
Quality Standard for Rehabilitation of Young Deaf Children Receiving Cochlear Implants
 , ,
, ,  , ,
, ,  , ,
, , {kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Interview Local Experts
- -
- What is your experience in rehabilitation of young deaf children with CI’s learning to speak and to develop spoken language?
- -
- Who (what kind of professionals/parents) should be involved in the rehabilitation process after CI in young deaf children?
- -
- What should be the role for the CI-team and what should we expect from local professionals? So, who is doing what?
- -
- What are important domains to focus on during the rehabilitation of young CI-children?
- -
- Should we involve the parents in the rehabilitation process? If so, Why + How + How often?
- -
- Do you prefer a specific rehabilitation program or approach for therapy? Which resources (books, publications) do you suggest for other therapists to become an expert too?
- -
- Do we have to monitor the listening, speech and spoken language development of these young CI-children? If so. Why and how often?
- -
- What frequency of therapy sessions do you suggest for these young CI-children and their families? How often? For how many minutes? For how many months/years?
2.2. Standards—Bibliographic Context Analysis
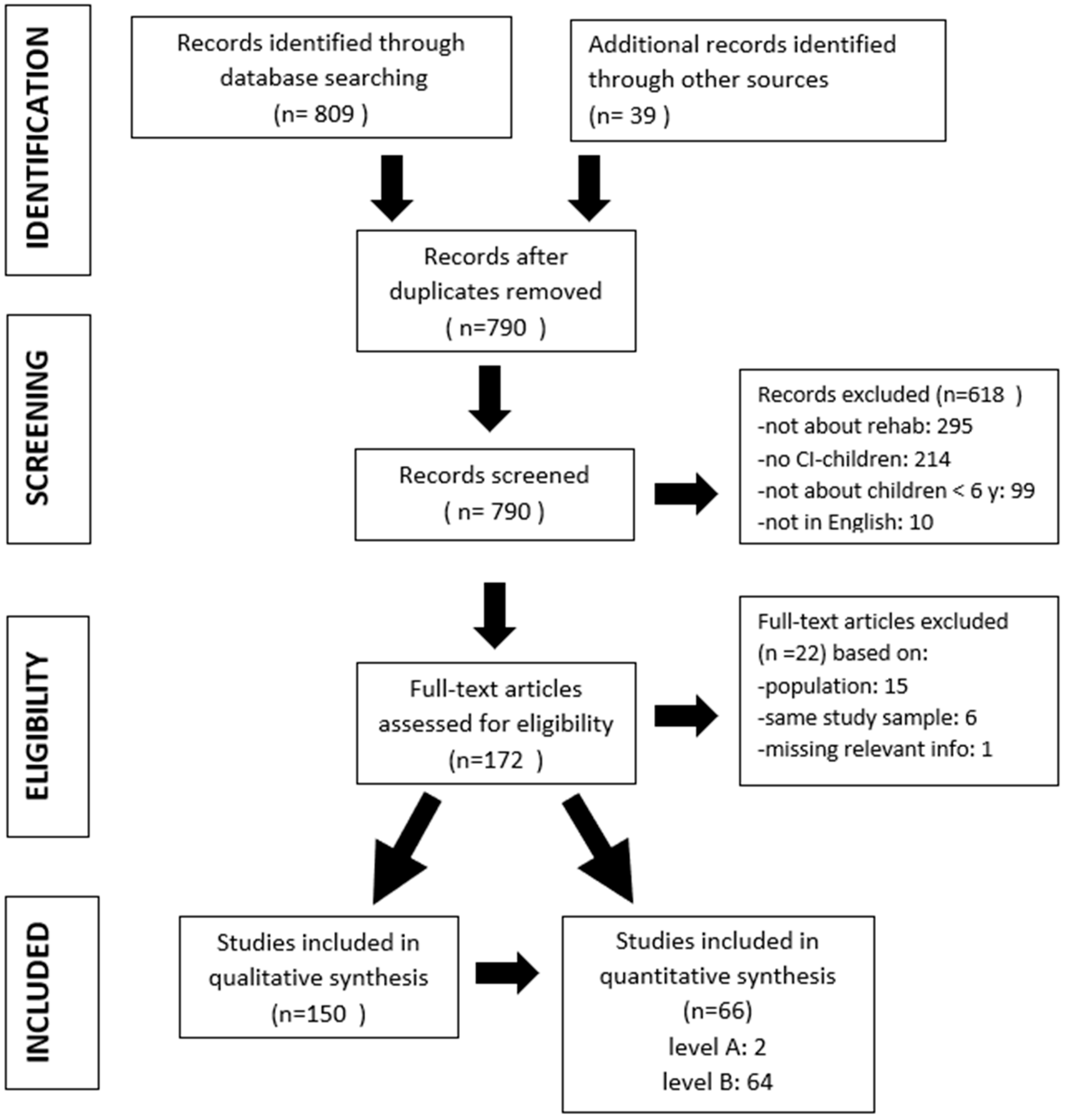
2.2.1. Search Strategy
2.2.2. Level of Evidence
2.3. Quality Standards
3. Results
3.1. Interview Local Experts
3.2. Bibliographic Analysis
3.3. Quality Standards
4. Quality Standard for Rehabilitation of Young Children Receiving CIs (Table S2 from Supplementary Materials)
4.1. General Quality Standards for Pediatric Cochlear Implantation in Relation to Rehabilitation
- ▪
- Providing a Child with a Cochlear Implant Requires a Dedicated Multi-Disciplinary Team Consisting at Minimum of an Otolaryngologist, Audiologist and a SLT Specialist
- -
- Ideally there should also be a psychologist and social worker included in the team.
- -
- The multidisciplinary team should work inter professionally (not next to each other but together) and in close cooperation with the parents/carers.
- -
- The multidisciplinary team will liaise and work with the child’s local support team.
- ▪
- The CI-Team of the Hospital Should Coordinate the Selection, Surgery, Fitting, Rehabilitation and after Care (Equipment Maintenance, Spare Materials)
- ▪
- Parents/Educators/Professionals Need Balanced and Unbiased Up-to-Date Information about CI’s and the Fitting/Rehabilitation Process
