | LSIA |
| 49 | [245] | Mental health | GHQ |
| 50 | [25] | Mental health | GHQ |
| 51 | [246] | Mental health | HS SF-36, K10 |
| 52 | [247] | Mental health | DOQ, CES-D, BAI, RCAS |
| 53 | [248] | Mental health | GHQ |
| 54 | [249] | Mental health | POPS, GHQ |
| 55 | [1] | Mental health | HPLP-II, BDI |
| 56 | [250] | Mental health | DASS |
| 57 | [251] | Mental health | DASS, MANSA |
| 58 | [252] | Mental health | PHQ, PSS, BSI |
| 59 | [253] | Mental health | DASS, |
| 60 | [254] | Mental health | PANAS, RSE |
| 61 | [255] | Mental health | GHQ |
| 62 | [256] | Mental health | CES-D |
| 63 | [257] | Mental health | PANAS, HAM-17 |
| 64 | [258] | Mental health | DOQ |
| 65 | [259] | Mental health | PS, GHQ, WEMWBS |
| 66 | [260] | Mental health | PSQ, GSES, MAAS |
| 67 | [261] | Mental health | PS |
| 68 | [262] | Mental health | IPA |
| 69 | [41] | Mental health | VQ |
| 70 | [263] | Mental health | RSE, PSS, POMS |
| 71 | [264] | Mental health | MHI-5 |
| 72 | [265] | Mental health | MHI-5 |
| 73 | [266] | Mental health | HS SF-12, |
| 74 | [267] | Mental health | PS, K10, |
| 75 | [268] | Mental health | HS SF-36, DOQ, |
| 76 | [269] | Mental health | HS SF-36 |
| 77 | [270] | Mental health | GHQ |
| 78 | [271] | Mental health | DASS |
| 79 | [272] | Mental health | GHQ, DOQ |
| 80 | [273] | Mental health | WEMEBS, HS SF-12 |
| 81 | [274] | Mental health | IPA |
| 82 | [275] | Mental health | WEMWBS |
| 83 | [52] | Mental stress | SRS-18 |
| 84 | [276] | Mental wellbeing | PS, HS SF-36, K10, BF, DOQ |
| 85 | [277] | Mental wellbeing | REP, PAQ |
| 86 | [278] | Mental wellbeing | DOQ, WEMWBS, |
| 87 | [279] | Mental wellbeing | PSS, WEMWBS |
| 88 | [280] | Mental wellbeing | WEMWBS |
| 89 | [281] | Mental wellbeing | QOLI, BDI |
| 90 | [282] | Mood | RSE, TMD |
| 91 | [283] | Mood | TBES, DOQ |
| 92 | [284] | Personal development | PGIS, QLS-ACI |
| 93 | [285] | Psychological distress | K10 |
| 94 | [286] | Psychological distress | DOQ |
| 95 | [54] | Psychological health | MMSE, GDS, PS |
| 96 | [287] | Psychological restoration | ES |
| 97 | [288] | Psychological stress | PRS, CN |
| 98 | [289] | Psychological wellbeing | ABS |
| 99 | [290] | Psychological wellbeing | FS, FAS, MSS |
| 100 | [291] | Psychological wellbeing | PRS, PANAS, PSS, CES-D, MUNSH, SPW |
| 101 | [292] | Psychological wellbeing | DOQ |
| 102 | [293] | Psychological wellbeing | CN, WHOQOL |
| 103 | [294] | Psychological wellbeing | STAI, PWB |
| 104 | [295] | Psychological wellbeing | SRSMS |
| 105 | [55] | Psychological wellbeing | DOQ, GHQ, SCTS, SHCI |
| 106 | [296] | Psychological wellbeing | CN, MAAS, FS, SPNE, SVS |
| 107 | [297] | Quality of life | PRQOL |
| 108 | [298] | Quality of life | EQ-5D |
| 109 | [299] | Quality of life | QLCELQ |
| 110 | [300] | Quality of life | CRC-QOL |
| 111 | [301] | Quality of life | DOQ |
| 112 | [302] | Quality of life | LSIA |
| 113 | [61] | Quality of life | QOLT |
| 114 | [303] | Quality of life | DOQ |
| 115 | [62] | Quality of life | QLS |
| 116 | [43] | Quality of life | DEMQOL, CS-DD, CMAI, MMSE |
| 117 | [304] | Recovery | REQ, DOQ |
| 118 | [305] | Restorativeness | EFI, NMS, |
| 119 | [306] | Restorativeness | POMS, PRS, NCPC |
| 120 | [50] | Restorativeness | ZIPERS, NCPC |
| 121 | [50] | Restorativeness | SRRS |
| 122 | [307] | Restorativeness | WUS, ZIPERS, OHS |
| 123 | [308] | Restorativeness | DOQ, PRS |
| 124 | [59] | Restorativeness | DOQ, SRSA |
| 125 | [309] | Restorativeness | NCPC, STAI |
| 126 | [310] | Restorativeness | PRS, SMBQ, HAD, NCPC, DOQ |
| 127 | [142] | Restorativeness | ISS, PRS, |
| 128 | [311] | Restorativeness | DOQ |
| 129 | [33] | Restorativeness | PRS |
| 130 | [312] | Restorativeness | PRS, INS |
| 130 | [313] | Restorativeness | PRS, GEBS, MC-SDS, |
| 131 | [314] | Restorativeness | WHOQOL, PRS, |
| 132 | [315] | Restorativeness | DOQ |
