
Mixed Eccrine Cutaneous Tumor with Folliculo–Sebaceous Differentiation: Case Report and Literature Review

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Background
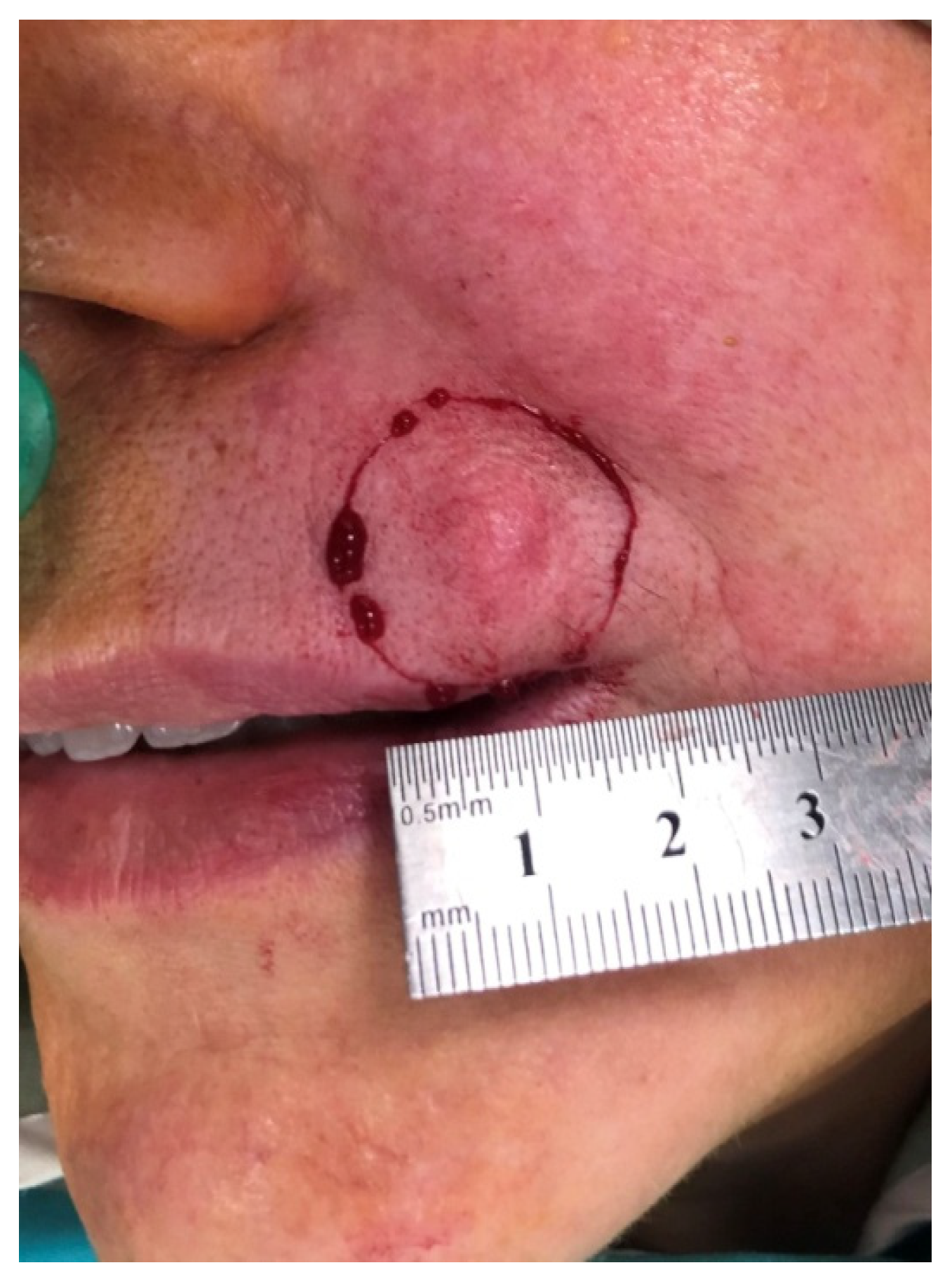
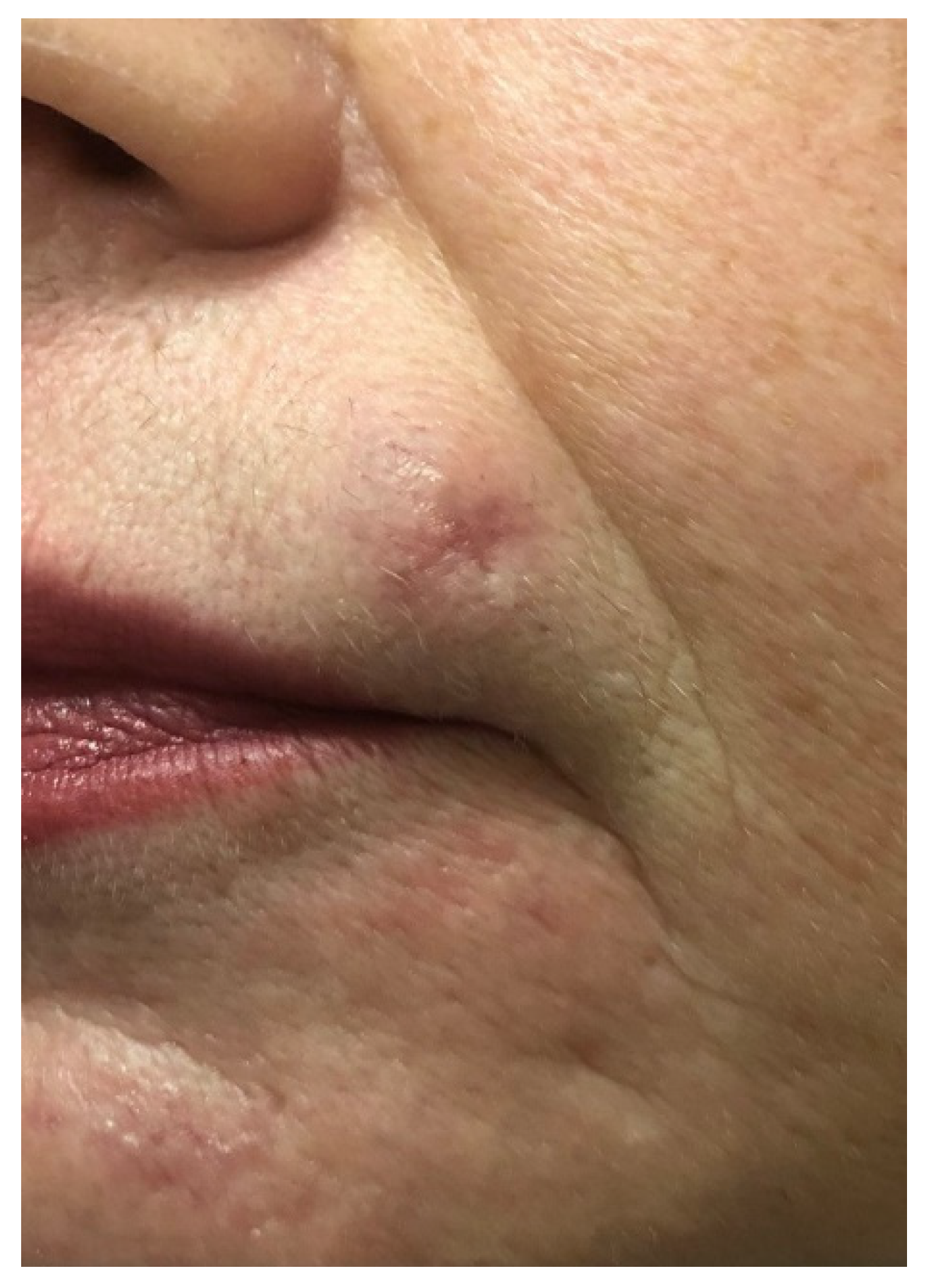
2. Case Report
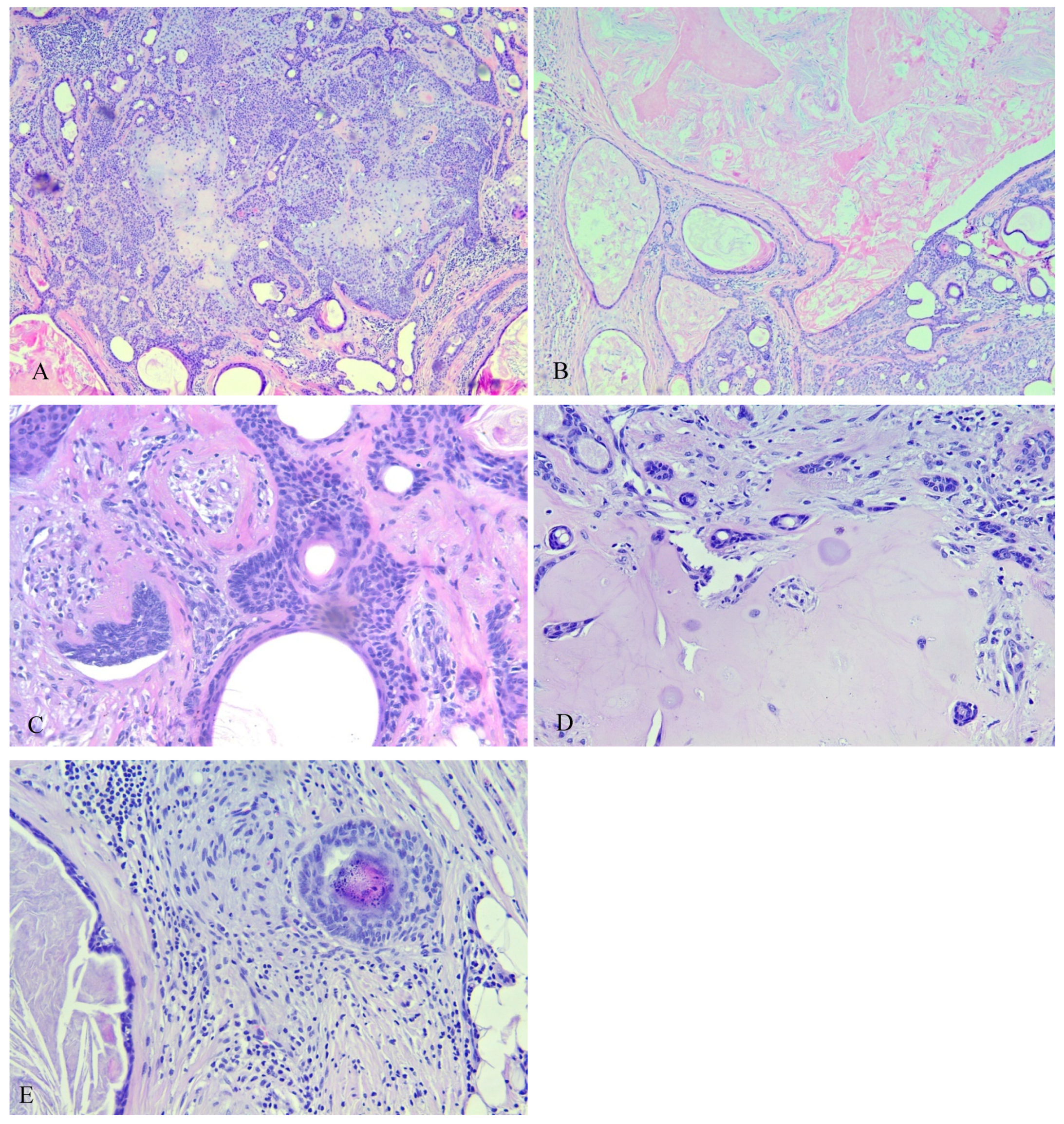
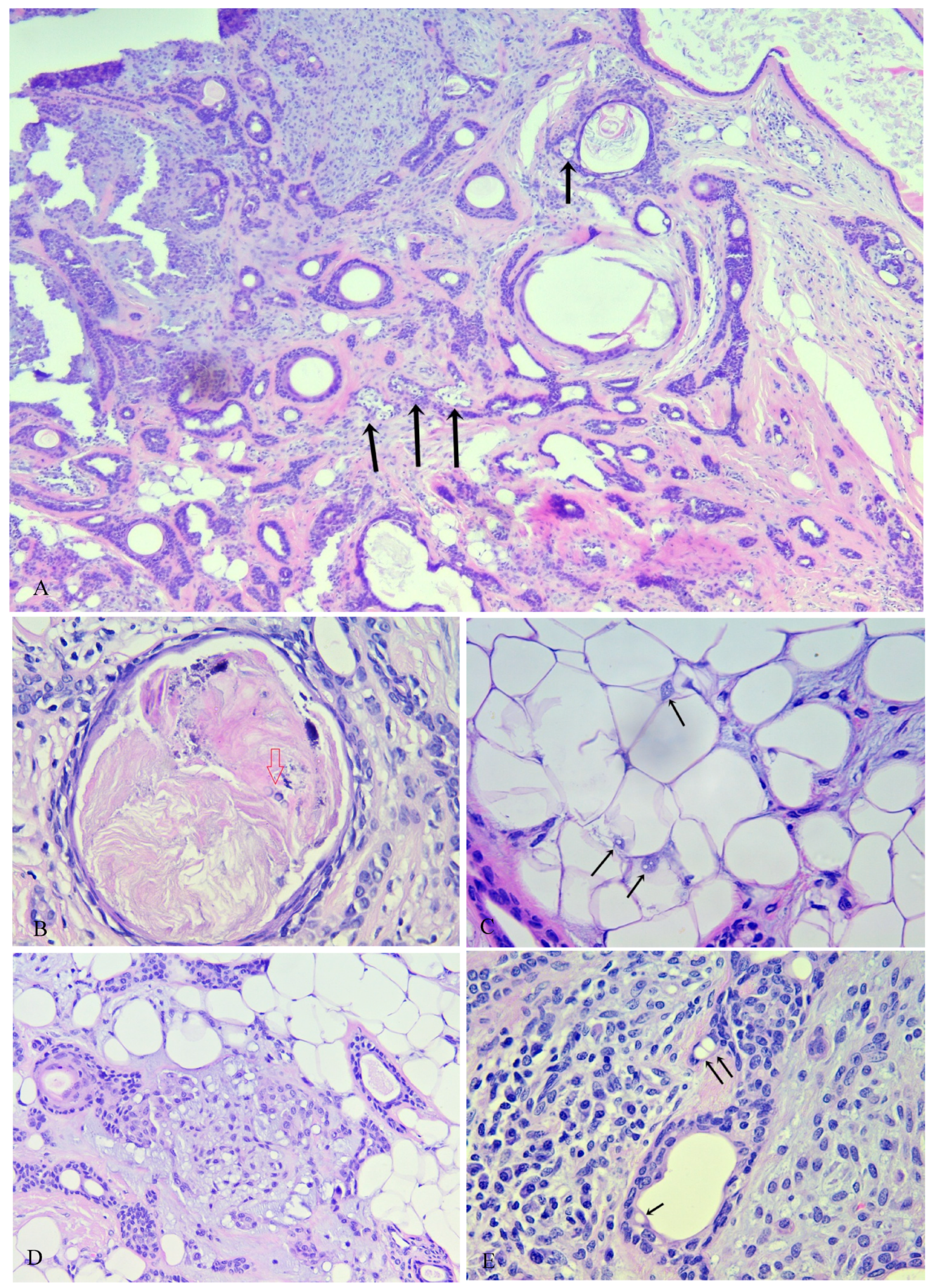
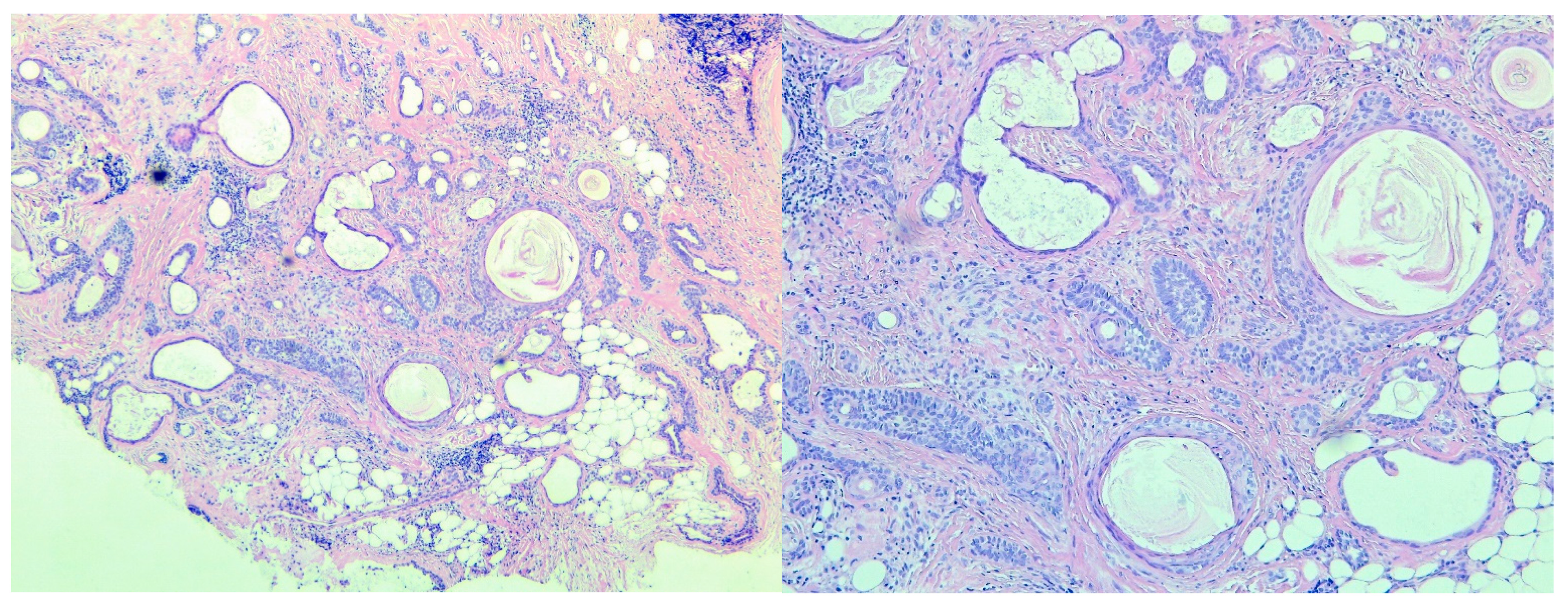
3. Histopathologic Assessment
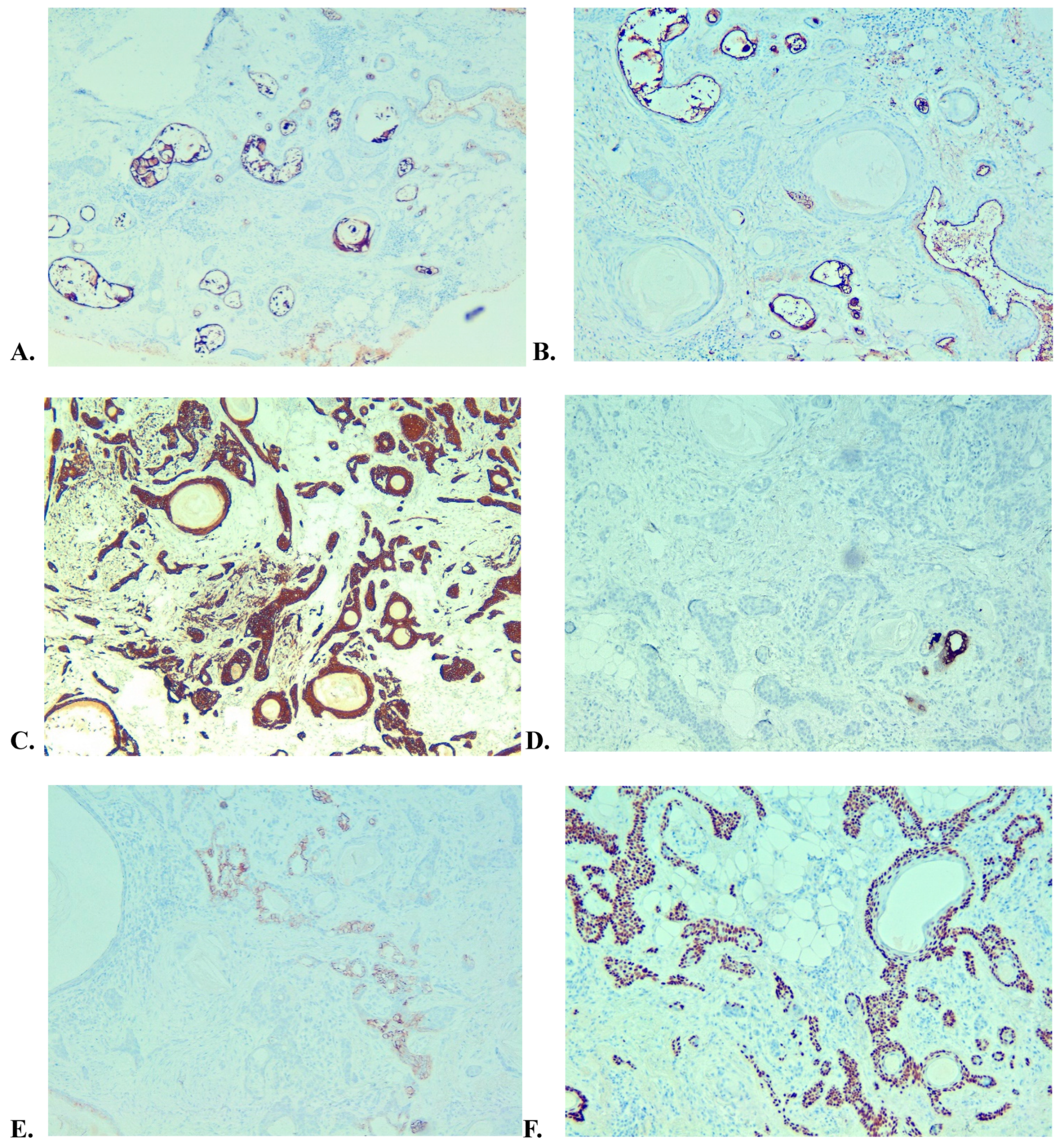
4. Immunohistochemical Study
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wan, H.; Xu, M.; Xia, T. Clinical and pathological study on mixed tumors of the skin. Medicine 2018, 97, e12216. [Google Scholar] [CrossRef] [PubMed]
- Kazakov, D.V.; Belousova, I.E.; Bisceglia, M.; Calonje, E.; Emberger, M.; Grayson, W.; Hantschke, M.; Kempf, W.; Kutzner, H.; Michal, M.; et al. Apocrine mixed tumor of