- -
- Ideally in their language.
- -
- Parents/educators/professionals should get appropriate counselling from the CI team and other professionals to have appropriate expectations from the cochlear implant, depending on several variables such as age at implantation or additional disabilities.
- -
- Parents/educators/professionals should have the opportunity to meet other families with CI children.
- -
- Parents/educators/professionals also need psychological support: taking care of their emotions and stress.
- ▪
- Rehabilitation should Be Delivered by the CI-Team in Close Cooperation with A Local Expert (Team) in Listening and Spoken Language Development. (See Quality Standard # 29)
- ▪
- Rehabilitation Is Not Possible without Parent/Family/Caregiver Involvement
- -
- In case of parents or legal guardians are not able to be actively engaged in the child’s rehabilitation due to very low Social Economical Status, mental health matters, or cognitive delays, other family members or carers should be involved.
- -
- Professionals should use a child/family cantered approach.
- ▪
- The Cochlear Implant Surgery Should Take Place as Soon as a Child Is Identified as a Candidate and Should Ideally Be Done by the Age of 12 Months or Sooner, Preferably under the Age of 36 Months, without Excluding Those Older Than 37 Months
- ▪
- A Child with Bilateral Deafness Should Be Fitted Bilaterally with CI’s, Preferably before the Age of 18 Months
- -
- We expect all countries to follow the principles and guidelines of the Joint Committee on Infant Hearing to have early hearing screening (before age 1 month), diagnosis (before 3 months) and start with rehabilitation (fitting hearing aids and early intervention) before 6 months of age.
- ▪
- The CI-Team will Issue or Dispatch Replacements for Faulty External Equipment within Two Working Days
- -
- There should be a written policy regarding who is responsible in the event of loss/damage and what spares can be provided as a matter of routine.
- ▪
- Each Child’s Sound Processor Must Be up Graded Every 5 Years
- ▪
- The National CI Program should Conduct and Publish Annual Audits and Comply with the Requirements of the Responsible National Authorities. Audits should Cover All Aspects Related to CI: Clinical Activity, Staff Expertise, Child Outcomes, Surgical Complications, Device Failures, and Child and Family/Caregiver Feedback on the Service Provided
- -
- The audits should become freely available to interested parties.