| 133 | [316] | Restorativeness | PRS |
| 134 | [317] | Restorativeness | DOQ |
| 135 | [318] | Restorativeness | PRS |
| 135 | [306] | Restorativeness | POMS, PRS, NCPC |
| 136 | [319] | Rumination | RRQ |
| 137 | [320] | Self-esteem | DOQ |
| 138 | [321] | Self-esteem | RSE, POMS, GHQ |
| 139 | [63] | Stress | ICD, SMBQ |
| 140 | [322] | Stress | PS |
| 141 | [323] | Stress | DOQ |
| 142 | [53] | Stress | PSS, SPS, HS SF-36 |
| 143 | [57] | Stress | SRI-MF |
| 144 | [58] | Stress | MBI-GS, WSRI, REQ |
| 145 | [32] | Stress | CES-D |
| 146 | [324] | Stress | PSQ |
| 147 | [154] | Stress | PSQ, BRFSS |
| 148 | [325] | Stress | DOQ |
| 149 | [326] | Stress | MMS-SF, STAI |
| 150 | [327] | Stress | DSI, MOS SF-20 |
| 151 | [328] | Stress | PSS, WEMWBS |
| 152 | [329] | Stress | PSS, WEMWBS, PS |
| 153 | [37] | Stress | DOQ, SMBQ |
| 154 | [330] | Stress | ICD, BM |
| 155 | [331] | Stress | SCI-93, EQ-5D, |
| 156 | [332] | Stress | PSS, WEMWBS, PS |
| 157 | [333] | Stress | PSS, WEMWBS, PS |
| 158 | [334] | Stress | ROS, PRS, PANAS |
| 159 | [335] | Stress | PANAS |
| 160 | [333] | Stress | PSS, WEMWBS, PS |
| 161 | [336] | Stress reduction | PANAS, NCPC |
| 162 | [337] | Stress reduction | NCQ, QPS, JSS-N, SHCI, DOQ |
| 163 | [36] | Stress related mental illness | SMBQ, BDI, BAI, PGWB |
| 164 | [338] | Stress restoration | TMM |
| 165 | [56] | Stress restoration | PS |
| 166 | [246] | Wellbeing | HS SF-36, DOQ |
| 167 | [339] | Wellbeing | HS SF-36, K10 |
| 168 | [340] | Wellbeing | PS |
| 169 | [45] | Wellbeing | DOQ |
| 170 | [341] | Wellbeing | PRS |
| 171 | [342] | Wellbeing | MDBF, SWLS, TPI, HS SF-36 |
| 172 | [343] | Wellbeing | SVS, UWES, QPS |
| 173 | [344] | Wellbeing | SVS, UWES, QPS |
| 174 | [345] | Wellbeing | DOQ |
| 175 | [346] | Wellbeing | PS |
| 176 | [347] | Wellbeing | WEMWBS, CD-RS, SOC, PS, DOQ |
| 177 | [348] | Wellbeing | CN, PANAS, SEES |
| 178 | [349] | Wellbeing | DOQ, IWG-2006, CN |
| 179 | [350] | Wellbeing | MDI, PSS, PANAS, WEMWBS, ISEL |
| 180 | [351] | Wellbeing | PWB, PANAS, SWLS, ES-SF |
| 181 | [352] | Wellbeing | PANAS, EES, SMS, CN |
| 182 | [353] | Wellbeing | DOQ, OHI, INS |
| 183 | [354] | Wellbeing | CN, PRS, PAQ, PANAS, PPWB |
| 184 | [355] | Wellbeing | STAI, PRS |
| 185 | [356] | Wellbeing | CN, QEWB, WHOQOL |
| 186 | [357] | Wellbeing | DOQ |
| 187 | [358] | Wellbeing | PANAS, INS |
| Mental Health | Wellbeing | Stress | Restorativeness | Depression | Quality of Life | Psychological Wellbeing | General Health | Mental Wellbeing | Life Satisfaction | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GHQ | 8 | DOQ | 7 | PSS | 6 | PRS | 11 | BDI | 5 | DOQ | 2 | DOQ | 2 | GHQ | 3 | WEMWBS | 3 | DOQ | 3 |
| DASS | 4 | PANAS | 6 | PS | 5 | DOQ | 6 | CES-D | 3 | CS-DD | 1 | CN | 2 | POPS | 3 | DOQ | 2 | LSIA | 1 |
| DOQ | 4 | CN | 5 | WEMWBS | 5 | NCPC | 5 | GDS | 3 | CMAI | 1 | FS | 2 | HS SF-36 | 3 | BDI | 1 | ||
| HS SF-36 | 3 | HS SF-36 | 3 | DOQ | 3 | POMS | 2 | PHQ | 3 | CRC-QOL | 1 | ABS | 1 | PSS | 2 | BF | 1 | ||
| PS | 3 | PRS | 3 | ICD | 2 | ZIPERS | 2 | DOQ | 2 | DEMQOL | 1 | CES-D | 1 | DOQ | 1 | HS SF-36 | 1 | ||
| RSE | 2 | PS | 3 | PANAS | 2 | EFI | 1 | PSS | 2 | EQ-5D | 1 | FAS | 1 | HS SF-12 | 1 | K10 | 1 | ||
| WEMWBS | 2 | INS | 2 | PSQ | 2 | HAD | 1 | PHQ | 2 | LSIA | 1 | GHQ | 1 | PANAS | 1 | PAQ | 1 | ||
| CES-D | 2 | QPS | 2 | SMBQ | 2 | ISS | 1 | STAI | 2 | MMSE | 1 | MSS | 1 | POMS | 1 | PS | 1 | ||
| HS SF-12 | 2 | SVS | 2 | BM | 1 | NMS | 1 | AFI | 1 | QLCELQ | 1 | MUNSH | 1 | ROS | 1 | PSS | 1 | ||
| IPA | 2 | SWLS | 2 | BRFSS | 1 | SMBQ | 1 | BRFSS | 1 | QLS | 1 | PANAS | 1 | SVS | 1 | QOLI | 1 | ||
| K10 | 2 | UWES | 2 | CES-D | 1 | SRRS | 1 | BS | 1 | QOLT | 1 | PRS | 1 | REP | 1 | ||||
| MHI-5 | 2 | WEMWBS | 2 | DSI | 1 | SRSA | 1 | EPDS | 1 | PSS | 1 | ||||||||
