
COVID-19 and the Use of Angiotensin II Receptor Blockers in Older Chronic Hypertensive Patients: Systematic Review and Meta-Analysis
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Information Sources and Search Strategy
2.3. Eligibility Criteria
2.4. Study Selection Process
2.5. Data Collection and Synthesis
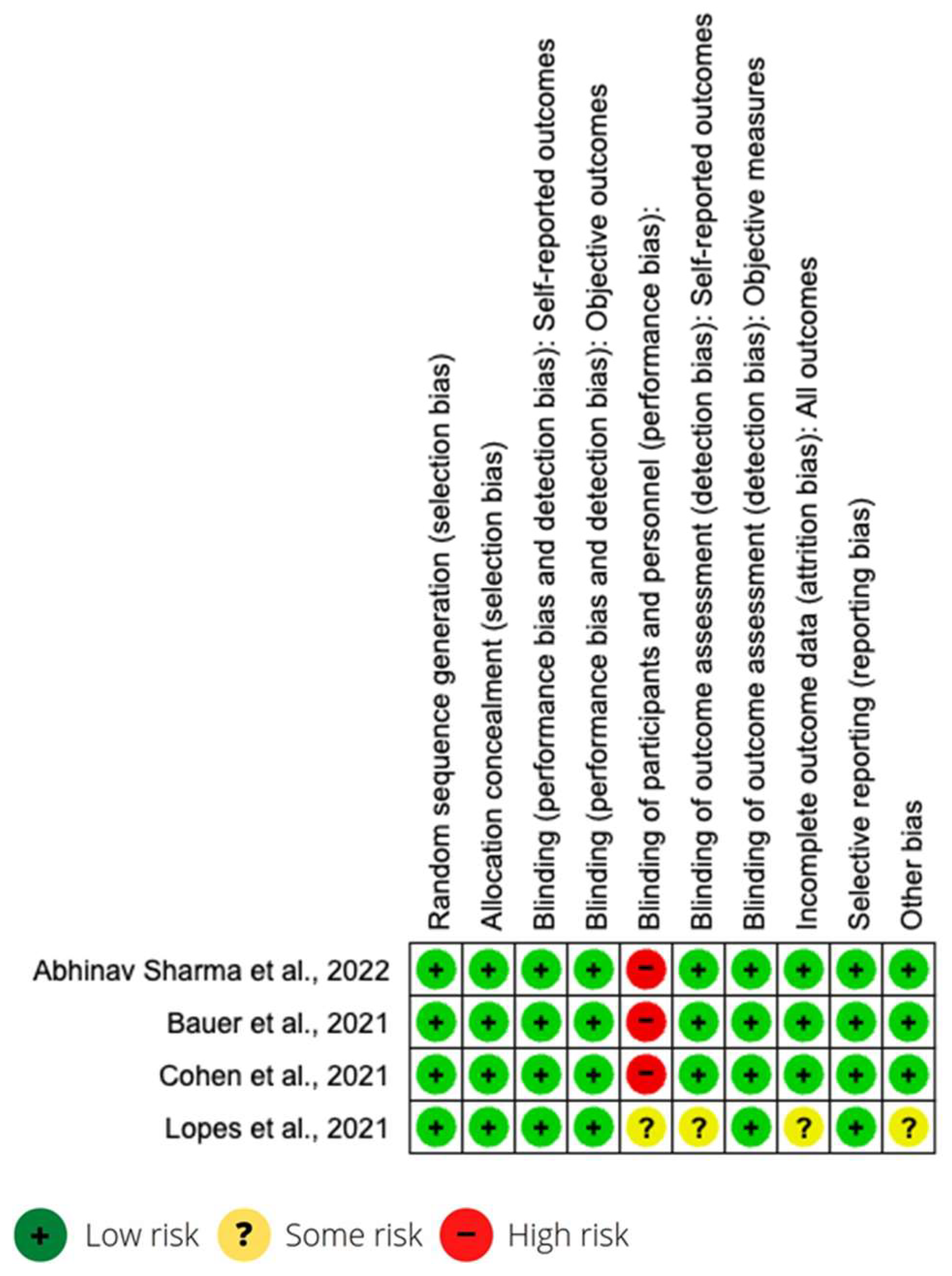
2.6. Risk of Bias Assessment and Level of Evidence
2.7. Data Analysis
3. Results
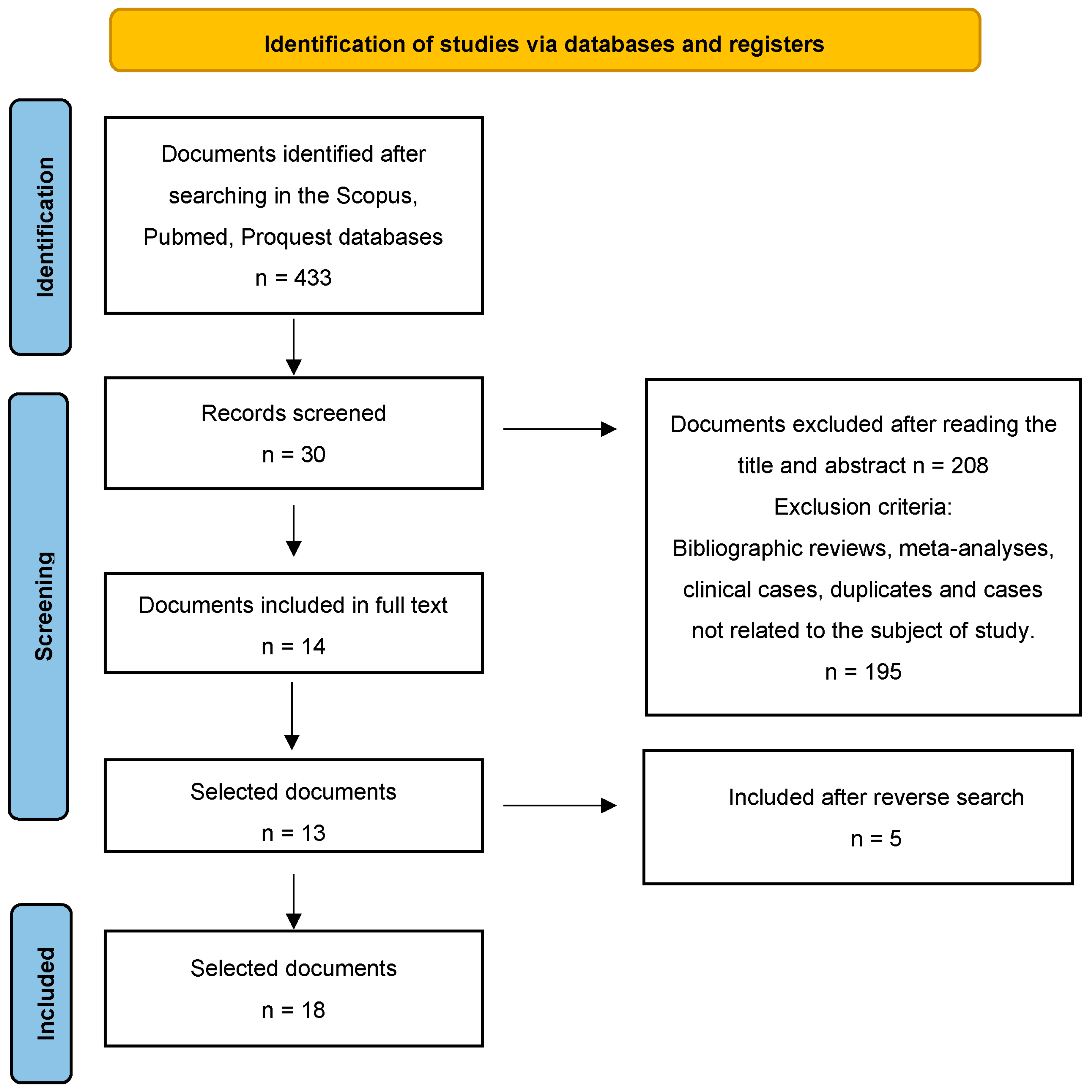
3.1. Study Selection and Study Characteristics of the Studies Included

| Author, Year, Country | Design | Sample/Age/Prevalence | Intervention | Mean ± SD | Measures | Main Results/ ICU Admission | LE/GR |
|---|---|---|---|---|---|---|---|
| Bauer et al., 2021 (Austria and Germany) [28] | Randomized controlled clinical trial (RCT) | n = 204 outpatients; Age = 75 Continuation Group (1) = 100; Discontinuation Group (2) = 104 Dyslipidaemia = 86 (42%); DMT2 = 67 (33%); Atrial Fibrilation = 35 (17%); Kidney Disease = 37 (18%); IMC = 27.5; HBP = 199 (98%) Vital Parameters Beats/mi: (1) 76–(2) 76; Respiratory/min: (1) 18–(2) 18; Temperature: (1) 37–(2) 37; Blood pressure: (1) 130/77–(2) 130/75; Oxygen Saturation: (1) 94%–(2) 95% Respiratory Therapy Oxygen substitution: (1) 45–(2) 41 Oxygen mask therapy: (1) 43–(2) 37 Non-invasive ventilation: (1) 5–(2) 0 Radiological Signs Bipulmonar infiltrates: (1) 36–(2) 38 Other opacities: (1) 29–(2) 26 C reactive protein: (1) 5.1–(2) 4.5 | Comparison ACEI/ARAII Versus not taking them regardless of whether they are hospitalized | N1 = 104 withdraws ACEI/ARA II N2 = 100 continues ACEI/ARA II Max SOFA score 0 (0–2) vs. 1 (0–3) p = 0.12 Lower AUCsofa 0 (0–9.25) vs. 3.5 (0–23.5) p = 0.040 Mean SOFA score 0 (0–31) vs. 0.12 (0–0.78) p = 0.040 30 days SOFA score 0 (0–1.20) vs. 0 (0–24) Patients with severe involvement with mechanical ventilation (10% N1 vs. 8% N2 p = 0.87) or in ICU (19% N1 vs. 18% N2 p = 0.96) At 30 days, 11% of the withdrawal group and 23% of the drug continuation group had signs of organ dysfunction or have passed away p = 0.017. | 1—Max SOFA score 2—Lower AUCSOFA 3—Mean SOFA 4—30 days SOFA score Prevalence Severity ICU Mechanical ventilation | Withdrawing ACEI/ARAII in COVID-19 patients had no effect in severely affected patients with mechanical ventilation or in ICU, but the results of this trial indicate that withdrawal of ACEI and ARAII may allow a faster and better recovery. / YES | 1a/A |
| Bean et al., 2020 (England) [29] | Cohorts | n = 1200 patients hospitalized in London Age = 63 +/− 20 SD Heart Disease = 107 (8%); DMT2 = 418 (35%); Kidney Disease = 206 (17%); Obesity = 182 (15%); Stroke = 235 (20%); Chronic Obstructive Lung Disease = 121 (10%); HBP = 645 (53%) | Comparison of ACEI/ARAII versus not taking them in hospitalized patients | N1 (ACEI/ARAII) = 399 N2 (no ACEI/ARAII) = 801 COVID-19 severity results OR 0.63 IC 0.47–0.84 (p = 0.01) | Odds Ratio Prevalence Severity | There is no evidence of an increase in the severity of COVID-19 in patients treated with ACEIs and ARBs in the study, and a possible protective factor is appreciated that must be corroborated in subsequent clinical trials. / NO | 2a/B |
| Cohen et al., 2021 (USA, Canada, Mexico, Sweden, Peru, Bolivia, Argentina) [30] | Randomized controlled clinical trial (RCT) | n = 152 hospitalized patients Age = 62 male (52%) and 68 female (48%) Hispanic 82 (54%) DMT2 79 (52%) with insuline 36 (23.7%) HBP = 152 | They compare ACEI/ARAII versus not taking them in hospitalized patients | N = 75 patients continue with ACEI/ARAII y N = 77 withdraws. Mean Rank 73 (IQR 40–100) for continuation group and 81 (IQR 38–117) for the group that withdraws. X2 for adverse events without differences between both groups p = 0.77 | Mean Rank X2 | No differences were found in the GLOBAL RANK SCORE, nor in adverse events, blood pressure, nor in serum levels of potassium or creatinine between both groups. / YES | 1a/A |
