
Current Role and Future Prospects of Positron Emission Tomography (PET)/Computed Tomography (CT) in the Management of Breast Cancer

{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results and Discussions
3.1. PET-CT in Primary Cancer Diagnosis
3.2. PET-CT in Breast Cancer Staging
3.3. PET-CT and Lymph Node Metastases
3.4. PET-CT and Distant Metastases
3.5. PET-CT and Prognosis
3.6. PET-CT and Treatment Response
3.7. PET-CT and Disease Recurrence
3.8. Impact of Indeterminate Lesions on PET-CT
3.9. PET-CT and Cost Effectiveness
3.10. PET-CT and Future Prospects
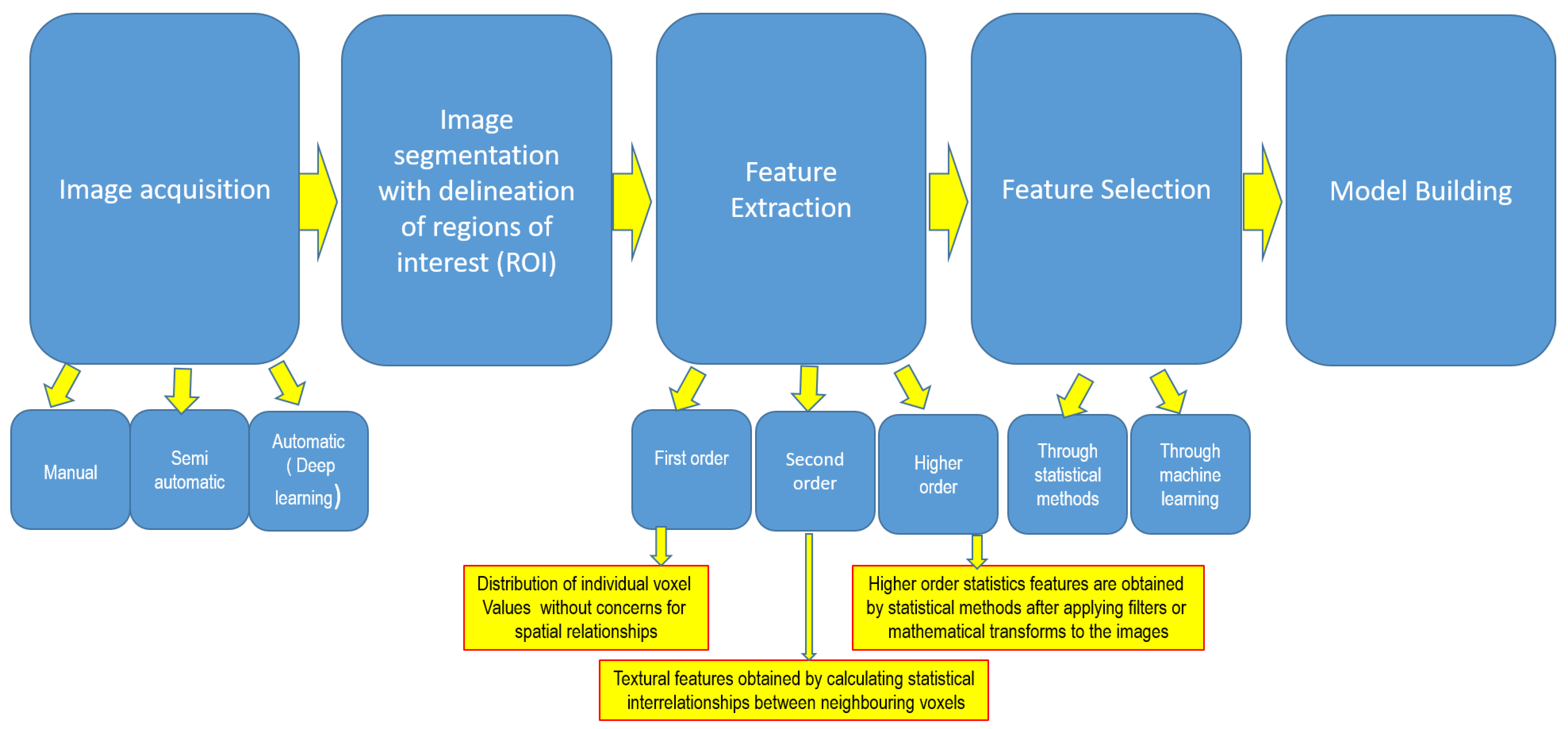
3.10.1. Artificial Intelligence and PET-CT Radiomics
3.10.2. Novel Tracers in PET-CT
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA A Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef]
- Groheux, D. FDG-PET/CT for Primary Staging and Detection of Recurrence of Breast Cancer. Semin. Nucl. Med. 2022, 52, 508–519. [Google Scholar] [CrossRef] [PubMed]
- Cancer Research UK. Breast Cancer Survival Statistics. 2023. Available online: https://web.archive.org/web/20220207071809/https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/breast-cancer/survival (accessed on 30 September 2023).
