
Fungal Infections Identified with Multiplex PCR in Severe COVID-19 Patients during Six Pandemic Waves
 , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Patients’ Inclusion and Exclusion Criteria
2.3. Study Materials and Variables
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Disease Management and Outcomes
3.3. Identification of Fungal Species and Drug Resistance
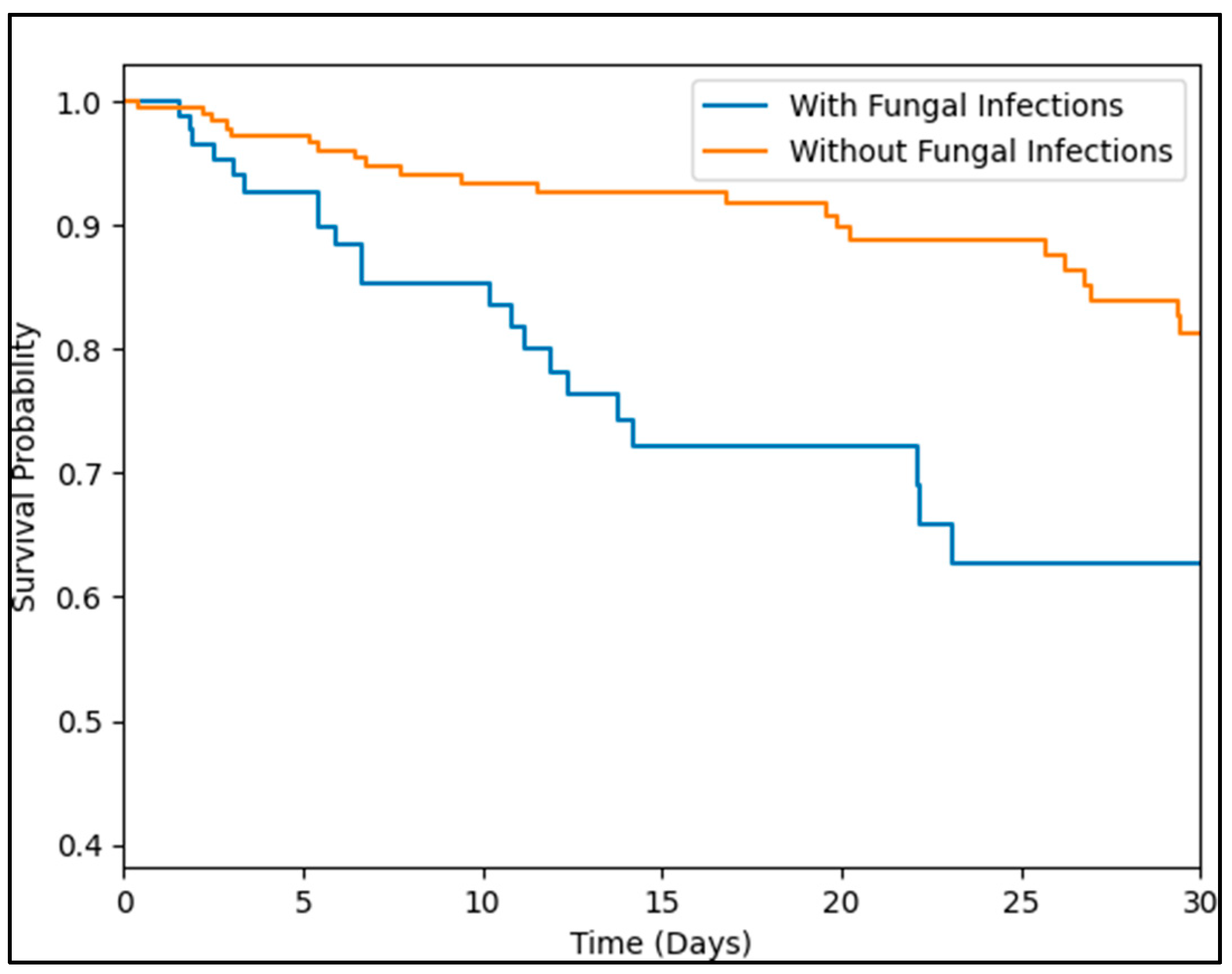
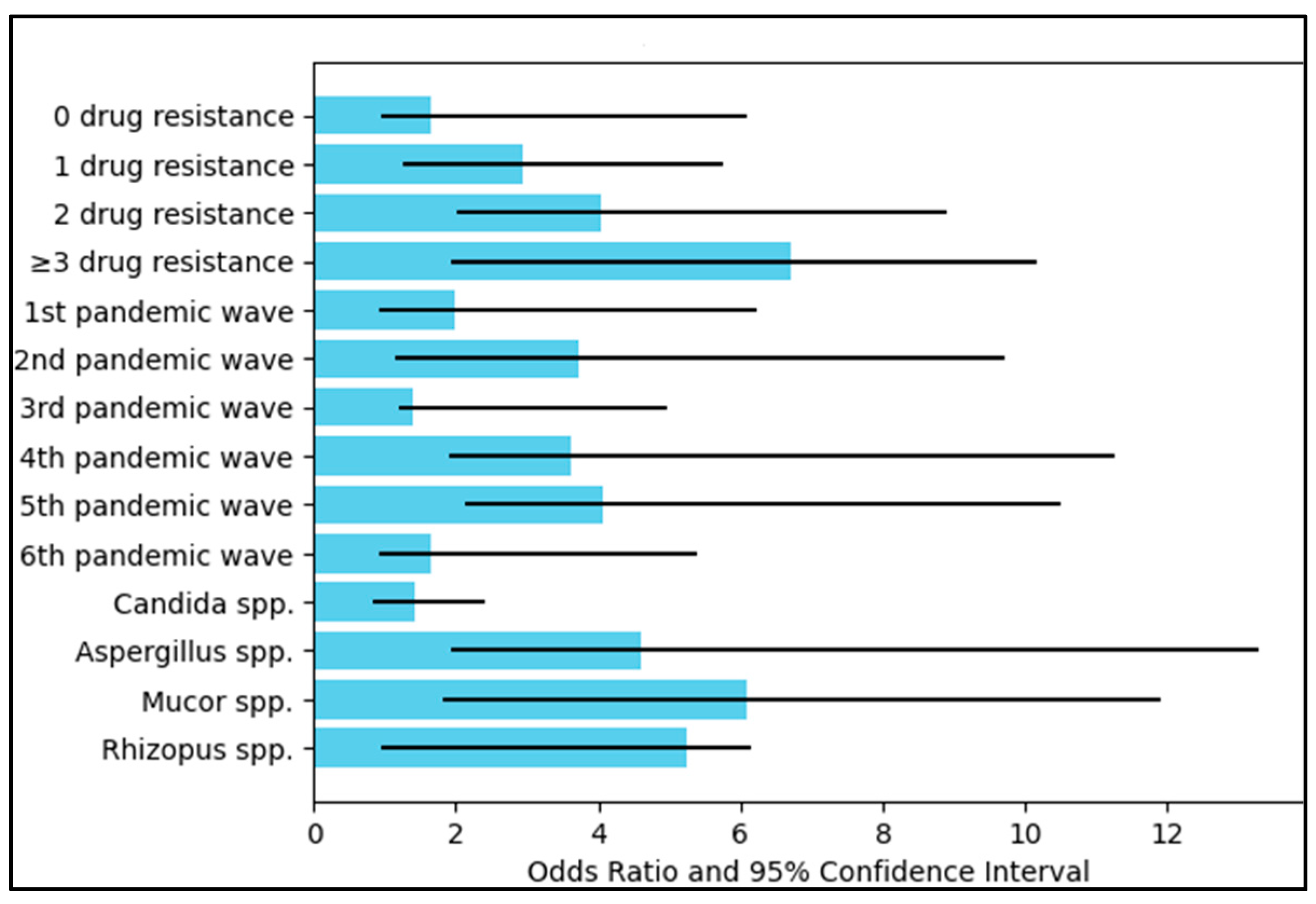
3.4. Mortality Risk Assessment
4. Discussion
4.1. Literature Findings
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Citu, C.; Burlea, B.; Gorun, F.; Motoc, A.; Gorun, O.M.; Malita, D.; Ratiu, A.; Margan, R.; Grigoras, M.L.; Bratosin, F.; et al. Predictive Value of Blood Coagulation Parameters in Poor Outcomes in COVID-19 Patients: A Retrospective Observational Study in Romania. J. Clin. Med. 2022, 11, 2831. [Google Scholar] [CrossRef] [PubMed]
- Pollard, C.A.; Morran, M.P.; Nestor-Kalinoski, A.L. The COVID-19 pandemic: A global health crisis. Physiol. Genom. 2020, 52, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Mallah, S.I.; Ghorab, O.K.; Al-Salmi, S.; Abdellatif, O.S.; Tharmaratnam, T.; Iskandar, M.A.; Sefen, J.A.N.; Sidhu, P.; Atallah, B.; El-Lababidi, R.; et al. COVID-19: Breaking down a global health crisis. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 35. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, transmission, diagnosis, and treatment of Coronavirus Disease 2019 (COVID-19): A review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Citu, I.M.; Citu, C.; Margan, M.-M.; Craina, M.; Neamtu, R.; Gorun, O.M.; Burlea, B.; Bratosin, F.; Rosca, O.; Grigoras, M.L.; et al. Calcium, Magnesium, and Zinc Supplementation during Pregnancy: The Additive Value of Micronutrients on Maternal Immune Response after SARS-CoV-2 Infection. Nutrients 2022, 14, 1445. [Google Scholar] [CrossRef]
- Cerbu, B.; Grigoras, M.L.; Bratosin, F.; Bogdan, I.; Citu, C.; Bota, A.V.; Timircan, M.; Bratu, M.L.; Levai, M.C.; Marincu, I. Laboratory Profile of COVID-19 Patients with Hepatitis C-Related Liver Cirrhosis. J. Clin. Med. 2022, 11, 652. [Google Scholar] [CrossRef]
- Timircan, M.; Bratosin, F.; Vidican, I.; Suciu, O.; Turaiche, M.; Bota, A.V.; Mitrescu, S.; Marincu, I. Coping Strategies and Health-Related Quality of Life in Pregnant Women with SARS-CoV-2 Infection. Medicina 2021, 57, 1113. [Google Scholar] [CrossRef]