| De Spiegeleer et al., 2020 (Belgium) [31] | Cohorts | n = 154 patients with COVID-19 in home care Age = 86 +/− 7 SD COVID symtoms = 113 Asymptoms = 41 DMT2 = 28 (18%) HBP = 39 (25%) | They compare ACEI/ARAII and statins versus not taking them in non-hospitalized patients | Statins and the absence of COVID-19 symptoms (OR 2.91; CI 1.27–6.71) Statins and COVID-19 clinical improvement (OR 0.75; CI 0.24–1.87) ACEI/ARAII and COVID-19 clinical improvement (OR 0.48; CI 0.1–1.97). | Odds Ratio Prevalence | Finds significantly statistical results in taking statins and the absence of symptoms during COVID-19 infection. / NO | 2a/B |
| Elabd et al., 2021 (Kuwait) [32] | Cohorts | n = 4019 hospitalized in Kuwait City Age = 43.49 Heart Disease = 168 (4%); DMT2 = 634 (15%); Chronic Obstructive Lung Disease = 17 (0.4%); HBP = 782 (20%) | They compare ACEI/ARAII versus not taking them in hospitalized patients | N1 (ACEI/ARAII) = 325 N2 (no ACEI/ARAII) = 3694 N1 is inversely associated with ICU admission OR 0.57 CI 0.34–0.88 (p = 0.01) and inversely associated with mortality OR 0.56 IC 0.33–0.95 (p = 0.032). | Odds Ratio Prevalence Mortality | The results recommend continuing ACEI/ARAII in patients who acquire COVID-19. The protective effects of the study support this hypothesis. / YES | 2a/B |
| Fosbϕl et al., 2020 (Denmark) [33] | Cohorts retrospectives | n = 4480 patients without discriminating hospitalized or not. Age = 54.6 Heart Disease = 243 (5%); Atrial Fibrillation = 317 (7%); DMT2 = 411 (9%); Kidney Disease = 172 (4%); Stroke = 402 (9%); Chronic Obstructive Lung Disease = 634 (14%); HBP = 843 (18%) | They compare ACEI and ARAII versus not taking them regardless of being hospitalized. | N1 (ACEI/ARAII) = 895 N2 (no ACEI/ARAII) = 3585 Mortality 0.83 HR IC 0.67–1.03 p = 0.05 Death in severe COVID-19 HR 1.04 IC 0.89–1.29 p = 0.05 Incidence of COVID-19 in N1 HR 1.05 IC 0.80–1.36 p = 0.05 | Hazard Ratio Incidence Mortality Severity | ACEI/ARAII is not significantly associated with the diagnosis of COVID-19, nor with the severity of the infection nor with increased mortality. / NO | 2a/B |
| Hippisley-Cox et al., 2020 (England) [34] | Cohorts retrospectives | n = 8,275,949 Age = 48.47 PV = 19,486 (0.2%) COVID patients without discriminating hospitalization (1286 ICU of them) Heart Disease = 433,631 (5%); Atrial Fibrillation = 201,911 (2.4%); DMT2 = 536,516 (6%); Kidney Disease = 338,693 (4%); Obesity = 1,709,529 (20%); Chronic Obstructive Lung Disease = 195,115 (2%); HBP = 1,414,021 (17%) | They compare ACEI and ARAII versus not taking them regardless of being hospitalized. | N1 = ACEI = 2864 N2 = ARAII = 1417 N2 = no ACEI/ARAII = 3304 N1 vs. N3 COVID-19 risk HR 0.71 IC 0.67–0.74 p = 0.05 N2 vs. N3 COVID-19 risk HR 0.63 IC 0.59–0.67 p = 0.05 N1 vs. N3 increase ICU risk HR 0.89 IC 0.75–1.06 p = 0.05 N2 vs. N3 increase ICU risk HR 1.02 IC 0.83–1.25 p = 0.05 | Hazard Ratio Prevalence Severity | ACEI and ARAII are significantly associated with a reduced risk of COVID-19 in this study. / YES | 2a/B |
| Jeffery et al., 2022 (USA) [35] | Cohorts retrospectives | n = 1,059,474 Age = 72,623 Heart Disease = 254,773 (24%); DMT2 = 422,780 (40%); Kidney Disease = 212,362 (20%); Obesity = 116,557 (11%); Stroke = 73,361 (7%); Chronic Obstructive Lung Disease = 372,735 (35%); HBP = 1,059,474 (100%) | Reported association between ACEI/ARAII use and respiratory viral diseases without discriminating in-hospital and out-of-hospital patients. | N1 = 653,797 IECA/ARAII N2 = 405,677 No IECA/ARAII ICU risk 1.5 pp IC (1.2–1.9) (p = 0.05) Dyspnea Risk 0.7 pp (0.1–1.2 IC) (p = 0.05) AVDS Risk 0.9 pp (0.4–1.3 IC) (p = 0.05) | Percentage Point | Patients with AVRIs using ACEi/ARAII for HTN had a greater increase in poor outcomes during the COVID-19 pandemic than those using other HTN drugs. / YES | 2a/B |