- James, J.; Teo, M.; Ramachandran, V.; Law, M.; Stoney, D.; Cheng, M. Performance of CT scan of abdomen and pelvis in detecting asymptomatic synchronous metastasis in breast cancer. Int. J. Surg. 2017, 46, 164–169. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Registry. Breast Cancer Incidence, Mortality, Treatment and Survival in Ireland: 1994–2009. [Internet]. Available online: http://www.ncri.ie/publications/statistical-reports/breast-cancer (accessed on 19 March 2023).
- Lyratzopoulos, G.; Abel, G.A.; Barbiere, J.M.; Brown, C.H.; Rous, B.A.; Greenberg, D.C. Variation in advanced stage at diagnosis of lung and female breast cancer in an English region 2006–2009. Br. J. Cancer 2012, 106, 1068–1075. [Google Scholar] [CrossRef]
- Johnson, R.H.; Chien, F.L.; Bleyer, A. Incidence of Breast Cancer with Distant Involvement among Women in the United States, 1976 to 2009. JAMA 2013, 309, 800. [Google Scholar] [CrossRef] [PubMed]
- Costelloe, C.M.; Rohren, E.M.; Madewell, J.E.; Hamaoka, T.; Theriault, R.L.; Yu, T.-K.; Lewis, V.O.; Ma, J.; Stafford, R.J.; Tari, A.M.; et al. Imaging bone metastases in breast cancer: Techniques and recommendations for diagnosis. Lancet Oncol. 2009, 10, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Brennan, M.E.; Houssami, N. Evaluation of the evidence on staging imaging for detection of asymptomatic distant metastases in newly diagnosed breast cancer. Breast 2012, 21, 112–123. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Early and Locally Advanced Breast Cancer: Diagnosis and Management. 2018. Available online: https://www.nice.org.uk/guidance/ng101 (accessed on 20 October 2023).
- National Comprehensive Cancer Network. NCCN Guidelines Breast Cancer. 2023. Available online: https://www.nccn.org/guidelines/recently-published-guidelines (accessed on 30 October 2023).
- Loibl, S.; André, F.; Bachelot, T.; Barrios, C.H.; Bergh, J.; Burstein, H.J.; Cardoso, M.J.; Carey, L.A.; Dawood, S.; Del Mastro, L.; et al. Early Breast Cancer: ESMO Clinical Practice Guideline for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2024, 35, 159–182. [Google Scholar] [CrossRef] [PubMed]
- Abouzied, M.M.; Fathala, A.; AlMuhaideb, A.; Al Qahtani, M.H. Role of 18F-fluorodeoxyglucose positron emission tomography/computed tomography in the evaluation of breast carcinoma: Indications and pitfalls with illustrative case examples. World J. Nucl. Med. 2020, 19, 187–196. [Google Scholar] [CrossRef]
- Niikura, N.; Costelloe, C.M.; Madewell, J.E.; Hayashi, N.; Yu, T.-K.; Liu, J.; Palla, S.L.; Tokuda, Y.; Theriault, R.L.; Hortobagyi, G.N.; et al. FDG-PET/CT compared with conventional imaging in the detection of distant metastases of primary breast cancer. Oncologist 2011, 16, 1111–1119. [Google Scholar] [CrossRef]
- Riedl, C.C.; Slobod, E.; Jochelson, M.; Morrow, M.; Goldman, D.A.; Gonen, M.; Weber, W.A.; Ulaner, G.A. Retrospective analysis of 18F-FDG PET/CT for staging asymptomatic breast cancer patients younger than 40 years. J. Nucl. Med. 2014, 55, 1578–1583. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Chauhan, A.; Zhuang, H.; Chandra, P.; Schnall, M.; Alavi, A. Clinicopathologic factors associated with false negative FDG-PET in primary breast cancer. Breast Cancer Res. Treat. 2006, 98, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Warning, K.; Hildebrandt, M.G.; Kristensen, B.; Ewertz, M. Utility of 18FDG-PET/CT in breast cancer diagnostics—A systematic review. Dan. Med. Bull. 2018, 58, A4289. [Google Scholar]
