
Superfoods for Type 2 Diabetes: A Narrative Review and Proposal for New International Recommendations


Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria, and the Timeframe Covered
2.2. Type of Study
2.3. Search Methodology and Data Extraction
2.4. Databases, Keywords and Data Presentation
2.5. Quality Assessment
2.6. Previously Identified Reviews on the Present Topic
3. Results
Selected Papers/Documents
4. Discussion
4.1. Identified ‘Superfoods’ That Can Reduce Glycaemic Levels in Patients with Type 2 Diabetes Mellitus (T2DM)
4.1.1. Foods with Polyphenols (e.g., Berries)
4.1.2. Fermented Dairy Products (with or without Vitamin D or Probiotic Supplementation)
4.1.3. Whole Cereals
4.1.4. Nuts
4.1.5. Proteins (Especially Plant Protein-Rich Diets)
4.1.6. Sunflower Seeds and Flaxseeds
4.1.7. Cabbage and Lupin
4.1.8. Prickly Pear Cacti (Opuntia spp.) Cladodes
4.1.9. Honey
4.2. Identified ‘Superfoods’ with the Potential to Reduce HbA1c in T2DM Patients
4.2.1. Foods with Polyphenols (e.g., Berries)
4.2.2. Fermented Dairy Products
4.2.3. Whole Cereals
4.2.4. Nuts: Almonds and Pistachios
4.2.5. Proteins (Especially Plant Protein-Rich Diets)
4.2.6. Flaxseed Supplementation
4.2.7. Lupin
4.2.8. The Most Significant Reductions in HbA1c
4.3. New Proposed International Guidance on the Consumption of Identified ‘Superfoods’ by T2DM Patients
- The isolated consumption of ‘superfoods’ should not be used to substitute a proper and successful diet or exercise plan for T2DM patients. The adoption of a certain diet, such as a Mediterranean-style, low-fat or low-carbohydrate diet, seems to be more relevant than the isolated consumption of ‘superfoods’ by T2DM patients, since it has been demonstrated that a successful medical nutrition therapy plan per se can reach a similar or greater reduction in HbA1c than medication for T2DM [8].
- It is likely that the goals of a proper medical nutrition therapy for T2DM patients may be more easily achieved and/or maintained with the concomitant use of ‘superfoods’, since some ‘superfoods’ are likely to improve or maintain metabolic control (glucose and lipid profiles, body mass weight, blood pressure and anti-inflammatory markers, among others).
- ‘Superfoods’ should preferably be integrated into the diet plan of T2DM patients with the involvement of a nutritionist. For instance, ‘superfoods’ can be used to substitute foods from the same group of the food wheel, respecting the principles of a diversified and rational nutritional plan.
- Metabolic supervision should be carried out in the months before and after the introduction of ‘superfoods’ into the diet of T2DM patients to identify and quantify eventual ameliorations.
- ‘Superfoods’ should be consumed in the right doses (quantitatively and qualitatively) to ensure that their bioactive properties are achieved, particularly given that ‘superfoods’ tend to be more expensive than other foods.
- Less-controlled T2DM patients can benefit more from the inclusion of ‘superfoods’ in their diet than more-controlled T2DM patients.
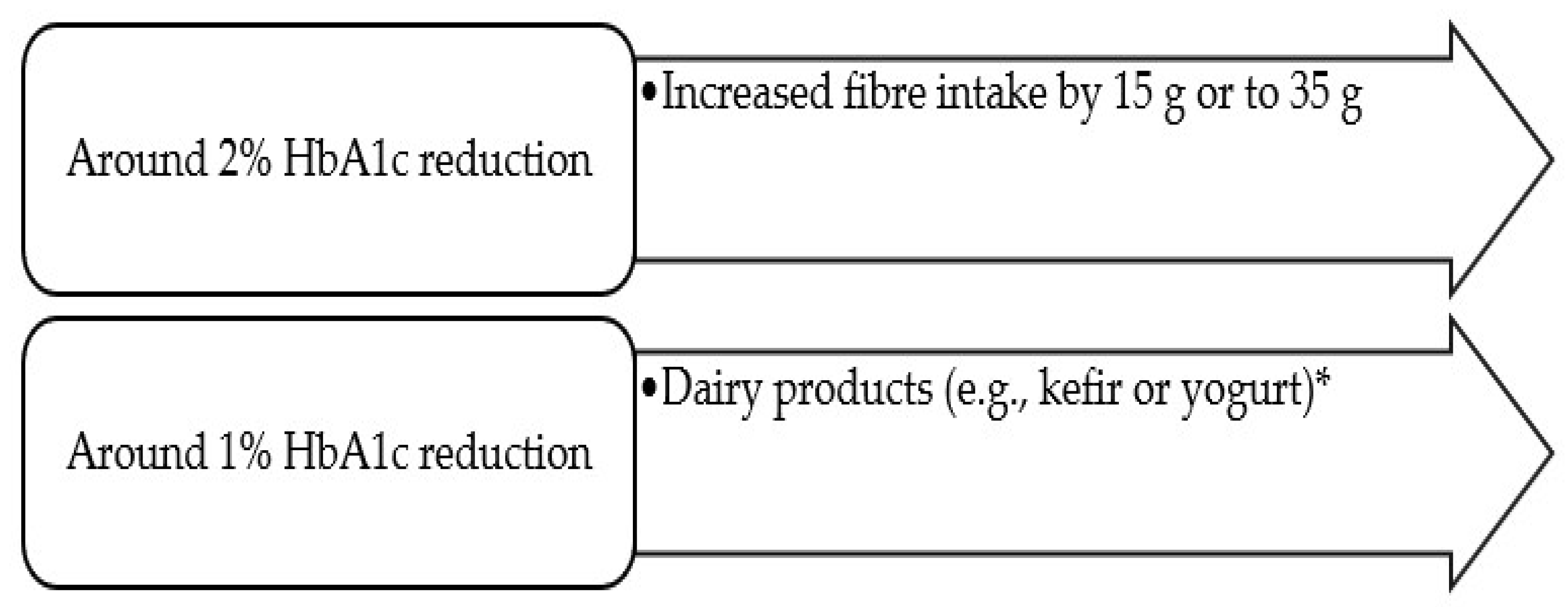
- More significant HbA1c reductions seem to be achieved with the consumption of dairy products (giving a reduction of around 1%, with or without the enrichment of vitamin D and probiotics, according to diverse studies) [57,58,60] and with fibre supplementation (based on the comparison between a daily dietary fibre intake of 35 g and the average intake of 19 g: increasing the daily fibre intake by 15 g or up to 35 g resulted in a reduction of −2.00 mmol/mol (−2.3%) HbaA1c) [30]. Thus, these ‘superfoods’ are recommended in the diet of T2DM patients, although this does not exclude the need for metabolic control (before and after any alteration in the diet plan), since results are not in agreement between studies.
