
Influence of Restorative Material on the Distribution of Loads to the Bone in Hybrid Abutment Crowns—In Vitro Study

 , and
, and
Abstract
:1. Introduction
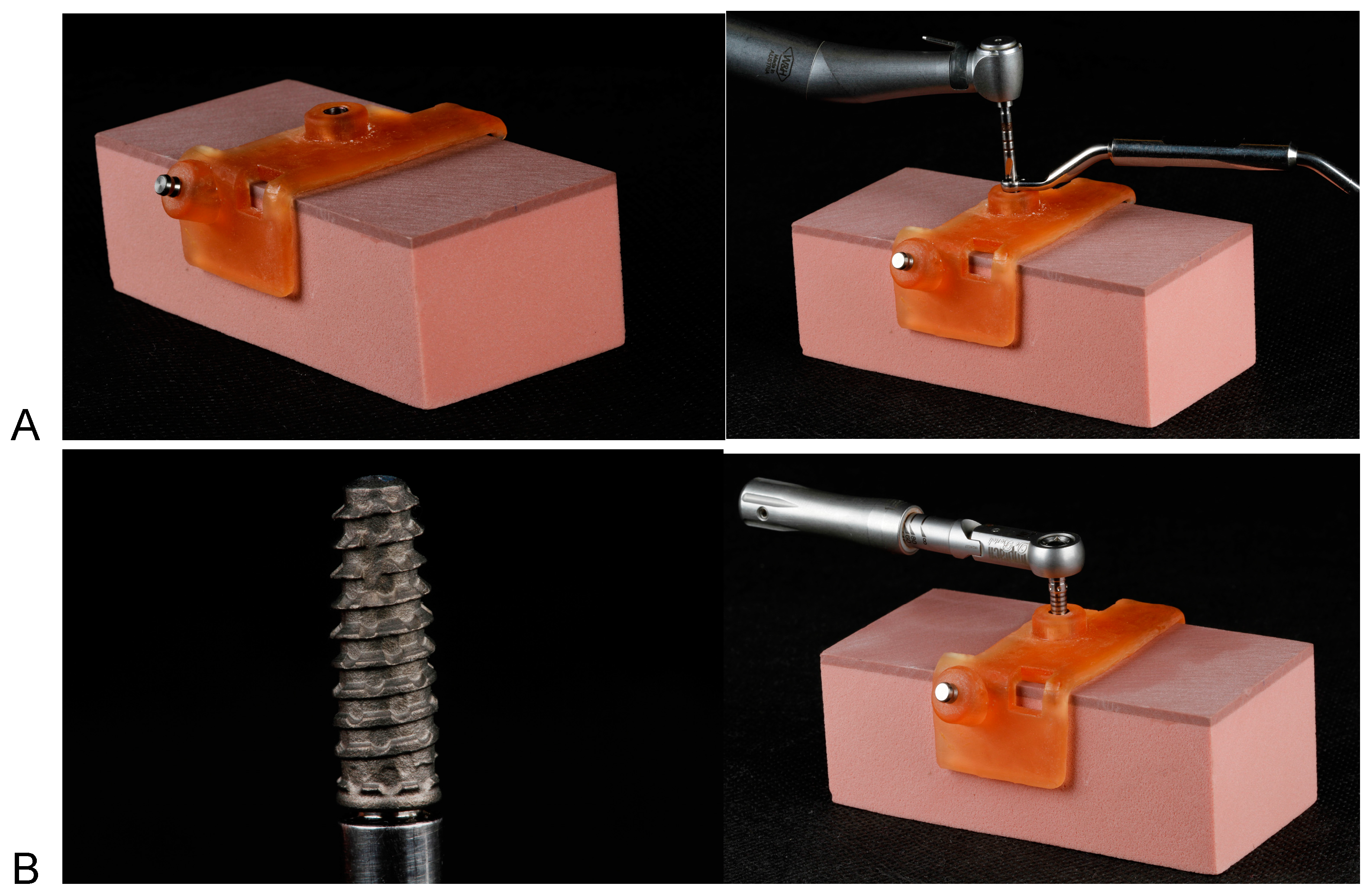
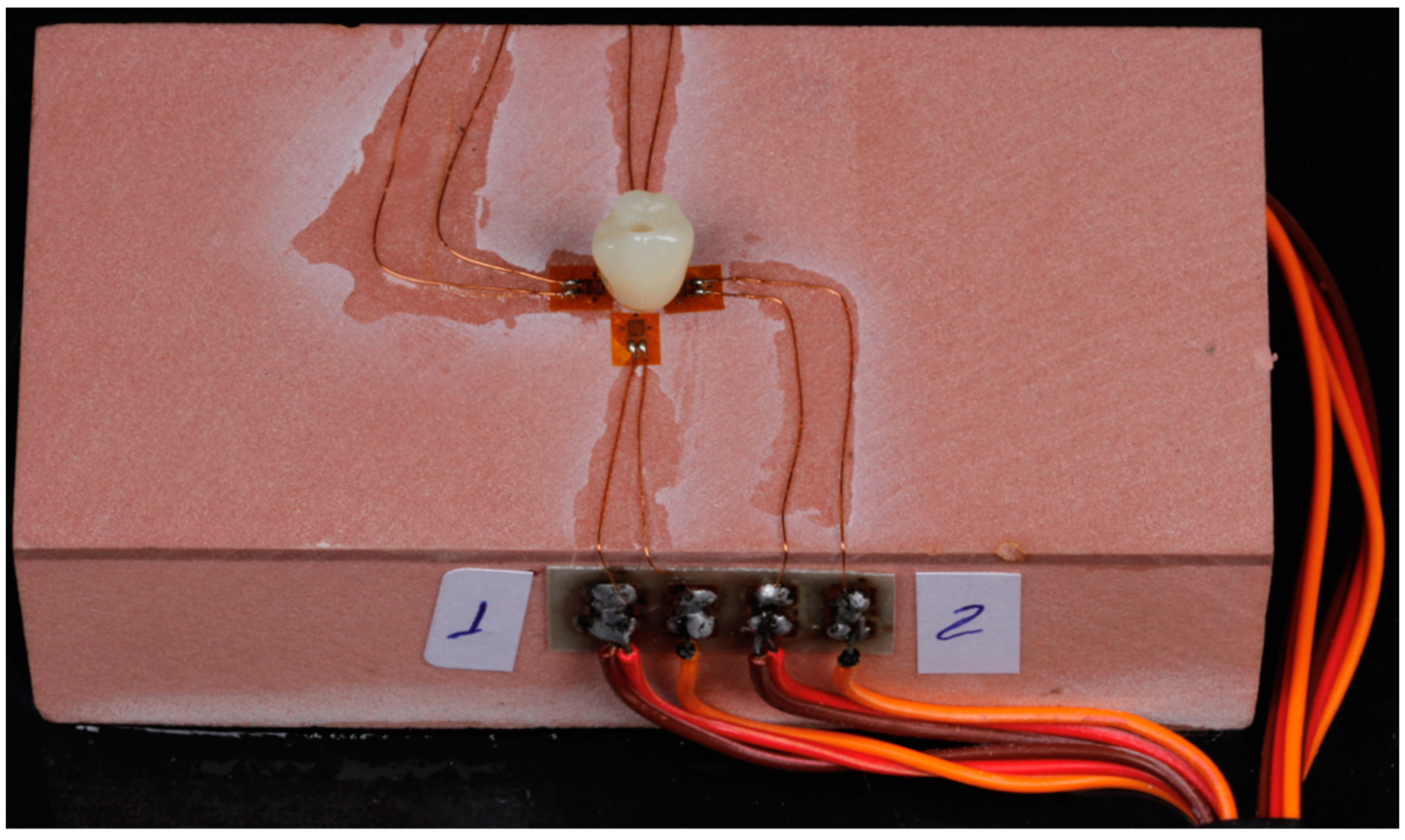
2. Materials and Methods
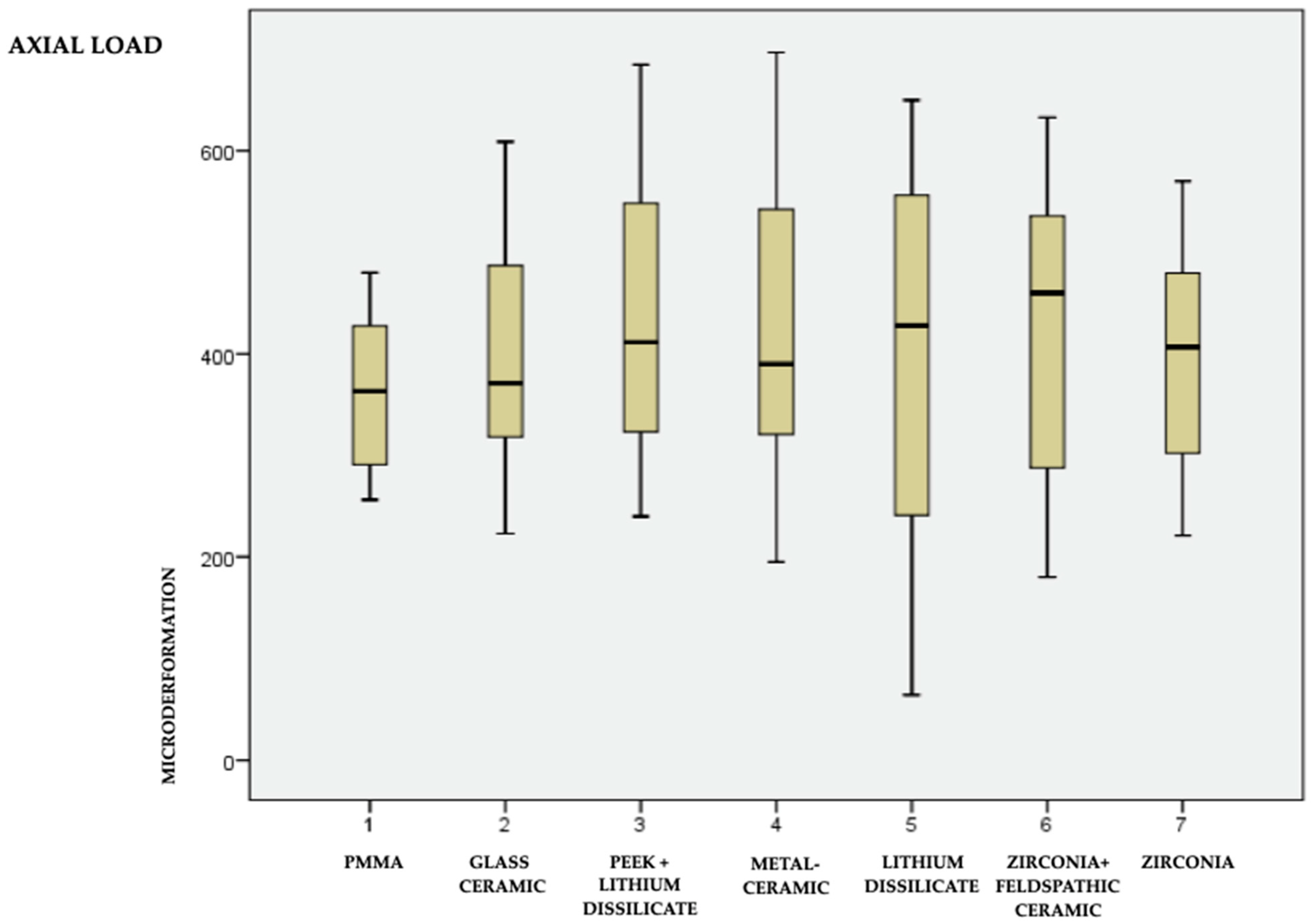
- Axial load, 150 N;
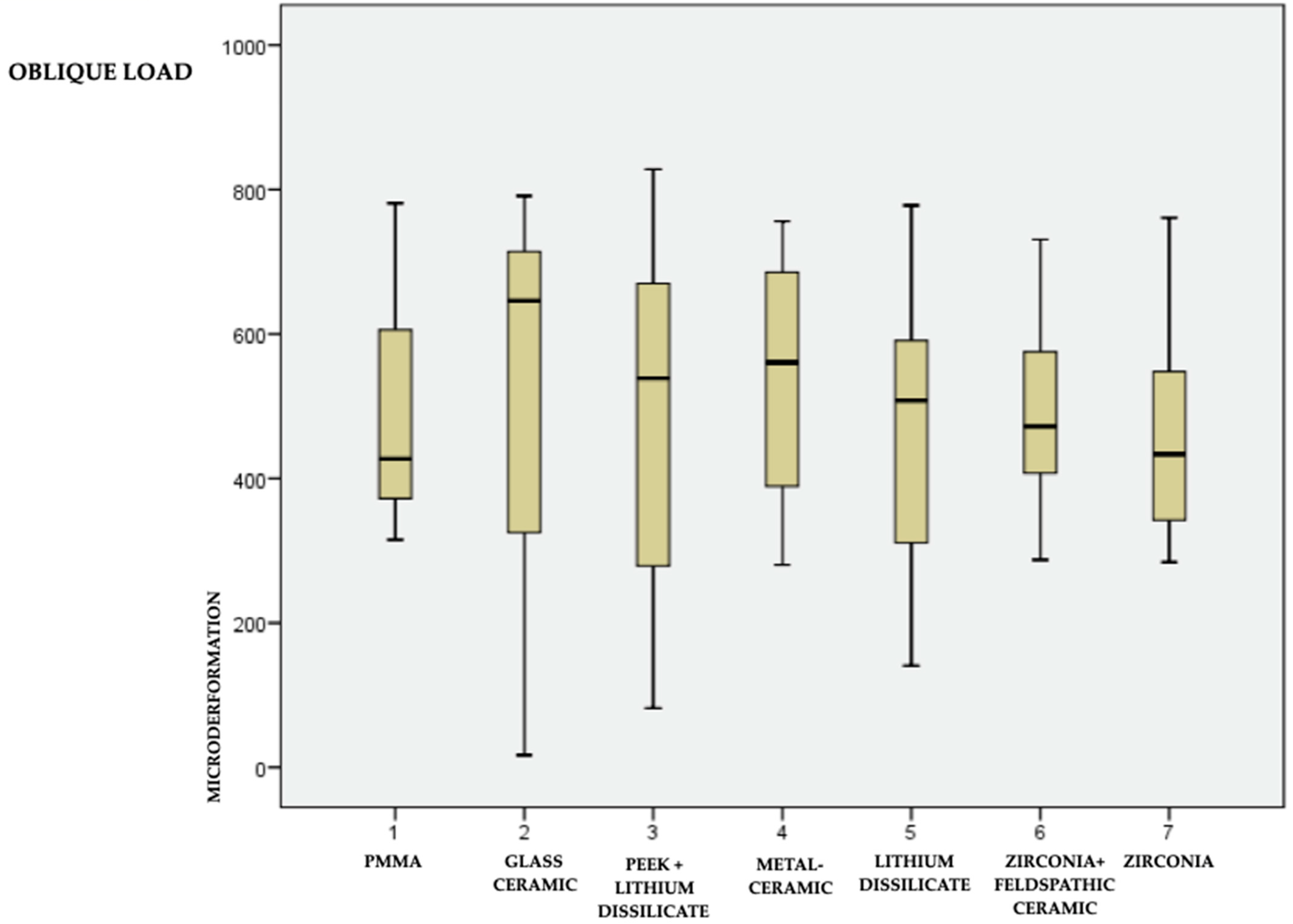
- 45° oblique load, 150 N.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Romeo, E.; Vogel, G. Aspectos diagnósticos e protéticos das 11. reabilitações implantossuportadas. In Reabilitação Oral Com Prótese Implantossuportada Para Casos Complexos; Chiapasco, M., Romeo, E., Eds.; São Paulo: Santos, Brazil, 2007; pp. 1–106. [Google Scholar]
- Misch, C.E. Carregamento progressivo do osso. In Implantes Dentários Contemponâneos; Misch, C.E., Ed.; Editora Santos: São Paulo, Brazil, 2000; pp. 595–608. [Google Scholar]
- Kim, Y.; Oh, T.J.; Misch, C.E.; Wang, H.L. Occlusal considerations in implant therapy: Clinical guidelines with biomechanical rationale. Clin. Oral Implant. Res. 2005, 16, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Crupi, V.; Guglielmino, E.; La Rosa, G.; Vander Sloten, J.; Van Oosterwyck, H. Numerical analysis of bone adaptation around an oral implant due to overload stress. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2004, 218, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.H.; Hsu, Y.T.; Wang, H.L. Identifying occlusal overload and how to deal with it to avoid marginal bone loss around implants. Eur. J. Oral Implantol. 2012. [Google Scholar]
- Bertolini, M.M.; Del Bel Cury, A.A.; Pizzoloto, L.; Acapa, I.R.; Shibli, J.A.; Bordin, D. Does traumatic occlusal forces lead to peri-implant bone loss? A systematic review. Braz. Oral Res. 2019, 33, e069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesquita, A.M.; Silva, J.H.; Saraceni, C.H.; Kojima, A.N.; Özcan, M. Effect of different abutments and connections in deformation crestal bone. Implant. Dent. 2016, 25, 328–334. [Google Scholar] [CrossRef]