- Cafardi, J.; Haas, D.; Lamarre, T.; Feinberg, J. Opportunistic Fungal Infection Associated With COVID-19. Open Forum. Infect Dis. 2021, 18, 8. [Google Scholar] [CrossRef]
- Kangabam, N.; Nethravathy, V. An overview of opportunistic fungal infections associated with COVID-19. 3 Biotech 2023, 13, 231. [Google Scholar] [CrossRef]
- Arastehfar, A.; Carvalho, A.; van de Veerdonk, F.L.; Jenks, J.D.; Koehler, P.; Krause, R.; Cornely, O.A.; Perlin, D.S.; Lass-Flörl, C.; Hoenigl, M. COVID-19 associated pulmonary aspergillosis (CAPA)—From immunology to treatment. J. Fungi 2020, 6, 91. [Google Scholar] [CrossRef] [PubMed]
- Gangneux, J.P.; Bougnoux, M.E.; Dannaoui, E.; Cornet, M.; Zahar, J.R. Invasive fungal diseases during COVID-19: We should be prepared. J. Mycol. Med. 2020, 30, 100971. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Cornely, O.A.; Böttiger, B.W.; Dusse, F.; Eichenauer, D.A.; Fuchs, F.; Hallek, M.; Jung, N.; Klein, F.; Persigehl, T.; et al. COVID-19 associated pulmonary aspergillosis. Mycoses 2020, 63, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Kuchi Bhotla, H.; Balasubramanian, B.; Meyyazhagan, A.; Pushparaj, K.; Easwaran, M.; Pappusamy, M.; Alwin Robert, A.; Arumugam, V.A.; Tsibizova, V.; Msaad Alfalih, A.; et al. Opportunistic mycoses in COVID-19 patients/survivors: Epidemic inside a pandemic. J. Infect. Public Health. 2021, 14, 1720–1726. [Google Scholar] [CrossRef] [PubMed]
- Altinkaya Çavuş, M.; Sav, H. Opportunistic Candida Infections in Critical COVID-19 Patients. Pol. J. Microbiol. 2022, 71, 411–419. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Pilut, C.N.; Citu, C.; Gorun, F.; Bratosin, F.; Gorun, O.M.; Burlea, B.; Citu, I.M.; Grigoras, M.L.; Manolescu, D.; Gluhovschi, A. The Utility of Laboratory Parameters for Cardiac Inflammation in Heart Failure Patients Hospitalized with SARS-CoV-2 Infection. Diagnostics 2022, 12, 824. [Google Scholar] [CrossRef]
- White, P.L.; Dhillon, R.; Cordey, A.; Hughes, H.; Faggian, F.; Soni, S.; Pandey, M.; Whitaker, H.; May, A.; Morgan, M.; et al. A national strategy to diagnose coronavirus disease 2019–associated invasive fungal disease in the intensive care unit. Clin. Infect. Dis. 2020, 71, 2212–2221. [Google Scholar] [CrossRef]
