
Updated Meta-Analysis of Randomized Controlled Trials Comparing External Fixation to Intramedullary Nailing in the Treatment of Open Tibial Fractures
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Selection
2.2. Search Strategy
2.3. Data Abstraction and Quality Assessment
2.4. Risk of Bias
2.5. Data Analysis
3. Results
3.1. Search Results
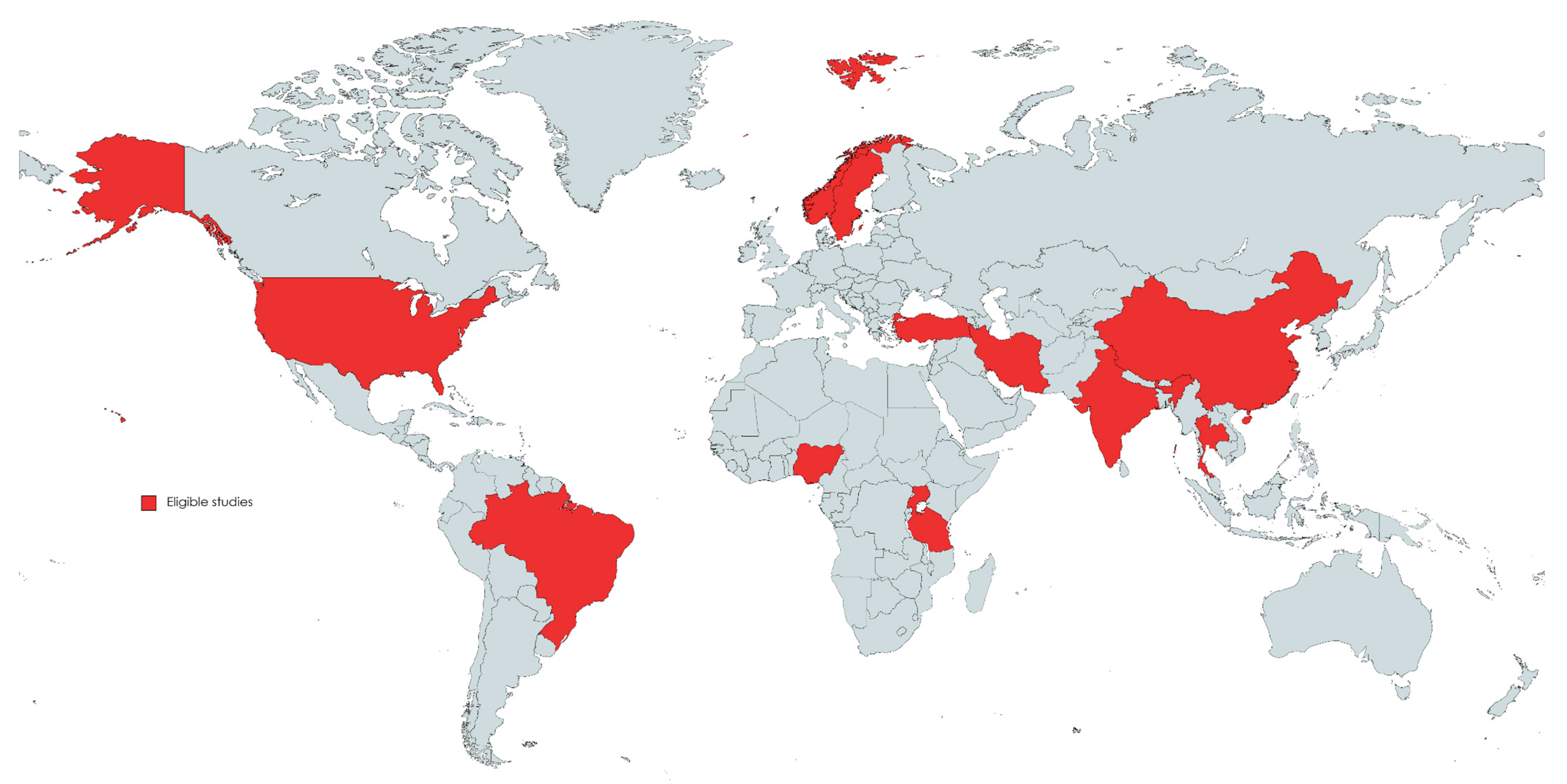
3.2. Characteristics of Eligible Studies
3.3. Quality Assessment of the Eligible Studies
4. Results of Meta-Analysis
4.1. Postoperative Superficial Infection
4.2. Postoperative Deep Infection
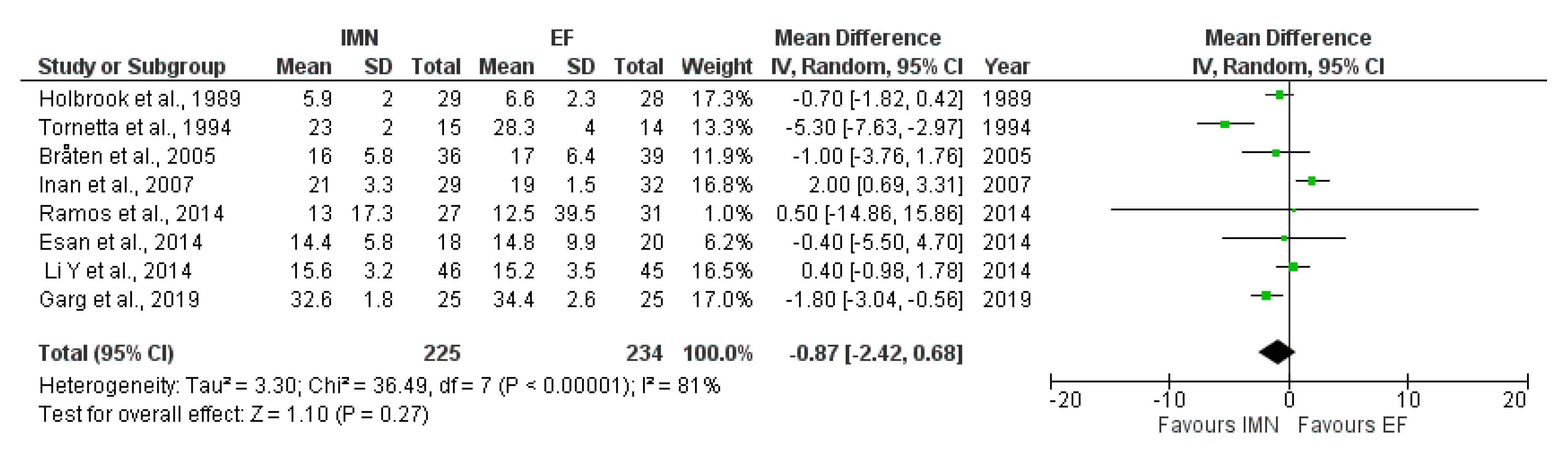
4.3. Time to Union
4.4. Delayed union
4.5. Malunion
4.6. Nonunion
4.7. Hardware Failure
4.8. Pain
4.9. Health-Related Quality of Life Measured after 3 Months
4.10. Health-Related Quality of Life Measured after 12 Months
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Court-Brown, C.M.; Rimmer, S.; Prakash, U.; McQueen, M.M. The epidemiology of open long bone fractures. Injury 1998, 29, 529–534. [Google Scholar] [CrossRef]
- Weiss, R.J.; Montgomery, S.M.; Ehlin, A.; Al Dabbagh, Z.; Stark, A.; Jansson, K.A. Decreasing incidence of tibial shaft fractures between 1998 and 2004, information based on 10,627 Swedish inpatients. Acta Orthop. 2008, 79, 526–533. [Google Scholar] [CrossRef]
- Okike, K. Current concepts review: Trends in the management of open fractures. J. Bone Jt. Surg. A 2006, 88, 2739–2747. [Google Scholar] [CrossRef]
- Elniel, A.R.; Giannoudis, P.V. Open fractures of the lower extremity: Current management and clinical outcomes. EFORT Open Rev. 2018, 3, 316–325. [Google Scholar] [CrossRef] [PubMed]