- High-fat dairy products are not recommended [21,23]. The consumption of cheese can result in a 5 to 24% increase in the risk of developing T2DM according to some prospective cohort studies [23]. Thus, the consumption of high-fat dairy products should be limited (or eliminated) in the diets of T2DM patients.
- Refined grain products should be substituted by whole grain foods, since diverse studies support an improvement in the metabolic metabolism and lipid profile of T2DM patients, a decreased risk of T2DM and a possible decreased risk of colon cancer, fatal coronary heart disease (CHD) and cardiovascular disease (CVD) mortality with the consumption of whole grain foods [28].
- Different classes of foods with polyphenols (e.g., berries) are recommended rather than a specific food due to a likely pleiotropic effect, i.e., a potential contribution towards the regulation of glycaemic and lipidic metabolism (increased HDL cholesterol and decreased LDL cholesterol), blood pressure control and anti-obesity, as well as an improvement in the anti-inflammatory and oxidative stress plasma markers [14,16].
- Proteins (especially plant protein-rich diets), such as beans/chickpeas, other leguminous plants (e.g., soybeans) and other proteins, such as whey protein, are recommended in the regular diet of T2DM patients, since they support an improvement in glycaemic control and insulin sensitivity [34,35,36].
- Nuts (without added salt or sugar) are recommended, especially to control the lipidic profile (total cholesterol, LDL and triacylglycerols) [31].
- Nuts seem to be an adequate alternative to the consumption of carbohydrates, with improved glycaemic control and lipid risk factors in individuals with T2DM [46].
- Other ‘superfoods’, such as sunflower seeds, flaxseeds, cabbage, lupin, prickly pear cacti (Opuntia spp.) cladodes and honey (short term), may also improve the metabolic control of T2DM patients, but further studies are recommended.
4.4. Strengths and Weaknesses of the Present Narrative Review
4.5. Future Research
5. Conclusions
Funding
Data Availability Statement
Conflicts of Interest
References
- WHO. Diabetes. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 23 March 2023).
- International Diabetes Federation. Diabetes around the World in 2021. Available online: https://diabetesatlas.org/idfawp/resource-files/2021/11/IDFDA10-global-fact-sheet.pdf (accessed on 23 May 2023).
- American Diabetes Association. Diagnosis. Available online: https://diabetes.org/diabetes/a1c/diagnosis (accessed on 23 March 2023).
- Barsby, J.P.; Cowley, J.M.; Leemaqz, S.Y.; Grieger, J.A.; McKeating, D.R.; Perkins, A.V.; Bastian, S.E.P.; Burton, R.A.; Bianco-Miotto, T. Nutritional properties of selected superfood extracts and their potential health benefits. PeerJ 2021, 9, e12525. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. What Superstar Foods Are Good for Diabetes? Available online: https://diabetes.org/healthy-living/recipes-nutrition/eating-well/diabetes-superstar-foods (accessed on 23 March 2023).
- van den Driessche, J.J.; Plat, J.; Mensink, R.P. Effects of superfoods on risk factors of metabolic syndrome: A systematic review of human intervention trials. Food Funct. 2018, 9, 1944–1966. [Google Scholar] [CrossRef] [PubMed]
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S.; et al. Nutrition Therapy for Adults with Diabetes or Prediabetes: A Consensus Report. Diabetes Care 2019, 42, 731–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, K.; McArdle, P. The ADA nutrition therapy consensus report: A quick guide. J. Diabetes Nurs. 2019, 23, 103. [Google Scholar]
- CDC—Centers for Disease and Control Prevention. Diabetes Meal Planning. Available online: https://www.cdc.gov/diabetes/managing/eat-well/meal-plan-method.html (accessed on 28 March 2023).
- Pollock, M.; Fernandes, R.M.; Becker, L.A.; Pieper, D.; Hartling, L. Chapter V: Overviews of reviews. In Cochrane Handbook for Systematic Reviews of Interventions, Version 6.0 (Updated March 2020); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpstone, M.S., Li, T., Page, M.J., Welch, V., Eds.; John Wiley & Sons: Chichester, UK, 2020; Available online: www.training.cochrane.org/handbook (accessed on 1 June 2020).
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA-a scale for the quality assessment of narrative review articles. Res. Integr. Peer Rev. 2019, 4, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gates, M.; Gates, A.; Guitard, S.; Pollock, M.; Hartling, L. Guidance for overviews of reviews continues to accumulate, but important challenges remain: A scoping review. Syst. Rev. 2020, 9, 254. [Google Scholar] [CrossRef]
- Kalt, W.; Cassidy, A.; Howard, L.R.; Krikorian, R.; Stull, A.J.; Tremblay, F.; Zamora-Ros, R. Recent Research on the Health Benefits of Blueberries and Their Anthocyanins. Adv. Nutr. 2020, 11, 224–236. [Google Scholar] [CrossRef]
- Chan, S.W.; Tomlinson, B. Effects of Bilberry Supplementation on Metabolic and Cardiovascular Disease Risk. Molecules 2020, 25, 1653. [Google Scholar] [CrossRef] [Green Version]
- Derrick, S.A.; Kristo, A.S.; Reaves, S.K.; Sikalidis, A.K. Effects of Dietary Red Raspberry Consumption on Pre-Diabetes and Type 2 Diabetes Mellitus Parameters. Int. J. Environ. Res. Public Health 2021, 18, 9364. [Google Scholar] [CrossRef]
- Hameed, A.; Galli, M.; Adamska-Patruno, E.; Krętowski, A.; Ciborowski, M. Select Polyphenol-Rich Berry Consumption to Defer or Deter Diabetes and Diabetes-Related Complications. Nutrients 2020, 12, 2538. [Google Scholar] [CrossRef]
- Sun, L.; Miao, M. Dietary polyphenols modulate starch digestion and glycaemic level: A review. Crit. Rev. Food Sci. Nutr. 2020, 60, 541–555. [Google Scholar] [CrossRef] [PubMed]
- Giacco, R.; Costabile, G.; Fatati, G.; Frittitta, L.; Maiorino, M.I.; Marelli, G.; Parillo, M.; Pistis, D.; Tubili, C.; Vetrani, C.; et al. Effects of polyphenols on cardio-metabolic risk factors and risk of type 2 diabetes. A joint position statement of the Diabetes and Nutrition Study Group of the Italian Society of Diabetology (SID), the Italian Association of Dietetics and Clinical Nutrition (ADI) and the Italian Association of Medical Diabetologists (AMD). Nutr. Metab. Cardiovasc. Dis. 2020, 30, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Restani, P.; Di Lorenzo, C.; Fradera, U.; Stockley, C.S.; Teissedre, P.L.; Ruf, J.C.; Iasiello, B.; Biella, S.; Colombo, F.; Kosti, R.I. Is it scientifically justifiable to exclude wine and/or unfermented grape derivatives from the diet of consumers with or at risk of developing type-2 diabetes? Food Funct. 2020, 11, 10266–10278. [Google Scholar] [CrossRef] [PubMed]