- Gupta, S.; Sabharwal, R.; Nazeer, J.; Taneja, L.; Choudhury, B.K.; Sahu, S. Platform switching technique and crestal bone loss around the dental implants: A systematic review. Ann. Afr. Med. 2019, 18, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Eskitascioglu, G.; Usumez, A.; Sevimay, M.; Soykan, E.; Unsal, E. The influence of occlusal loading location on stresses transferred to implant-supported prostheses and supporting bone: A three-dimensional finite element study. J. Prosthet. Dent. 2004, 91, 144–150. [Google Scholar] [CrossRef]
- Mahajan, A.; Kadam, K.N. The influence of mechanical loads on the biomechanics of dental implant. Int. J. Sci. Res. 2014, 3, 1085–1090. [Google Scholar]
- Sugiura, T.; Yamamoto, K.; Horita, S.; Murakami, K.; Tsutsumi, S.; Kirita, T. The effects of bone density and crestal cortical bone thickness on micromotion and peri-implant bone strain distribution in an immediately loaded implant: A nonlinear finite element analysis. J. Periodontal Implant Sci. 2016, 46, 152–165. [Google Scholar] [CrossRef] [Green Version]
- Petrie, C.S.; Williams, J.L. Comparative evaluation of implant designs: Influence of diameter, length, and taper on strains in the alveolar crest: A three-dimensional finite-element analysis. Clin. Oral Implant. Res. 2005, 16, 486–494. [Google Scholar] [CrossRef]
- Rubo, J.H.; Souza, E.A. Métodos computacionais aplicados à bioengenharia: Solução de problemas de carregamento em próteses sobre implantes. Rev. Fac. Odontol. Bauru 2001, 9, 97–103. [Google Scholar]
- Datte, C.E.; Tribst, J.P.; Dal Piva, A.O.; Nishioka, R.S.; Bottino, M.A.; Evangelhista, A.M.; Monteiro, F.M.M.; Borges, A.L. Influence of different restorative materials on the stress distribution in dental implants. J. Clin. Exp. Dent. 2018, 10, e439–e444. [Google Scholar] [CrossRef] [PubMed]