- Rawson, T.M.; Antcliffe, D.B.; Wilson, R.C.; Abdolrasouli, A.; Moore, L.S.P. Management of Bacterial and Fungal Infections in the ICU: Diagnosis, Treatment, and Prevention Recommendations. Infect. Drug Resist. 2023, 16, 2709–2726. [Google Scholar] [CrossRef]
- Chakraborti, A.; Jaiswal, A.; Verma, P.K.; Singhal, R. A Prospective Study of Fungal Colonization and Invasive Fungal Disease in Long-Term Mechanically Ventilated Patients in a Respiratory Intensive Care Unit. Indian J. Crit Care Med. 2018, 22, 597–601. [Google Scholar] [CrossRef]
- Arastehfar, A.; Carvalho, A.; Nguyen, M.H.; Hedayati, M.T.; Netea, M.G.; Perlin, D.S.; Hoenigl, M. COVID-19-Associated Candidiasis (CAC): An Underestimated Complication in the Absence of Immunological Predispositions? J. Fungi 2020, 6, 211. [Google Scholar] [CrossRef] [PubMed]
- Guarner, J.; Brandt, M.E. Histopathologic diagnosis of fungal infections in the 21st century. Clin. Microbiol. Rev. 2011, 24, 247–280. [Google Scholar] [CrossRef] [Green Version]
- Freeman Weiss, Z.; Leon, A.; Koo, S. The Evolving Landscape of Fungal Diagnostics, Current and Emerging Microbiological Approaches. J. Fungi 2021, 7, 127. [Google Scholar] [CrossRef] [PubMed]
- Luethy, P.M.; Johnson, J.K. The Use of Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry (MALDI-TOF MS) for the Identification of Pathogens Causing Sepsis. J. Appl. Lab. Med. 2019, 3, 675–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avni, T.; Leibovici, L.; Paul, M. PCR diagnosis of invasive candidiasis: Systematic review and meta-analysis. J. Clin. Microbiol. 2011, 49, 665–670. [Google Scholar] [CrossRef] [Green Version]
- White, P.L.; Bretagne, S.; Klingspor, L.; Melchers, W.J.; McCulloch, E.; Schulz, B.; Finnstrom, N.; Mengoli, C.; Barnes, R.A.; Donnelly, J.P.; et al. Aspergillus PCR: One step closer to standardization. J. Clin. Microbiol. 2010, 48, 1231–1240. [Google Scholar] [CrossRef] [Green Version]
- Bogdan, I.; Gadela, T.; Bratosin, F.; Dumitru, C.; Popescu, A.; Horhat, F.G.; Negrean, R.A.; Horhat, R.M.; Mot, I.C.; Bota, A.V.; et al. The Assessment of Multiplex PCR in Identifying Bacterial Infections in Patients Hospitalized with SARS-CoV-2 Infection: A Systematic Review. Antibiotics 2023, 12, 465. [Google Scholar] [CrossRef]