the skin (“mixed tumor of the folliculosebaceous-apocrine complex”). Spectrum of differentiations and metaplastic changes in the epithelial, myoepithelial, and stromal components based on a histopathologic study of 244 cases. J. Am. Acad. Dermatol. 2007, 57, 467–483. [Google Scholar] [CrossRef] [PubMed]
- Kazakov, D.V.; Kacerovska, D.; Hantschke, M.; Zelger, B.; Kutzner, H.; Requena, L.; Grayson, W.; Bisceglia, M.; Schaller, J.; Kempf, W.; et al. Cutaneous mixed tumor, eccrine variant: A clinicopathologic and immunohistochemical study of 50 cases, with emphasis on unusual histopathologic features. Am. J. Dermatopathol. 2011, 33, 557–568. [Google Scholar] [CrossRef]
- Rodríguez-Díaz, E.; Armijo, M. Mixed tumors with follicular differentiation: Complex neoplasms of the primary epithelial germ. Int. J. Dermatol. 1995, 34, 782–785. [Google Scholar] [CrossRef]
- Mills, S.E. Mixed tumor of the skin: A model of divergent differentiation. J. Cutan. Pathol. 1984, 11, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Ansai, S.; Takayama, R.; Kimura, T.; Kawana, S. Ber-EP4 is a useful marker for follicular germinative cell differentiation of cutaneous epithelial neoplasms. J. Dermatol. 2012, 39, 688–692. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, P.; Helwig, E.B. Chondroid Syringoma: Mixed Tumor of Skin, Salivary Gland Type. Arch. Dermatol. 1961, 84, 835–847. [Google Scholar] [CrossRef]
- Yavuzer, R.; Başterzi, Y.; Sari, A.; Bir, F.; Sezer, C. Chondroid syringoma: A diagnosis more frequent than expected. Dermatol. Surg. 2003, 29, 179–181. [Google Scholar] [CrossRef]
- Baran, J.L.; Hoang, M.P. Apocrine mixed tumor of the skin with a prominent pilomatricomal component. J. Cutan. Pathol. 2009, 36, 882–886. [Google Scholar] [CrossRef]