- Grueneisen, J.; Nagarajah, J.; Buchbender, C.; Hoffmann, O.; Schaarschmidt, B.M.; Poeppel, T.; Forsting, M.; Quick, H.H.; Umutlu, L.; Kinner, S. Positron emission tomography/magnetic resonance imaging for local tumor staging in patients with primary breast cancer: A comparison with positron emission tomography/computed tomography and magnetic resonance imaging. Investig. Radiol. 2015, 50, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Miyake, K.K.; Nakamoto, Y.; Kanao, S.; Tanaka, S.; Sugie, T.; Mikami, Y.; Toi, M.; Togashi, K. Journal Club: Diagnostic value of 18F-FDG PET/CT and MRI in predicting the clinicopathologic subtypes of invasive breast cancer. Am. J. Roentgenol. 2014, 203, 272–279. [Google Scholar] [CrossRef]
- Koo, H.R.; Park, J.S.; Kang, K.W.; Cho, N.; Chang, J.M.; Bae, M.S.; Kim, W.H.; Lee, S.H.; Kim, M.Y.; Kim, J.Y.; et al. 18F-FDG uptake in breast cancer correlates with immunohistochemically defined subtypes. Eur. Radiol. 2014, 24, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Hogan, M.P.; Goldman, D.A.; Dashevsky, B.; Riedl, C.C.; Gönen, M.; Osborne, J.R.; Jochelson, M.; Hudis, C.; Morrow, M.; Ulaner, G.A. Comparison of 18F-FDG PET/CT for Systemic Staging of Newly Diagnosed Invasive Lobular Carcinoma Versus Invasive Ductal Carcinoma. J. Nucl. Med. 2015, 56, 1674–1680. [Google Scholar] [CrossRef]
- Lopez, J.K.; Bassett, L.W. Invasive lobular carcinoma of the breast: Spectrum of mammographic US, and MR imaging findings. Radiographics 2009, 29, 165–176. [Google Scholar] [CrossRef]
- Avril, N.; Menzel, M.; Dose, J.; Schelling, M.; Weber, W.; Jänicke, F.; Nathrath, W.; Schwaiger, M. Glucose metabolism of breast cancer assessed by 18F-FDG PET: Histologic and immunohistochemical tissue analysis. J. Nucl. Med. 2001, 42, 9–16. [Google Scholar]
- Bos, R.; Van der Hoeven, J.J.; Van der Wall, E.; Van der Groep, P.; Van Diest, P.J.; Comans, E.F.; Joshi, U.; Semenza, G.L.; Hoekstra, O.S.; Lammertsma, A.A.; et al. Biologic correlates of 18fluorodeoxyglucose uptake in human breast cancer measured by positron emission tomography. J. Clin. Oncol. 2002, 20, 379–387. [Google Scholar] [CrossRef]
- Dashevsky, B.Z.; Goldman, D.A.; Parsons, M.; Gönen, M.; Corben, A.D.; Jochelson, M.S.; Hudis, C.A.; Morrow, M.; Ulaner, G.A. Appearance of untreated bone metastases from breast cancer on FDG PET/CT: Importance of histologic subtype. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1666–1673. [Google Scholar] [CrossRef]
- Cook, G.J.; Houston, S.; Rubens, R.; Maisey, M.N.; Fogelman, I. Detection of bone metastases in breast cancer by 18FDG PET: Differing metabolic activity in osteoblastic and osteolytic lesions. J. Clin. Oncol. 1998, 16, 3375–3379. [Google Scholar] [CrossRef]
- Nakai, T.; Okuyama, C.; Kubota, T.; Yamada, K.; Ushijima, Y.; Taniike, K.; Suzuki, T.; Nishimura, T. Pitfalls of FDG-PET for the diagnosis of osteoblastic bone metastases in patients with breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2005, 32, 1253–1258. [Google Scholar] [CrossRef]
- Algafri, A.; Al-Tweigeri, T.; Al-Sugair, A.; Al-Seabee, M.; Al-Alawi, E.; Fathala, A.; Almuhaideb, A.; Tuli, M.; Abouzied, M. The Diagnostic Accuracy of FEG PET Low Dose Non Enhanced CT in Detection of Local Recurrence and Distant Metastases during Follow-up of Breast Cancer Patients: A Comparison to Enhanced CT and Bone Scan. In Proceedings of the European Congress of Radiology 2012, Vienna, Austria, 5 March 2012; 5 March 2012. [Google Scholar]
- Davidson, T.; Shehade Nissan, E.; Sklair-Levy, M.; Ben-Haim, S.; Barshack, I.; Zippel, D.; Halevy, A.; Chikman, B. PET/CT in breast cancer staging is useful for evaluation of axillary lymph node and distant metastases. Surg. Oncol. 2021, 38, 101567. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, Y.; Luo, H.; Zhang, J. PET/CT and MRI for Identifying Axillary Lymph Node Metastases in Breast Cancer Patients: Systematic Review and Meta-Analysis. J. Magn. Reson. Imaging 2020, 52, 1840–1851. [Google Scholar] [CrossRef]