- Carvalho-Pereira, J.; Fernandes, F.; Araújo, R.; Springer, J.; Loeffler, J.; Buitrago, M.J.; Pais, C.; Sampaio, P. Multiplex PCR Based Strategy for Detection of Fungal Pathogen DNA in Patients with Suspected Invasive Fungal Infections. J. Fungi 2020, 6, 308. [Google Scholar] [CrossRef]
- Loeffler, J.; Stevens, D.A. Antifungal drug resistance. Clin. Infect. Dis. 2003, 36, S31–S41. [Google Scholar] [CrossRef] [Green Version]
- Bogdan, I.; Citu, C.; Bratosin, F.; Malita, D.; Romosan, I.; Gurban, C.V.; Bota, A.V.; Turaiche, M.; Bratu, M.L.; Pilut, C.N.; et al. The Impact of Multiplex PCR in Diagnosing and Managing Bacterial Infections in COVID-19 Patients Self-Medicated with Antibiotics. Antibiotics 2022, 11, 437. [Google Scholar] [CrossRef]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149–e162. [Google Scholar] [CrossRef]
- Fericean, R.M.; Citu, C.; Manolescu, D.; Rosca, O.; Bratosin, F.; Tudorache, E.; Oancea, C. Characterization and Outcomes of SARS-CoV-2 Infection in Overweight and Obese Patients: A Dynamic Comparison of COVID-19 Pandemic Waves. J. Clin. Med. 2022, 11, 2916. [Google Scholar] [CrossRef]
- Fericean, R.M.; Oancea, C.; Reddyreddy, A.R.; Rosca, O.; Bratosin, F.; Bloanca, V.; Citu, C.; Alambaram, S.; Vasamsetti, N.G.; Dumitru, C. Outcomes of Elderly Patients Hospitalized with the SARS-CoV-2 Omicron B.1.1.529 Variant: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 2150. [Google Scholar] [CrossRef]
- Alanio, A.; Dellière, S.; Fodil, S.; Bretagne, S.; Mégarbane, B. Prevalence of putative invasive pulmonary aspergillosis in critically ill patients with COVID-19. Lancet Respir. Med. 2020, 8, e48–e49. [Google Scholar] [CrossRef]
- Gangneux, J.P.; Reizine, F.; Guegan, H.; Pinceaux, K.; Le Balch, P.; Prat, E.; Pelletier, R.; Belaz, S.; Le Souhaitier, M.; Le Tulzo, Y.; et al. Is the COVID-19 pandemic a good time to include Aspergillus molecular detection to categorize aspergillosis in ICU patients? A monocentric experience. J. Fungi 2020, 6, 105. [Google Scholar] [CrossRef]
- Li, X.; Zhong, X.; Wang, Y.; Zeng, X.; Luo, T.; Liu, Q. Clinical determinants of the severity of COVID-19: A systematic review and meta-analysis. PLoS ONE 2001, 16, e0250602. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision, 2nd ed.; World Health Organization: Geneva, Switzerland, 2004; Available online: https://apps.who.int/iris/handle/10665/42980 (accessed on 5 March 2023).