| PANAS | 2 | CD-RS | 1 | EQ-5D | 1 | STAI | 1 | GHQ | 1 | PWB | 1 | ||||||||
| PSS | 2 | EES | 1 | HS SF-36 | 1 | IBD | 1 | SCTS | 1 | ||||||||||
| BAI | 1 | ES-SF | 1 | MBI-GS | 1 | ICD | 1 | SHCI | 1 | ||||||||||
| POMS | 1 | ISEL | 1 | MMS-SF | 1 | MINI | 1 | SPW | 1 | ||||||||||
| BSI | 1 | IWG-2006 | 1 | MOS SF-20 | 1 | PANAS | 1 | SRSMS | 1 | ||||||||||
| GSES | 1 | K10 | 1 | PRS | 1 | PRS | 1 | STAI | 1 | ||||||||||
| HPLP-II | 1 | MDBF | 1 | REQ | 1 | ROS | 1 | SVS | 1 | ||||||||||
| MANSA | 1 | MDI | 1 | ROS | 1 | WEMWBS | 1 | WHOQOL | 1 | ||||||||||
| MAAS | 1 | OHI | 1 | SCI-93 | 1 | WHOQOL | 1 | ||||||||||||
| PHQ | 1 | PAQ | 1 | SPS | 1 | ZSDS | 1 | ||||||||||||
| POPS | 1 | PPWB | 1 | SRI-MF | 1 | ||||||||||||||
| PSQ | 1 | PSS | 1 | STAI | 1 | ||||||||||||||
| RCAS | 1 | PWB | 1 | WSRI | 1 | ||||||||||||||
| VQ | 1 | QEWB | 1 | ||||||||||||||||
| SEES | 1 | ||||||||||||||||||
| SMS | 1 | ||||||||||||||||||
| SOC | 1 | ||||||||||||||||||
| STAI | 1 | ||||||||||||||||||
| TPI | 1 | ||||||||||||||||||
| WHOQOL | 1 | ||||||||||||||||||
| Paper Number | Country/Green Space | Participant Type | # of Subjects/Male/Female | Mean Age/min/max | Positive/Negative | Health Outcome | Health Assessment | Green Space Assessment | Quantitative/Qualitative Study Methods | Intervention/Control Group | Comments |
| 2-arm randomised controlled crossover design | |||||||||||
| [50] Study 2 * | UK/Natural | University students | 17/7/10 | 23.18 (±6.23)/18/43 | Mixed/Negative | Restorativeness | Questionnaire, heart rate | Photos, videos. No in-depth quality assessment, description, or quantitative measures | Quantitative | Walk through low prospect-high refuge natural environment/Walk through high prospect-low refuge environment | Small study with indication the GS is restorative only when there is an open aspect and few places where someone might hide. |
| [361] | USA/Urban | General public | 12/8/4 | x/x/x | Positive | Stress, Health | Heart rate | Observations. No quantitative assessment | Quantitative | Self-paced walk in local neighbourhood past sites receiving greening treatment/Self-paced walk in local neighbourhood past sites not receiving greening treatment | Small study only measuring heart rate. Based on heart rate only, the results indicated that in-view proximity to a greened vacant lot decreased heart rate compared to in-view proximity to a non-greened vacant lot. |
| [57] | Korea/Natural | University students | 41/14/27 | x/18/35 | Positive | Stress | Cytokine serum levels, questionnaire | No quantitative or qualitative assessment | Quantitative/Qualitative | 2 h exposure to a forest environment/2 h exposure to an urban environment | Small study indicating the level of somatic and depressive symptoms decrease significantly after exposure to forest environments. Weak design; no before-and-after measurements allowing for comparison. |
| [57] | Japan/Natural | Male university students | 12/12/0 | 21.3 (±1.1)/20/23 | Mixed/Negative | Restorativeness | Cortisol, blood pressure, pulse rate, questionnaire | No quantitative or qualitative assessment | Quantitative/Qualitative | 15 min visits to forest environments/15 min visits to urban environments | Small study with no clear conclusion from the quantitative data about the effect of GS. Subjective evaluation data showed significantly more positive responses after exposure to forest environments. |
| [326] | Japan/Natural | General public | 498/244/254 | 56.2 (±10.6)/20/x | Positive | Stress, Mental health | Questionnaire | No quantitative or qualitative assessment | Qualitative | 2 x forest walks/2 days where a forest was not visited | Relatively large number of participants, but no quantitative objective data. The study concluded that a forest environment significantly reduces hostility and depression. The largest benefit was seen for the most stressed participants. |