- Kutluturk, K.; Simsek, A.; Comak, A.; Gonultas, F.; Unal, B.; Kekilli, E. Factors affecting the accuracy of 18F-FDG PET/CT in evaluating axillary metastases in invasive breast cancer. Niger. J. Clin. Pract. 2019, 22, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Cho, H.; Gwak, G.; Yang, K.; Kim, J.-Y.; Shin, Y.-J.; Seo, Y.Y.; Park, I. Factors affecting the negative predictive value of positron emission tomography/computed tomography for axillary lymph node staging in breast cancer patients. Asian J. Surg. 2020, 43, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Parisse-Di Martino, S.; Faure, C.; Mognetti, T. Discordant results in 18F-FDG PET/CT and ultrasound-based assessment for axillary lymph node metastasis detection: A large retrospective analysis in 560 patients with breast cancer. Cancer Treat. Res. Commun. 2021, 27, 100344. [Google Scholar] [CrossRef] [PubMed]
- Kong, E.; Choi, J. The new perspective of PET/CT for axillary nodal staging in early breast cancer patients according to ACOSOG Z0011 trial PET/CT axillary staging according to Z0011. Nucl. Med. Commun. 2021, 42, 1369–1374. [Google Scholar] [CrossRef]
- Brown, A.H.; Shah, S.; Groves, A.M.; Wan, S.; Malhotra, A. The Challenge of Staging Breast Cancer with PET/CT in the Era of COVID Vaccination. Clin. Nucl. Med. 2021, 46, 1006–1010. [Google Scholar] [CrossRef]
- Yararbas, U.; Çetin, N.; Yeniay, L.; Argon, A.M. The value of 18F-FDG PET/CT imaging in breast cancer staging. Bosn. J. Basic Med Sci. 2018, 18, 72–79. [Google Scholar] [CrossRef]
- Ko, H.; Baghdadi, Y.; Love, C.; Sparano, J.A. Clinical Utility of 18F-FDG PET/CT in Staging Localized Breast Cancer Before Initiating Preoperative Systemic Therapy. J. Natl. Compr. Cancer Netw. 2020, 18, 1240–1246. [Google Scholar] [CrossRef] [PubMed]
- Seo, M.J.; Lee, J.J.; Kim, H.O.; Chae, S.Y.; Park, S.H.; Ryu, J.S.; Ahn, S.H.; Lee, J.W.; Son, B.H.; Gong, G.Y.; et al. Detection of internal mammary lymph node metastasis with 18F-fluorodeoxyglucose positron emission tomography/computed tomography in patients with stage III breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 438–445. [Google Scholar] [CrossRef]
- Vogsen, M.; Jensen, J.D.; Christensen, I.Y.; Gerke, O.; Jylling, A.M.B.; Larsen, L.B.; Braad, P.E.; Søe, K.L.; Bille, C.; Ewertz, M.; et al. FDG-PET/CT in high-risk primary breast cancer-a prospective study of stage migration and clinical impact. Breast Cancer Res. Treat. 2021, 185, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Hansen, J.A.; Naghavi-Bezhad, M.; Gerke, O.; Baun, C.; Falch, K.; Duvnjak, S.; Alavi, A.; Hoilund-Carlsen, P.F.; Hildebrandt, M.G. Diagnosis of bone metastases in breast cancer: Lesion-based sensitivity of dual-time-point FDG-PET/CT compared to low-dose CT and bone scintigraphy. PLoS ONE 2021, 16, e0260066. [Google Scholar] [CrossRef]
- Evangelista, L.; Panunzio, A.; Polverosi, R.; Ferretti, A.; Chondrogiannis, S.; Pomerri, F.; Rubello, D.; Muzzio, P.C. Early bone marrow metastasis detection: The additional value of FDG-PET/CT vs. CT imaging. Biomed. Pharmacother. 2012, 66, 448–453. [Google Scholar] [CrossRef]