- Chen, A.H.; Moreano, E.H.; Houston, B.; Funk, F.G. Chondroid syringoma of the head and neck: Clinical management and literature review. Ear Nose Throat J. 1996, 75, 104–108. [Google Scholar] [CrossRef]
- Tirumalae, R.; Boer, A. Calcification and ossification in eccrine mixed tumors: Underrecognized feature and diagnostic pitfall. Am. J. Dermatopathol. 2009, 31, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Linares González, L.; Aguayo Carreras, P.; Rueda Villafranca, B.; Navarro-Triviño, F.J. Chondroid Syringoma Mimicking Basal Cell Carcinoma. Actas Dermo-Sifiliográficas 2020, 111, 341–343. [Google Scholar] [CrossRef]
- Shimizu, S.; Han-Yaku, H.; Fukushima, S.; Shimizu, H. Immunohistochemical study of mixed tumor of the skin with marked ossification. Dermatology 1996, 193, 255–257. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.; Squires, S.; Machan, M.; Fraga, G.R.; Aires, D. Cutaneous mixed tumor with extensive chondroid metaplasia: A potential mimic of cutaneous chondroma. Dermatol. Online J. 2012, 18, 9. [Google Scholar] [CrossRef] [PubMed]
- Kazakov, D.V.; Bisceglia, M.; Spagnolo, D.V.; Kutzner, H.; Belousova, I.E.; Hes, O.; Sima, R.; Vanecek, T.; Yang, Y.; Michal, M. Apocrine mixed tumors of the skin with architectural and/or cytologic atypia: A retrospective clinicopathologic study of 18 cases. Am. J. Surg. Pathol. 2007, 31, 1094–1102. [Google Scholar] [CrossRef]
- Gottschalk-Sabag, S.; Glick, T. Chondroid syringoma diagnosed by fine-needle asp iration: A case report. Diagn. Cytopathol. 1994, 10, 152–155. [Google Scholar] [CrossRef]
- Srinivasan, R.; Rajwanshi, A.; Padmanabhan, Y.; Dey, P. Fine needle aspiration cytology of chondroid syringoma and syringocystadenoma papilliferum: A report of two cases. Acta Cytol. 1993, 37, 535–538. [Google Scholar]