- Abarno, S.; Gehrke, A.F.; Dedavid, B.A.; Gehrke, S.A. Stress distribution around dental implants, generated by six different ceramic materials for unitary restoration: An experimental photoelastic study. Dent. Med. Probl. 2021, 58, 453–461. [Google Scholar] [CrossRef]
- Clelland, N.L.; Carr, A.B.; Gilat, A. Comparison of strains transferred to a bone simulant between as-cast and postsoldered implant frameworks for a five-implant-supported fixed prosthesis. J. Prosthodont. 1996, 5, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Spiekermann, H.; Donath, K.; Hassell, T.; Jovanovic, S.; Richter, J. Biomechanics. In Color Atlas of Dental Medicine Implantology; Thieme Medical Publishers: New York, NY, USA, 1995; pp. 81–90. [Google Scholar]
- Corciolani, G.; Vichi, A.; Louca, C.; Ferrari, M. Influence of layering thickness on the color parameters of a ceramic system. Dent. Mater. 2010, 26, 737–742. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.T.; Fu, J.H.; Al-Hezaimi, K.; Wang, H.L. Biomechanical implant treatment complications: A systematic review of clinical studies of implants with at least 1 year of functional loading. Int. J. Oral Maxillofac. Implant. 2012, 27, 894–904. [Google Scholar]
- Zafar, M.S.; Amin, F.; Fareed, M.A.; Ghabbani, H.; Riaz, S.; Khurshid, Z.; Kumar, N. Biomimetic aspects of restorative dentistry biomaterials. Biomimetics 2020, 5, 34. [Google Scholar] [CrossRef]
- Magne, P.; Belser, U. Bonded Porcelain Restorations in the Anterior Dentition: A Biomimetic Approach; Quintessence Publishing Company: Berlin, Germany, 2002; pp. 23–55. [Google Scholar]
- Hossain, N.; Mobarak, M.H.; Hossain, A.; Khan, F.; Mim, J.J.; Chowdhury, M.A. Advances of plant and biomass extracted zirconium nanoparticles in dental implant application. Heliyon 2023, 9, e15973. [Google Scholar] [CrossRef]