- Rong, J.; Wang, S.; Ding, Q.; Yun, M.; Zheng, Z.; Ye, S. Comparison of 18 FDG PET-CT and bone scintigraphy for detection of bone metastases in breast cancer patients. A meta-analysis. Surg. Oncol. 2013, 22, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Baba, S.; Isoda, T.; Maruoka, Y.; Kitamura, Y.; Sasaki, M.; Yoshida, T.; Honda, H. Diagnostic and prognostic value of pretreatment SUV in 18F-FDG/PET in breast cancer: Comparison with apparent diffusion coefficient from diffusion weighted MR imaging. J. Nucl. Med. 2014, 55, 736–742. [Google Scholar] [CrossRef]
- Chang, C.C.; Tu, H.P.; Chen, Y.W.; Lin, C.Y.; Hou, M.F. Tumour and lymph node uptakes on dual-phased 2-deoxy-2-[18F]fluoro-D-glucose positron emission tomography/computed tomography correlate with prognostic parameters in breast cancer. J. Int. Med. Res. 2014, 42, 1209–1221. [Google Scholar] [CrossRef]
- Diao, W.; Tian, F.; Jia, Z. The prognostic value of SUVmax measuring on primary lesion and ALN by 18F-FDG PET or PET/CT in patients with breast cancer. Eur. J. Radiol. 2018, 105, 1–7. [Google Scholar] [CrossRef]
- Kitajima, K.; Higuchi, T.; Fujimoto, Y.; Ishikawa, E.; Yokoyama, H.; Komoto, H.; Inao, Y.; Yamakado, K.; Miyoshi, Y. Relationship between FDG-PET and the immune microenvironment in breast cancer. Eur. J. Radiol. 2023, 158, 110661. [Google Scholar] [CrossRef] [PubMed]
- Groheux, D.; Giacchetti, S.; Delord, M.; de Roquancourt, A.; Merlet, P.; Hamy, A.S.; Espié, M.; Hindié, E. Prognostic impact of 18F-FDG PET/CT staging and of pathological response to neoadjuvant chemotherapy in triple-negative breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Choi, J.Y. Prognostic value of 18F-FDG PET and PET/CT for assessment of treatment response to neoadjuvant chemotherapy in breast cancer: A systematic review and metaanalysis. Breast Cancer Res. 2020, 22, 119. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Wang, L.; Jiang, X.; She, W.; He, L.; Hu, G. Diagnostic efficacy of 18F-FDG-PET or PET/CT in breast cancer with suspected recurrence: A systematic review and meta-analysis. Nucl. Med. Commun. 2016, 37, 1180–1188. [Google Scholar] [CrossRef]
- Hildebrandt, M.G.; Gerke, O.; Baun, C.; Falch, K.; Hansen, J.A.; Farahani, Z.A.; Petersen, H.; Larsen, L.B.; Duvnjak, S.; Buskevica, I.; et al. [18F]Fluorodeoxyglucose (FDG)-Positron Emission Tomography (PET)/Computed Tomography (CT) in suspected recurrent breast cancer: A prospective comparative study of dual-time-point FDG-PET/CT, Contrast-Enhanced CT, and bone scintigraphy. J. Clin. Oncol. 2016, 34, 1889–1897. [Google Scholar] [CrossRef] [PubMed]
- Vogsen, M.; Jensen, J.D.; Gerke, O.; Jylling, A.M.B.; Asmussen, J.T.; Christensen, I.Y.; Braad, P.E.; Thye-Rønn, P.; Søe, K.L.; Ewertz, M.; et al. Benefits and harms of implementing [18F]FDG-PET/CT for diagnosing recurrent breast cancer: A prospective clinical study. EJNMMI Res. 2021, 11, 93. [Google Scholar] [CrossRef]
- Dong, Y.; Hou, H.; Wang, C.; Li, J.; Yao, Q.; Amer, S.; Tian, M. The Diagnostic Value of 18F-FDG PET/CT in Association with Serum Tumor Marker Assays in Breast Cancer Recurrence and Metastasis. BioMed Res. Int. 2015, 2015, 489021. [Google Scholar] [CrossRef]
- Corso, G.; Gilardi, L.; Girardi, A.; De Scalzi, A.M.; Pagani, G.; Rossi, E.M.C.; Montagna, G.; Veronesi, P.; Pagan, E.; Bagnardi, V.; et al. How useful are tumor markers in detecting metastases with FDG-PET/CT during breast cancer surveillance? Oncology 2020, 98, 714–718. [Google Scholar] [CrossRef]
- Ishimori, T.; Patel, P.V.; Wahl, R.L. Detection of unexpected additional primary malignancies with PET/CT. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2005, 46, 752–757. [Google Scholar]
- Britt, C.J.; Maas, A.M.; Kennedy, T.A.; Hartig, G.K. Incidental findings on FDG PET/CT in head and neck cancer. Otolaryngol. Head. Neck Surg. 2018, 158, 484–488. [Google Scholar] [CrossRef]