- Bacconi, A.; Richmond, G.S.; Baroldi, M.A.; Laffler, T.G.; Blyn, L.B.; Carolan, H.E.; Frinder, M.R.; Toleno, D.M.; Metzgar, D.; Gutierrez, J.R.; et al. Improved sensitivity for molecular detection of bacterial and Candida infections in blood. J. Clin. Microbiol. 2014, 52, 3164–3174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing: Twenty-Second Informational Supplement; CLSI: Wayne, PA, USA, 2012; Volume 32, pp. 1–184. [Google Scholar]
- Lehmann, L.E.; Hunfeld, K.P.; Emrich, T.; Haberhausen, G.; Wissing, H.; Hoeft, A.; Stüber, F. A multiplex real-time PCR assay for rapid detection and differentiation of 25 bacterial and fungal pathogens from whole blood samples. Med. Microbiol. Immunol. 2008, 197, 313–324. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Laboratory Biosafety Guidance Related to Coronavirus Disease (COVID-19)—Interim Guidance (28 January 2021); World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Steenblock, C.; Schwarz, P.E.H.; Ludwig, B.; Linkermann, A.; Zimmet, P.; Kulebyakin, K.; Tkachuk, A.V.; Markov, A.G.; Lehnert, H.; de Angelis, M.H.; et al. COVID-19 and metabolic disease: Mechanisms and clinical management. Lancet Diabetes Endocrinol. 2021, 9, 786–798. [Google Scholar] [CrossRef]
- Ganji, R.; Reddy, P.H. Impact of COVID-19 on Mitochondrial-Based Immunity in Aging and Age-Related Diseases. Front. Aging Neurosci. 2021, 12, 614650. [Google Scholar] [CrossRef]
- Lazar, M. Sequencing of the SARS-CoV-2 Virus Genome in Romania. National Institute of Medical-Military Research and Development “Cantacuzino”. Available online: https://cantacuzino.mapn.ro/pages/view/249 (accessed on 5 March 2023).
- Hodcroft, E.B.; Zuber, M.; Nadeau, S.; Vaughan, T.G.; Crawford, K.H.D.; Althaus, C.L.; Reichmuth, M.L.; Bowen, J.E.; Walls, A.C.; Corti, D.; et al. Spread of a SARS-CoV-2 variant through Europe in the summer of 2020. Nature 2021, 595, 707–712. [Google Scholar] [CrossRef]
- Dascalu, S.; Geambasu, O.; Valentin Raiu, C.; Azoicai, D.; Damian Popovici, E.; Apetrei, C. COVID-19 in Romania: What Went Wrong? Front. Public Health 2021, 9, 813941. [Google Scholar] [CrossRef] [PubMed]
- Streinu-Cercel, A.; Săndulescu, O.; Miron, V.D.; Paraschiv, S.; Casangiu, C.; Hohan, R.; Bănică, L.; Surleac, M.; Streinu-Cercel, A. Undetected Omicron Transmission in Romania-Report of the First Detected Case of Locally Acquired Omicron Infection and Complete Epidemiological Investigation. Diagnostics 2022, 12, 348. [Google Scholar] [CrossRef] [PubMed]
- Popa, A.D.; Antoniu, S.A.; Enache, A.I.; Popa, I.V.; Dragomir, R.A.; Burlacu, A. Development and Validation of a Questionnaire to Assess Knowledge and Attitudes toward COVID-19 Preventive Measures in Romania. Healthcare 2022, 10, 1827. [Google Scholar] [CrossRef]
- Hamza, A.; Shah, N.N.; Azad, A.M.; Ghanshyam, O.S.; Khan, Z. Impact of age, gender and comorbidities affecting the severity of COVID-19 infection in Kashmir. J. Fam. Med. Prim. Care 2022, 11, 1519–1524. [Google Scholar] [CrossRef]