- Zalavras, C.G.; Patzakis, M.J. Open fractures: Evaluation and management. JAAOSJ Am. Acad. Orthopaed. Surg. 2003, 11, 212–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foote, C.J.; Guyatt, G.H.; Vignesh, K.N.; Mundi, R.; Chaudhry, H.; Heels-Ansdell, D.; Thabane, L.; Tornetta, P., 3rd; Bhandari, M. Which Surgical Treatment for Open Tibial Shaft Fractures Results in the Fewest Reoperations? A Network Meta-analysis. Clin. Orthop. Relat. Res. 2015, 473, 2179–2192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosny, G.; Fadel, M. Ilizarov external fixator for open fractures of the tibial shaft. Int. Orthop. 2003, 27, 303–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inan, M.; Halici, M.; Ayan, I.; Tuncel, M.; Karaoglu, S. Treatment of type IIIA open fractures of tibial shaft with Ilizarov external fixator versus unreamed tibial nailing. Arch. Orthop. Trauma Surg. 2007, 127, 617–623. [Google Scholar] [CrossRef]
- Court-Brown, C.M.; Wheelwrigh, E.F.; Christie, J.; McQueen, M.M. External fixation for type III open tibial fractures. J. Bone Jt. Surg. Br. 1990, 72, 801–804. [Google Scholar] [CrossRef] [Green Version]
- Whitelaw, G.P.; Cimino, W.G.; Segal, D. The treatment of open tibial fractures using nonreamed fexible intramedullary fixation. Orthop. Rev. 1990, 19, 244–256. [Google Scholar]
- Greco, T.; Vitiello, R.; Cazzato, G.; Cianni, L.; Malerba, G.; Maccauro, G.; Perisano, C. Intramedullary antibiotic coated nail in tibial fracture: A systematic review. J. Biol. Regul. Homeost. Agents 2020, 34, 63–69. [Google Scholar] [PubMed]