- Awwad, S.F.; Abdalla, A.; Howarth, F.C.; Stojanovska, L.; Kamal-Eldin, A.; Ayyash, M.M. Invited review: Potential effects of short- and long-term intake of fermented dairy products on prevention and control of type 2 diabetes mellitus. J. Dairy Sci. 2022, 105, 4722–4733. [Google Scholar] [CrossRef]
- Lombardo, M.; Bellia, C.; Moletto, C.; Aulisa, G.; Padua, E.; Della-Morte, D.; Caprio, M.; Bellia, A. Effects of Quality and Quantity of Protein Intake for Type 2 Diabetes Mellitus Prevention and Metabolic Control. Curr. Nutr. Rep. 2020, 9, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Emadzadeh, M.; Sahebi, R.; Khedmatgozar, H.; Sadeghi, R.; Farjami, M.; Sharifan, P.; Ravanshad, Y.; Ferns, G.A.; Ghayour-Mobarhan, M. A systematic review and meta-analysis of the effect of Vitamin D-fortified food on glycemic indices. Biofactors 2020, 46, 502–513. [Google Scholar] [CrossRef]
- Companys, J.; Pla-Pagà, L.; Calderón-Pérez, L.; Llauradó, E.; Solà, R.; Pedret, A.; Valls, R.M. Fermented Dairy Products, Probiotic Supplementation, and Cardiometabolic Diseases: A Systematic Review and Meta-analysis. Adv. Nutr. 2020, 11, 834–863. [Google Scholar] [CrossRef]
- Yanni, A.E.; Kartsioti, K.; Karathanos, V.T. The role of yoghurt consumption in the management of type II diabetes. Food Funct. 2020, 11, 10306–10316. [Google Scholar] [CrossRef]
- Companys, J.; Pedret, A.; Valls, R.M.; Solà, R.; Pascual, V. Fermented dairy foods rich in probiotics and cardiometabolic risk factors: A narrative review from prospective cohort studies. Crit. Rev. Food Sci. Nutr. 2021, 61, 1966–1975. [Google Scholar] [CrossRef]
- Tiderencel, K.A.; Hutcheon, D.A.; Ziegler, J. Probiotics for the treatment of type 2 diabetes: A review of randomized controlled trials. Diabetes Metab. Res. Rev. 2020, 36, e3213. [Google Scholar] [CrossRef]
- Wu, W.; Qiu, J.; Wang, A.; Li, Z. Impact of whole cereals and processing on type 2 diabetes mellitus: A review. Crit. Rev. Food Sci. Nutr. 2020, 60, 1447–1474. [Google Scholar] [CrossRef]
- Tieri, M.; Ghelfi, F.; Vitale, M.; Vetrani, C.; Marventano, S.; Lafranconi, A.; Godos, J.; Titta, L.; Gambera, A.; Alonzo, E.; et al. Whole grain consumption and human health: An umbrella review of observational studies. Int. J. Food Sci. Nutr. 2020, 71, 668–677. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.; Khan, M.Z.; Ma, Y.; Meng, Y.; Mushtaq, A.; Shen, Q.; Xue, Y. Overview of the Composition of Whole Grains’ Phenolic Acids and Dietary Fibre and Their Effect on Chronic Non-Communicable Diseases. Int. J. Environ. Res. Public Health 2022, 19, 3042. [Google Scholar] [CrossRef]
- Reynolds, A.N.; Akerman, A.P.; Mann, J. Dietary fibre and whole grains in diabetes management: Systematic review and meta-analyses. PLoS Med. 2020, 17, e1003053. [Google Scholar] [CrossRef]
- Alasalvar, C.; Salvadó, J.S.; Ros, E. Bioactives and health benefits of nuts and dried fruits. Food Chem. 2020, 314, 126192. [Google Scholar] [CrossRef] [PubMed]
- Dreher, M.L. A Comprehensive Review of Almond Clinical Trials on Weight Measures, Metabolic Health Biomarkers and Outcomes, and the Gut Microbiota. Nutrients 2021, 13, 1968. [Google Scholar] [CrossRef] [PubMed]
- Nowrouzi-Sohrabi, P.; Hassanipour, S.; Sisakht, M.; Daryabeygi-Khotbehsara, R.; Savardashtaki, A.; Fathalipour, M. The effectiveness of pistachio on glycemic control and insulin sensitivity in patients with type 2 diabetes, prediabetes and metabolic syndrome: A systematic review and meta-analysis. Diabetes Metab. Syndr. 2020, 14, 1589–1595. [Google Scholar] [CrossRef]
- Pfeiffer, A.F.H.; Pedersen, E.; Schwab, U.; Risérus, U.; Aas, A.M.; Uusitupa, M.; Thanopoulou, A.; Kendall, C.; Sievenpiper, J.L.; Kahleová, H.; et al. The Effects of Different Quantities and Qualities of Protein Intake in People with Diabetes Mellitus. Nutrients 2020, 12, 365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullins, A.P.; Arjmandi, B.H. Health Benefits of Plant-Based Nutrition: Focus on Beans in Cardiometabolic Diseases. Nutrients 2021, 13, 519. [Google Scholar] [CrossRef]
- Reister, E.J.; Belote, L.N.; Leidy, H.-J. The Benefits of Including Hummus and Hummus Ingredients into the American Diet to Promote Diet Quality and Health: A Comprehensive Review. Nutrients 2020, 12, 3678. [Google Scholar] [CrossRef]
- Amirani, E.; Milajerdi, A.; Reiner, Ž.; Mirzaei, H.; Mansournia, M.A.; Asemi, Z. Effects of whey protein on glycemic control and serum lipoproteins in patients with metabolic syndrome and related conditions: A systematic review and meta-analysis of randomized controlled clinical trials. Lipids Health Dis. 2020, 19, 209. [Google Scholar] [CrossRef]
- Rehman, A.; Saeed, A.; Kanwal, R.; Ahmad, S.; Changazi, S.H. Therapeutic Effect of Sunflower Seeds and Flax Seeds on Diabetes. Cureus 2021, 13, e17256. [Google Scholar] [CrossRef] [PubMed]
- Uuh-Narvaez, J.J.; Segura-Campos, M.R. Cabbage (Brassica oleracea var. capitata): A food with functional properties aimed to type 2 diabetes prevention and management. J. Food Sci. 2021, 86, 4775–4798. [Google Scholar] [CrossRef] [PubMed]
- Bryant, L.; Rangan, A.; Grafenauer, S. Lupins and Health Outcomes: A Systematic Literature Review. Nutrients 2022, 14, 327. [Google Scholar] [CrossRef] [PubMed]
- Kashif, R.R.; D’Cunha, N.M.; Mellor, D.D.; Alexopoulos, N.I.; Sergi, D.; Naumovski, N. Prickly Pear Cacti (Opuntia spp.) Cladodes as a Functional Ingredient for Hyperglycemia Management: A Brief Narrative Review. Medicina 2022, 58, 300. [Google Scholar] [CrossRef]
- Terzo, S.; Mulè, F.; Amato, A. Honey and obesity-related dysfunctions: A summary on health benefits. J. Nutr. Biochem. 2020, 82, 108401. [Google Scholar] [CrossRef]
- American Diabetes Association. Alcohol & Diabetes. Available online: https://diabetes.org/healthy-living/medication-treatments/alcohol-diabetes (accessed on 29 March 2023).