4.2. Quality Standards on Fitting/Programming in Relation to Rehabilitation
- ▪
- The Fitting of the Sound Processor should Be Carried out by Qualified Paediatric Audiologist Preferably in Clinic, Face-to-Face Rather Than Remotely
- ▪
- There should Be a Liaison between the Audiologist of the CI-Team and the Local Rehabilitation Expert/Local Support Team (and Vice Versa) to Exchange Information about the Progress of the Child’s Auditory Skills
- -
- It is recommended that local professionals receives writen reports on the child’s auditory function
- -
- It is recommended that local professionals received written reports on the child’s auditory performance.
- ▪
- Instructions on the Use of the Sound Processor Must Be Given to the Parent/Caregiver on or before the Day of Activation and should Be Repeated at Least Twice within the Six Months Following Activation
- -
- This is within the role of the audiologist and the rehabilitation therapist.
- -
- Supporting materials on the handling, operating and care of the sound processor should be issued to the parent/carer.
- -
- The recommended use of assistive listening accessories (e.g.,: AudioStream, Mini mic, Roger) should be explained to the parent/carer by the CI team (see Quality standard # 1) before the CI surgery and the information reviewed after the activation.
- ▪
- Appropriate Audiological, Standardized Speech Perception Tests and Functional Hearing Assessment (by Family/Other Professionals’ Questionnaire) should Be Performed at 6 Months Intervals to Enable Hearing to Be Monitored
- -
- It is recommended to assess speech perception with standardized tests and a functional hearing questionnaire. Ideally: every 6 months in the first 2 years after the cochlear implant activation and then every year minimum of once a year.
- -
- Measuring speech perception of soft speech and speech in noise should begin after two years of CI use.
- -
- The results should be shared with the child’s parents/educators and local professionals.
4.3. Quality Standards on Rehabilitation of Young Children Receiving CI’s
- ▪
- Rehabilitation should Begin before Implantation and at the Latest Immediately after Initial Fitting, According to the Individual Needs of the Child
- -
- Even if rehabilitation does not start until initial fitting, written material about the content of rehabilitation should be shared with the parent/carer well before initial fitting, so that they have a good idea of what is needed to promote an appropriate child’s listening and spoken language development.
- ▪
- Parents/Educators/Professionals Are Considered and Valued as Equal Partners in the Rehabilitation Process of Their Child
- -
- Parents/educators/professionals must have equal access to information on CI in their preferred language.
- -
- CI companies should make their brochures available in the preferred language of the parents/caregivers.
- ▪
- Appropriate Measures should Be Performed Yearly (Ideally Every 6 Months) to Monitor Progress in Language, Communicational and Educational Outcomes the First 3 Years after Implantation
- -
- Standardized assessments for typical hearing children should be used for comparisons.
- -
- Additional rehabilitation and/or referrals should take place where progress is slower than expected.
- ▪
- A Diagnostic Coaching Approach to CI Rehabilitation Yields the Most Efficient and Best Benefit, Both to Children and to Parents/Educators/Professionals
- -
- Additional needs should be identified as soon as possible, so rehabilitation and expectations can be adapted to the special needs. Additional specialists in other fields can be incorporated into the team to share their expertise.
- ▪
- The Audiologist and Speech and Language Therapist Together with the Parents should Decide on the Frequency of Specialist Contact Sessions for Fitting and for Rehabilitation Based on the Individual Needs of the Child and Their Family
- ▪
- As the Recommended Approach of Services Is Family-Centered, It Is Understood That Rehabilitation Therapy Sessions can Take Place Weekly or Fortnightly, Considering That Most Listening and Spoken Language Experience Will Occur at Home between the Sessions
- ▪
- Children with CI’s should have Annually the Opportunity to Trial and Assess Assistive Listening Devices (FM-Systems, Bluetooth Accessories)
- ▪
- Rehabilitation of Young CI-Children should Involve Collaboration between the CI Centre, Local Professionals, and Parents/Educators to Cover the Following Areas:
- -
- Listening skills/functional listening/speech perception.
- -
- Speech intelligibility, voice quality and prosody.
- -
- Communication skills including repair strategies.
- -
- All aspects of language development.
- -
- Theory of Mind development.
- -
- Ability to troubleshoot and maintain external equipment.
- -
- Using assistive listening devices.
- -
- Music.
- -
- Literacy (reading).
- -
- Cognitive skills (Executive Functions).
- -
- Mainstream education (inclusion).
- -
- Advocacy.