| [318] | Sweden/Virtual, indoor | Undergraduates | 74/x/x | x/x/x | Positive | Restorativeness | Questionnaire | 852 colour photos of two gardens were sampled. Final sample consisted of 12 photos for each garden. | Qualitative | 2 ha large spacious garden with large as well as small garden rooms and many views without buildings/Small and detailed courtyard garden of 13 × 17 m. Views at eye-level always include buildings. | A study using only one qualitative measure and no quantitative data. The data showed that gardens are likely to be restorative to varying degrees, depending on the design and the surroundings of the garden. |
| [233] | Japan/Urban | Undergraduates | 45/45/0 | 21.13 (±1.25)/x/x | Positive | General health | Questionnaire | Photos. No in-depth quality assessment, description, or quantitative measures | Qualitative | A 15 min walk in a forest environment/A 15 min walk in an urban environment | Relatively small study looking only at young men. Four different validated questionnaires were used; some revealed significant positive effects of the forest environment, some did not. The results indicated the combination of activity and GS results in greater psychological benefits. The feelings of vigour, positive effects, subjective recovery, and vitality were stronger in the forest environment. |
| [209] | USA/Urban | People with depression | 20/8/12 | 26/x/x | Mixed/Negative | Cognition, Affect | Interview, questionnaire | Satellite GPS images. No in-depth quality assessment, description, or quantitative measures | Qualitative | 50 min walk in natural setting/50 min walk in urban setting | Small study with no clear conclusions about the effect of GS. |
| 2-arm randomised controlled design, no crossover | |||||||||||
| Author | Country/Green space | Participant type | # of subjects/male/female | Mean age/min/max | Positive/Negative | Health outcome | Health assessment | Green space assessment | Quantitative/Qualitative | Intervention/Control group | Comments |
| [60] | Korea/Natural | Patients with history of stroke | 59/40/19 | 60.8 (±9.1)/36/79 | Positive | Depression. anxiety | Questionnaire, physiological measurement (Reactive oxygen metabolites (dROM). Biological antioxidant potential (BAPs)) | No in-depth quality assessment, description, or quantitative measures | Quantitative/Qualitative | Patients randomly assigned to a forest therapy group or an urban control group. | The study found that forest therapy can significantly lower oxidative stress and improve anti-oxidative capacity for patients with a history of stroke. High levels of oxidative stress and reduced anti-oxidative capacity are indicative of depression and anxiety. |
| [306] | China/Urban | College students | 32/16/16 | 20.6 (±1.6)/x/x | Positive | Cognition, restorativeness | Questionnaire, EEG | Photos. Quantification of green elements, buildings and paved areas of the two environments used. | Quantitative/Qualitative | 20 min exposure to one of two environments: A wooded campus garden/A traffic island under an elevated highway | Positive EEG results identified from a brief exposure to photographs of nature compared to urban environment (20 min). |
| [319] | USA/Urban | General public | 30/14/16 | 26.6/x/x | Positive | Rumination | Questionnaire, neural activity in the sgPFC | Detailed description of the two walk. | Quantitative/Qualitative | 5.3 km nature walk/5.3 km urban walk | The study found a significant reduction in self-reported rumination driven by a decreased cerebral blood flow in the sgPFC for the nature group, but not for the urban group. |