- Hove, K.D.; Brøns, C.; Færch, K.; Lund, S.S.; Rossing, P.; Vaag, A. Effects of 12 weeks of treatment with fermented milk on blood pressure, glucose metabolism and markers of cardiovascular risk in patients with type 2 diabetes: A randomised double-blind placebo-controlled study. Eur. J. Endocrinol. 2015, 172, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Mohamadshahi, M.; Veissi, M.; Haidari, F.; Javid, A.Z.; Mohammadi, F.; Shirbeigi, E. Effects of probiotic yogurt consumption on lipid profile in type 2 diabetic patients: A randomized controlled clinical trial. J. Res. Med. Sci. 2014, 19, 531–536. [Google Scholar]
- Jenkins, D.J.A.; Kendall, C.W.C.; Lamarche, B.; Banach, M.S.; Srichaikul, K.; Vidgen, E.; Mitchell, S.; Parker, T.; Nishi, S.; Bashyam, B.; et al. Nuts as a replacement for carbohydrates in the diabetic diet: A reanalysis of a randomised controlled trial. Diabetologia 2018, 61, 1734–1747. [Google Scholar] [CrossRef] [Green Version]
- Wallace, T.C.; Murray, R.; Zelma, K.M. The Nutritional Value and Health Benefits of Chickpeas and Hummus. Nutrients 2016, 8, 766. [Google Scholar] [CrossRef] [Green Version]
- Badely, M.; Sepandi, M.; Samadi, M.; Parastouei, K.; Taghdir, M. The effect of whey protein on the components of metabolic syndrome in overweight and obese individuals; a systematic review and meta-analysis. Diabetes Metab. Syndr. 2019, 13, 3121–3131. [Google Scholar] [CrossRef] [PubMed]
- Darand, M.; Alizadeh, S.; Mansourian, M. The effect of Brassica vegetables on blood glucose levels and lipid profiles in adults. A systematic review and meta-analysis. Phytother. Res. PTR 2022, 36, 1914–1929. [Google Scholar] [CrossRef] [PubMed]
- López-Romero, P.; Pichardo-Ontiveros, E.; Avila-Nava, A.; Vázquez-Manjarrez, N.; Tovar, A.R.; Pedraza-Chaverri, J.; Torres, N. The effect of nopal (Opuntia ficus indica) on postprandial blood glucose, incretins, and antioxidant activity in Mexican patients with type 2 diabetes after consumption of two different composition breakfasts. J. Acad. Nutr. Diet. 2014, 114, 1811–1818. [Google Scholar] [CrossRef]
- Nazir, L.; Samad, F.; Haroon, W.; Kidwai, S.S.; Siddiqi, S.; Zehravi, M. Comparison of glycaemic response to honey and glucose in type 2 diabetes. J. Pak. Med. Assoc. 2014, 64, 69–71. [Google Scholar] [PubMed]
- Huang, H.; Chen, G.; Liao, D.; Zhu, Y.; Xue, X. Effects of Berries Consumption on Cardiovascular Risk Factors: A Meta-analysis with Trial Sequential Analysis of Randomized Controlled Trials. Sci. Rep. 2016, 6, 23625. [Google Scholar] [CrossRef]
- Calvano, A.; Izuora, K.; Oh, E.C.; Ebersole, J.L.; Lyons, T.J.; Basu, A. Dietary berries, insulin resistance and type 2 diabetes: An overview of human feeding trials. Food Funct. 2019, 10, 6227–6243. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Zhou, R.; Wang, B.; Chen, K.; Shi, L.Y.; Zhu, J.D.; Mi, M.T. Effect of green tea on glucose control and insulin sensitivity: A meta-analysis of 17 randomized controlled trials. Am. J. Clin. Nutr. 2013, 98, 340–348. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, J.K.; Thomas, S.; Nanjan, M.J. Resveratrol supplementation improves glycemic control in type 2 diabetes mellitus. Nutr. Res. 2012, 32, 537–541. [Google Scholar] [CrossRef]
- Vitale, M.; Vaccaro, O.; Masulli, M.; Bonora, E.; Del Prato, S.; Giorda, C.B.; Nicolucci, A.; Squatrito, S.; Auciello, S.; Babini, A.C.; et al. Polyphenol intake and cardiovascular risk factors in a population with type 2 diabetes: The TOSCA.IT study. Clin. Nutr. 2017, 36, 1686–1692. [Google Scholar] [CrossRef]
- El-Bashiti, T.A.; Zabut, B.M.; Abu Safia, F.F. Effect of Probiotic Fermented Milk (Kefir) on Some Blood Biochemical Parameters Among Newly Diagnosed Type 2 Diabetic Adult Males in Gaza Governorate. Curr. Res. Nutr. Food Sci. 2019, 7, 568–575. [Google Scholar] [CrossRef]
- Shab-Bidar, S.; Neyestani, T.R.; Djazayery, A.; Eshraghian, M.R.; Houshiarrad, A.; Gharavi, A.; Kalayi, A.; Shariatzadeh, N.; Zahedirad, M.; Khalaji, N.; et al. Regular consumption of vitamin D-fortified yogurt drink (Doogh) improved endothelial biomarkers in subjects with type 2 diabetes: A randomized double-blind clinical trial. BMC Med. 2011, 9, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonucci, L.B.; Santos, K.M.O.; de Oliveira, L.L.; Ribeiro, S.M.R.; Martino, H.S.D. Clinical application of probiotics in type 2 diabetes mellitus: A randomized, double-blind, placebo-controlled study. Clin. Nutr. 2017, 36, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Ostadrahimi, A.; Taghizadeh, A.; Mobasseri, M.; Farrin, N.; Payahoo, L.; Beyramalipoor Gheshlaghi, Z.; Vahedjabbari, M. Effect of probiotic fermented milk (kefir) on glycemic control and lipid profile in type 2 diabetic patients: A randomized double-blind placebo-controlled clinical trial. Iran. J. Public Health 2015, 44, 228–237. [Google Scholar]
