
Epidemiology and Outcome of Acute Appendicitis during and before the COVID-19 Pandemic: A Retrospective Single-Center Analysis

Abstract
:1. Introduction
2. Materials and Methods
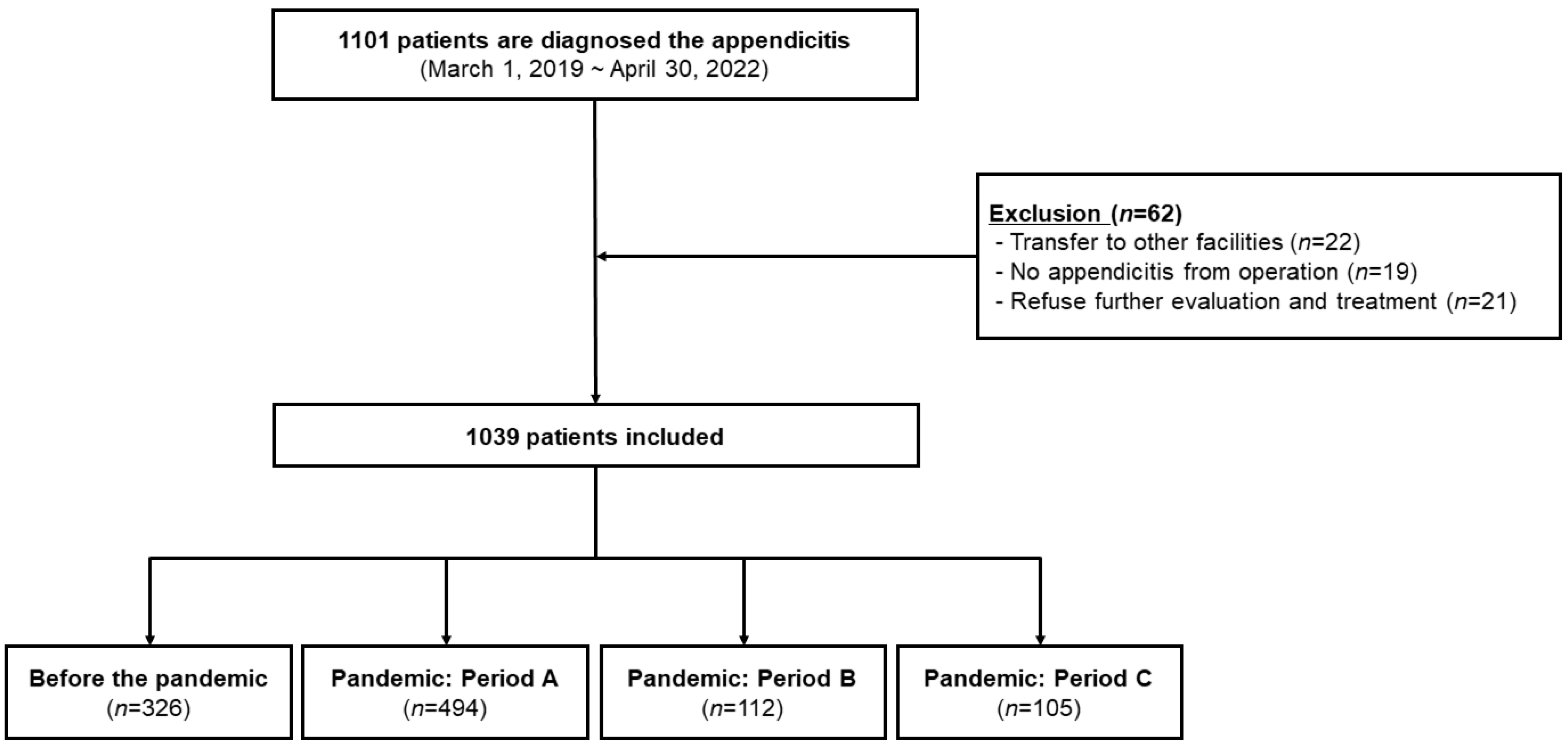
2.1. Study Design and Population
2.2. During and before the Pandemic Period, and the Changed Environment in the Emergency Room during the Pandemic
2.3. Data Collection and Outcome Measurement
2.4. Statistical Analysis
2.5. Ethics Statement
3. Results
3.1. Population and Demographics
3.2. Outcomes
3.3. Influencing Factors for Incidence of Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blumenthal, D.; Fowler, E.J.; Abrams, M.; Collins, S.R. COVID-19—Implications for the Health Care System. N. Engl. J. Med. 2020, 383, 1483–1488. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Ahn, C.; Namgung, M. Comparative Evaluation of the Prognosis of Septic Shock Patients from Before to After the Onset of the COVID-19 Pandemic: A Retrospective Single-Center Clinical Analysis. J. Pers. Med. 2022, 12, 10103. [Google Scholar] [CrossRef]
- Ahn, J.Y.; Ryoo, H.W.; Cho, J.W.; Kim, J.H.; Lee, S.H.; Jang, T.C. Impact of the COVID-19 outbreak on adult out-of-hospital cardiac arrest outcomes in Daegu, South Korea: An observational study. Clin. Exp. Emerg. Med. 2021, 8, 137–144. [Google Scholar] [CrossRef]
- Furnica, C.; Chistol, R.O.; Chiran, D.A.; Stan, C.I.; Sargu, G.D.; Girlescu, N.; Tinica, G. The Impact of the Early COVID-19 Pandemic on ST-Segment Elevation Myocardial Infarction Presentation and Outcomes-A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 588. [Google Scholar] [CrossRef]
- Ishaque, N.; Butt, A.J.; Kamtchum-Tatuene, J.; Nomani, A.Z.; Razzaq, S.; Fatima, N.; Vekhande, C.; Nair, R.; Akhtar, N.; Khan, K.; et al. Trends in Stroke Presentations before and during the COVID-19 Pandemic: A Meta-Analysis. J. Stroke 2022, 24, 65–78. [Google Scholar] [CrossRef] [PubMed]
- Lim, Z.J.; Ponnapa Reddy, M.; Afroz, A.; Billah, B.; Shekar, K.; Subramaniam, A. Incidence and outcome of out-of-hospital cardiac arrests in the COVID-19 era: A systematic review and meta-analysis. Resuscitation 2020, 157, 248–258. [Google Scholar] [CrossRef]