| Lopes et al. 2021 (Brazil) [36] | Randomized controlled clinical trial (RCT) | n = 659 Age = 55.5 (46.1–66.1) Heart Disease = 39 (5%); DMT2 = 210 (32%); Kidney Disease = 9 (1%); Obesity = 341 (52%); HBP = 659 (100%) | Determine whether discontinuation compared with continuation of ACEI or ARAII changed the number of days alive and out of hospital within 30 days. | N1 Discontinue IECA/ARAII = 334 N2 Continue IECA/ARAII = 325 Not statistical association for Death Cardiovascular Death Evolution Days alive Day salive out of hospital p = 0.3 | Odds Ratio | In patients hospitalized with mild-to-moderate COVID-19 and who were taking ACE inhibitors or ARBs prior to hospital admission, there was no significant difference in the mean number of days alive and out of hospital for those assigned to Discontinue vs. continue these medications. / NO | 1a/A |
| Mancia et al., 2020 (Italy) [37] | Control cases | n = 37,031 Age = 68 +/− 13 SD VP = 6272 (16.93%) C = 30,759 Heart Disease = 8570 (23%); Kidney Disease = 1129 (3%); Chronic Obstructive Lung Disease = 521 (1%); Cancer = 5729 (15%) | They compare ACEI and ARAII versus not taking it and with other antihypertensive regardless of being hospitalized or not | N1 = ACEI 1508 N2 = ARAII 1394 N3 = ACC 1446 N4 = DIURETICS 1902 OR N1 COVID-19 = 0.95 (0.86–1.05) p = 0.05 OR N2 COVID-19 = 0.96 (0.87–1.07) p = 0.05 OR N1 Severity/Lethality 0.83 (0.63–1.10) p = 0.05 OR N2 0.91 (0.69–1.21) p = 0.05 | Odds Ratio Severity Mortality | There is no evidence of an association between ACEI and ARA II and the risk of COVID-19 or increased severity or lethality / NO | 2b/B |
| Mazzoni et al., 2022 (Italy) [38] | Cohorts retrospectives | n = 615 Age = 70.9 Atrial Fibrillation = 54 (9%); DMT2 = 107 (17%); Kidney Disease = 15 (2%); Obesity = 38 (6%); Chronic Obstructive Lung Disease = 25 (4%); Heart Disease = 59 (10%); ICU = 96 (15,6%); HBP = 86 (14%) | Analyzes hospitalized patients in one area of Italy and compares deaths who have taken ACEI/ARAII with Haven taken other hypertensive drug to observe a possible association. | N1 IECA/ARAII Death 86 N2 no IECA/ARAII Death 78 30 days alive 94.9% N1 91.8 N2 Mortality 2.8% N1 2.7% N2 IC (0.3–2.52) (p = 0.03) | Odds Ratio | The apparent increase in morbidity in patients with COVID-19 who received long-term treatment with ACE inhibitors or ARBs is not due to the drugs themselves, but to the conditions associated with their use. / NO | 2a/B |
| Morales et al., 2021 (Spain and USA) [39] | Cohorts | n = 1,355,349 hypertensive patients using ACE inhibitors/ARBs (363,785 monotherapy) Age = 67.20 Data from: SIDIAP 37796 (System for Research in Primary care) (1) VA-OMOP 320450 (Veterans Affair Observational Medicals outcomes) (2) CUIMC 5539 (Columbia University Irving medical Center) (3) Adjusted dates for Analysis Dyslipidemia: (1) 27%–(2) 44.7%–(3) 35.5%; DMT2: (1) 20.7%–(2) 29.5%–(3) 16.7%; Heart Disease: (1) 21.8%–(2) 13.3%–(3) 26.4%; Atrial Fibrillation: (1) 4.1%–(2) 2.7%–(3) 5%; Kidney disease: (1) 9.4%–(2) 6.7%–(3) 7.8%; Obesity: (1) 35.5%–(2) 11.9%–(3) 9.3%; Stroke/Cerebrovascular: (1) 2.2%–(2) 2.3%–(3) 5.2%; Chronic Obstructive Lung: (1) 6.2%–(2) 8.4%–(3) 2.9%; HBP: (1) 99.2%–(2) 68%–(3) 61% | They compare ACEI and ARAII versus not taking them regardless of being hospitalized. | N1 (ACEI/ARAII in monotherapy) = 363,785 N2 (ACC/HCLTZ in monotherapy) = 248,915 N3 (ACEI/ARAII in combination) = 711,799 N4 (ACC/HCLTZ in combination) = 473,076 Risk N1 vs. Risk N2 HR 0.98 IC 0.84–1.14 p < 0.05 Risk N3 vs. Risk N4 HR 1.01 IC 0.9–1.15 p < 0.05 Risk ACEI vs. Risk N2 HR 0.91 IC 0.68–1.21 p < 0.05 Risk ACEI vs. Risk N4 HR 0.95 IC 0.83–1.07 p < 0.05 Risk ACEI vs. Risk ARAII (both in combination) HR 0.88 IC 0.79–0.99 p < 0.05 Risk ACEI vs. risk ARAII (monotherapy) (HR 0.85 IC 0.69–1.05) | Relative risk | There is no significant increase in the risk of diagnosis of COVID-19 or in the results associated with ACEI/ARAII. / NO | 2a/B |