- Hartvigsen, M.L.; Jeppesen, P.B.; Lærke, H.N.; Njabe, E.N.; Knudsen, K.E.; Hermansen, K. Concentrated arabinoxylan in wheat bread has beneficial effects as rye breads on glucose and changes in gene expressions in insulin-sensitive tissues of Zucker diabetic fatty (ZDF) rats. J. Agric. Food Chem. 2013, 61, 5054–5063. [Google Scholar] [CrossRef] [PubMed]
- Ding, Q.; Ren, J.; Zhou, Y.; Bai, Z.; Yan, J.; Na, G.; Shan, Y. Whole grain germinated brown rice regulates intestinal immune homeostasis and gastrointestinal hormones in type 2 diabetic patients-a randomized control trial. Food Funct. 2022, 13, 8274–8282. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.J.; Kendall, C.W.; Augustin, L.S.; Mitchell, S.; Sahye-Pudaruth, S.; Blanco Mejia, S.; Chiavaroli, L.; Mirrahimi, A.; Ireland, C.; Bashyam, B.; et al. Effect of legumes as part of a low glycemic index diet on glycemic control and cardiovascular risk factors in type 2 diabetes mellitus: A randomized controlled trial. Arch. Intern. Med. 2012, 172, 1653–1660. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Yan, H.; Chen, L.; Wang, Y.; Liang, J.; Feng, X.; Hui, S.; Wang, K. Effects of whole grain intake on glycemic control: A meta-analysis of randomized controlled trials. J. Diabetes Investig. 2022, 13, 1814–1824. [Google Scholar] [CrossRef]
- Tindall, A.M.; Johnston, E.A.; Kris-Etherton, P.M.; Petersen, K.S. The effect of nuts on markers of glycemic control: A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2019, 109, 297–314. [Google Scholar] [CrossRef] [Green Version]
- Shinde, S.; Thieu, V.; Kwan, A.; Houghton, K.F.; Schapiro, D.; Meyers, J. 952-P: The Relationship between Weight Loss and HbA1c in People with Type 2 Diabetes. Diabetes 2022, 71 (Suppl. S1), 952–P. [Google Scholar] [CrossRef]
- Winham, D.M.; Thompson, S.V.; Heer, M.M.; Davitt, E.D.; Hooper, S.D.; Cichy, K.A.; Knoblauch, S.T. Black Bean Pasta Meals with Varying Protein Concentrations Reduce Postprandial Glycemia and Insulinemia Similarly Compared to White Bread Control in Adults. Foods 2022, 11, 1652. [Google Scholar] [CrossRef]
- Ma, J.; Stevens, J.E.; Cukier, K.; Maddox, A.F.; Wishart, J.M.; Jones, K.L.; Clifton, P.M.; Horowitz, M.; Rayner, C.K. Effects of a protein preload on gastric emptying, glycemia, and gut hormones after a carbohydrate meal in diet-controlled type 2 diabetes. Diabetes Care 2009, 32, 1600–1602. [Google Scholar] [CrossRef] [Green Version]
- Mignone, L.E.; Wu, T.; Horowitz, M.; Rayner, C.K. Whey protein: The “whey” forward for treatment of type 2 diabetes? World J. Diabetes 2015, 6, 1274–1284. [Google Scholar] [CrossRef]
- Xi, H.; Zhou, W.; Sohaib, M.; Niu, Y.; Zhu, R.; Guo, Y.; Wang, S.; Mao, J.; Wang, X.; Guo, L. Flaxseed supplementation significantly reduces hemoglobin A1c in patients with type 2 diabetes mellitus: A systematic review and meta-analysis. Nutr. Res. 2023, 110, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Fornasini Salvador, M.V.; Abril-Ulloa, S.V.; Beltrán Carreño, J.P.; Villacrés, E.; Cuadrado-Merino, L.; Robalino, F.; Sánchez, R.; Ricaurte Ortiz, P.S.; Muñoz, E.B.; Benítez Loza, N.B.; et al. Efficacy of a Lupinus mutabilis Sweet snack as complement to conventional type 2 diabetes mellitus treatment. Eficacia de un tentempié de Lupinus mutabilis Sweet como complemento al tratamiento convencional de la diabetes mellitus tipo 2. Nutr. Hosp. 2019, 36, 905–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, N.C.; Mori, T.A.; Beilin, L.J.; Johnson, S.; Williams, C.; Gan, S.K.; Puddey, I.B.; Woodman, R.; Phillips, M.; Connolly, E.; et al. The effect of regular consumption of lupin-containing foods on glycaemic control and blood pressure in people with type 2 diabetes mellitus. Food Funct. 2020, 11, 741–747. [Google Scholar] [CrossRef] [PubMed]
- DeFelice, S.L.; FIM Rationale and Proposed Guidelines for the Nutraceutical Research & Education Act—NREA, 10 November 2002. Foundation for Innovation in Medicine. Available online: http://www.fimdefelice.org/archives/arc.researchact.html (accessed on 23 May 2023).