- ▪
- It Is Recommended That All Children to Receive, Based on Their Need, Listening and Spoken Language Therapy after Implantation, Even Those Who Benefit Little from CI and Who Are Anticipated to Still Be Sign Reliant
- -
- Among all auditory-based early intervention approaches for children receiving CI, evidence-based practice has proven that an approach focusing on listening and spoken language has the most impact on the child’s speech perception skills and expressive spoken language development.
- -
- The decision to add signed support or sign language in the rehabilitation therapy will be discussed among parents and professionals so parents can make an informed decision.
- ▪
- Rehabilitation Therapists and Parents/Educators will Collaboratively Generate Measurable and Appropriate Goals in All Areas of the Child’s Development (Auditory, Receptive, and Expressive Language, Speech, Cognition, and Social Skills), and Identify Ways to Integrate the Goals and Strategies to Achieve them in a Nurturing and Rich Language
- ▪
- Music should Be Integrated in the Rehabilitation of Young Children Using CI’s, Particularly as a Home-Based Fun Activity Rather Than in a Formal Setting
4.4. Quality Standards for Professionals in Relation to Rehabilitation
- ▪
- Every Country should Have Training Opportunities for Professionals in the Various Communication Approaches (From Auditory Verbal to Sign Bilingualism) to Become An Expert in the Field of Rehabilitation and Education of CI-Children
- ▪
- The Staff of the CI Team in the Hospital and Local Rehabilitation Therapists should Have the Knowledge and Expertise That Enables Them to Work Effectively with Children Wearing CI’s, Including Those with Additional Needs Than Their Hearing Loss
- -
- Some very complex children may need a very specialized service.
- ▪
- Rehabilitation of Young CI-Children should Be Carried out by An Expert in Promoting Listening, Speech and Spoken Language Development, in Managing the Technology and the Environment
- -
- The therapist should also have expertise in coaching and counselling parents.
- -
- The therapist should also have expertise in a family-centered approach.
- ▪
- The Expertise of the Rehabilitation Therapist/Rehabilitation Team should Include the Following Skills:
- -
- Expertise and skills working with infants and very young children (for pediatric services).
- -
- Expertise in auditory development and listening skills.
- -
- Knowledge on how to manage the technology.
- -
- Knowledge on how to manage the acoustics of the environment and on how to address challenging listening situations (e.g., assistive listening devices).
- -
- Gain insight into the impact of hearing loss on a child’s overall development (eg mental health, language, speech, cognition, social and literacy) and how to support these skills.
- -
- Knowledge of communication support teams, i.e., speech to text or sign language interpreters.
- -
- Knowledge of audiology and assistive listening technology.
- -
- To get to know the culture and language of the deaf community.
- -
- Knowledge on how to coach/guide families.
- -
- Knowledge on inclusion of a CI-child (in education and in the local environment).
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix B
References
- Moeller, M.P. Early intervention and language development in children who are deaf and hard of hearing. Pediatrics 2000, 106, E43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshinaga-Itano, C.; Sedey, A. Language, Speech and Social–Emotional Development of Children Who are Deaf or Hard of Hearing: The Early Years. Volta Rev. 2000, 100, 286–295. [Google Scholar]
- Yoshinago-Itano, C. Early Identification, Communication Modality, and the Development of Speech an Spoken Language: Patterns and Considerations. In Advances in the Spoken Language Development of Deaf and Hard-of-Hearing Children; Spencer, P., Marschark, M., Eds.; Oxford University Press: New York, NJ, USA, 2006; pp. 298–327. [Google Scholar]