- Rohde, C.; Greives, M.R.; Cetrulo, C.; Lerman, O.Z.; Levine, J.P.; Hazen, A. Gustilo grade IIIB tibial fractures requiring microvascular free faps: External fxation versus intramedullary rod fixation. Ann. Plast. Surg. 2007, 59, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Fu, Q.; Zhu, L.; Lu, J.; Ma, J.; Chen, A. External fixation versus unreamed tibial intramedullary nailing for open tibial fractures: A meta-analysis of randomized controlled trials. Sci. Rep. 2018, 8, 12753. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Li, X.; Liu, L.; Wu, W. A meta-analysis of external fixator versus intramedullary nails for open tibial fracture fixation. J. Orthop. Surg. Res. 2014, 9, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, F.; Zhu, Y.; Li, W.; Chen, W.; Tian, Y.; Zhang, Y. Unreamed Intramedullary Nailing is a better alternative than External Fixator for Gustilo grade IIIB Tibial Fractures based on a meta-analysis. Scand. J. Surg. 2016, 105, 117–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Xie, L.; Liu, L.; Gao, G.; Zhou, P.; Chu, D.; Qiu, D.; Tao, J. Comparing external fixators and intramedullary nailing for treating open tibia fractures: A meta-analysis of randomized controlled trials. J. Orthop. Surg. Res. 2023, 18, 13. [Google Scholar] [CrossRef]
- Fang, X.; Jiang, L.; Wang, Y.; Zhao, L. Treatment of Gustilo grade III tibial fractures with unreamed intramedullary nailing versus external fxator: A meta-analysis. Med. Sci. Monit. 2012, 18, RA49–RA56. [Google Scholar] [CrossRef] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2, a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A.C. Chapter 8, Assessing risk of bias in a randomized trial. In Handbook for Systematic Reviews of Interventions Version 6.3, updated February 2022, 2nd ed.; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; John Wiley & Sons: Chichester, UK, 2019; Available online: www.training.cochrane.org/handbook (accessed on 5 January 2023).