{kind=link}
| Food | Year and Country/Type of Review (Total Number of References) | Objective(s) | Examples of Clinical Evidence | Main Findings: Effect on Type 2 Diabetes and Other Related Diseases |
|---|---|---|---|---|
| Blueberries [13] | Canada, United Kingdom, USA, Spain Narrative review (n = 198 references) | To review the role of blueberries in cardiometabolic health. | Biomarkers: improved insulin sensitivity, plasma lipid profiles and reduced plasma markers of oxidative stress (for both short- and long-term interventions). | A reduced risk of type 2 diabetes, cardiovascular disease, weight gain and death were reported. As well, neuroprotection and vision (in less extended) benefits. |
| Bilberry [14] | China Narrative review (n = 100 references) | To review the potential effects of bilberry supplementation on metabolic and cardiovascular risk factors. | Anti-inflammatory and hypoglycemic effects (e.g., decreased postprandial glycaemia and insulin level). Improvement of hyperlipidaemia: increased HDL cholesterol and decreased LDL cholesterol. Reduced blood pressure. | Bilberry supplementation can present a positive effect on metabolic and cardiovascular risk factors. |
| Red Raspberry (RR) [15] | USA Narrative review (n = 60 references) | To investigate the potential metabolic benefits of dietary red raspberry in individuals with T2DM and prediabetes. | The consumption of 250 g of frozen RR with a high-fat breakfast meal reduced postprandial plasma glucose levels and area under the curve (AUC): individuals with either T2DM or prediabetes and overweight or obesity (2 RCTs). Reduction of low-density lipoprotein cholesterol (LDL-c) (32 RCT). | Improvements in glycaemia profile and insulin sensitivity, adiposity, lipid profiles, ectopic lipid accumulation, inflammation, oxidative stress and cardiac health. |
| Berries * [16] | Poland Narrative review, with application of PRISMA flow diagram (n = 329 references) | To summarise both clinical and non-clinical findings that the consumption of berries, berry extracts, purified compounds, juices, jams, jellies and other berry byproducts aided in the prevention or otherwise management of T2DM. | Glucose-lowering and insulin sensitivity improvements. Lower of dyslipidaemia markers. Anti-obesity. Reduced oxidative stress markers. Improvement in endothelial function of subjects with metabolic syndrome. Anti-inflammatory and anti-hypertensive. Daily recommended dose: 200 to 400 g (70 kg; middle-aged person). Reduction of HbA1c was reported with berries in some studies (strawberries, raspberry and Acai berries). | The consumption of berry products is effective to prevent and control metabolic hyperglycaemic and hyperlipidaemic conditions. |
| Food with polyphenols [17] | China Narrative review (n = 159 references) | To analyse how dietary polyphenols affect starch digestion. | Polyphenols can directly inhibit key digestive enzymes (α-glucosidase) and bind with starch; bounded polyphenols are still able to show the inhibitory activity against the enzymes (in vitro studies). | A better postprandial hyperglycaemia profile by polyphenols may be explained by both inhibited starch digestion and impact on glucose transport. |
| Foods with polyphenols * [18] | Italy Narrative review (n = 136 references) | To discuss the effect of polyphenol/phenolic compounds on the main cardiometabolic risk factors. | Epidemiological studies: polyphenol-rich diets seem to benefit the prevention of T2DM risk. Medium-term clinical trials (6–8 weeks) improve blood glucose, lipids and blood pressure (individuals with and without T2DM). Best results for long-term RCTs, with polyphenol-rich foods and beverages. Improvement of HbA1c (green tea, catechins or total polyphenols intake) in some trials. | Different polyphenol food subclasses seem to present a pleiotropic effect on cardiometabolic risk factors. Fasting glucose, insulin or HbA1c can be improved according to some trials. |
| Grapes and their derivatives (wine) [19] | Italy, Germany, Australia, France, Greece Narrative review (n = 62 references) | To confirm whether there is a difference between alcoholic beverages in inducing beneficial health effects in T2DM individuals and whether the consumption of alcoholic beverages can be included in the daily diet of diabetics. | A reduced risk of T2DM with light to moderate wine consumption (ten studies). | Wine was the alcoholic beverage with the most favourable outcomes. Light/moderate wine consumption is associated with improved metabolic control in T2DM individuals. |
| Short- and long-term intake of fermented dairy products * [20] | Canada, UAE, USA Narrative review (n = 47) | To evaluate the evidence from a cross-sectional analysis of longitudinal studies and human and animal experimental trials to further understand the current knowledge linking short- and long-term consumption of fermented dairy products to T2DM. | Cohort studies: protective effect of fermented dairy products on the prevention and control of T2DM, especially with yoghurt’s potential to decrease insulin resistance and improve glycemic control: improved glucose tolerance, fasting blood sugar, HbA1c (1.2% to 2% reduction) and 2 h postprandial glucose. | Higher intake of fermented dairy products may decrease the risk of developing T2DM in the long term. In the short term, improvements in the glycaemic control markers were also achieved. Yoghurt was the most consistent food protecting against T2DM. |
| Dairy products and plant proteins (e.g., legumes and soy) [21] | Italy and USA Systematic review (n = 50) | To evaluate the ideal protein quality and quantity and the dietary composition for the prevention and metabolic control of T2DM. | RR (relative risk) 95% CI of T2DM: 0.89 (0.84–0.94) total dairy products, 0.87 (0.78–0.96) whole milk, 0.83 (0.70–0.98) yoghurt and 0.74 (0.59–0.93) soy (women). | Higher intake of plant protein and dairy products is associated with a modestly reduced risk of T2DM. Red meat, processed protein foods and high-fat dairy products could have negative effects in the long term. |
| Both dairy and not-dairy products fortified with vitamin D * [22] | Iran and UK Systematic review and meta-analyses (n = 48) | To evaluate effects of Vitamin D fortification on indices of glycaemic control. | In total, 11 RCTs; the impact of enriched food with vitamin D (100 IU to 28,000 IU vitamin/day) on fasting serum glucose in diabetics was significant (mean difference: −2.772, p = 0.041, and 95% CI: −5.435 to −0.109) as well as on serum insulin (mean difference: −2.937; 95% CI:−4.695 to −1.178). | Vitamin D fortification of dairy products leads to an improvement in Homeostasis Model Assessment of Insulin Resistance (HOMA-IR), fasting plasma glucose and HbA1C. |