- Hu, D.; Lou, X.; Meng, N.; Li, Z.; Teng, Y.; Zou, Y.; Wang, F. Influence of age and gender on the epidemic of COVID-19: Evidence from 177 countries and territories-an exploratory, ecological study. Wien. Klin. Wochenschr. 2021, 133, 321–330. [Google Scholar] [CrossRef]
- Singh, R.; Rathore, S.S.; Khan, H.; Karale, S.; Chawla, Y.; Iqbal, K.; Bhurwal, A.; Tekin, A.; Jain, N.; Mehra, I.; et al. Association of Obesity With COVID-19 Severity and Mortality: An Updated Systemic Review, Meta-Analysis, and Meta-Regression. Front. Endocrinol. 2022, 13, 780872. [Google Scholar] [CrossRef] [PubMed]
- Barber, K.E.; Wagner, J.L.; Miller, J.M.; Lewis, E.A.; Stover, K.R. Impact of Obesity in Patients with Candida Bloodstream Infections: A Retrospective Cohort Study. Infect. Dis. Ther. 2020, 9, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Comoglu, S.; Kant, A. Does the Charlson comorbidity index help predict the risk of death in COVID-19 patients? North. Clin. Istanbul. 2022, 9, 117–121. [Google Scholar] [CrossRef]
- Gangneux, J.P.; Dannaoui, E.; Fekkar, A.; Luyt, C.E.; Botterel, F.; De Prost, N.; Tadié, J.M.; Reizine, F.; Houzé, S.; Timsit, J.F.; et al. Fungal infections in mechanically ventilated patients with COVID-19 during the first wave: The French multicentre MYCOVID study. Lancet Respir. Med. 2022, 10, 180–190. [Google Scholar] [CrossRef]
- Delisle, M.S.; Williamson, D.R.; Albert, M.; Perreault, M.M.; Jiang, X.; Day, A.G.; Heyland, D.K. Impact of Candida species on clinical outcomes in patients with suspected ventilator-associated pneumonia. Can Respir. J. 2011, 18, 131–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razazi, K.; Arrestier, R.; Haudebourg, A.F.; Benelli, B.; Carteaux, G.; Decousser, J.W.; Fourati, S.; Woerther, P.L.; Schlemmer, F.; Charles-Nelson, A.; et al. Risks of ventilator-associated pneumonia and invasive pulmonary aspergillosis in patients with viral acute respiratory distress syndrome related or not to Coronavirus 19 disease. Crit. Care 2020, 24, 699. [Google Scholar] [CrossRef]
- Seyedjavadi, S.S.; Bagheri, P.; Nasiri, M.J.; Razzaghi-Abyaneh, M.; Goudarzi, M. Fungal Infection in Co-infected Patients With COVID-19: An Overview of Case Reports/Case Series and Systematic Review. Front. Microbiol. 2022, 13, 888452. [Google Scholar] [CrossRef] [PubMed]
- Allou, N.; Larsen, K.; Dubernet, A.; Traversier, N.; Masse, L.; Foch, E.; Bruneau, L.; Maillot, A.; André, M.; Lagrange-Xelot, M.; et al. Co-Infection in Patients with Hypoxemic Pneumonia Due to COVID-19 in Reunion Island. Medicine 2021, 100, e24524. [Google Scholar] [CrossRef] [PubMed]
- Caméléna, F.; Moy, A.-C.; Dudoignon, E.; Poncin, T.; Deniau, B.; Guillemet, L.; Le Goff, J.; Budoo, M.; Benyamina, M.; Chaussard, M.; et al. Performance of a Multiplex Polymerase Chain Reaction Panel for Identifying Bacterial Pathogens Causing Pneumonia in Critically Ill Patients with COVID-19. Diagn. Microbiol. Infect. Dis. 2021, 99, 115183. [Google Scholar] [CrossRef] [PubMed]
- Lapa, S.A.; Miftakhov, R.A.; Klochikhina, E.S.; Ammur, Y.I.; Blagodatskikh, S.A.; Shershov, V.E.; Zasedatelev, A.S.; Chudinov, A.V. Development of Multiplex RT-PCR with Immobilized Primers for Identification of Infectious Human Pneumonia Pathogens. Mol. Biol. 2021, 55, 828–838. [Google Scholar] [CrossRef] [PubMed]