- Chowdhury, M.A.; Hossain, N.; Mostofa, M.G.; Mia, M.R.; Tushar, M.; Rana, M.M.; Hossain, M.H. Green synthesis and characterization of zirconium nanoparticlefor dental implant applications. Heliyon 2023, 9, e12711. [Google Scholar] [CrossRef]
- Edelhoff, D.; Schweiger, J.; Prandtner, O.; Stimmelmayr, M.; Güth, J.F. Metal-free implant-supported single-tooth restorations. Part I: Abutments and cemented crowns. Quintessence Int. 2019, 50, 176–184. [Google Scholar] [CrossRef]
- Blatz, M.B.; Vonderheide, M.; Conejo, J. The effect of resin bonding on long-term success of high-strength ceramics. J. Dent. Res. 2018, 97, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Bidez, M.W. Considerações sobre a oclusão das 6. próteses implantossuportadas: Oclusão protetora do implante e materiais oclusais. In Implantes Dentários Contemporâneos; Misch, C.E., Ed.; Editora Santos: São Paulo, Brazil, 2000; pp. 609–628. [Google Scholar]
- Schwarz, M.S. Mechanical complications of dental implants. Clin. Oral Implant. Res. 2000, 11, 156–158. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, M.; Di Mambro, A.; Giansanti, M.; Brandetti, G. The Survival of Morse Cone-Connection Implants with Platform Switch. Int. J. Oral Maxillofac. Implant. 2016, 31, 1031–1039. [Google Scholar] [CrossRef] [Green Version]
- Quaresma, S.E.; Cury, P.R.; Sendyk, W.R.; Sendyk, C. A finite element analysis of two different dental implants: Stress distribution in the prosthesis, abutment, implant, and supporting bone. J. Oral Implantol. 2008, 34, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Schiegnitz, E.; Al-Nawas, B. Narrow-diameter implants: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29, 21–40. [Google Scholar] [CrossRef] [Green Version]