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Tornetta, P., 3rd; Bergman, M.; Watnik, N.; Berkowitz, G.; Steuer, J. Treatment of grade-IIIb open tibial fractures: A prospective randomised comparison of external fixation and non-reamed locked nailing. J. Bone Jt. Surg. Br. 1994, 76, 13–19. [Google Scholar] [CrossRef]
- Haonga, B.T.; Liu, M.; Albright, P.; Challa, S.T.; Ali, S.H.; Lazar, A.A.; Eliezer, E.N.; Shearer, D.W.; Morshed, S. Intramedullary Nailing Versus External Fixation in the Treatment of Open Tibial Fractures in Tanzania: Results of a Randomized Clinical Trial. J. Bone Jt. Surg. Am. 2020, 102, 896–905. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, J.L.; Swiontkowski, M.F.; Sanders, R. Treatment of open fractures of the tibial shaft: Ender nailing versus external fixation: A randomized, prospective comparison. J. Bone Jt. Surg. Am. 1989, 71, 1231–1238. [Google Scholar] [CrossRef]
- Rohilla, R.; Arora, S.; Kundu, A.; Singh, R.; Govil, V.; Khokhar, A. Functional and radiological outcomes of primary ring fixator versus antibiotic nail in open tibial diaphyseal fractures: A prospective study. Injury 2022, 53, 3464–3470. [Google Scholar] [CrossRef] [PubMed]
- Kisitu, D.K.; O’Hara, N.N.; Slobogean, G.P.; Howe, A.L.; Blachut, P.A.; O’Brien, P.J.; Stockton, D.J. Unreamed Intramedullary Nailing Versus External Fixation for the Treatment of Open Tibial Shaft Fractures in Uganda: A Randomized Clinical Trial. J. Orthop. Trauma 2022, 36, 349–357. [Google Scholar] [CrossRef]
- Ramos, T.; Eriksson, B.I.; Karlsson, J.; Nistor, L. Ilizarov external fixation or locked intramedullary nailing in diaphyseal tibial fractures: A randomized, prospective study of 58 consecutive patients. Arch. Orthop. Trauma Surg. 2014, 134, 793–802. [Google Scholar] [CrossRef]
- Li, Y.; Jiang, X.; Guo, Q.; Zhu, L.; Ye, T.; Chen, A. Treatment of distal tibial shaft fractures by three different surgical methods: A randomized, prospective study. Int. Orthop. 2014, 38, 1261–1267. [Google Scholar] [CrossRef] [Green Version]
- Garg, S.; Khanna, V.; Goyal, M.P.; Joshi, N. Unreamed Intra-Medullary Nail Versus Half Pin External Fixator in Grade III [A & B] Open tibia fractures. J. Clin. Orthop. Trauma 2019, 10, 941–948. [Google Scholar]
- Mohseni, M.A.; Soleimanpour, J.; Mohammadpour, H.; Shahsavari, A. AO tubular external fixation vs. unreamed intramedullary nailing in open grade IIIA-IIIB tibial shaft fractures: A single-center randomized clinical trial. Pak. J. Biol. Sci. 2011, 14, 490–495. [Google Scholar] [CrossRef] [Green Version]
- Bråten, M.; Helland, P.; Grøntvedt, T.; Aamodt, A.; Benum, P.; Mølster, A. External fixation versus locked intramedullary nailing in tibial shaft fractures: A prospective, randomised study of 78 patients. Arch. Orthop. Trauma Surg. 2005, 125, 21–26. [Google Scholar] [CrossRef]