- Faur, C.I.; Moldovan, M.A.; Văleanu, M.; Rotar, H.; Filip, L.; Roman, R.C. The Prevalence and Treatment Costs of Non-Melanoma Skin Cancer in Cluj-Napoca Maxillofacial Center. Medicina 2023, 59, 220. [Google Scholar] [CrossRef]
- Harrist, T.J.; Aretz, T.H.; Mihm, M.C., Jr.; Evans, G.W.; Rodriquez, F.L. Malignant chondroid syringoma. Arch. Dermatol. 1981, 117, 719–724. [Google Scholar] [CrossRef]
- Lal, K.; Morrell, T.J.; Cunningham, M.; O’Donnell, P.; Levin, N.A.; Cornejo, K.M. A Case of a Malignant Cutaneous Mixed Tumor (Chondroid Syringoma) of the Scapula Treated With Staged Margin-Controlled Excision. Am. J. Dermatopathol. 2018, 40, 679–681. [Google Scholar] [CrossRef]
- Lu, H.; Chen, L.F.; Chen, Q.; Shen, H.; Liu, Z. A rare large cutaneous chondroid syringoma involving a toe: A case report. Medicine 2018, 97, e9825. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kisova, D.; Dikov, T.; Ivanova, V.; Stoyanov, H.; Yordanova, G. Mixed Eccrine Cutaneous Tumor with Folliculo–Sebaceous Differentiation: Case Report and Literature Review. Medicina 2023, 59, 1465. https://doi.org/10.3390/medicina59081465
Kisova D, Dikov T, Ivanova V, Stoyanov H, Yordanova G. Mixed Eccrine Cutaneous Tumor with Folliculo–Sebaceous Differentiation: Case Report and Literature Review. Medicina. 2023; 59(8):1465. https://doi.org/10.3390/medicina59081465
Chicago/Turabian StyleKisova, Dimitrinka, Tihomir Dikov, Vesela Ivanova, Hristo Stoyanov, and Greta Yordanova. 2023. "Mixed Eccrine Cutaneous Tumor with Folliculo–Sebaceous Differentiation: Case Report and Literature Review" Medicina 59, no. 8: 1465. https://doi.org/10.3390/medicina59081465