| Palazzuoli et al., 2020 (Italy) [40] | Cohorts retrospetives | n = 781 patients hospitalized for COVID-19 Age = 69 Heart Disease = 171 (21%); DMT2 = 143 (18%); Chronic Obstructive Lung Disease = 84 (11%); BP = 451 (58%); ICU care = 225 (29%) | They compare ACEI/ARAII versus not in hospital for patients over 50 years old. | N1 (ARAII) = 131 N2 (ACEI) = 171 N3 (no ACEI/ARAII) = 477 Mortality N1 OR 0.58 IC 0.35–1.07 p = 0.0796 Mortality N2 OR 0.55 IC 0.3–0.98 p = 0.0436 | Odds Ratio Prevalence Mortality | In patients over 50 years of age hospitalized for COVID-19, the use of ACEIs significantly reduces the risk of death. / NO | 2a/B |
| Peñalvo et al., 2021 (Belgium) [41] | Cohorts | n = 10,866 hospitalized patients from 119 Belgian hospitals Age = 67.82 Heart Disease (CVD) = 3984 (37%); DMT2 = 2522 (23%); Kidney Disease = 1513 (14%); Obesity = 782 (7%); Chronic obstructive Lung Disease = 1731 (16%); HBP = 4593 (42%); Cognitive issues = 1320 (12%); ICU care: (1) 425–(2) 990; Length of hospital stay: (1) 13.9–(2) 12.1 | They compare ACEI/ARAII versus not taking them in hospitalized patients | ACEI/ARAII in non-ICU patients are associated with a slight increase in recovery HR 1.07 IC 1.01–1.13 (p = 0.027) and mortality reduction HR 0.83 IC 0.75–0.93 (p = 0.001) not so in ICU patients in recovery HR 1.16 IC 0.97–1.38 (p = 0.098) nor in reduction of ICU mortality HR 0.91 IC 0.73–1.12 (p = 0.381) | Hazard Ratio Prevalence Recovery Mortality | The use of ACEI/ARAII in hospitalized patients, according to the results observed, protects the patient not admitted to the ICU, being associated with a discreet reduction in mortality. / YES | 2a/B |
| Sha et al., 2020 (USA) [42] | Cohorts retrospetives | n = 531 Afro-american patients hospitalized for COVID-19 Age = 60.01 +/− 15 Congestive Heart Disease = 79 (14%); DMT2 = 228 (42%); Kidney disease = 77 (14%); Chronic Obstructive Lung Disease = 36 (6%); BMI = 35 +/− 8.1; HBP = 425 (80%) | Comparison of ACEI/ARAII versus not taking them in hospitalized Afro-Americans | N1 (ACEI/ARAII) = 207 N2 (no ACEI/ARAII) =324 Hospital Mortality 18,4% N1 vs. 14,8% N2 (p = 0.28) Mechanical ventilation 22.2% N1 vs. 16% N2 (p = 0.07) Hospital length of stay 10 days N1 vs. 8.8 days N2 (p = 0.14) | Relative risk | The use of ACEI/ARAII in hospitalized Afro-Americans in the study carried out does not show differences with respect to withdrawing them. / YES | 2a/B |
| Sharma et al., 2022 (Canada) [43] | Randomized controlled clinical trial (RCT) | n = 46 Age = 69 Dislypidaemia = 27 (59%); Heart disease = 15 (32%); Atrial Fibrillation = 7 (15%); DMT2 = 20 (43%); Kidney Disease = 9 (20%); HBP = 46 (100%); Stroke = 3 (6%); Chronic Obstructive Lung Disease = 2 (4%) | Compares continue ACEI/ARAII treatment versus Discontinuation ACEI/ARAII. Hospital Study | N1 continue IECA/ARA II = 21 N2 discontinue IECA/ARAII = 25 Results p greater than 0.05 not statistically significant for BNP increase, heart failure and risk of adverse outcome. | Standard deviation | The continuation of RAASi in hospitalized participants with COVID-19 appears safe. It cannot be associated with the data increased risk of COVID-19 disease or morbidity and mortality to ACEi/ARAII. / YES | 1a/A |
| Trifiró et al., 2020 (Italy) [44] | Cohorts retrospectives | n = 42,926 hospitalized patients Age = 69 Heart Disease = 10,019 (23%); Atrial Fibrillation = 2899 (7%); DMT2 = 7710 (18%); Kidney Disease = 1046 (2%); Stroke = 3441 (8%); Chronic Obstructive Lung Disease = 1521 (4%); HBP = 5610 (13%); Death = 11,205 (26%) | They compare ACEI/ARAII against calcium antagonists and against no antihypertensive in hospitalized patients | N1 = ACEI 4663 N2 = ARA II 4859 N3 = ACC 2178 N4 no ATH treatment = 21,974 N5 Other antihypertensive = 4068 Death risk N1 HR 0.97 IC 0.89–1.06 p = 0.05 Death risk N2 HR 0.98 IC 0.89–1.06 p = 0.05 Compared both with ACC | Hazard Ratio Mortality | ACEI and ARA II are not associated with an increased or decreased risk of mortality compared to ACC. / YES | 2a/B |