- Henley, M.B.; Chapman, J.R.; Agel, J.; Harvey, E.J.; Whorton, A.M.; Swiontkowski, M.F. Treatment of type II, IIIA, and IIIB open fractures of the tibial shaft: A prospective comparison of unreamed interlocking intramedullary nails and half-pin external fixators. J. Orthop. Trauma 1998, 12, 1–7. [Google Scholar] [CrossRef]
- Tu, Y.K.; Lin, C.H.; Su, J.I.; Hsu, D.T.; Chen, R.J. Unreamed interlocking nail versus external fixator for open type III tibia fractures. J. Trauma 1995, 39, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, F.L.; de Abreu, L.C.; Valenti, V.E.; Valente, A.L.; da Costa Pereira Cestari, R.; Pohl, P.H.; Rodrigues, L.M. Bone tissue repair in patients with open diaphyseal tibial fracture treated with biplanar external fixation or reamed locked intramedullary nailing. Injury 2014, 45 (Suppl. S5), S32–S35. [Google Scholar] [CrossRef] [PubMed]
- Frihagen, F.; Madsen, J.E.; Sundfeldt, M.; Flugsrud, G.B.; Andreassen, J.S.; Andersen, M.R.; Andreassen, G.S. Taylor Spatial Frame or Reamed Intramedullary Nailing for Closed Fractures of the Tibial Shaft: A Randomized Controlled Trial. J. Orthop. Trauma 2020, 34, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Esan, O.; Ikem, I.C.; Oginni, L.M.; Esan, O.T. Comparison of unreamed interlocking nail and external fixation in open tibia shaft fracture management. West Afr. J. Med. 2014, 33, 16–20. [Google Scholar]
- Melvin, J.S.; Dombroski, D.G.; Torbert, J.T.; Kovach, S.J.; Esterhai, J.L.; Mehta, S. Open tibial shaft fractures: II. Definitive management and limb salvage. J. Am. Acad. Orthop. Surg. 2010, 18, 108–117. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Available online: http://www.prisma-statement.org/ (accessed on 6 July 2023).














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Country | No. of Patients | Gender (Male/Female) | Age (Yrs), Mean ± Sd | Follow Up (Month), Mean ± Sd | GA | Type | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IMN | EF | IMN | EF | IMN | EF | IMN | EF | IMN | EF | ||||
| Holbrook et al. [25] | 1989 | USA | 29 | 28 | NA | NA | 28 (15–66) ꭝ | 25 (7–65) ꭝ | 16.8 (14–21) ꭝ | 18.5 (12–24) ꭝ | I, II, III | Ender | Half-pin |
| Rohilla et al. [26] | 2022 | India | 16 | 16 | 13/3 | 13/3 | 33.1 ± 11.2 | 31.1 ± 9.7 | 24.1 | 23.3 | II, III | Antibiotic, interlocking | Standard ring frame |
| Kisitu et al. [27] | 2022 | Uganda | 31 | 24 | 21/10 | 16/8 | 39 ± 11 | 39 ± 13 | 12 | 4.5 | II, IIIa | Unreamed | NA |
| Haonga et al. [24] | 2020 | Tanzania | 111 | 110 | 98/13 | 91/19 | 33.3 ± 11.8 | 31.8 ± 9.5 | 12 | 12 | I, II, IIIa | Hand-reamed, interlocking (SIGN) | AO uniplanar DISPOFIX |
| Ramos et al. [28] | 2014 | Sweden | 27 | 31 | 19/8 | 22/9 | 38 (19–70) ꭝ | 46 (18–71) ꭝ | 12 | 12 | I, II; | Reamed, locked. cannulated (Syntes) | Original Ilizarov design |