- Kim, J.H.; Ahn, C.; Namgung, M. Epidemiology and Outcome of Out-of-Hospital Cardiac Arrests during the COVID-19 Pandemic in South Korea: A Systematic Review and Meta-Analyses. Yonsei Med. J. 2022, 63, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Ahn, C.; Park, Y.; Won, M. Comparison of out-of-hospital cardiac arrest during the COVID-19 pandemic with those before the pandemic: An updated systematic review and meta-analysis. Front. Public Health 2023, 11, 1180511. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Milanović, K.; Veršić, A.B.; Pasini, M.; Divković, D.; Pavlović, O.; Lučev, J.; Žufić, V. Is there an increased incidence of orchiectomy in pediatric patients with acute testicular torsion during COVID-19 pandemic?—A retrospective multicenter study. J. Pediatr. Urol. 2021, 17, 479.e1–479.e6. [Google Scholar] [CrossRef]
- Obamiro, E.; Trivedi, R.; Ahmed, N. Changes in trends of orthopedic services due to the COVID-19 pandemic: A review. World J. Orthop. 2022, 13, 955–968. [Google Scholar] [CrossRef]
- Köhler, F.; Müller, S.; Hendricks, A.; Kastner, C.; Reese, L.; Boerner, K.; Flemming, S.; Lock, J.F.; Germer, C.T.; Wiegering, A. Changes in appendicitis treatment during the COVID-19 pandemic—A systematic review and meta-analysis. Int. J. Surg. 2021, 95, 106148. [Google Scholar] [CrossRef] [PubMed]
- English, W.; Habib Bedwani, N.; Smith, C.; Doganay, E.; Marsden, M.; Muse, S.; Mak, W.K.; Chana, M.; Eves, J.; Shatkar, V. Suspected appendicitis and COVID-19, a change in investigation and management—A multicentre cohort study. Langenbecks Arch. Surg. 2021, 406, 357–365. [Google Scholar] [CrossRef]
- Fisher, J.C.; Tomita, S.S.; Ginsburg, H.B.; Gordon, A.; Walker, D.; Kuenzler, K.A. Increase in Pediatric Perforated Appendicitis in the New York City Metropolitan Region at the Epicenter of the COVID-19 Outbreak. Ann. Surg. 2021, 273, 410–415. [Google Scholar] [CrossRef]
- Slagman, A.; Behringer, W.; Greiner, F.; Klein, M.; Weismann, D.; Erdmann, B.; Pigorsch, M.; Möckel, M. Medizinische notfälle während der COVID-19-pandemie. Dtsch. Arztebl. Int. 2020, 117, 545–552. [Google Scholar]
- Dick, L.; Green, J.; Brown, J.; Kennedy, E.; Cassidy, R.; Othman, S.; Berlansky, M. Changes in emergency general surgery during Covid-19 in Scotland: A prospective cohort study. World J. Surg. 2020, 44, 3590–3594. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (2019-nCoV) Infection Is Suspected: Interim Guidance, 28 January 2020, Geneva. 2020. Available online: https://apps.who.int/iris/handle/10665/330893 (accessed on 3 May 2023).