| Zhang et al., 2020 (China) [45] | Cohorts retrospectives | n = 3611; PV = 1128 (31.23%); HBP = 525 (47%); Age = 64; HBP = 1128 (31%); Heart Disease in HBP = 131 (12%); DMT2 in HBP = 200 (18%); Stroke in HBP = 41 (3%); Chronic Obstructive Lung in HBP = 6 (0.5%) | They compare ACEI and ARAII versus not taking them regardless of being hospitalized | N1 = ACEI/ARAII = 188 N2 = no ACEI/ARAII = 940 Mortality N1 vs. N2 HR = 0.42 (0.19–0.92) p = 0.03 COVID-19 Mortality Risk N1 vs. N2 HR = 0.37 (0.15–0.89) p = 0.03. Comparison of other antihypertensive drugs Mortality N1 HR = 0.3 (0.12–0.70) p = 0.01 | Hazard Ratio Mortality | ACEI/ARAII in patients hospitalized for COVID-19 with hypertension is associated with lower mortality than all causes and from COVID-19. / NO | 2a/B |
3.2. Risk Association to the Use of ACEI/ARAII
3.3. Risk Association to the Use of ACEI vs. ARAII
3.4. Risk Association to the Use of ACEI/ARAII vs. Calcium Antagonists (CA) in COVID
3.5. Risk Association to the Use of ACEI/ARAII vs. Diuretics in COVID
3.6. ACEI/ARAII Complications in COVID
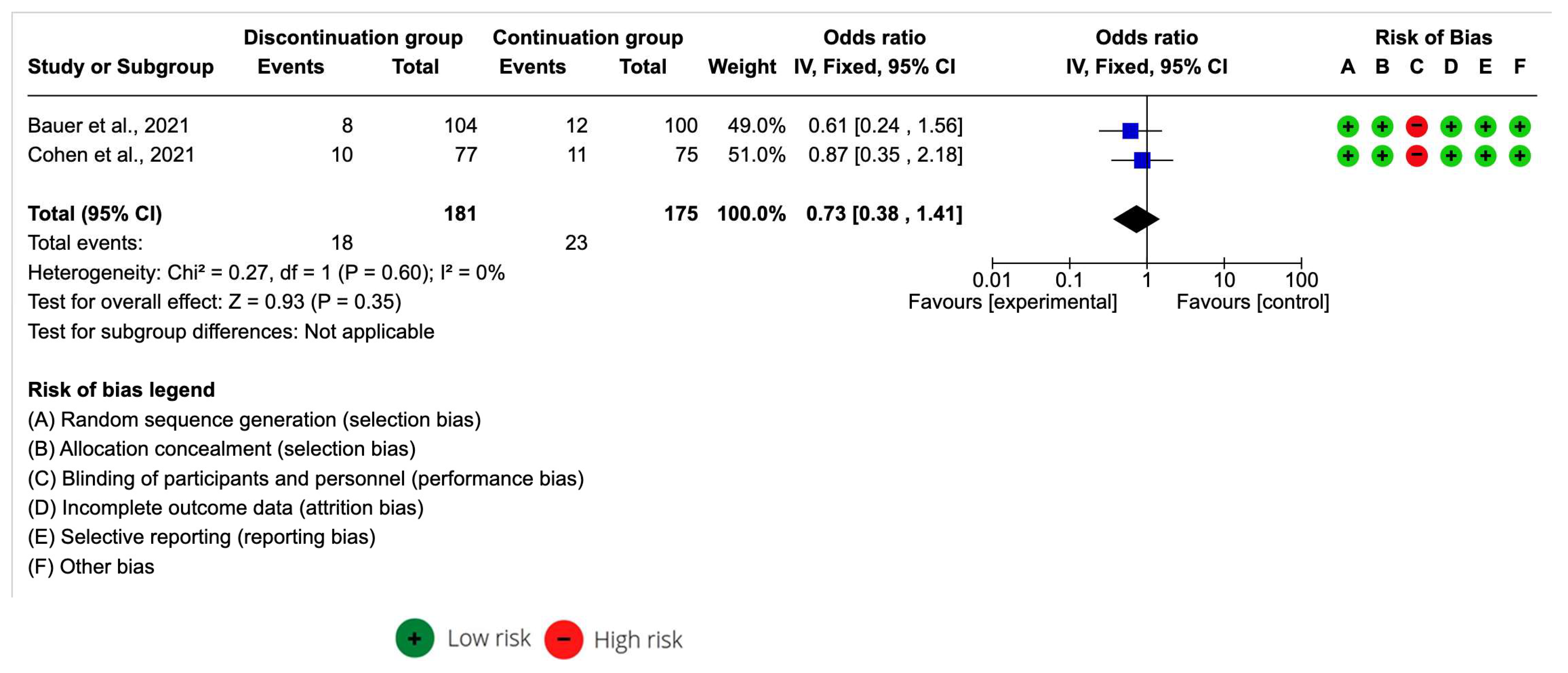
3.7. Meta-Analysis of ACEI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Campbell, N.R.; Burnens, M.P.; Whelton, P.K.; Angell, S.Y.; Jaffe, M.G.; Cohn, J.; Brito, A.E.; Irazola, V.; Brettler, J.W.; Roccella, E.J.; et al. 2021 World Health Organization guideline on pharmacological treatment of hypertension: Policy implications for the Region of the Americas [Directrices de la Organización Mundial de la Salud del 2021 sobre el tratamiento farmacológico de la hipertensión: Implicaciones de política para la Región de las Américas]. Rev. Pan Am. Salud Publica 2022, 46, 1. [Google Scholar] [CrossRef]
- Zhou, B.; Carrillo-Larco, R.M.; Danaei, G.; Riley, L.M.; Paciorek, C.J.; Stevens, G.A.; Gregg, E.W.; Solomon, B.; Singleton, R.F.K.; Iurilli, M.L.C.; et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Lisy, K.; Campbell, J.M.; Tufanaru, C.; Moola, S.; Lockwood, C. The prevalence of disability among people with cancer, cardiovascular disease, chronic respiratory disease and/or diabetes: A systematic review. Int. J. Evid. Based Healthc. 2018, 16, 154–166. [Google Scholar] [CrossRef]
- Bueno, H.; Moura, B.; Lancellotti, P.; Bauersachs, J. The year in cardiovascular medicine 2020: Heart failure and cardiomyopathies. Eur. Heart J. 2021, 42, 657–670. [Google Scholar] [CrossRef]
- Yang, Y.S.; Pei, Y.H.; Gu, Y.Y.; Zhu, J.F.; Yu, P.; Chen, X.H. Association between short-term exposure to ambient air pollution and heart failure: An updated systematic review and meta-analysis of more than 7 million participants. Front. Public Health 2023, 10, 948765. [Google Scholar] [CrossRef]
- Gordon, J.; Miller, G.C.; Britt, H. What are chronic conditions that contribute to multimorbidity? Aust. J. Gen. Pract. 2018, 47, 21–22. [Google Scholar] [CrossRef]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Ott, C.; Schmieder, R.E. Diagnosis and treatment of arterial hypertension 2021. Kidney Int. 2022, 101, 36–46. [Google Scholar] [CrossRef]
- Adler, A.; Agodoa, L.; Algra, A.; Asselbergs, F.W.; Beckett, N.S.; Berge, E.; Black, H.; Brouwers, F.P.J.; Brown, M.; Bulpitt, C.J.; et al. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: An individual participant-level data meta-analysis. Lancet 2021, 397, 1625–1636. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069, Erratum in: JAMA 2021, 325, 1113. [Google Scholar] [CrossRef]
- Kollias, A.; Foukarakis, E.; Karakousis, K.; HYPEDIA Study Group; Stergiou, G.S. Implementation of the 2018 ESC/ESH Guidelines for the management of hypertension in primary care: The HYPEDIA study. J. Hum. Hypertens. 2022; in press. [Google Scholar] [CrossRef]
- Letko, M.; Marzi, A.; Munster, V. Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses. Nat. Microbiol. 2020, 5, 562–569. [Google Scholar] [CrossRef] [Green Version]
- Guidance on Routine Immunization Services during COVID-19 Pandemic in the WHO European Region, 20 March 2020. Available online: https://www.who.int/europe/publications/i/item/WHO-EURO-2020-1059-40805-55114 (accessed on 13 July 2022).
