
A Comprehensive Analysis of the Radiation Exposure and the Diagnostic Benefit of PanCT in Pediatric Cases with Multiple Trauma

Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jindal, A.; Velmahos, G.C.; Rofougaran, R. Computed tomography for evaluation of mild to moderate pediatric trauma: Are we overusing it? World J. Surg. 2002, 26, 13. [Google Scholar] [CrossRef] [PubMed]
- Çorbacıoğlu, Ş.K.; Aksel, G. Whole body computed tomography in multi trauma patients: Review of the current literature. Turk. J. Emerg. Med. 2018, 18, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Scaife, E.R.; Rollins, M.D. (Eds.) Managing radiation risk in the evaluation of the pediatric trauma patient. In Seminars in Pediatric Surgery; WB Saunders: Philadelphia, PA, USA, 2010. [Google Scholar]
- Shah, N.B.; Platt, S.L. ALARA: Is there a cause for alarm? Reducing radiation risks from computed tomography scanning in children. Curr. Opin. Pediatr. 2008, 20, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Nenot, J.-C.; Brenot, J.; Laurier, D.; Rannou, A.; Thierry, D. ICRP Publication 103: The 2007 Recommendations of the International Commission on Radiological Protection; ICRP: Ottawa, ON, Canada, 2009. [Google Scholar]
- International Commission on Radiological Protection. Recommendations of the International Commission on Radiological Protection: Adopted January 17, 1977; International Commission on Radiological Protection (ICRP): Ottawa, ON, Canada, 1977. [Google Scholar]
- Abuelhia, E.; Tajaldeen, A.; Alghamdi, A.; Mabrouk, O.; Aluraik, W.; Msmar, A.; Elsadig, M.; Osman, E.; Al-Othman, A.; Alghamdi, S.; et al. Evaluating Effective Dose: A Comparison of Methods Based on Organ Dose Calculations versus Dose-Length Product and Monte Carlo Simulation. Appl. Sci. 2022, 12, 6691. [Google Scholar] [CrossRef]
- Zalis, M.E.; Barish, M.A.; Choi, J.R.; Dachman, A.H.; Fenlon, H.M.; Ferrucci, J.T.; Glick, S.N.; Laghi, A.; Macari, M.; McFarland, E.G.; et al. CT colonography reporting and data system: A consensus proposal. Radiology 2005, 236, 3–9. [Google Scholar] [CrossRef]
- Kim, P.K.; Zhu, X.; Houseknecht, E.; Nickolaus, D.; Mahboubi, S.; Nance, M.L. Effective radiation dose from radiologic studies in pediatric trauma patients. World J. Surg. 2005, 29, 1557–1562. [Google Scholar] [CrossRef]