- Bae, S.J.; Chung, H.S.; Namgung, M.; Choi, Y.H.; Min, J.H.; Lee, D.H. Comparison of the Clinical Process and Outcomes in Patients after Coronavirus Infection 2019 Outbreak. Medicina 2021, 57, 1086. [Google Scholar] [CrossRef]
- Wax, R.S.; Christian, M.D. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can. J. Anaesth. 2020, 67, 568–576. [Google Scholar] [CrossRef]
- Zuo, M.Z.; Huang, Y.G.; Ma, W.H.; Xue, Z.G.; Zhang, J.Q.; Gong, Y.H.; Che, L.; Chinese Society of Anesthesiology Task Force on Airway Management. Expert Recommendations for Tracheal Intubation in Critically ill Patients with Noval Coronavirus Disease 2019. Chin. Med. Sci. J. 2020, 35, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Al-Muharraqi, M.A. Testing recommendation for COVID-19 (SARS-CoV-2) in patients planned for surgery—Continuing the service and ‘suppressing’ the pandemic. Br. J. Oral. Maxillofac. Surg. 2020, 58, 503–505. [Google Scholar] [CrossRef]
- Ribal, M.J.; Cornford, P.; Briganti, A.; Knoll, T.; Gravas, S.; Babjuk, M.; Harding, C.; Breda, A.; Bex, A.; Rassweiler, J.J.; et al. European Association of Urology Guidelines Office Rapid Reaction Group: An Organisation-wide Collaborative Effort to Adapt the European Association of Urology Guidelines Recommendations to the Coronavirus Disease 2019 Era. Eur. Urol. 2020, 78, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Blouhos, K.; Boulas, K.A.; Paraskeva, A.; Triantafyllidis, A.; Nathanailidou, M.; Hatzipourganis, K.; Hatzigeorgiadis, A. Understanding Surgical Risk During COVID-19 Pandemic: The Rationale Behind the Decisions. Front. Surg. 2020, 7, 33. [Google Scholar] [CrossRef]
- de Bock, E.; Filipe, M.D.; Simmermacher, R.K.J.; Kroese, A.C.; Vriens, M.R.; Richir, M.C. Meta-analysis of COVID-19 prevalence during preoperative COVID-19 screening in asymptomatic patients. BMJ Open 2022, 12, e058389. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.W.; Lee, S.H. Impact of COVID-19 on the care of acute appendicitis: A single-center experience in Korea. Ann. Surg. Treat Res. 2021, 101, 240–246. [Google Scholar] [CrossRef]