- Parize, H.N.; Lima Bohner, L.O.; Tavares Gama, L.; Luís Porporatti, A.; Mendonca Mezzomo, L.A.; Martin, W.C.; Gonçalves, T.M.S.V. Narrow-diameter implants in the anterior region: A meta-analysis. Int. J. Oral Maxillofac. Implant. 2019, 34, 1347–1358. [Google Scholar] [CrossRef] [PubMed]
- Corcuera-Flores, J.R.; Pérez-Fierro, M.; Blanco-Carrión, A.; Torres-Lagares, D.; Castellanos-Cosano, L.; Machuca-Portillo, G. Bone loss around narrow implants versus standard diameter implants: Retrospective 2-years case-control study. J. Clin. Exp. Dent. 2020, 12, e79–e84. [Google Scholar] [CrossRef]
- Allen, R.F.; Baldini, N.C.; Donofrio, P.E.; Gutman, E.L.; Keefe, E.; Kramer, J.G. Standard Specification for Rigid Polyurethane Foam for Use as a Standard Material for Testing Orthopedic Devices and Instruments (ASTM F1839-97); ASTM: West Conshohocken, PA, USA, 2001. [Google Scholar]
- Yang, Y.M.; Maeda, Y. The biomechanical effect of platform switching on external-and internal-connection implants. Int. J. Oral Maxillofac. Implant. 2013, 28, 143–147. [Google Scholar] [CrossRef] [Green Version]
- Vasconcellos, L.G.; Nishioka, R.S.; Vasconcellos, L.M.; Nishioka, L.N. Effect of axial loads on implant-supported partial fixed prostheses by strain gauge analysis. J. Appl. Oral Sci. 2011, 19, 610–615. [Google Scholar] [CrossRef] [Green Version]
- Gehrke, S.A.; Pérez-Díaz, L.; Mazón, P.; De Aza, P.N. Biomechanical effects of a new macrogeometry design of dental implants: An in vitro experimental analysis. J. Funct. Biomater. 2019, 10, 47. [Google Scholar] [CrossRef] [Green Version]
- Ha, S.R. Biomechanical three-dimensional finite element analy- sis of monolithic zirconia crown with different cement type. J. Adv. Prosthodont. 2015, 7, 475–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdulmajeed, A.; Sulaiman, T.; Abdulmajeed, A.; Bencharit, S.; Närhi, T. Fracture Load of Different Zirconia Types: A Mastication Simulation Study. J. Prosthodont. 2020, 29, 787–791. [Google Scholar] [CrossRef] [PubMed]