- Watkin, P.; McCann, D.; Law, C.; Mullee, M.; Petrou, S.; Stevenso, J.; Worsfold, S.; Yuen, H.M.; Kennedy, C. Language ability in children with permanent hearing impairment: The influence of early management and family participation. Pediatrics 2007, 120, e694–e701. [Google Scholar] [CrossRef] [PubMed]
- Verhaert, N.; Willems, M.; Van Kerschaver, E.; Desloovere, C. Impact of early hearing screening and treatment on language development and education level: Evaluation of 6 years of universal newborn hearing screening (ALGO) in Flanders, Belgium. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 599–608. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Hearing; Licence: CC, BY-NC-SA 3.0 IGO: Geneva, Switzerland, 2021. [Google Scholar]
- De Raeve, L. Auditory Rehabilitation Therapy Guidelines for optimizing the benefits of Binaural Hearing, a Cochlear white paper. Basel Cochlear Eur. 2008, 1–8. [Google Scholar]
- Kirk, K.; Miyamoto, R.; Ying, E.; Perdew, A.; Zuganelis, H. Cochlear Implantation in Young Children: Effect of Age of Implanta-tion and Communication Mode. Volta Rev. 2000, 102, 127–144. [Google Scholar]
- De Raeve, L. A longitudinal study on auditory perception and speech intelligibility in deaf children implanted under the age of 18 months, in comparison to those implanted at later ages. Otol. Neurotol. 2010, 31, 1261–1267. [Google Scholar] [CrossRef]
- Svirsky, M.A.; Teoh, S.W.; Neuburger, H. Development of language and speech perception in congenitally, profoundly deaf children as a function of age at cochlear implantation. Audiol. Neurootol. 2004, 9, 224–233. [Google Scholar] [CrossRef]
- Schauwers, K.; Gillis, S.; Govaerts, P. Language acquisition in child-ren with a cochlear implant. In Trends in Language Acquisition Research 4: Developmental Theory and Language Disorders; Fletcher, P., Miller, J., Eds.; John Benjamins Press: Amsterdam, The Netherlands, 2005; pp. 324–329. [Google Scholar]
- Vermeulen, A.; van Bon, W.; Schreuder, R.; Knoors, H.; Snik, A. Reading skills of deaf children with CI’s. J. Deaf. Stud. Deaf. Educ. 2007, 12, 283–302. [Google Scholar] [CrossRef]
- Anderson, I.; Weichbold, V.; D’Haese, P.; Szuchnik, J.; Quevedo, M.; Martin, J.; Dieler, W.S.; Phillips, L. Cochlear implantation in children under the age of two—What do the outcomes show us? Int. J. Pediatr. Otorhinolaryngol. 2004, 68, 425–431. [Google Scholar] [CrossRef]
- Miyamoto, R.T.; Houston, D.M.; Kirk, K.I.; Perdew, A.E.; Svirsky, M.A. Language development in deaf infants following cochlear implantation. Acta Otolaryngol. 2003, 123, 241–244. [Google Scholar] [CrossRef]
- Spencer, L.; Barker, B.; Tomblin, J. Exploring the language and literacy outcomes of pediatric cochlear implant users. Ear Hear. 2003, 24, 236–247. [Google Scholar] [CrossRef] [Green Version]
- Tomblin, J.; Barker, B.; Hubbs, S. Developmental constraints on language development in children with CI’s. Int. J. Audiol. 2007, 46, 512–523. [Google Scholar] [CrossRef]
- Zwolan, T.A.; Ashbaugh, C.M.; Alarfaj, A.; Kileny, P.R.; Arts, H.A.; El-Kashlan, H.K.; Telian, S.A. Pediatric cochlear implant patient performance as a function of age at implantation. Otol. Neurotol. 2004, 25, 112–120. [Google Scholar] [CrossRef]
- Percy-Smith, L.; Busch, G.W.; Sandahl, M.; Nissen, L.; Josvassen, J.L.; Bille, M.; Lange, T.; Cayé-Thomasen, P. Significant regional differences in Denmark in outcome after cochlear implants in children. Dan. Med. J. 2012, 59, A4435. [Google Scholar]
- Dyrberg, S. The Auditory Verbal Therapy (AVT) program—Evaluation of the 3-year AVT-program 2017–2021. EURO-CIU Newsl. 2022, 11–12. Available online: https://decibel.dk/files/media/document/Final2_Evalrapport_V.3.2_CalibriLight%20copy.pdf (accessed on 25 February 2023).