- Lee, J.F.; Leow, C.K.; Lau, W.Y. Appendicitis in the elderly. ANZ J. Surg. 2000, 70, 593–596. [Google Scholar] [CrossRef]
- Körner, H.; Söndenaa, K.; Söreide, J.A.; Andersen, E.; Nysted, A.; Lende, T.H.; Kjellevold, K.H. Incidence of acute nonperforated and perforated appendicitis: Age-specific and sex-specific analysis. World J. Surg. 1997, 21, 313–317. [Google Scholar] [CrossRef]
- Kirshtein, B.; Perry, Z.H.; Mizrahi, S.; Lantsberg, L. Value of laparoscopic appendectomy in the elderly patient. World J. Surg. 2009, 33, 918–922. [Google Scholar] [CrossRef] [PubMed]
- van Rossem, C.C.; Schreinemacher, M.H.; Treskes, K.; van Hogezand, R.M.; van Geloven, A.A. Duration of antibiotic treatment after appendicectomy for acute complicated appendicitis. Br. J. Surg. 2014, 101, 715–719. [Google Scholar] [CrossRef]
- Li, M.; Wang, H.; Tian, L.; Pang, Z.; Yang, Q.; Huang, T.; Fan, J.; Song, L.; Tong, Y.; Fan, H. COVID-19 vaccine development: Milestones, lessons and prospects. Signal Transduct. Target. Ther. 2022, 7, 146. [Google Scholar] [CrossRef]
- Strasser, Z.H.; Greifer, N.; Hadavand, A.; Murphy, S.N.; Estiri, H. Estimates of SARS-CoV-2 Omicron BA.2 Subvariant Severity in New England. JAMA Network Open 2022, 5, e2238354. [Google Scholar] [CrossRef] [PubMed]
- Cheng, V.C.C.; Ip, J.D.; Chu, A.W.H.; Tam, A.R.; Chan, W.M.; Abdullah, S.M.U.; Chan, B.P.C.; Wong, S.C.; Kwan, M.Y.W.; Chua, G.T. Rapid spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) Omicron subvariant BA. 2 in a single-source community outbreak. Clin. Infect. Dis. 2022, 75, e44–e49. [Google Scholar] [CrossRef] [PubMed]
- Wilms, I.M.; Suykerbuyk-de Hoog, D.E.; de Visser, D.C.; Janzing, H.M. Appendectomy versus antibiotic treatment for acute appendicitis. Cochrane Database Syst. Rev. 2020, 10, Cd008359. [Google Scholar] [CrossRef] [PubMed]
- Bhangu, A.; Søreide, K.; Di Saverio, S.; Assarsson, J.H.; Drake, F.T. Acute appendicitis: Modern understanding of pathogenesis, diagnosis, and management. Lancet 2015, 386, 1278–1287. [Google Scholar] [CrossRef]
- Boserup, B.; McKenney, M.; Elkbuli, A. The impact of the COVID-19 pandemic on emergency department visits and patient safety in the United States. Am. J. Emerg. Med. 2020, 38, 1732–1736. [Google Scholar] [CrossRef] [PubMed]