- Abd Alraheam, I.; Donovan, T.E.; Rodgers, B.; Boushell, L.; Sulaiman, T.A. Effect of masticatory simulation on the translucency of different types of dental zirconia. J. Prosthet. Dent. 2019, 122, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Ilie, N.; Hilton, T.J.; Heintze, S.D.; Hickel, R.; Watts, D.C.; Silikas, N.; Stansbury, J.W.; Cadenaro, M.; Ferracane, J.L. Academy of dental materials guidance—Resin composites: Part I—Mechanical properties. Dent. Mater. 2017, 33, 880–894. [Google Scholar] [CrossRef]
- Conserva, E.; Menini, M.; Tealdo, T.; Bevilacqua, M.; Ravera, G.; Pera, F.; Pera, P. The use of a masticatory robot to analyze the shock absorption capacity of different restorative materials for prosthetic implants: A preliminary report. Int. J. Prosthodont. 2009, 22, 53–55. [Google Scholar] [PubMed]
- Awada, A.; Nathanson, D. Mechanical properties of resin-ceramic CAD/CAM restorative materials. J. Prosthet. Dent. 2015, 114, 587–593. [Google Scholar] [CrossRef]
- Menini, M.; Conserva, E.; Tealdo, T.; Bevilacqua, M.; Pera, F.; Signori, A.; Pera, P. Shock absorption capacity of restorative materials for dental implant prostheses: An in vitro study. Int. J. Prosthodont. 2013, 26, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Edelhoff, D.; Schweiger, J.; Prandtner, O.; Stimmelmayr, M.; Güth, J.F. Metal-free implant-supported single-tooth restorations. Part II: Hybrid abutment crowns and material selection. Quintessence Int. 2019, 50, 260–269. [Google Scholar] [CrossRef]
- Gracis, S.; Thompson, V.P.; Ferencz, J.L.; Silva, N.R.; Bonfante, E.A. A new classification system for all-ceramic and ceramic-like restorative materials. Int. J. Prosthodont. 2015, 28, 227–235. [Google Scholar] [CrossRef] [Green Version]