- Weekly Epidemiological Update on COVID-19—13 July 2022. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---13-july-2022 (accessed on 13 July 2022).
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Wang, J.; Zhao, H.; An, Y. ACE2 Shedding and the Role in COVID-19. Front. Cell. Infect. Microbiol. 2021, 11, 1422. [Google Scholar] [CrossRef]
- Águila Gordo, D.; Martínez del Rio, J.; Piqueras Flores, J. Changes in antihypertensive treatment in surviving patients SARS-CoV-2 respiratory infection and its cardiovascular impact after one year of follow-up. Med. Clin. 2022, 158, 196–197, (In English, Spanish). [Google Scholar] [CrossRef]
- Oran, D.P.; Topol, E.J. The Proportion of SARS-CoV-2 Infections That Are Asymptomatic: A Systematic Review. Ann. Intern. Med. 2021, 174, 655–662. [Google Scholar] [CrossRef]
- Luis, J.; Rubio, C.; Millán, I.A.; Moreno Higueras, M.; Mu, L.M.; Medina, M.; López López, M.; Ceballos Torres, A. Revista Española de Geriatría y Gerontología. Tratamiento y evolución del síndrome de tormenta de citoquinas asociados a infección por SARS-CoV-2 en pacientes octogenarios. Rev. Esp. Geriatr. Gerontol. 2020, 55, 286–288. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Warren-Gash, C.; Davidson, J.A.; Strongman, H.; Herrett, E.; Smeeth, L.; Breuer, J.; Banerjee, A. Severe COVID-19 outcomes by cardiovascular risk profile in England in 2020: A population-based cohort study. Lancet Reg. Health Eur. 2023, 27, 100604. [Google Scholar] [CrossRef]
- Underlying Medical Conditions Associated with Higher Risk for Severe COVID-19: Information for Healthcare Professionals|CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/underlyingconditions.html (accessed on 14 July 2022).
- COVID-19 Forecasting Team. Variation in the COVID-19 infection-fatality ratio by age, time, and geography during the pre-vaccine era: A systematic analysis. Lancet 2022, 399, 1469–1488. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H. Explanation of the 2011 Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence (Background Document). Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 30 October 2021).
- Bauer, A.; Schreinlechner, M.; Sappler, N.; Dolejsi, T.; Tilg, H.; Aulinger, B.A.; Weiss, G.; Bellmann-Weiler, R.; Adolf, C.; Wolf, D.; et al. Discontinuation versus continuation of renin-angiotensin-system inhibitors in COVID-19 (ACEI-COVID): A prospective, parallel group, randomised, controlled, open-label trial. Lancet Respir. Med. 2021, 9, 863–872. [Google Scholar] [CrossRef]
- Bean, D.M.; Kraljevic, Z.; Searle, T.; Bendayan, R.; Kevin, O.; Pickles, A.; Folarin, A.; Roguski, L.; Noor, K.; Shek, A.; et al. Angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers are not associated with severe COVID-19 infection in a multi-site UK acute hospital trust. Eur. J. Heart Fail. 2020, 22, 967–974. [Google Scholar] [CrossRef]
- Cohen, J.B.; Hanff, T.C.; William, P.; Sweitzer, N.; Rosado-Santander, N.R.; Medina, C.; Andrade-Villanueva, J.F.; Barbagelata, A.; Cristodulo-Cortez, R.; Díaz Cucho, O.; et al. Continuation versus discontinuation of renin–angiotensin system inhibitors in patients admitted to hospital with COVID-19: A prospective, randomised, open-label trial. Lancet Respir. Med. 2021, 9, 275–284. [Google Scholar] [CrossRef]
- De Spiegeleer, A.; Bronselaer, A.; Teo, J.T.; Byttebier, G.; De Tré, G.; Belmans, L.; Dobson, R.; Wynendaele, E.; Van De Wiele, C.; Vandaele, F.; et al. The Effects of ARBs, ACEis, and Statins on Clinical Outcomes of COVID-19 Infection Among Nursing Home Residents. J. Am. Med. Dir. Assoc. 2020, 21, 909–914.e2. [Google Scholar] [CrossRef]
- ElAbd, R.; AlTarrah, D.; AlYouha, S.; Bastaki, H.; Almazeedi, S.; Al-Haddad, M.; Jamal, M.; AlSabah, S. Angiotensin-Converting Enzyme (ACE) Inhibitors and Angiotensin Receptor Blockers (ARB) Are Protective against ICU Admission and Mortality for Patients with COVID-19 Disease. Front. Med. 2021, 8, 600385. [Google Scholar] [CrossRef]
- Fosbϕl, E.L.; Butt, J.H.; Østergaard, L.; Andersson, C.; Selmer, C.; Kragholm, K.; Schou, M.; Phelps, M.; Gislason, G.H.; Gerds, T.A.; et al. Association of Angiotensin-Converting Enzyme Inhibitor or Angiotensin Receptor Blocker Use with COVID-19 Diagnosis and Mortality. JAMA 2020, 324, 168–177. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Young, D.; Coupland, C.; Channon, K.M.; Tan, P.S.; Harrison, D.A.; Rowan, K.; Aveyard, P.; Pavord, I.D.; Watkinson, P.J. Risk of severe COVID-19 disease with ACE inhibitors and angiotensin receptor blockers: Cohort study including 8.3 million people Special populations. Heart 2020, 106, 1503–1511. [Google Scholar] [CrossRef]
- Jeffery, M.M.; Oliveira, J.; Silva, L.; Bellolio, F.; Garovic, V.D.; Dempsey, T.M.; Limper, A.; Cummins, N.W. Association of outpatient use of renin–angiotensin–aldosterone system blockers on outcomes of acute respiratory illness during the COVID-19 pandemic: A cohort study. BMJ Open 2022, 12, e060305. [Google Scholar] [CrossRef]
- Lopes, R.D.; Macedo, A.V.S.; De Barros, E.; Silva, P.G.M.; Moll-Bernardes, R.J.; Dos Santos, T.M.; Mazza, L.; Feldman, A.; D’Andréa Saba Arruda, G.; De Albuquerque, D.C.; et al. Effect of Discontinuing vs Continuing Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers on Days Alive and Out of the Hospital in Patients Admitted With COVID-19: A Randomized Clinical Trial. JAMA 2021, 325, 254–264. [Google Scholar] [CrossRef]