- Mandeville, K.; Monuteaux, M.; Pottker, T.; Bulloch, B. Effects of Timing to Diagnosis and Appendectomy in Pediatric Appendicitis. Pediatr. Emerg. Care 2015, 31, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Rothrock, S.G.; Pagane, J. Acute appendicitis in children: Emergency department diagnosis and management. Ann. Emerg. Med. 2000, 36, 39–51. [Google Scholar] [CrossRef]
- Brender, J.D.; Marcuse, E.K.; Koepsell, T.D.; Hatch, E.I. Childhood appendicitis: Factors associated with perforation. Pediatrics 1985, 76, 301–306. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Anand, S.; Žuvela, T.; Singh, A.; Križanac, Z.; Krishnan, N. Incidence of Complicated Appendicitis during the COVID-19 Pandemic versus the Pre-Pandemic Period: A Systematic Review and Meta-Analysis of 2782 Pediatric Appendectomies. Diagnostics 2022, 12, 127. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Before the Pandemic (n = 326) | Pandemic (n = 711) | p-Value | |
|---|---|---|---|
| Sex, male | 148 (45.4%) | 343 (48.2%) | 0.395 |
| Age, years | 39.0 ± 20.6 | 42.4 ± 20.4 | 0.012 0.009 |
| Child (<15) | 44 (13.5%) | 57 (8.0%) | |
| Adult (15–64) | 242 (74.2%) | 537 (75.5%) | |
| Eldely (≥65) | 40 (12.3%) | 117 (16.5%) | |
| Underlying disease | |||
| Hypertension | 39 (12.0%) | 113 (15.9%) | 0.097 |
| Diabetes mellitus | 18 (5.5%) | 40 (5.6%) | 0.946 |
| Cancer | 11 (3.4%) | 27 (3.8%) | 0.736 |
| Stroke | 3 (0.9%) | 12 (1.7%) | 0.337 |
| Cardiovascular disease | 11 (3.4%) | 25 (3.5%) | 0.908 |
| History of operation | 133 (40.8%) | 241 (33.9%) | 0.032 |
| Time from symptom onset to ED, min | 47.8 ± 84.3 | 35.0 ± 54.1 | 0.003 |
| Variables | Before the Pandemic (n = 326) | Pandemic | p | |||
|---|---|---|---|---|---|---|
| Period A (n = 494) | Period B (n = 112) | Period C (n = 105) | Total | |||
| Symptom onset, hour | 47.8 ± 84.3 | 35.3 ± 51.4 | 39.0 ± 61.8 | 29.7 ± 57.6 | 35.0 ± 54.1 | 0.054 |
| Time from ED to antibiotics injection, min | 50.9 ± 84.3 | 38.4 ± 51.4 | 42.5 ± 62.0 | 32.7 ± 57.4 | 38.2 ± 54.1 | 0.053 |
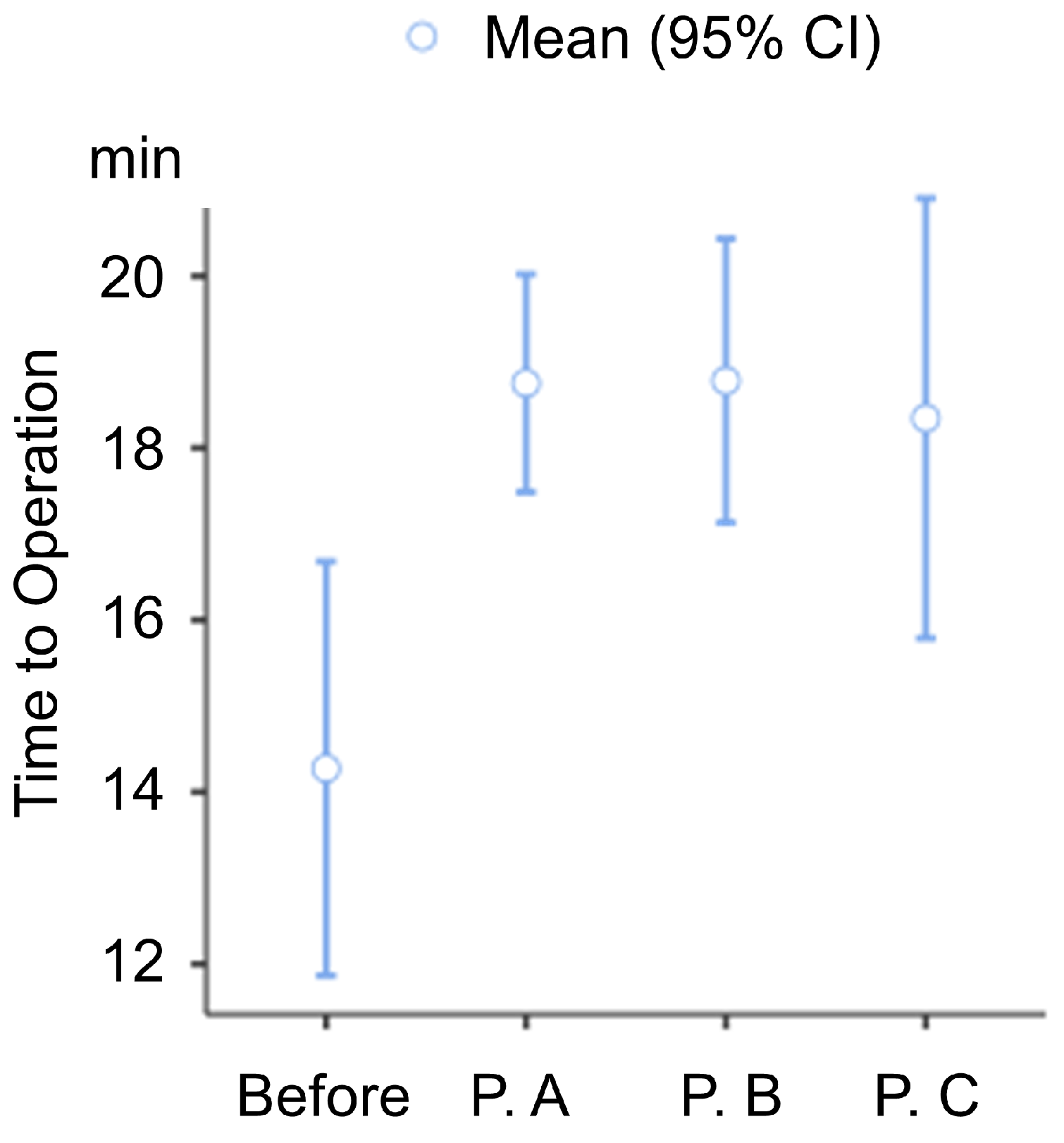