- Miuțescu, B.; Vuletici, D.; Burciu, C.; Turcu-Stiolica, A.; Bende, F.; Rațiu, I.; Moga, T.; Sabuni, O.; Anjary, A.; Dalati, S.; et al. Identification of Microbial Species and Analysis of Antimicrobial Resistance Patterns in Acute Cholangitis Patients with Malignant and Benign Biliary Obstructions: A Comparative Study. Medicina 2023, 59, 721. [Google Scholar] [CrossRef]
- Aljeldah, M.M. Antimicrobial Resistance and Its Spread Is a Global Threat. Antibiotics 2020, 11, 1082. [Google Scholar] [CrossRef]
- Shishido, A.A.; Mathew, M.; Baddley, J.W. Overview of COVID-19-Associated Invasive Fungal Infection. Curr. Fungal Infect. Rep. 2022, 16, 87–97. [Google Scholar] [CrossRef]
- Domán, M.; Bányai, K. COVID-19-Associated Fungal Infections: An Urgent Need for Alternative Therapeutic Approach? Front. Microbiol. 2022, 13, 919501. [Google Scholar] [CrossRef]
- Song, G.; Liang, G.; Liu, W. Fungal Co-infections Associated with Global COVID-19 Pandemic: A Clinical and Diagnostic Perspective from China. Mycopathologia 2020, 185, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Kuehn, B.M. Aspergillosis Is Common Among COVID-19 Patients in the ICU. JAMA 2021, 326, 1573. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables * | Fungal Infection (n = 96) | No Infection (n = 192) | p-Value |
|---|---|---|---|
| Age (mean ± SD) | 64.6 ± 12.1 | 62.0 ± 11.5 | 0.076 |
| Men (n, %) | 61 (63.5%) | 107 (55.7%) | 0.205 |
| BMI obese (>29.9 kg/m2) | 34 (35.4%) | 41 (21.4%) | 0.010 |
| COVID-19 vaccinated with ≥2 doses (n, %) | 9 (9.4%) | 20 (10.4%) | 0.781 |
| Smoking (n, %) | 42 (43.8%) | 66 (34.4%) | 0.121 |
| Pulmonary disease | |||
| Chronic bronchitis | 14 (14.6%) | 39 (20.3%) | 0.236 |
| COPD | 18 (18.8%) | 22 (11.5%) | 0.092 |
| Asthma | 12 (12.5%) | 20 (10.4%) | 0.595 |
| Pulmonary hypertension | 3 (3.1%) | 8 (4.2%) | 0.663 |
| CCI (>2) | 36 (37.5%) | 48 (25.0%) | 0.027 |
| Pandemic wave | 0.272 | ||
| 1st pandemic wave | 7 (7.3%) | 23 (12.0%) | |
| 2nd pandemic wave | 13 (13.5%) | 34 (17.7%) | |
| 3rd pandemic wave | 20 (20.8%) | 30 (15.6%) | |
| 4th pandemic wave | 18 (18.8%) | 29 (15.1%) | |
| 5th pandemic wave | 29 (30.2%) | 46 (24.0%) | |
| 6th pandemic wave | 9 (9.4%) | 30 (15.6%) |
| Variables | Fungal Infection (n = 96) | No Infection (n = 192) | p-Value |
|---|---|---|---|
| Performed blood tests | |||
| Conventional culture | 62 (64.6%) | 108 (56.3%) | 0.175 |
| Multiplex PCR | 96 (100%) | 192 (100%) | - |
| Oxygen supplementation | |||
| AIRVO | 66 (68.8%) | 141 (73.4%) | 0.404 |
| CPAP | 35 (36.5%) | 98 (51.0%) | 0.019 |
| Ventilator | 44 (45.8%) | 36 (18.8%) | <0.001 |
| Time of sampling | 0.156 | ||
| Within 48 h from admission | 59 (61.5%) | 134 (69.8%) | |
| After 48 h from admission | 37 (38.5%) | 58 (30.2%) | |
| Outcomes | |||
| ICU admission | 38 (39.6%) | 51 (26.6%) | 0.024 |
| Days in the ICU (mean ± SD) | 12.8 ± 7.2 | 10.5 ± 6.9 | 0.009 |
| Days between symptom onset until death (mean ± SD) | 13.6 ± 9.4 | 16.2 ± 8.0 | 0.014 |
| Mortality | 31 (32.3%) | 23 (12.0%) | <0.001 |