| Inan et al. [8] | 2007 | Turkey | 29 | 32 | 24/5 | 28/4 | 31.7 (17–54) ꭝ | 32.3 (15–64) ꭝ | 43.3 (30–61) ꭝ | 46.5 (33–67) ꭝ | IIIa | Unreamed | Hybrid Ilizarov |
| Li Y et al. [29] | 2014 | China | 46 | 45 | 41/5 | 37/8 | 44 (18–78) ꭝ | 43 (20–82) ꭝ | 14.6 (13–17) ꭝ | 14.6 (12–17) ꭝ | I, II | Reamed and static locking | Combined with limited open reduction and absorbable internal fixation |
| Garg et al. [30] | 2019 | India | 25 | 25 | 18/7 | 19/6 | Mean: 40.4 | Mean: 38.8 | 36 weeks * | IIIa, IIIb | Unreamed | Half-pin | |
| Mohseni et al. [31] | 2011 | Iran | 25 | 25 | 20/5 | 22/3 | 30.8 ± 5.2 | 28.9 ± 8.9 | 12 | 12 | IIIa, IIIb | Unreamed | AO tubular external fixation |
| Braten et al. [32] | 2005 | Norway | 36 | 39 | NA | NA | 43 (16–90) ꭝ | 41 (16–83) ꭝ | I, II | Grosse-Kempf reamed | Ex-fi-re device | ||
| Henley et al. [33] | 1998 | USA | 104 | 70 | 79/21 | 53/15 | 33 (14–81) ꭝ | 33 (16–77) ꭝ | 472 days | 529 days | II, IIIa, IIIb | Unreamed interlocking | Half-pin |
| Tu et al. [34] | 1995 | Taiwan | 18 | 18 | 30/6 * | 38.5 (16–65) *ꭝ | 20.5 (18–24) * | IIIa, IIIb | Unreamed interlocking | Hoffmann skeletal fixation | |||
| Tornetta et al. [23] | 1994 | USA | 15 | 14 | 11/4 | 9/5 | 41 (21–73) ꭝ | 37 (19–86) ꭝ | 21 (19–36) *ꭝ | IIIb | Non reamed, statically locked (Gross-Kempf, Alta, AO) | Hoffmann anterior and ACE multiplane | |
| Rodrigues et al. [35] | 2014 | Brazil | 26 | 31 | 24/2 | 28/3 | 30.5 ± 2 | 30.3 ± 2.2 | 12 | 12 | I, II, IIIa | Reamed | Biplanar |
| Frihagen et al. [36] | 2020 | Norway | 32 | 31 | 22/10 | 20/11 | 41.8 ± 14.7 | 43.4 ± 13.5 | 24 | 24 | 42 A-B ﮺ | Reamed, locked | TSF ring |
| Esan et al. [37] | 2014 | Nigeria | 20 | 20 | 17/3 | 16/4 | 38.1 ± 16.3 | 40.7 ± 17.1 | 24 | 24 | II, IIIa | Interlocking (SIGN) | AO/ASIF and Orthofix |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeremić, D.; Rajovic, N.; Gluscevic, B.; Krivokapic, B.; Rajkovic, S.; Bogosavljevic, N.; Davidovic, K.; Tomic, S. Updated Meta-Analysis of Randomized Controlled Trials Comparing External Fixation to Intramedullary Nailing in the Treatment of Open Tibial Fractures. Medicina 2023, 59, 1301. https://doi.org/10.3390/medicina59071301
Jeremić D, Rajovic N, Gluscevic B, Krivokapic B, Rajkovic S, Bogosavljevic N, Davidovic K, Tomic S. Updated Meta-Analysis of Randomized Controlled Trials Comparing External Fixation to Intramedullary Nailing in the Treatment of Open Tibial Fractures. Medicina. 2023; 59(7):1301. https://doi.org/10.3390/medicina59071301
Chicago/Turabian StyleJeremić, Danilo, Nina Rajovic, Boris Gluscevic, Branislav Krivokapic, Stanislav Rajkovic, Nikola Bogosavljevic, Kristina Davidovic, and Slavko Tomic. 2023. "Updated Meta-Analysis of Randomized Controlled Trials Comparing External Fixation to Intramedullary Nailing in the Treatment of Open Tibial Fractures" Medicina 59, no. 7: 1301. https://doi.org/10.3390/medicina59071301