| [335] | Netherlands/Horticulture, garden | General public | 30/8/22 | 57.6 (±8.49)/38/79 | Positive/mixed | Stress | Questionnaire, salivary cortisol | Very brief description of allotment complex but no in depth description or quantitative measures of the GS investigated | Quantitative/Qualitative | After stress induction: 30 min of outdoor gardening in own allotment/30 min of indoor reading in allotment home with no view of nature (popular magazines chosen by researcher) | The small study found that both reading and gardening showed a significant reduction in cortisol levels after stress. Cortisol levels were lower after gardening compared to reading, but the difference was not significant. Positive mood was significantly higher after gardening compared to reading. There were indications that gardening is more restorative after stress than reading. |
| [204] – study 1 | USA/Virtual, indoor | General public | 86/22/64 | 35.47 (±14.05)/x/x | Positive | Aggression | Questionnaire | Qualitative | Ostracised individuals exposed to urban or nature pictures/Non-ostracised individuals exposed to urban or nature pictures | The qualitative study found that among participants with a high feeling of ostracism, those who viewed nature pictures reported a significantly lower level of aggression than those who viewed urban pictures. The authors concluded that nature exposure can counteract the relationship between ostracism and aggression. | |
| [289] | USA/Virtual, indoor | Older adults | 62/6/56 | x/x/x | Mixed, negative | Physiological wellbeing | Questionnaire | No in-depth quality assessment, description, or quantitative measures | Qualitative | Horticultural activity program in a care home, once a week for 7 weeks/Normal daily activities in a care home, over 7 weeks | The study found no statistically significant differences in the effect of a horticultural activity program on physiological wellbeing of older adults in a care home. However, there were some indications that horticultural activities may have a positive effect on wellbeing. |
| [202] | USA/Urban | General public | 60/27/33 | 22.9/x/x | Mixed | Affect, cognition | Questionnaire | Photos. No in-depth quality assessment, description, or quantitative measures | Qualitative | A nature walk/An urban walk | The study found significant evidence that a nature walk improves affect, but no clear evidence that it improves cognition. |
| [324] | USA/Urban | University office staff | 37/34/3 | 48.8/x/x | Positive | Stress | Questionnaire | No description or quantitative measures of the GS investigated. | Qualitative | Work breaks over 4 weeks: 10–15 min outdoor booster break/standard work break | The small qualitative study found that a 10–15 min outdoor booster break during the work day results in a significantly greater reduction in stress than an indoor work break. |
| [320] | USA/Horticulture, garden | Undergraduates | 32/x/x | x/18/32 | Mixed/Negative | Self-esteem | Questionnaire | No in-depth quality assessment, description, or quantitative measures | Qualitative | 4 h of gardening work over a period of 3 weeks/No gardening activities | This small qualitative study found no significant differences regarding ethnocentrism and self-esteem, in relation to the effects of GS. There were indications that gardening can positively affect self-esteem. |
| [271] | Serbia/Horticulture, garden | Psychiatric patients | 30/9/21 | 45.35 (±10.16)/25/65 | Mixed | Mental health | Questionnaire | Map, photos and short description. No in-depth quality assessment or quantitative measures | Qualitative | Four weeks (12 sessions) of horticultural therapy/Four weeks of occupational art therapy | The small qualitative study found a significantly larger reduction in stress after horticultural therapy compared to occupational art therapy. However, no significant differences were identified for anxiety or depression after the two treatments. |
| 3-arm randomised controlled design, no crossover | |||||||||||