- Kousgaard, S.J.; Thorlacius-Ussing, O. Incidental colorectal FDG uptake on PET/CT scan and lesions observed during subsequent colonoscopy: A systematic review. Tech. Coloproctol. 2017, 21, 521–529. [Google Scholar] [CrossRef]
- Rohde, M.; Nielsen, A.L.; Johansen, J.; Sørensen, J.A.; Nguyen, N.; Diaz, A.; Nielsen, M.K.; Asmussen, J.T.; Christiansen, J.M.; Gerke, O.; et al. Head-to-head comparison of chest X-ray/head and neck MRI, chest CT/head and neck MRI, and (18)F-FDG PET/CT for detection of distant metastases and synchronous cancer in oral, pharyngeal, and laryngeal cancer. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2017, 58, 1919–1924. [Google Scholar]
- Sponholtz, S.E.; Mogensen, O.; Hildebrandt, M.G.; Jensen, P.T. Clinical impact of pre-treatment FDG-PET/CT staging of primary ovarian, fallopian tube, and peritoneal cancers in women. Acta Obstet. Gynecol. Scand. 2020, 99, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Hyland, C.J.; Varghese, F.; Yau, C.; Beckwith, H.; Khoury, K.; Varnado, W.; Hirst, G.L.; Flavell, R.R.; Chien, A.J.; Yee, D.; et al. Use of 18F-FDG PET/CT as an Initial Staging Procedure for Stage II–III Breast Cancer: A Multicenter Value Analysis. J. Natl. Compr. Cancer Netw. 2020, 18, 1510–1517. [Google Scholar] [CrossRef]
- Katal, S.; Eibschutz, L.S.; Saboury, B.; Gholamrezanezhad, A.; Alavi, A. Advantages and Applications of Total-Body PET Scanning. Diagnostics 2022, 12, 426. [Google Scholar] [CrossRef] [PubMed]
- Sui, X.; Liu, G.; Hu, P.; Chen, S.; Yu, H.; Wang, Y.; Shi, H. Total-Body PET/Computed Tomography Highlights in Clinical Practice. PET Clin. 2021, 16, 9–14. [Google Scholar] [CrossRef]
- Lan, X.; Fan, K.; Li, K.; Cai, W. Dynamic PET imaging with ultra-low-activity of 18F-FDG: Unleashing the potential of total-body PET. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4138–4141. [Google Scholar] [CrossRef] [PubMed]
- Roop, M.J.; Singh, B.; Singh, H.; Watts, A.; Kohli, P.S.; Mittal, B.R.; Singh, G. Incremental Value of Cocktail 18F-FDG and 18F-NaF PET/CT over 18F-FDG PET/CT Alone for Characterization of Skeletal Metastases in Breast Cancer. Clin. Nucl. Med. 2017, 42, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Ulaner, G.A.; Hyman, D.M.; Lyashchenko, S.K.; Lewis, J.S.; Carrasquillo, J.A. 89Zr-Trastuzumab PET/CT for detection of human epidermal growth factor receptor 2-positive metastases in patients with human epidermal growth factor receptor 2-negative primary breast cancer. Clin. Nucl. Med. 2017, 42, 912–917. [Google Scholar] [CrossRef]
- Haynes, B.; Sarma, A.; Nangia-Makker, P.; Shekhar, M.P. Breast cancer complexity: Implications of intratumoral heterogeneity in clinical management. Cancer Metastasis Rev. 2017, 36, 547–555. [Google Scholar] [CrossRef]
- Cajal, S.R.Y.; Sesé, M.; Capdevila, C.; Aasen, T.; Mattos-Arruda, L.; Diaz-Cano, S.J.; Hernández-Losa, J.; Castellví, J. Clinical implications of intratumor heterogeneity: Challenges and opportunities. J. Mol. Med. 2020, 98, 161. [Google Scholar] [CrossRef]
- Castello, A.; Castellani, M.; Florimonte, L.; Urso, L.; Mansi, L.; Lopci, E. The Role of Radiomics in the Era of Immune Checkpoint Inhibitors: A New Protagonist in the Jungle of Response Criteria. J. Clin. Med. 2022, 11, 1740. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.; Primakov, S.; Beuque, M.; Woodruff, H.; Halilaj, I.; Wu, G.; Refaee, T.; Granzier, R.; Widaatalla, Y.; Hustinx, R.; et al. Radiomics for precision medicine: Current challenges, future prospects, and the proposal of a new framework. Methods 2021, 188, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Fallahpoor, M.; Chakraborty, S.; Pradhan, B.; Faust, O.; Barua, P.D.; Chegeni, H.; Acharya, R. Deep learning techniques in PET/CT imaging: A comprehensive review from sinogram to image space. Comput. Methods Programs Biomed. 2024, 243, 107880. [Google Scholar] [CrossRef]