| Fermented dairy products (FDFs) and probiotic supplementation * [23] | Spain Systematic review and meta-analysis (n = 107) | To study the relation between the regular consumption of FDFs and cardiometabolic diseases (CMD) risk factors (assessed by prospective cohort studies–PCSs), and the effect of probiotic supplementation added into a dairy matrix on CMD parameters (evaluated by RCTs). | In total, 20 PCSs and 52 RCTs. Probiotic intake in capsule/powder displayed a significant reduction on HbA1c changes. However, the effects of probiotic supplementation into a dairy matrix on diabetic parameters in T2DM subjects did not show significant results, regarding the alterations of fasting insulin, HbA1c and plasma CRP. | Yoghurt intake: reduced risk of T2DM and metabolic syndrome development. Fermented milk: reduced cardiovascular risk. Probiotic supplementation added into dairy matrices: can reduce lipid concentrations and anthropometric parameters. Probiotic capsule/powder supplementation: can favour T2DM management and reduce anthropometric parameters. |
| Yoghurt (enriched with probiotics) * [24] | Greece Narrative review (n = 97) | To present the RCTs which have been conducted in the last decade in patients with T2DM. | Significant reductions of HbA1 were reported in some trials. However, the number of trials is limited. Enrichment of yoghurts with vitamin D, calcium and probiotics (e.g., L. acidophilus and B. lactis during a short period of 4–12 weeks). Yoghurt enriched in flaxseed or complex B vitamins may have impact on glycaemia control. | The daily intake of yoghurt, especially when enriched with probiotics, vitamin D and calcium has a positive impact on the metabolic control of diabetic patients. |
| Fermented dairy (FD) foods rich in probiotics (e.g., cheese and yoghurt) [25] | Spain Narrative review (n = 76) | To evaluate the relationship between the FD products: yoghurt and cheese, and cardiometabolic risk factors obtained from meta-analyses, systematic reviews of prospective cohort studies (PCSs). | In all, 13 PCSs supported a potential protective role of yoghurt consumption and prevention of T2DM. Reduction in the risk of T2DM: 14% with a yoghurt intake of 80 g/d compared with no yoghurt intake and 22% with a yoghurt intake of 200 g/d (meta-analyses of PCSs). | Intake of yoghurt seems to be associated with a lower risk of developing type 2 diabetes. A lower risk of developing stroke and cardiovascular disease may be explained by the total consumption of FD. |
| Probiotics * [26] Dairy medium (e.g., goat’s milk, kefir and yoghurt); enriched with multiple probiotic strains). | USA Systematic review (n = 65) | To evaluate nine randomised controlled trials that tested the effects of probiotics on glycaemic outcomes and insulin resistance. | Nine randomised controlled trials. Improvement of insulin resistance; reduction of FPG, A1c, FPI and HOMA-IR with probiotic supplementation among subjects withT2DM. | Probiotic (dairy products and capsules) supplementation seems to favour metabolic control in adults with T2DM. |
| Whole cereals (e.g., wheat, rice, maize, barley, sorghum, millet, oat, rye, buckwheat) [27] | China, USA Narrative review (n = 384) | To highlight recent findings on the influences of both bioactive constituents and processing on the anti-diabetic effects and physiological properties of cereals. | The bioactive components of whole cereals, such as resistant starch, dietary fibre or β-glucan can contribute to reducing postprandial serum glucose and increasing insulin sensitivity. | Reduced risk of T2DM, with improvement of metabolic metabolism and lipidic profile. |
| Whole grains [28] | Italy, UK, Netherlands, Australia Systematic review (n = 75) | To systematically review current evidence on whole grain consumption and various health outcomes provided from meta-analyses of observational studies. | Whole grain consumption improves acute postprandial glucose and insulin homeostasis compared to similar refined foods in healthy subjects (meta-analysis of RCTs). | Strongest evidence: a decreased risk of T2DM and colorectal cancer with higher compared to lower dietary intake of whole grains. Possible: decreased risk of colon cancer, fatal coronary heart disease and cardiovascular disease (CVD) mortality. |
| Whole grains’ phenolic acids and dietary fibre (wheat, barley, oats, rice and buckwheat) [29] | China Narrative review (n = 172) | To review the existing literature on the linkages between the consumption of whole grains and the development of the following chronic non-communicable diseases: CVDs, obesity, T2DM and cancer. | Clinical and epidemiological studies support a positive association between the consumption of whole grains, phenolic acids and dietary fibres with a lower risk of disease. For instance, three or more servings of whole grains/day (20–30% lower risk of diseases). | The consumption of whole grains reduces the risk of CVDs, obesity, T2DM and cancer, with improved glycaemic control, and prevention of insulin resistance. |
| Dietary fibre and whole grains * [30] | New Zealand Systematic review and meta-analyses (n = 97) | To evaluate the role of high-fibre diets on mortality and increasing fibre intake on glycaemic control and other cardiometabolic risk factors of adults with prediabetes or diabetes. | Higher intakes of dietary fibre produced a reduced risk of premature mortality (prospective cohort studies) and improvement of glycaemic control and other risk factors for cardiovascular disease, such as cholesterol levels, HbA1c and body weight (controlled trials). | Improvement of glycaemic control and other risk factors for cardiovascular disease, such as cholesterol levels and body weight. Reduction of premature mortality. |
| Nuts (e.g., almonds, Brazil nuts, cashews, hazelnuts, macadamias, pecans, pine nuts, pistachios and walnuts) [31] | Turkey and Spain Narrative review (n = 64) | To provide an overview of recent findings on bioactive constituents, health claims and health benefits of nuts and dried fruits. | Reduction: total cholesterol; LDL-cholesterol; and triacylglycerols. No change: HDL and inflammation. No change/slight reduction: body weight and visceral adiposity (evidence from many studies). Epidemiologic studies (evidence from many studies): reduction of the risk of cardiovascular disease; coronary heart disease; cancer and all-cause mortality. | Nuts (e.g., 30 or 42.5 g/day without added salt or sugars) are potentially relevant to reduce total cholesterol, LDL and triacylglycerols (cardiovascular and coronary heart disease). The evidence regarding diabetes control improvement, including insulin sensitivity, is limited in clinical studies. The consumption of dried fruits presents similar benefits, although the level of evidence is more limited than for nuts. |
| Almond [32] | USA Comprehensive review (n = 131) | To provide an in-depth analysis of the effect of almonds on weight measures, metabolic health biomarkers and outcomes and the colonic microbiota. | RCTs (randomised controlled trials) are not consensual, regarding the benefits for glycaemic and HbA1s, with some studies showing positive results (and others not). | Consistent improvement of blood lipid profiles and modest reductions in blood pressure, but inconsistent and/or insignificant beneficial effects of glycaemic control, and HbA1c. |
