

Cleaning and Disinfecting Oval-Shaped Root Canals: Ex Vivo Evaluation of Three Rotary Instrumentation Systems with Passive Ultrasonic Irrigation

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
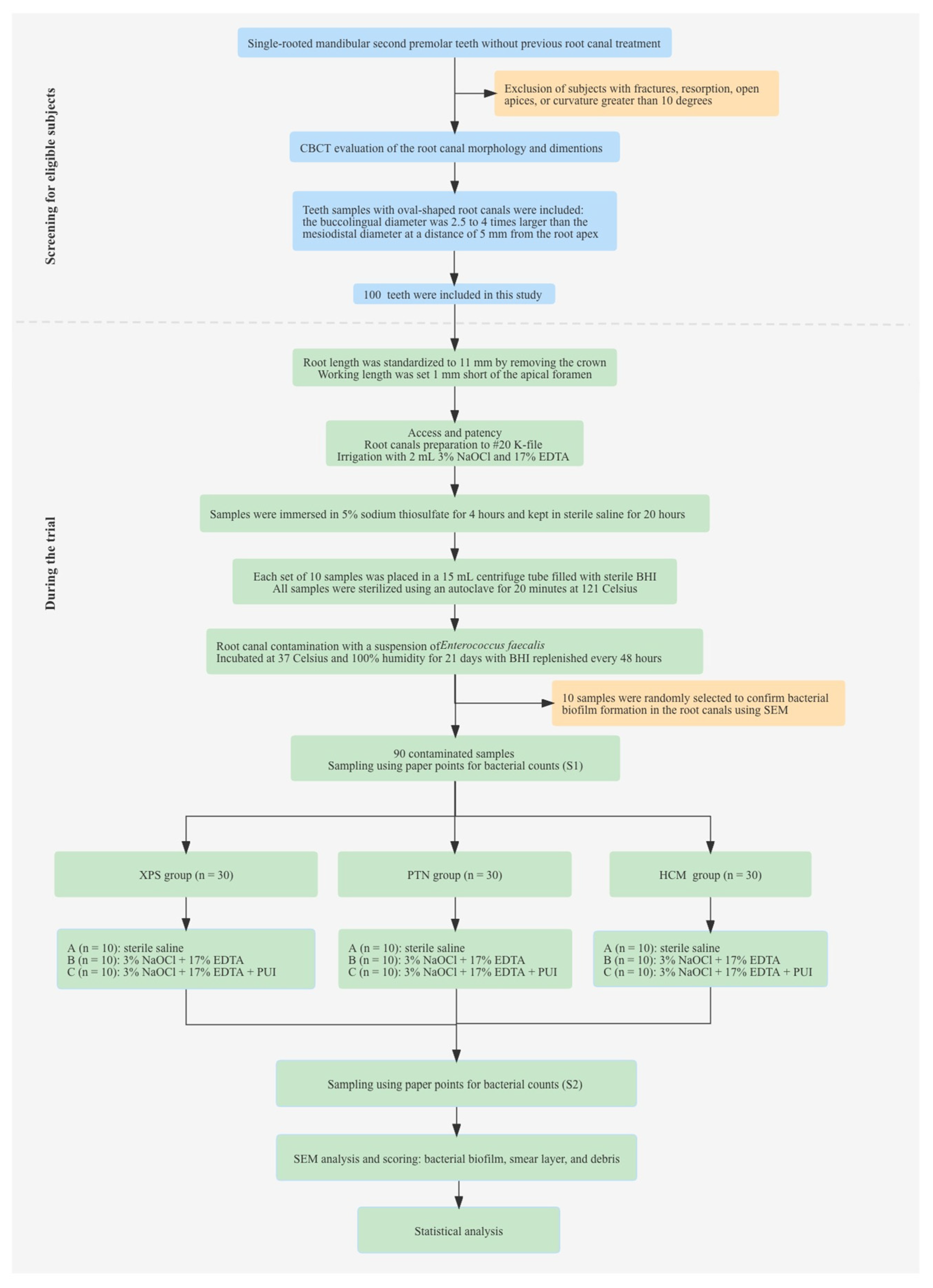
2.1. Samples Size Calculation and Selection
2.2. Samples Preparation and Sterilization
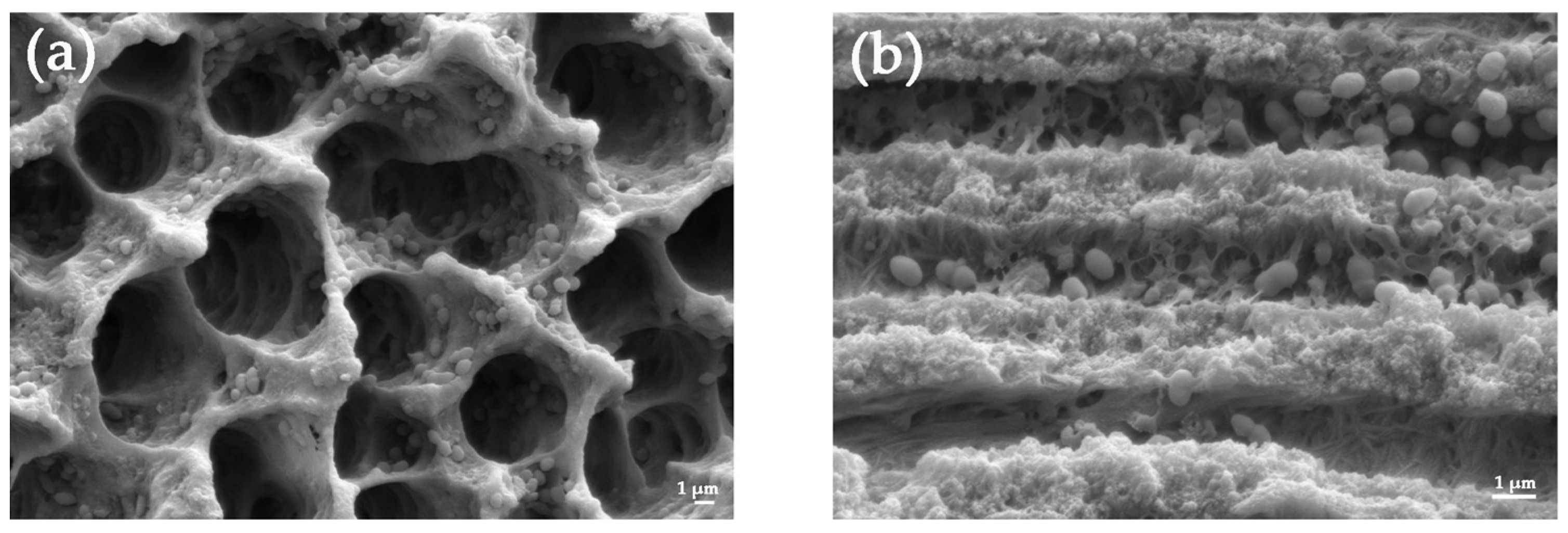
2.3. Root Canal Contamination with Enterococcus faecalis
2.4. Root Canal Instrumentation and Bacterial Sampling
2.5. Scanning Electron Microscope Analysis
- No bacteria on the surface of the root canal;
- Isolated bacteria over the surface with no signs of viability/organization (mitosis, biofilm matrix);
- Agglomeration of bacteria with signs of viability/organization (mitosis, biofilm, matrix);
- More than 50% of the root canal walls were covered with viable bacteria;
- Complete or nearly complete root canal wall coverage with viable bacteria.
- Clean root canal wall, only a few small debris particles;
- Few small agglomerations of debris, less than 25%;
- Many agglomerations of debris covering less than 50% of the root canal wall;
- More than 50% of the root canal wall covered by debris;
- Complete or nearly complete root canal wall covered by debris, more then 75%.
- No smear layer, more then 90% dentinal tubules open;
- Small amount of smear layer, some dentinal tubules open, more then 50%;
- Homogenous smear layer covering the root canal wall, only few dentinal tubules open;
- Complete root canal wall covered by a homogenous smear layer, less then 25% dentinal tubules open;
- Heavy, nonhomogenous smear layer covering the complete root canal wall, no open dentinal tubule.