- Aktolun, C. Artificial intelligence and radiomics in nuclear medicine: Potentials and challenges. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2731–2736. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.J.; Kim, Y.; Kim, B.S. Intratumoral metabolic heterogeneity predicts invasive components in breast ductal carcinoma in situ. Eur. Radiol. 2015, 25, 3648–3658. [Google Scholar] [CrossRef]
- Lemarignier, C.; Martineau, A.; Teixeira, L.; Vercellino, L.; Espié, M.; Merlet, P.; Groheux, D. Correlation between tumour characteristics, SUV measurements, metabolic tumour volume, TLG and textural features assessed with 18F-FDG PET in a large cohort of oestrogen receptor-positive breast cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1145–1154. [Google Scholar] [CrossRef]
- Ha, S.; Park, S.; Bang, J.I.; Kim, E.K.; Lee, H.Y. Metabolic Radiomics for Pretreatment 18F-FDG PET/CT to Characterize Locally Advanced Breast Cancer: Histopathologic Characteristics, Response to Neoadjuvant Chemotherapy, and Prognosis. Sci. Rep. 2017, 7, 1556. [Google Scholar] [CrossRef]
- Aide, N.; Elie, N.; Blanc-Fournier, C.; Levy, C.; Salomon, T.; Lasnon, C. Hormonal Receptor Immunochemistry Heterogeneity and 18F-FDG Metabolic Heterogeneity: Preliminary Results of Their Relationship and Prognostic Value in Luminal Non-Metastatic Breast Cancers. Front. Oncol. 2021, 10, 599050. [Google Scholar] [CrossRef]
- Molina-García, D.; García-Vicente, A.M.; Pérez-Beteta, J.; Amo-Salas, M.; Martínez-González, A.; Tello-Galán, M.J.; Soriano-Castrejón, Á.; Pérez-García, V.M. Intratumoral heterogeneity in (18)F-FDG PET/CT by textural analysis in breast cancer as a predictive and prognostic subrogate. Ann. Nucl. Med. 2018, 32, 379–388. [Google Scholar] [CrossRef]
- Yoon, H.J.; Kim, Y.; Chung, J.; Kim, B.S. Predicting neo-adjuvant chemotherapy response and progression-free survival of locally advanced breast cancer using textural features of intratumoral heterogeneity on F-18 FDG PET/CT and diffusion-weighted MR imaging. Breast J. 2019, 25, 373–380. [Google Scholar] [CrossRef]
- Park, J.E.; Kim, D.; Kim, H.S.; Park, S.Y.; Kim, J.Y.; Cho, S.J.; Shin, J.H.; Kim, J.H. Quality of science and reporting of radiomics in oncologic studies: Room for improvement according to radiomics quality score and TRIPOD statement. Eur. Radiol. 2020, 30, 523–536. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Wang, X.; Xu, C.; Liu, C.; Zheng, C.; Fulham, M.J.; Feng, D.; Wang, L.; Song, S.; Huang, G. 18F-FDG PET/CT radiomic predictors of pathologic complete response (pCR) to neoadjuvant chemotherapy in breast cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1116–1126. [Google Scholar] [CrossRef]
- Song, B.-I. A machine learning-based radiomics model for the prediction of axillary lymph-node metastasis in breast cancer. Breast Cancer 2021, 28, 664–671. [Google Scholar] [CrossRef]
- Moreau, N.; Rousseau, C.; Fourcade, C.; Santini, G.; Brennan, A.; Ferrer, L.; Lacombe, M.; Guillerminet, C.; Colombié, M.; Jézéquel, P.; et al. Automatic segmentation of metastatic breast cancer lesions on18f-fdg pet/ct longitudinal acquisitions for treatment response assessment. Cancers 2022, 14, 101. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Franc, B.L.; Harnish, R.J.; Liu, G.; Mitra, D.; Copeland, T.P.; Arasu, V.A.; Kornak, J.; Jones, E.F.; Behr, S.C.; et al. Exploration of PET and MRI radiomic features for decoding breast cancer phenotypes and prognosis. Npj Breast Cancer 2018, 4, 24. [Google Scholar] [CrossRef]