- Woosley, C.R.; Mayes, T.C. (Eds.) The pediatric patient and thoracic trauma. In Seminars in Thoracic and Cardiovascular Surgery; WB Saunders: Philadelphia, PA, USA, 2008. [Google Scholar]
- Gupta, M.; Schriger, D.L.; Hiatt, J.R.; Cryer, H.G.; Tillou, A.; Hoffman, J.R.; Baraff, L.J. Selective use of computed tomography compared with routine whole body imaging in patients with blunt trauma. Ann. Emerg. Med. 2011, 58, 407–416.e15. [Google Scholar] [CrossRef]
- Bedry, T.; Tadele, H. Pattern and outcome of pediatric traumatic brain injury at hawassa university comprehensive specialized hospital, southern Ethiopia: Observational cross-sectional study. Emerg. Med. Int. 2020, 2020, 1965231. [Google Scholar] [CrossRef] [Green Version]
- Strait, L.; Sussman, R.; Ata, A.; Edwards, M.J. Utilization of CT imaging in minor pediatric head, thoracic, and abdominal trauma in the United States. J. Pediatr. Surg. 2020, 55, 1766–1772. [Google Scholar] [CrossRef]
- Aoki, M.; Abe, T.; Saitoh, D.; Oshima, K. Epidemiology, patterns of treatment, and mortality of pediatric trauma patients in Japan. Sci. Rep. 2019, 9, 917. [Google Scholar] [CrossRef] [Green Version]
- Sharma, M.; Lahoti, B.; Khandelwal, G.; Mathur, R.; Sharma, S.; Laddha, A. Epidemiological trends of pediatric trauma: A single-center study of 791 patients. J. Indian Assoc. Pediatr. Surg. 2011, 16, 88. [Google Scholar] [CrossRef] [PubMed]
- Bliss, D.; Silen, M. Pediatric thoracic trauma. Crit. Care Med. 2002, 30, S409–S415. [Google Scholar] [CrossRef] [PubMed]
- Lynch, T.; Kilgar, J.; Al Shibli, A. Pediatric abdominal trauma. Curr. Pediatr. Rev. 2018, 14, 59–63. [Google Scholar] [CrossRef]
- Miele, V.; Piccolo, C.L.; Trinci, M.; Galluzzo, M.; Ianniello, S.; Brunese, L. Diagnostic imaging of blunt abdominal trauma in pediatric patients. Radiol. Med. 2016, 121, 409–430. [Google Scholar] [CrossRef]
- Feliz, A.; Shultz, B.; McKenna, C.; Gaines, B.A. Diagnostic and therapeutic laparoscopy in pediatric abdominal trauma. J. Pediatr. Surg. 2006, 41, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Tilford, J.M.; Simpson, P.M.; Yeh, T.S.; Lensing, S.; Aitken, M.E.; Green, J.W.; Harr, J.; Fiser, D.H. Variation in therapy and outcome for pediatric head trauma patients. Crit. Care Med. 2001, 29, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Köksal, Ö.; Özeren, G.; Yenice, H.; Çildir, E. Is Cranial Computerized Tomography Really Necessary for Infants with Minor Head Trauma? Eurasian J. Emerg. Med. 2011, 10, 56. [Google Scholar] [CrossRef]