- Mancia, G.; Rea, F.; Ludergnani, M.; Apolone, G.; Corrao, G. Renin-Angiotensin-Aldosterone System Blockers and the Risk of COVID-19. N. Engl. J. Med. 2020, 382, 2431–2440. [Google Scholar] [CrossRef]
- Mazzoni, T.; Maraia, Z.; Ruggeri, B.; Polidori, C.; Micioni di Bonaventura, M.V.; Armillei, L.; Pomilio, I.; Mazzoni, I. Sartans and ACE Inhibitors: Mortality in Patients Hospitalized with COVID-19. Retrospective Study in Patients on Long-Term Treatment Who Died in the Italian Hospitals of Area Vasta n.5—Marche Region. J. Clin. Med. 2022, 11, 2580. [Google Scholar] [CrossRef]
- Morales, D.R.; Conover, M.M.; You, S.C.; Pratt, N.; Kostka, K.; Duarte-Salles, T.; Fernández-Bertolín, S.; Aragón, M.; DuVall, S.L.; Lynch, K.; et al. Renin–angiotensin system blockers and susceptibility to COVID-19: An international, open science, cohort analysis. Lancet Digit. Health 2021, 3, e98–e114. [Google Scholar] [CrossRef]
- Palazzuoli, A.; Mancone, M.; De Ferrari, G.M.; Forleo, G.; Secco, G.G.; Ruocco, G.M.; D’Ascenzo, F.; Monticone, S.; Paggi, A.; Vicenzi, M.; et al. Antecedent Administration of Angiotensin-Converting Enzyme Inhibitors or Angiotensin II Receptor Antagonists and Survival After Hospitalization for COVID-19 Syndrome. J. Am. Heart Assoc. 2020, 9, e017364. [Google Scholar] [CrossRef]
- Peñalvo, J.L.; Genbrugge, E.; Mertens, E.; Sagastume, D.; Van der Sande, M.A.B.; Widdowson, M.A.; Van Beckhoven, D.; Belgian Collaborative Group on COVID-19 Hospital Surveillance. Insights into the association of ACEIs/ARBs use and COVID-19 prognosis: A multistate modelling study of nationwide hospital surveillance data from Belgium. BMJ Open 2021, 11, e053393. [Google Scholar] [CrossRef]
- Shah, P.; Owens, J.; Franklin, J.; Jani, Y.; Kumar, A.; Doshi, R. Baseline use of angiotensin-converting enzyme inhibitor/AT1blocker and outcomes in hospitalized coronavirus disease 2019 African-American patients. J. Hypertens. 2020, 38, 2537–2541. [Google Scholar] [CrossRef]
- Sharma, A.; Elharram, M.; Afilalo, J.; Flannery, A.; Afilalo, M.; Tselios, C.; Ni, J.; Ezekowitz, J.A.; Cheng, M.P.; Ambrosy, A.P.; et al. A randomized controlled trial of renin-angiotensin-aldosterone system inhibitor management in patients admitted in hospital with COVID-19. Am. Heart J. 2022, 247, 76–89. [Google Scholar] [CrossRef]
- Trifirò, G.; Massari, M.; Da Cas, R.; Menniti Ippolito, F.; Sultana, J.; Crisafulli, S.; Giorgi Rossi, P.; Marino, M.; Zorzi, M.; Bovo, E.; et al. Renin-Angiotensin-Aldosterone System Inhibitors and Risk of Death in Patients Hospitalised with COVID-19: A Retrospective Italian Cohort Study of 43,000 Patients. Drug Saf. 2020, 43, 1297–1308. [Google Scholar] [CrossRef]
- Zhang, P.; Zhu, L.; Cai, J.; Lei, F.; Qin, J.J.; Xie, J.; Liu, Y.M.; Zhao, Y.C.; Huang, X.; Lin, L.; et al. Association of Inpatient Use of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers with Mortality among Patients with Hypertension Hospitalized with COVID-19. Circ. Res. 2020, 126, 1671–1681. [Google Scholar] [CrossRef] [Green Version]
- Makani, H.; Bangalore, S.; Desouza, K.A.; Shah, A.; Messerli, F.H. Efficacy and safety of dual blockade of the renin-angiotensin system: Meta-analysis of randomised trials. BMJ 2013, 346, f360. [Google Scholar] [CrossRef] [Green Version]
- Reindl-Schwaighofer, R.; Hödlmoser, S.; Domenig, O.; Krenn, K.; Eskandary, F.; Krenn, S.; Schörgenhofer, C.; Rumpf, B.; Karolyi, M.; Traugott, M.T.; et al. The systemic renin-angiotensin system in COVID-19. Sci. Rep. 2022, 12, 20117. [Google Scholar] [CrossRef]
- Zhang, S.; Liu, L.; Yang, B.; Li, R.; Luo, J.; Huang, J.; Long, Y.; Huang, Y.; Zhou, J.; Zha, Y.; et al. Clinical characteristics of 134 convalescent patients with COVID-19 in Guizhou, China. Respir. Res. 2020, 21, 314. [Google Scholar] [CrossRef]
- Meng, J.; Xiao, G.; Zhang, J.; He, X.; Ou, M.; Bi, J.; Yang, R.; Di, W.; Wang, Z.; Li, Z.; et al. Renin-angiotensin system inhibitors improve the clinical outcomes of COVID-19 patients with hypertension. Emerg. Microbes Infect. 2020, 9, 757–760. [Google Scholar] [CrossRef]
- Golpe, R.; Pérez-de-Llano, L.A.; Dacal, D.; Guerrero-Sande, H.; Pombo-Vide, B.; Ventura-Valcárcel, P. Risk of severe COVID-19 in hypertensive patients treated with renin-angiotensin-aldosterone system inhibitors. Med. Clin. 2020, 155, 488–490. [Google Scholar] [CrossRef]
- De Abajo, F.J.; Rodríguez-Martín, S.; Lerma, V.; Mejía-Abril, G.; Aguilar, M.; García-Luque, A.; Laredo, L.; Laosa, O.; Centeno-Soto, G.A.; Ángeles Gálvez, M.; et al. Use of renin-angiotensin-aldosterone system inhibitors and risk of COVID-19 requiring admission to hospital: A case-population study. Lancet 2020, 395, 1705–1714. [Google Scholar] [CrossRef]
- Vaduganathan, M.; Vardeny, O.; Michel, T.; McMurray, J.J.V.; Pfeffer, M.A.; Solomon, S.D. Renin–Angiotensin–Aldosterone System Inhibitors in Patients with COVID-19. N. Engl. J. Med. 2020, 382, 1653–1659. [Google Scholar] [CrossRef]
- Yoshihara, F.; Ohtsu, H.; Nakai, M.; Tsuzuki, S.; Hayakawa, K.; Terada, M.; Matsunaga, N.; Yasuda, S.; Ogawa, H.; Ohmagari, N. Renin-angiotensin system blocker and the COVID-19 aggravation in patients with hypertension, diabetes, renal failure, Cerebro-cardiovascular disease, or pulmonary disease: Report by the COVID-19 Registry Japan. J. Cardiol. 2022, 80, 292–297. [Google Scholar] [CrossRef]
- Puskarich, M.A.; Ingraham, N.E.; Merck, L.H.; Driver, B.E.; Wacker, D.A.; Black, L.P.; Jones, A.E.; Fletcher, C.V.; South, A.M.; Murray, T.A.; et al. Efficacy of Losartan in Hospitalized Patients With COVID-19-Induced Lung Injury: A Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e222735. [Google Scholar] [CrossRef]