- Satoh, Y.; Imokawa, T.; Fujioka, T.; Mori, M.; Yamaga, E.; Takahashi, K.; Takahashi, K.; Kawase, T.; Kubota, K.; Tateishi, U.; et al. Deep learning for image classification in dedicated breast positron emission tomography (dbPET). Ann. Nucl. Med. 2022, 36, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Urso, L.; Manco, L.; Castello, A.; Evangelista, L.; Guidi, G.; Massimo Castellani, M.; Florimonte, L.; Cittanti, C.; Turra, A.; Panareo, S. PET-Derived Radiomics and Artificial Intelligence in Breast Cancer: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 13409. [Google Scholar] [CrossRef]
- Balma, M.; Liberini, V.; Racca, M.; Laudicella, R.; Bauckneht, M.; Buschiazzo, A.; Nicolotti, D.G.; Peano, S.; Bianchi, A.; Albano, G.; et al. Non-conventional and Investigational PET Radiotracers for Breast Cancer: A Systematic Review. Front. Med. 2022, 9, 881551. [Google Scholar] [CrossRef]
- Ulaner, G.A.; Schuster, D.M. Amino acid metabolism as a target for breast cancer imaging. PET Clin. 2018, 13, 437–444. [Google Scholar] [CrossRef]
- Ulaner, G.A.; Goldman, D.A.; Gönen, M.; Pham, H.; Castillo, R.; Lyashchenko, S.K.; Lewis, J.S.; Dang, C. Initial results of a prospective clinical trial of 18FFluciclovine PET/CT in newly diagnosed invasive ductal and invasive lobular breast cancers. J. Nucl. Med. 2016, 57, 1350–1356. [Google Scholar] [CrossRef]
- Tade, F.I.; Cohen, M.A.; Styblo, T.M.; Odewole, O.A.; Holbrook, A.I.; Newell, M.S.; Savir-Baruch, B.; Li, X.; Goodman, M.M.; Nye, J.A.; et al. Anti-3-18F-FACBC (18F-Fluciclovine) PET/CT of breast cancer: An exploratory study. J. Nucl. Med. 2016, 57, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Kurland, B.F.; Wiggins, J.R.; Coche, A.; Fontan, C.; Bouvet, Y.; Webner, P.; Divgi, C.; Linden, H.M. Whole-body characterization of estrogen receptor status in metastatic breast cancer with 16a-18F-Fluoro-17b-estradiol positron emission tomography: Meta-analysis and recommendations for integration into clinical applications. Oncologist 2020, 25, 835–844. [Google Scholar] [CrossRef] [PubMed]
- Bensch, F.; Brouwers, A.H.; Hooge, M.N.L.-D.; de Jong, J.R.; van der Vegt, B.; Sleijfer, S.; de Vries, E.G.E.; Schröder, C.P. 89Zr-trastuzumab PET supports clinical decision making in breast cancer patients, when HER2 status cannot be determined by standard work up. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2300–2306. [Google Scholar] [CrossRef] [PubMed]
- Bensch, F.; Van der veen, E.L.; Lub-de Hooge, M.N.; Jorritsma-Smit, A.; Boellaard, R.; Kok, I.C.; Oosting, S.F.; Schröder, C.P.; Hiltermann, T.J.N.; Van Der Wekken, A.J.; et al. 89Zr-atezolizumab imaging as a non-invasive approach to assess clinical response to PD-L1 blockade in cancer. Nat. Med. 2018, 24, 1852–1858. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robson, N.; Thekkinkattil, D.K. Current Role and Future Prospects of Positron Emission Tomography (PET)/Computed Tomography (CT) in the Management of Breast Cancer. Medicina 2024, 60, 321. https://doi.org/10.3390/medicina60020321
Robson N, Thekkinkattil DK. Current Role and Future Prospects of Positron Emission Tomography (PET)/Computed Tomography (CT) in the Management of Breast Cancer. Medicina. 2024; 60(2):321. https://doi.org/10.3390/medicina60020321
Chicago/Turabian StyleRobson, Nicole, and Dinesh Kumar Thekkinkattil. 2024. "Current Role and Future Prospects of Positron Emission Tomography (PET)/Computed Tomography (CT) in the Management of Breast Cancer" Medicina 60, no. 2: 321. https://doi.org/10.3390/medicina60020321