| Author | Country/Green space | Participant type | # of subjects/male/female | Mean age/min/max | Positive/Negative | Health outcome | Health assessment | Green space assessment | Quantitative/Qualitative | Intervention/Control group | Comments |
| [307]-Study 2 ** | USA/Urban | College students | 34/17/17 | 20/x/x | Positive | Restorativeness | Questionnaire, physiological measurements (blood pressure and pulse) | Very brief description of GS | Quantitative/Qualitative | College students were randomly assigned to a nature walk, an urban walk, or a relaxation condition | Small study showing that happiness and positive affect significantly increase and anger and aggression significantly decreased after being in a natural environment compared to an urban environment. |
| [304] | Finland/Urban | Office workers | 153/137/20 | 47.2/x/x | Mixed | Stress, wellbeing | Questionnaire (paper format and mobile text messages) | No in-depth quality assessment, description, or quantitative measures | Qualitative | Park walk/relaxation exercises/usual break activities | The study found no clear conclusions about the effect of park walks on employees’ wellbeing. The effects on wellbeing were of a small magnitude and short duration. |
| [338] | USA/Urban | Park visitors | 108/48/60 | 22/x/x | Mixed, negative | Stress reduction, restorativeness | Questionnaire | No in-depth quality assessment, description, or quantitative measures | Qualitative | ||
| [282] | UK/Urban | Adults with mental health issues | 53/20/33 | 53 (±15.4)/21/83 | Mixed | Mood, self-esteem | Questionnaire | No in-depth quality assessment, description, or quantitative measures | Qualitative | Three health-promoting interventions: Walking in GS/Swimming/Quizzes, bingo, games, crafts and music | The study found that green exercise was as health-promoting for people experiencing mental ill health as existing non-green interventions. There was no conclusive evidence that GS activity was more health-promoting than other activities. |
| [217] | USA/Horticulture, garden | Older adults with mild to moderate depression | 39/16/23 | 74.3 (±6.40)/x/x | Positive | Depression | Questionnaire, focus groups | No in-depth quality assessment, description, or quantitative measures | Qualitative | The participants were randomly assigned to one of 3 treatments; walk alone, guided imagery, or art therapy. | Small study surmising that GS as well as art interventions were helpful in improving mood and overall attitude. However, only subjective, anecdotal evidence was explored. |
| [215] | USA/Horticulture, garden | Older adults with mild to moderate depression | 39/x/x | 75/x/x | Positive/Mixed | Depression | Questionnaire, focus groups | No in-depth quality assessment, description, or quantitative measures | Qualitative | The participants were randomly assigned to one of 3 treatments; walk alone, group walking, or art therapy. | The study found that assisted and unassisted GS walks as well as art therapy interventions can significantly reduce symptoms of depression. |
| [336] | Iceland/Urban | University students | 18/9/9 *** | x/x/x | Mixed/negative | Stress | Interviews, observations | Photos. No in-depth quality assessment, description, or quantitative measures | Qualitative | Three treatments for alleviation of stress: Walking in the gym/Walking in nature/Watching nature on TV | The very small study using personal narratives involving restoration found no clear conclusions about the effect of GS on stress. |
| 4-arm randomised controlled crossover design | |||||||||||
| Author | Country/Green space | Participant type | # of subjects/male/female | Mean age/min/max | Positive/Negative | Health outcome | Health assessment | Green space assessment | Quantitative/Qualitative | Intervention/Control group | Comments |