- Haydel, M.J.; Shembekar, A.D. Prediction of intracranial injury in children aged five years and older with loss of consciousness after minor head injury due to nontrivial mechanisms. Ann. Emerg. Med. 2003, 42, 507–514. [Google Scholar] [CrossRef]
- Türedi, S.; Hasanbasoglu, A.; Gunduz, A.; Yandi, M. Clinical decision instruments for CT scan in minor head trauma. J. Emerg. Med. 2008, 34, 253–259. [Google Scholar] [CrossRef]
- Hall, E.J. Lessons we have learned from our children: Cancer risks from diagnostic radiology. Pediatr. Radiol. 2002, 32, 700–706. [Google Scholar] [CrossRef]
- Hall, E.; Brenner, D. Cancer risks from diagnostic radiology. Br. J. Radiol. 2008, 81, 362–378. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, J.A.; Stone, M.E.; Reddy, S.H.; Silver, E.J. Association of whole-body computed tomography with mortality risk in children with blunt trauma. JAMA Pediatr. 2018, 172, 542–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flood, R.G.; Mooney, D.P. Rate and prediction of traumatic injuries detected by abdominal computed tomography scan in intubated children. J. Trauma 2006, 61, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Sorantin, E.; Weissensteiner, S.; Hasenburger, G.; Riccabona, M. CT in children–dose protection and general considerations when planning a CT in a child. Eur. J. Radiol. 2013, 82, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Streck, C.J., Jr.; Jewett, B.M.; Wahlquist, A.H.; Gutierrez, P.S.; Russell, W.S. Evaluation for intra-abdominal injury in children after blunt torso trauma: Can we reduce unnecessary abdominal computed tomography by utilizing a clinical prediction model? J. Trauma Acute Care Surg. 2012, 73, 371–376. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| C-RADS Category | Radiological Findings |
|---|---|
| 1 | Anatomic variations, normal findings |
| 2 | Soft tissue swelling, superficial skin defects |
| 3 | Suspicious radiological findings of focal solid organ contusions suitable for conservative treatment, the presence of suspicious abdominopelvic fluid and traumatic lesions in bone structures that will not require surgery |
| 4 | Intracranial hemorrhage and cerebral contusion, the presence of evident thoracic or abdominopelvic free fluid, solid organ contusions and lacerations, stable or unstable vertebral column fractures, vascular injuries |