| Days until discharge (mean ± SD) | 18.8 ± 9.0 | 15.3 ± 9.7 | 0.003 |
| Findings | 1st Wave (n = 7) | 2nd Wave (n = 13) | 3rd Wave (n = 20) | 4th Wave (n = 18) | 5th Wave (n = 29) | 6th Wave (n = 9) | p-Value |
|---|---|---|---|---|---|---|---|
| Fungal infections | 0.209 | ||||||
| Candida spp. | 5 (71.4%) | 8 (61.5%) | 7 (35.0%) | 10 (55.6%) | 17 (58.6%) | 4 (44.4%) | |
| Aspergillus spp. | 2 (28.6%) | 4 (30.8%) | 11 (55.0%) | 6 (33.3%) | 9 (31.0%) | 4 (44.4%) | |
| Mucor spp. | 0 (20.0%) | 1 (7.7%) | 1 (5.0%) | 0 (0.0%) | 1 (3.4%) | 0 (0.0%) | |
| Rhizopus spp. | 0 (20.0%) | 0 (0.0%) | 1 (5.0%) | 2 (11.1%) | 2 (6.9%) | 1 (11.1%) | |
| Outcomes | |||||||
| ICU admissions | 5 (13.2%) | 6 (15.8%) | 8 (21.1%) | 11 (28.9%) | 5 (13.2%) | 3 (7.9%) | 0.024 |
| Mortality | 5 (16.1%) | 5 (16.1%) | 6 (19.4%) | 10 (32.3%) | 4 (12.9%) | 3 (3.2%) | 0.018 |
| Findings | Candida spp. (n = 51) | Aspergillus spp. (n = 36) | Mucor spp. (n = 3) | Rhizopus spp. (n = 6) |
|---|---|---|---|---|
| 0 drug resistance | 10 (19.6%) | 7 (19.4%) | 1 (33.3%) | 0 (0.0%) |
| 1 drug resistance | 18 (35.3%) | 12 (33.3%) | 1 (33.3%) | 3 (50.0%) |
| 2 drug resistance | 20 (39.2%) | 15 (41.7%) | 1 (33.3%) | 1 (16.7%) |
| ≥3 drug resistance | 3 (5.9%) | 2 (5.6%) | 0 (0.0%) | 2 (33.3%) |
| Mortality Risk | OR | 95% CI | p |
|---|---|---|---|
| By drug resistance features | |||
| 0 drug resistance | 1.66 | 0.94–6.10 | 0.062 |
| 1 drug resistance | 2.95 | 1.26–5.74 | 0.001 |
| 2 drug resistance | 4.03 | 2.02–8.91 | <0.001 |
| ≥3 drug resistance | 6.71 | 1.93–10.16 | <0.001 |
| By pandemic wave | |||
| 1st pandemic wave | 1.98 | 0.91–6.24 | 0.119 |
| 2nd pandemic wave | 3.72 | 1.15–9.70 | <0.001 |
| 3rd pandemic wave | 1.40 | 1.21–4.96 | 0.003 |
| 4th pandemic wave | 3.61 | 1.90–11.27 | <0.001 |
| 5th pandemic wave | 4.08 | 2.12–10.49 | <0.001 |
| 6th pandemic wave | 1.66 | 0.93–5.39 | 0.084 |
| By type of fungal infection | |||
| Candida spp. | 1.43 | 0.85–2.41 | 0.194 |
| Aspergillus spp. | 4.61 | 1.92–13.27 | <0.001 |
| Mucor spp. | 6.08 | 1.82–11.90 | <0.001 |
| Rhizopus spp. | 5.26 | 0.96–6.15 | 0.107 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bogdan, I.; Reddyreddy, A.R.; Nelluri, A.; Maganti, R.K.; Bratosin, F.; Fericean, R.M.; Dumitru, C.; Barata, P.I.; Tapalaga, G.; Marincu, I. Fungal Infections Identified with Multiplex PCR in Severe COVID-19 Patients during Six Pandemic Waves. Medicina 2023, 59, 1253. https://doi.org/10.3390/medicina59071253
Bogdan I, Reddyreddy AR, Nelluri A, Maganti RK, Bratosin F, Fericean RM, Dumitru C, Barata PI, Tapalaga G, Marincu I. Fungal Infections Identified with Multiplex PCR in Severe COVID-19 Patients during Six Pandemic Waves. Medicina. 2023; 59(7):1253. https://doi.org/10.3390/medicina59071253
Chicago/Turabian StyleBogdan, Iulia, Akash Reddy Reddyreddy, Aditya Nelluri, Ram Kiran Maganti, Felix Bratosin, Roxana Manuela Fericean, Catalin Dumitru, Paula Irina Barata, Gianina Tapalaga, and Iosif Marincu. 2023. "Fungal Infections Identified with Multiplex PCR in Severe COVID-19 Patients during Six Pandemic Waves" Medicina 59, no. 7: 1253. https://doi.org/10.3390/medicina59071253