- Fasbinder, D.J.; Neiva, G.F. Surface evaluation of polishing techniques for new resilient CAD/CAM restorative materials. J. Esthet. Restor. Dent. 2016, 28, 56–66. [Google Scholar] [CrossRef]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Siddiqui, F. Applications of polyetheretherketone (PEEK) in oral implantology and prosthodontics. J. Prosthodont. Res. 2016, 60, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.E.; Thoma, D.; Jung, R.; Zwahlen, M.; Zembic, A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDP s) after a mean observation period of at least 5 years. Clin. Oral Implant. Res. 2012, 23, 22–38. [Google Scholar] [CrossRef] [PubMed]
- Junior, J.F.; Pellizzer, E.P.; Verri, F.R.; de Carvalho, P.S. Stress analysis in bone tissue around single implants with different diameters and veneering materials: A 3-D finite element study. Mater. Sci. Eng. C 2013, 33, 4700–4714. [Google Scholar]
- Abou-Ayash, S.; Strasding, M.; Rücker, G.; Att, W. Impact of prosthetic material on mid-and long-term outcome of dental implants supporting single crowns and fixed partial dentures: A systematic review and meta-analysis. Eur. J. Oral Implantol. 2017, 10 (Suppl. 1), 47–65. [Google Scholar]
- Wang, T.M.; Leu, L.J.; Wang, J.S.; Lin, L.D. Effects of prosthesis materials and prosthesis splinting on peri-implant bone stress around implants in poor-quality bone: A numeric analysis. Int. J. Oral Maxillofac. Implant. 2002, 17, 231–237. [Google Scholar]
- Aldebes, A.; Al-Khanati, N.M.; Abou Nassar, J.; Kharboutly, N.A.; Aldamman, F. Effect of restoration material on marginal bone resorption around modified anatomic zirconia dental implants: A randomised controlled trial. Ann. Med. Surg. 2022, 80, 104313. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | PMMA—polymethylmethacrylate (VIPI Block Trilux) |