| n (%) | ||
|---|---|---|
| Gender | Female | 89 (33.2%) |
| Male | 179 (66.8%) | |
| Trauma Occurrence | Unknown | 84 (31.3%) |
| Non-vehicle traffic accident | 2 (0.7%) | |
| Traffic accident | 85 (31.7%) | |
| Fall | 61 (22.8%) | |
| Forensic Case | 32 (11.9%) | |
| Foreign Body Trauma | 1 (0.4%) | |
| Firearm Injury | 2 (0.7%) | |
| Syncope | 1 (0.4%) | |
| Pathology (C-RADS) | 1 | 182 (67.9%) |
| 2 | 12 (4.5%) | |
| 3 | 16 (6%) | |
| 4 | 58 (21.6%) | |
| Total | 268 (100%) | |
| Mean ± SD 1, Median (min-max) | ||
| Age | 8.81 ± 5.21 8 (1–19) | |
| Effective Dose (mSv) | 18.14 ± 10.44 16.58 (0–87.21) | |
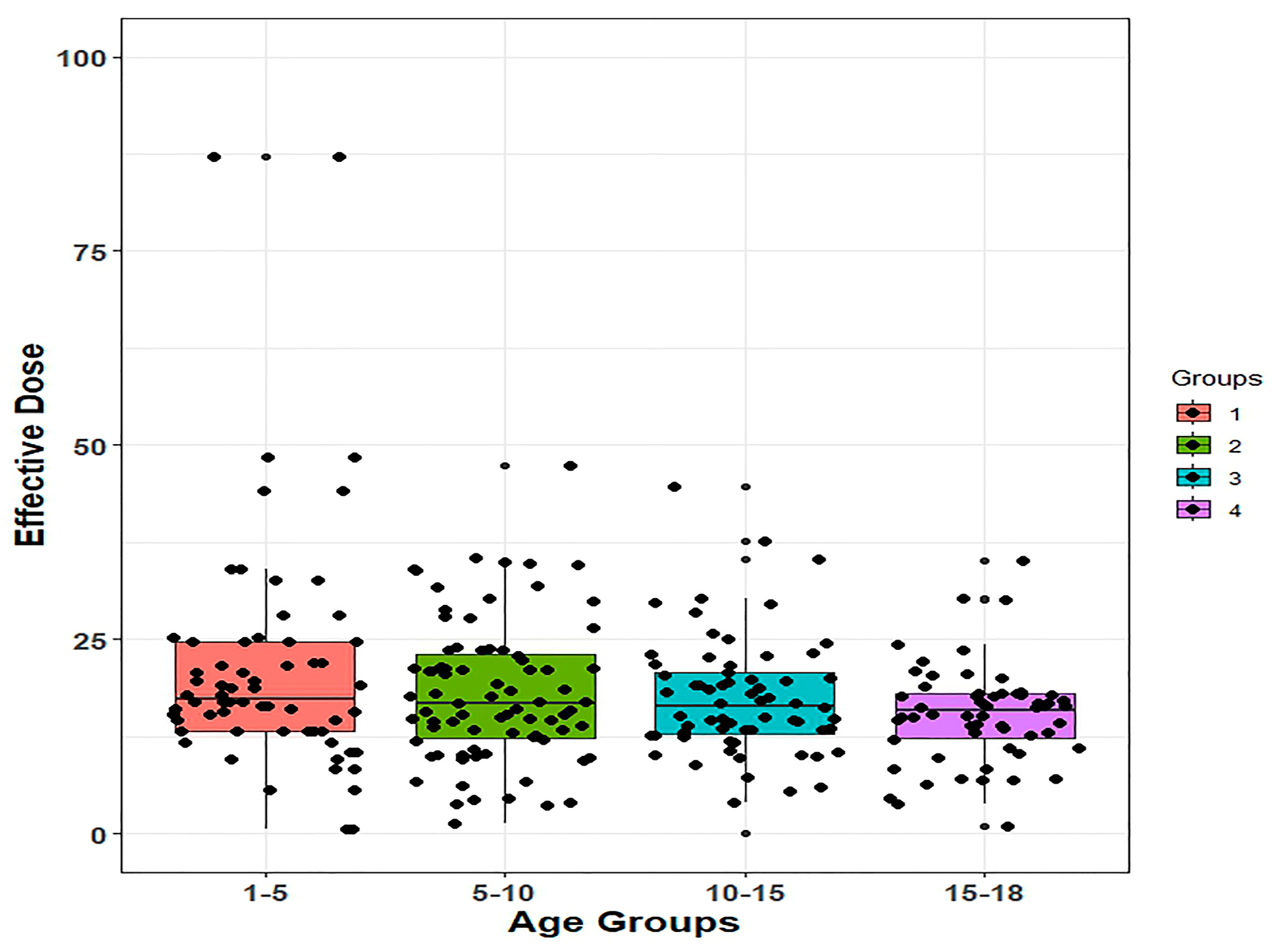
| Effective Doses (mSv) (n = 268) | p Value | Post-Hoc p Value | ||
|---|---|---|---|---|
| Age groups | 1–5 age (1) | 21.45 ± 15.53 | 0.011 | 1–2: 0.441 1–3: 0.246 1–4: 0.024 2–3: 0.944 2–4: 0.138 3–4: 0.375 |
| 5–10 age (2) | 18.16 ± 9.038 | |||
| 10–15 age (3) | 17.39 ± 7.845 | |||
| 15–18 age (4) | 15.33 ± 6.316 |
| Pathology (C-RADS) | Total | p Value | Post-Hoc p Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||||||
| Age groups | 1–5 age (1) | n | 44 | 0 | 2 | 18 | 64 | 0.028 | 1–2: 0.029 1–3: 0.016 1–4: 0.726 2–3: 0.075 2–4: 0.306 3–4: 0.158 |
| % | 68.8% | 0% | 3.1% | 28.1% | 100% | ||||
| 5–10 age (2) | n | 61 | 4 | 5 | 10 | 80 | |||
| % | 76.3% | 5% | 6.3% | 12.5% | 100% | ||||
| 10–15 age (3) | n | 37 | 7 | 6 | 16 | 66 | |||
| % | 56.1% | 10.6% | 9.1% | 24.2% | 100% | ||||
| 15–18 age (4) | n | 40 | 1 | 3 | 14 | 58 | |||
| % | 69% | 1.7% | 5.2% | 24.1% | 100% | ||||
| Total | n | 182 | 12 | 16 | 58 | 268 | |||
| % | 67.9% | 4.5% | 6.0% | 21.6% | 100% | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Komut, S.; Afşarlar, Ç.E. A Comprehensive Analysis of the Radiation Exposure and the Diagnostic Benefit of PanCT in Pediatric Cases with Multiple Trauma. Medicina 2023, 59, 1228. https://doi.org/10.3390/medicina59071228
Komut S, Afşarlar ÇE. A Comprehensive Analysis of the Radiation Exposure and the Diagnostic Benefit of PanCT in Pediatric Cases with Multiple Trauma. Medicina. 2023; 59(7):1228. https://doi.org/10.3390/medicina59071228
Chicago/Turabian StyleKomut, Seval, and Çağatay Evrim Afşarlar. 2023. "A Comprehensive Analysis of the Radiation Exposure and the Diagnostic Benefit of PanCT in Pediatric Cases with Multiple Trauma" Medicina 59, no. 7: 1228. https://doi.org/10.3390/medicina59071228