- Dettman, S.; Pinder, D.; Briggs, R.; Dowell, R.; Leigh, J. Communication development in children who receive the cochlear implant younger than 12 months: Risks versus benefits. Ear Hear. 2007, 28, 11S–18S. [Google Scholar] [CrossRef]
- Archbold, S.; Mayer, C. Deaf Education: The impact of cochlear implantation. Deaf. Educ. Int. 2012, 14, 2–15. [Google Scholar] [CrossRef]
- Boons, T.; Brokx, J.P.; Frijns, J.H.; Peeraer, L.; Philips, B.; Vermeulen, A.; Wouters, J.; van Wieringen, A. Effect of pediatric bilateral cochlear implantation on language development. Arch. Pediatr. Adolesc. Med. 2012, 166, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Joint Committee on Infant Hearing. Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs. J. Early Hear. Detect. Interv. 2019, 4, 1–44. [Google Scholar]
- Demers, D.; Bergeron, F. Effectiveness of rehabilitation approaches proposed to children with severe-to-profound prelinguistic deafness on the development of auditory, speech and language skills: A systematic review. J. Speech Lang. Hear. Res. 2019, 62, 4196–4230. [Google Scholar] [CrossRef]
- World Health Organization. 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/rehabilitation. (accessed on 17 February 2023).
- New York State Speech, Language and Hearing Association. 2012, adapted from Fed. Reg. 52530; NAIC Glossary of Health Insurance and Medical Terms: 3. Available online: https://content.naic.org/sites/default/files/inline-files/committees_b_consumer_information_ppaca_glossary.pdf (accessed on 20 February 2023).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lebwohl, M.; Heymann, W.R.; Berth-Jones, J.; Coulson, I. Treatment of Skin Disease—Comprehensive Therapeutic Strategies, 3rd ed.; Saunders-Elsevier: New York, NY, USA, 2010. [Google Scholar]
- Monshizadeh, L.; Vameghi, R.; Rahimi, M.; Sajedi, F.; Yadegari, F.; Hashemi, S.B. The effectiveness of a specifically-designed language intervention protocol on the cochlear implanted children’s communication development. Int. J. Pediatr. Otorhinolaryngol. 2019, 126, 109631. [Google Scholar] [CrossRef]
- Qiao, X.F.; Ren, Q.; Li, X.; Li, T.L.; Mariano, R.S. Analysis of subjective perception and influencing factors of different inclusive education models among prelingually deaf children with a cochlear implant. J. Int. Med. Res. 2020, 48, 300060520929855. [Google Scholar] [CrossRef]
- Hyde, M.L. Newborn hearing screening programs: Overview. J. Otolaryngol. 2005, 34, S70–S78. [Google Scholar]
- Fitzpatrick, E.M.; Hamel, C.; Stevens, A.; Pratt, M.; Moher, D.; Doucet, S.P.; Na, E. Sign language and spoken language for children with hearing loss: A systematic review. Pediatrics 2016, 137, e20151974. [Google Scholar] [CrossRef] [Green Version]
- Kaipa, R.; Danser, M.L. Efficacy of auditory–verbal therapy in children with hearing impairment: A systematic review from 1993 to 2015. Int. J. Pediatr. Otorhinolaryngol. 2016, 86, 124–134. [Google Scholar] [CrossRef]
- Rosenfeld, R.M.; Nnacheta, L.C.; Corrigan, M.D. Clinical Consensus Statement Development Manual. Otolaryngol. Head Neck Surg. 2015, 153, S1–S14. [Google Scholar] [CrossRef] [Green Version]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Raeve, L.; Cumpăt, M.-C.; van Loo, A.; Costa, I.M.; Matos, M.A.; Dias, J.C.; Mârțu, C.; Cavaleriu, B.; Gherguț, A.; Maftei, A.; et al. Quality Standard for Rehabilitation of Young Deaf Children Receiving Cochlear Implants. Medicina 2023, 59, 1354. https://doi.org/10.3390/medicina59071354
De Raeve L, Cumpăt M-C, van Loo A, Costa IM, Matos MA, Dias JC, Mârțu C, Cavaleriu B, Gherguț A, Maftei A, et al. Quality Standard for Rehabilitation of Young Deaf Children Receiving Cochlear Implants. Medicina. 2023; 59(7):1354. https://doi.org/10.3390/medicina59071354
Chicago/Turabian StyleDe Raeve, Leo, Marinela-Carmen Cumpăt, Aimée van Loo, Isabel Monteiro Costa, Maria Assunção Matos, João Canossa Dias, Cristian Mârțu, Bogdan Cavaleriu, Alois Gherguț, Alexandra Maftei, and et al. 2023. "Quality Standard for Rehabilitation of Young Deaf Children Receiving Cochlear Implants" Medicina 59, no. 7: 1354. https://doi.org/10.3390/medicina59071354