| Time from ED to operation room, hour | 14.3 ± 21.67 | 18.8 ± 14.02 | 18.8 ± 8.57 | 18.3 ± 12.95 | 18.7 ± 13.1 | 0.001 |
| Hospital stay, day | 4.59 ± 2.88 | 4.84 ± 2.50 | 4.72 ± 2.51 | 4.51 ± 1.78 | 4.78 ± 2.41 | 0.451 |
| Complication | 189 (58.0%) | 311 (62.7%) | 62 (55.4%) | 61 (58.1%) | 434 (60.1%) | 0.358 |
| Peritonitis | 53 (16.3%) | 86 (17.3%) | 22 (19.6%) | 36 (34.3%) | 144 (20.2%) | |
| Perforation | 100 (30.7%) | 172 (34.7%) | 29 (25.9%) | 15 (14.3%) | 216 (30.3%) | |
| Abscess | 36 (11.0%) | 53 (10.7%) | 11 (9.8%) | 10 (9.5%) | 74 (10.4%) | |
| Percentage without surgery | 12 (3.7%) | 21 (4.3%) | 6 (5.4%) | 4 (3.8%) | 31 (4.4%) | 0.738 |
| B | S.E. | OR | 95% CI | p | |
|---|---|---|---|---|---|
| Intercept | 0.1025 | 0.24869 | 0.773 | 0.559–1.07 | 0.121 |
| Sex | 0.23265 | 0.13188 | 1.262 | 0.974–1.63 | 0.078 |
| History of operation | 0.08886 | 0.14318 | 0.915 | 0.691–1.21 | 0.535 |
| Time from symptom onset to ED | 0.00961 | 0.00961 | 1.010 | 1.006–1.01 | <0.001 |
| Age | |||||
| Adult | (ref) * | ||||
| Child | 0.10651 | 0.22161 | 1.112 | 0.720–1.72 | 0.631 |
| Elderly | 0.86796 | 0.22077 | 2.382 | 1.545–3.67 | <0.001 |
| Period | |||||
| Before the pandemic | (ref) ** | ||||
| Pandemic: Period A | 0.26458 | 0.15201 | 1.303 | 0.967–1.76 | |
| Pandemic: Period B | −0.02126 | 0.22918 | 0.979 | 0.625–1.53 | |
| Pandemic: Period C | 0.10545 | 0.24024 | 1.111 | 0.694–1.78 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Won, M.; Ahn, C. Epidemiology and Outcome of Acute Appendicitis during and before the COVID-19 Pandemic: A Retrospective Single-Center Analysis. Medicina 2023, 59, 902. https://doi.org/10.3390/medicina59050902
Won M, Ahn C. Epidemiology and Outcome of Acute Appendicitis during and before the COVID-19 Pandemic: A Retrospective Single-Center Analysis. Medicina. 2023; 59(5):902. https://doi.org/10.3390/medicina59050902
Chicago/Turabian StyleWon, Moonho, and Chiwon Ahn. 2023. "Epidemiology and Outcome of Acute Appendicitis during and before the COVID-19 Pandemic: A Retrospective Single-Center Analysis" Medicina 59, no. 5: 902. https://doi.org/10.3390/medicina59050902