- Loader, J.; Taylor, F.C.; Lampa, E.; Sundström, J. Renin-Angiotensin Aldosterone System Inhibitors and COVID-19: A Systematic Review and Meta-Analysis Revealing Critical Bias Across a Body of Observational Research. J. Am. Heart Assoc. 2022, 11, 25289. [Google Scholar] [CrossRef]
- Kumar, S.; Nikravesh, M.; Chukwuemeka, U.; Randazzo, M.; Flores, P.; Choday, P.; Raja, A.; Aseri, M.; Shivang, S.; Chaudhuri, S.; et al. Safety of ACEi and ARB in COVID-19 management: A retrospective analysis. Clin. Cardiol. 2022, 45, 759–766. [Google Scholar] [CrossRef]
- Job, R.; Abdul Qader, M.; Torres, P.; Al Abbasi, B.; Dewaswala, N.; Abdallah, A.; Chen, K.; Pino, J.E.; Chait, R.D. Renin-Angiotensin System Blocker in COVID-19. A Single Center Study. J. Cardiovasc. Pharmacol. 2022, 79, 311–314. [Google Scholar] [CrossRef]
- Liu, Q.; Fu, W.; Zhu, C.J.; Ding, Z.H.; Dong, B.B.; Sun, B.Q.; Chen, R.C. Effect of continuing the use of renin-angiotensin system inhibitors on mortality in patients hospitalized for coronavirus disease 2019: A systematic review, meta-analysis, and meta-regression analysis. BMC Infect. Dis. 2023, 23, 53. [Google Scholar] [CrossRef]
- Yin, J.; Wang, C.; Song, X.; Li, X.; Miao, M. Effects of Renin-Angiotensin System Inhibitors on Mortality and Disease Severity of COVID-19 Patients: A Meta-analysis of Randomized Controlled Trials. Am. J. Hypertens. 2022, 35, 462–469. [Google Scholar] [CrossRef]
- Flack, J.M.; Adekola, B. Blood pressure and the new ACC/AHA hypertension guidelines. Trends Cardiovasc. Med. 2020, 30, 160–164. [Google Scholar] [CrossRef]
- Al-Makki, A.; DiPette, D.; Whelton, P.K.; Murad, M.H.; Mustafa, R.A.; Acharya, S.; Beheiry, H.M.; Champagne, B.; Connell, K.; Cooney, M.T.; et al. Hypertension Pharmacological Treatment in Adults: A World Health Organization Guideline Executive Summary. Hypertension 2022, 79, 293–301. [Google Scholar] [CrossRef]
- Chan, C.K.; Huang, Y.S.; Liao, H.W.; Tsai, I.J.; Sun, C.Y.; Pan, H.C.; Chueh, J.S.; Wang, J.T.; Wu, V.C.; Chu, T.S.; et al. Renin-Angiotensin-Aldosterone System Inhibitors and Risks of Severe Acute Respiratory Syndrome Coronavirus 2 Infection: A Systematic Review and Meta-Analysis. Hypertension 2020, 76, 1563–1571. [Google Scholar] [CrossRef]
- Xiong, S.; Liu, L.; Lin, F.; Shi, J.; Han, L.; Liu, H.; He, L.; Jiang, Q.; Wang, Z.; Fu, W.; et al. Clinical characteristics of 116 hospitalized patients with COVID-19 in Wuhan, China: A single-centered, retrospective, observational study. BMC Infect. Dis. 2020, 20, 787. [Google Scholar] [CrossRef]
- Semenzato, L.; Botton, J.; Drouin, J.; Baricault, B.; Vabre, C.; Cuenot, F.; Penso, L.; Herlemont, P.; Sbidian, E.; Weill, A.; et al. Antihypertensive Drugs and COVID-19 Risk: A Cohort Study of 2 Million Hypertensive Patients. Hypertension 2021, 77, 833–842. [Google Scholar] [CrossRef]
- Wojciechowska, W.; Terleck, M.; Klocek, M.; Pac, A.; Olszanecka, A.; Stolarz-Skrzypek, K.; Jastrzębski, M.; Jankowski, P.; Ostrowska, A.; Drożdż, T.; et al. Impact of Arterial Hypertension and Use of Antihypertensive Pharmacotherapy on Mortality in Patients Hospitalized due to COVID-19: The CRACoV-HHS Study. Hypertension 2022, 79, 2601–2610. [Google Scholar] [CrossRef]
- Palazzuoli, A.; Tecson, K.M.; Vicenzi, M.; D’Ascenzo, F.; De Ferrari, G.M.; Monticone, S.; Secco, G.G.; Tavazzi, G.; Forleo, G.; Severino, P.; et al. Usefulness of Combined Renin-Angiotensin System Inhibitors and Diuretic Treatment In Patients Hospitalized with COVID-19. Am. J. Cardiol. 2022, 167, 133–138. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}

| Study | Question 1 | Question 2 | Question 3 |
|---|---|---|---|
| Bean et al., 2020 [29] | Yes | Yes | Yes |
| De Spiegeleer et al., 2020 [31] | Yes | Yes | Yes |
| Elabd et al., 2021 [32] | Yes | Yes | Yes |
| Fosbϕl et al., 2020 [33] | Yes | Yes | Yes |
| Hippisley-Cox et al., 2020 [34] | Yes | Yes | Yes |
| Jeffery et al., 2022 [35] | Yes | Yes | Yes |
| Mancia et al., 2020 [37] | Yes | Yes | Yes |
| Mazzoni et al., 2022 [38] | Yes | Yes | Yes |
| Morales et al., 2021 [39] | Yes | Yes | Yes |
| Palazzuoli et al., 2020 [40] | Yes | Yes | Yes |
| Peñalvo et al., 2021 [41] | Yes | Yes | Yes |
| Sha et al., 2020 [42] | Yes | Yes | Yes |
| Trifiró et al., 2020 [44] | Yes | Yes | Yes |
| Zhang et al., 2020 [45] | Yes | Yes | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quesada-Caballero, M.; Carmona-García, A.; Chami-Peña, S.; Albendín-García, L.; Membrive-Jiménez, C.; Romero-Béjar, J.L.; Cañadas-De la Fuente, G.A. COVID-19 and the Use of Angiotensin II Receptor Blockers in Older Chronic Hypertensive Patients: Systematic Review and Meta-Analysis. Medicina 2023, 59, 1200. https://doi.org/10.3390/medicina59071200
Quesada-Caballero M, Carmona-García A, Chami-Peña S, Albendín-García L, Membrive-Jiménez C, Romero-Béjar JL, Cañadas-De la Fuente GA. COVID-19 and the Use of Angiotensin II Receptor Blockers in Older Chronic Hypertensive Patients: Systematic Review and Meta-Analysis. Medicina. 2023; 59(7):1200. https://doi.org/10.3390/medicina59071200
Chicago/Turabian StyleQuesada-Caballero, Miguel, Ana Carmona-García, Sara Chami-Peña, Luis Albendín-García, Cristina Membrive-Jiménez, José L. Romero-Béjar, and Guillermo A. Cañadas-De la Fuente. 2023. "COVID-19 and the Use of Angiotensin II Receptor Blockers in Older Chronic Hypertensive Patients: Systematic Review and Meta-Analysis" Medicina 59, no. 7: 1200. https://doi.org/10.3390/medicina59071200