| Pistachio [33] | Iran, Australia A systematic review and meta-analysis (n = 44) | To evaluate the effects of pistachio nuts on glycaemic control and insulin sensitivity in patients with T2DM, prediabetes and metabolic syndrome. | In all, 6 RCT; significant reduction in fasting blood glucose (FBG) and homeostasis model assessment of insulin resistance, but no significant improvement was observed with regard to hemoglobin A1c and fasting plasma insulin level. | Pistachio nuts might cause a significant reduction in fasting blood glucose and HOMA-IR, although HbA1c and fasting plasma insulin might not significantly improve. |
| Proteins * (especially plant protein rich diets) [34] | Germany, Australia, Finland, Sweden, Norway, Greece, Canada, USA, Croatia, Spain, Denmark Narrative review (n = 53) | To review the literature regarding protein intakes. | For instance, plant protein diet containing 65% plant protein, including 30% soy protein and 35% animal protein vs. control diet containing 30% plant and 70% animal protein (n = 41 participants); improvement in fasting glucose. Weight loss reduced HbA1c in all studies, although without significant differences between groups (high vs. low protein groups). | Protein rich diets, especially plant protein rich diets, improve the total levels of cholesterol and fasting blood glucose levels. High protein hypocaloric diets may moderately favour weight loss, when compared to lower protein hypocaloric diets, with a possible improvement in HbA1c and systolic and diastolic blood pressure. |
| Beans [35] | USA Narrative review (n = 96) | To provide an overview of the benefits of plant-based eating, with a concise focus on the nutritional properties unique to dry beans and their connection to improved health parameters of obesity including cardiovascular, metabolic, gastrointestinal gut health and low-grade inflammation. | Coronary heart disease (CHD) risk reduction and improved glycaemic control in T2DM patients. | The inclusion of beans in a plant-based diet presents a protective cardiovascular, metabolic and colon effect; improvement of obesity; management of immune-related disease and low-grade inflammation. |
| Chickpeas/Hummus (i.e., primarily chickpeas and tahini) [36] | USA Comprehensive review (n = 86) | To provide a comprehensive review of the scientific evidence examining the effects of acute and long-term consumption of hummus and hummus ingredients on diet quality and risk factors related to T2DM, cardiovascular disease and obesity. | Healthy adults (n = 10) consumed hummus (28, 56, 112, 259 g servings) with and without white bread vs. white bread alone: postprandial glucose AUC was lower for hummus alone < hummus and white bread < white bread alone. The 28 and 112 g servings of hummus also resulted in lower insulin AUC than the white bread serving (both, p < 0.05), but not with the 259 g serving (p > 0.05). | Improvement of postprandial glycaemic control, fasting lipids, appetite control and daily food intake with hummus compared to other consumed foods, such as white bread. Tahini showed a little impact on glucose control. |
| Whey protein * [37] | Iran A systematic review and meta-analysis (n = 54) | To assess the effects of whey protein on serum lipoproteins and glycaemic status in patients with metabolic syndrome (MetS) and related disorders. | Twenty-two studies: significant reduction of HbA1c, insulin and HOMA-IR, triglycerides levels, total cholesterol, LDL-cholesterol levels and total cholesterol/HDL cholesterol ratio. | The consumption of whey protein can improve HbA1c, insulin, HOMA-IR, triglycerides, total cholesterol, LDL cholesterol and total/HDL-cholesterol ratio in patients with MetS and related disorders. |
| Sunflower seeds and flax seeds [38] | Pakistan Narrative review (n = 21) | To determine the effect of sunflower seeds and flax seeds on T2DM. | For instance, 20 g/day of flaxseeds for three months reduced FPG concentrations, insulin resistance and insulin sensitivity. | Sunflower and flax seeds consumption can reduce glucose levels with better insulin resistance and improved insulin production. |
| Cabbage [39] | Mexico Narrative review (n = 201) | To analyse the effects of cabbage, and its bioactive compounds, on glucose homeostasis. | Improvement of glucose levels and oxidative stress and hypolipaemic markers. | Cabbage consumption can regulate glucose homeostasis. |
| Lupin * [40] | Australia, Systematic review (n = 37) | To investigate the effects of lupin on a range of health outcome measures. | There were 21 studies (998 participants): statistically significant decrease of glucose AUC in some studies. Benefits, such as satiety, glycaemic control or improved serum lipid profile and blood pressure were better with whole lupin. | The benefits on glycaemic control and serum lipid profile were moderate. |
| Prickly pear cacti (Opuntia spp.) cladodes [41] | Australia, UK, Greece, Italy Narrative review (n = 73) | To summarise the latest findings on the consumption of the prickly pear (PP; Opuntia spp.) cladode as a potential nutritional tool for the management of hyperglycaemia. | Reduction of glucose levels after prickly pear cladodes’ consumption (mainly acute studies). | Prickly pear cladodes show potential hypoglycaemic effects. |
| Honey [42] | Italy Narrative review (n = 112) | To summarise the current literature concerning the beneficial effects of honey in the management of the obesity-related dysfunctions, including neurodegeneration. | Honey significantly reduced plasma glucose concentration (especially, in the short term). However, plasma levels of haemoglobin A1c increased, after 8-week honey consumption in one clinical study. | Honey seems to improve glycaemic control and lipidic profile (honey acute effects/short term). Long-term clinical studies are limited. |
| ‘Superfoods’ | Examples | Reference(s) |
|---|---|---|
| Foods with polyphenols | Berries, tea, coffee, wine or grapes | [13,14,15,16,17,18,19] |
| Fermented dairy products | Yoghurt (fortified or not with vitamin D or probiotics) | [20,21,22,23,24,25,26] |
| Whole cereals/grains | Mixed grains, barley or oatmeal | [27,28,29,30] |
| Nuts | Almonds, Brazil nuts, cashews, hazelnuts, macadamias, pecans, pine nuts, pistachios and walnuts | [31,32,33] |
| Proteins (especially, plant protein-rich diets) | Chickpeas (e.g., hummus), beans or other proteins–whey protein | [34,35,36,37] |
| Other foods | Sunflower seeds and flax seeds; cabbage; lupin, prickly pear cacti (Opuntia spp.) cladodes and honey (especially for short-term use) | [38,39,40,41,42] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pires, C. Superfoods for Type 2 Diabetes: A Narrative Review and Proposal for New International Recommendations. Medicina 2023, 59, 1184. https://doi.org/10.3390/medicina59071184
Pires C. Superfoods for Type 2 Diabetes: A Narrative Review and Proposal for New International Recommendations. Medicina. 2023; 59(7):1184. https://doi.org/10.3390/medicina59071184
Chicago/Turabian StylePires, Carla. 2023. "Superfoods for Type 2 Diabetes: A Narrative Review and Proposal for New International Recommendations" Medicina 59, no. 7: 1184. https://doi.org/10.3390/medicina59071184