| 2 | Glass ceramic in resin matrix (GC—Cerasmart) |
| 3 | PEEK—thermoplastic polymer (Juvora) with lithium disilicate coating (Rosetta) |
| 4 | Metal–ceramic (NiCr + GC Initial—MC Classic) |
| 5 | Lithium disilicate (Rosetta) |
| 6 | Zirconia infrastructure (Zolid Amann Girrbach) and feldspathic ceramic coating (Leucite GC Initial LRF) |
| 7 | Monolithic zirconia (Zolid Amann Girrbach) |
| Materials | Axial Means | Axial Deviations | 45° Mean | 45° Deviation | p-Value |
|---|---|---|---|---|---|
| 1—PMMA | 361.70 | 75.487 | 486.00 | 151.392 | 0.00 |
| 2—Hybrid resin | 402.45 | 112.629 | 515.40 | 282.465 | 0.20 |
| 3—PEEK + disilicate | 437.55 | 149.387 | 487.25 | 250.764 | 0.15 |
| 4—Metal–ceramic | 427.80 | 148.991 | 533.35 | 166.678 | 0.00 |
| 5—Monolithic disilicate | 391.80 | 200.403 | 471.95 | 201.646 | 0.00 |
| 6—Zirconia + disilicate | 418.80 | 143.448 | 496.30 | 127.304 | 0.00 |
| 7—Monolithic disilicate | 397.60 | 114.196 | 462.75 | 139.496 | 0.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martins, R.G.; Castro, T.S.d.; Dib, L.L.; Gehrke, S.A.; Mesquita, A.M.M. Influence of Restorative Material on the Distribution of Loads to the Bone in Hybrid Abutment Crowns—In Vitro Study. Medicina 2023, 59, 1188. https://doi.org/10.3390/medicina59071188
Martins RG, Castro TSd, Dib LL, Gehrke SA, Mesquita AMM. Influence of Restorative Material on the Distribution of Loads to the Bone in Hybrid Abutment Crowns—In Vitro Study. Medicina. 2023; 59(7):1188. https://doi.org/10.3390/medicina59071188
Chicago/Turabian StyleMartins, Rafael Garcia, Tayna Silva de Castro, Luciano Lauria Dib, Sergio Alexandre Gehrke, and Alfredo Mikail Melo Mesquita. 2023. "Influence of Restorative Material on the Distribution of Loads to the Bone in Hybrid Abutment Crowns—In Vitro Study" Medicina 59, no. 7: 1188. https://doi.org/10.3390/medicina59071188