| [310] | Sweden/Natural | Females diagnosed with exhaustion disorder | 20/0/20 | 41.6 (±7.3)/24/55 | Positive | Restorativeness | Questionnaire, heart rate, blood pressure, heart rate recovery | Photos, detailed description. No quantitative assessment. | Quantitative/Qualitative | 90 min test procedure in 3 different forest environments/and in 1 city environment | Small study indicating significantly higher perceived restorativeness in the forest environments compared to the city. |
| 4-arm randomised controlled design, no crossover | |||||||||||
| Author | Country/Green space | Participant type | # of subjects/male/female | Mean age/min/max | Positive/Negative | Health outcome | Health assessment | Green space assessment | Quantitative/qualitative | Intervention/Control group | Comments |
| [227] | Taiwan/Urban | College students | 116/52/64 | 20.85 (±1.14)/x/x | Mixed/Negative | Emotion, attention | Questionnaire | Photos used to quantify the level of greenness, aerial maps | Quantitative/Qualitative | Walking or jogging in natural environment/Walking or jogging in built environment | The study found no clear conclusions about the effect of GS and exercise on emotion and attention. The key finding is the indication that walking in a setting with at least 40% visible greenness elicits the largest benefits. |
| [204] – study 2 | USA/Virtual, indoor | General public | 150/48/102 | 36.87 (±13.30)/x/x | Mixed | Aggression | Questionnaire | Photos. No in-depth quality assessment, description, or quantitative measures | Qualitative | Ostracised individuals exposed to urban or nature pictures/Non-ostracised individuals exposed to urban or nature pictures | The study found no clear conclusions about the effect of viewing nature photos to moderate the relationship between ostracism and aggression. There were some indications that viewing nature photos can alleviate aggressive responses following ostracism. |
| [204] – study 3 | USA/Virtual, indoor | General public | 144/47/97 | 35.47 (±11.99)/x/x | Mixed | Aggression | Questionnaire | Photos. No in-depth quality assessment, description, or quantitative measures | Qualitative | Ostracised individuals exposed to urban or nature pictures/Non-ostracised individuals exposed to urban or nature pictures | The study found no clear conclusions about the effect of viewing nature photos to moderate the relationship between ostracism and aggression. There were some indications that viewing nature photos can alleviate aggressive responses following ostracism. |
| [205] | China/Virtual, indoor | Undergraduate students | 118/25/93 | 21.23 (±2.26) | Mixed, negative | Aggression, mood | Questionnaire | Video. No in-depth quality assessment, description, or quantitative measures | Qualitative | Depleted individuals exposed to a natural or urban video/Non-depleted individuals exposed to a natural or urban video | The study found no clear conclusions about the effect of viewing a natural video to counteract aggression after depletion. The study suggests that watching a natural video helps to restore self-control after depletion. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wendelboe-Nelson, C.; Kelly, S.; Kennedy, M.; Cherrie, J.W. A Scoping Review Mapping Research on Green Space and Associated Mental Health Benefits. Int. J. Environ. Res. Public Health 2019, 16, 2081. https://doi.org/10.3390/ijerph16122081
Wendelboe-Nelson C, Kelly S, Kennedy M, Cherrie JW. A Scoping Review Mapping Research on Green Space and Associated Mental Health Benefits. International Journal of Environmental Research and Public Health. 2019; 16(12):2081. https://doi.org/10.3390/ijerph16122081
Chicago/Turabian StyleWendelboe-Nelson, Charlotte, Sarah Kelly, Marion Kennedy, and John W. Cherrie. 2019. "A Scoping Review Mapping Research on Green Space and Associated Mental Health Benefits" International Journal of Environmental Research and Public Health 16, no. 12: 2081. https://doi.org/10.3390/ijerph16122081