2.6. Statistical Analysis
3. Results
3.1. Bacterial Counts before and after Chemomechanical Preparation
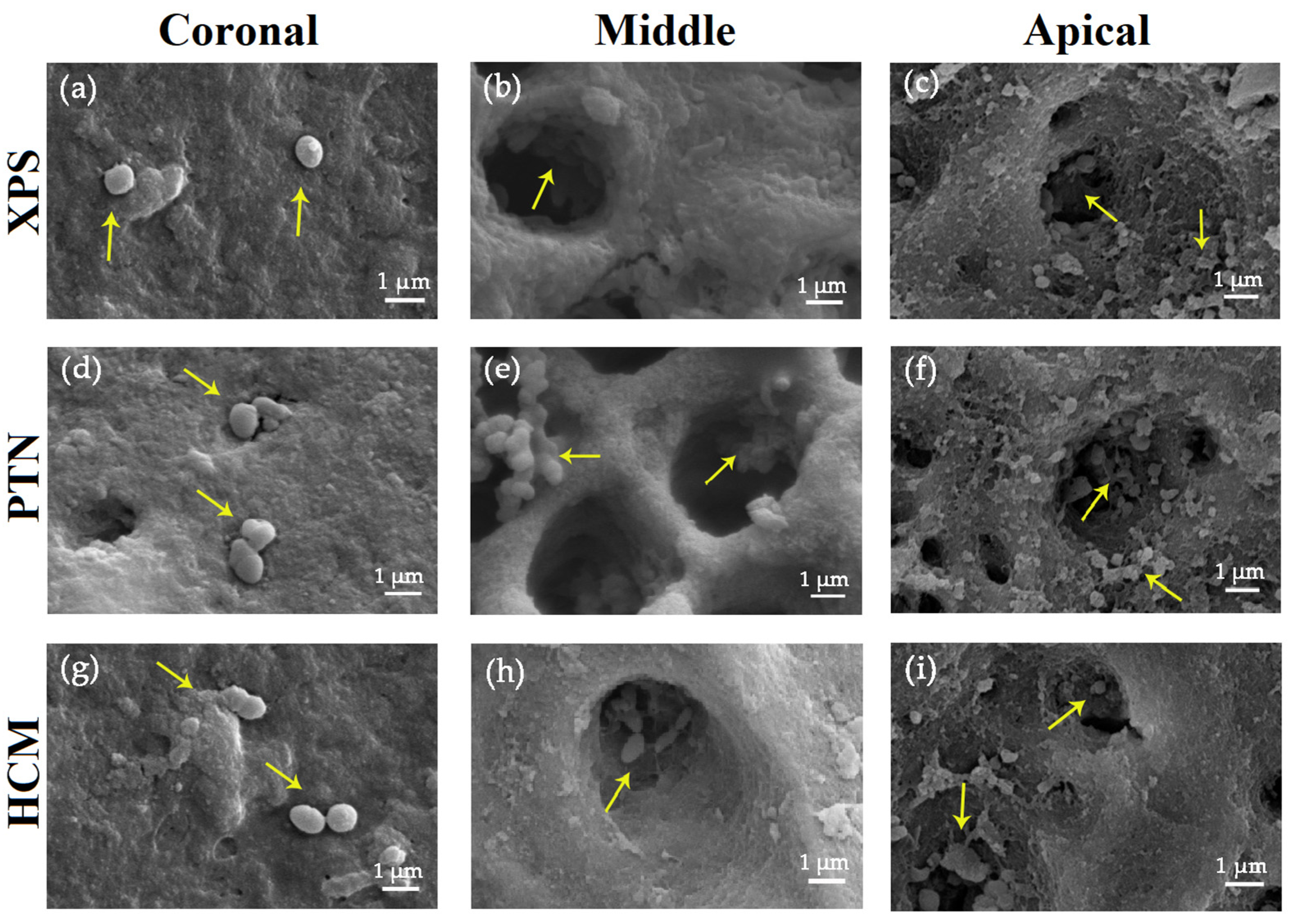
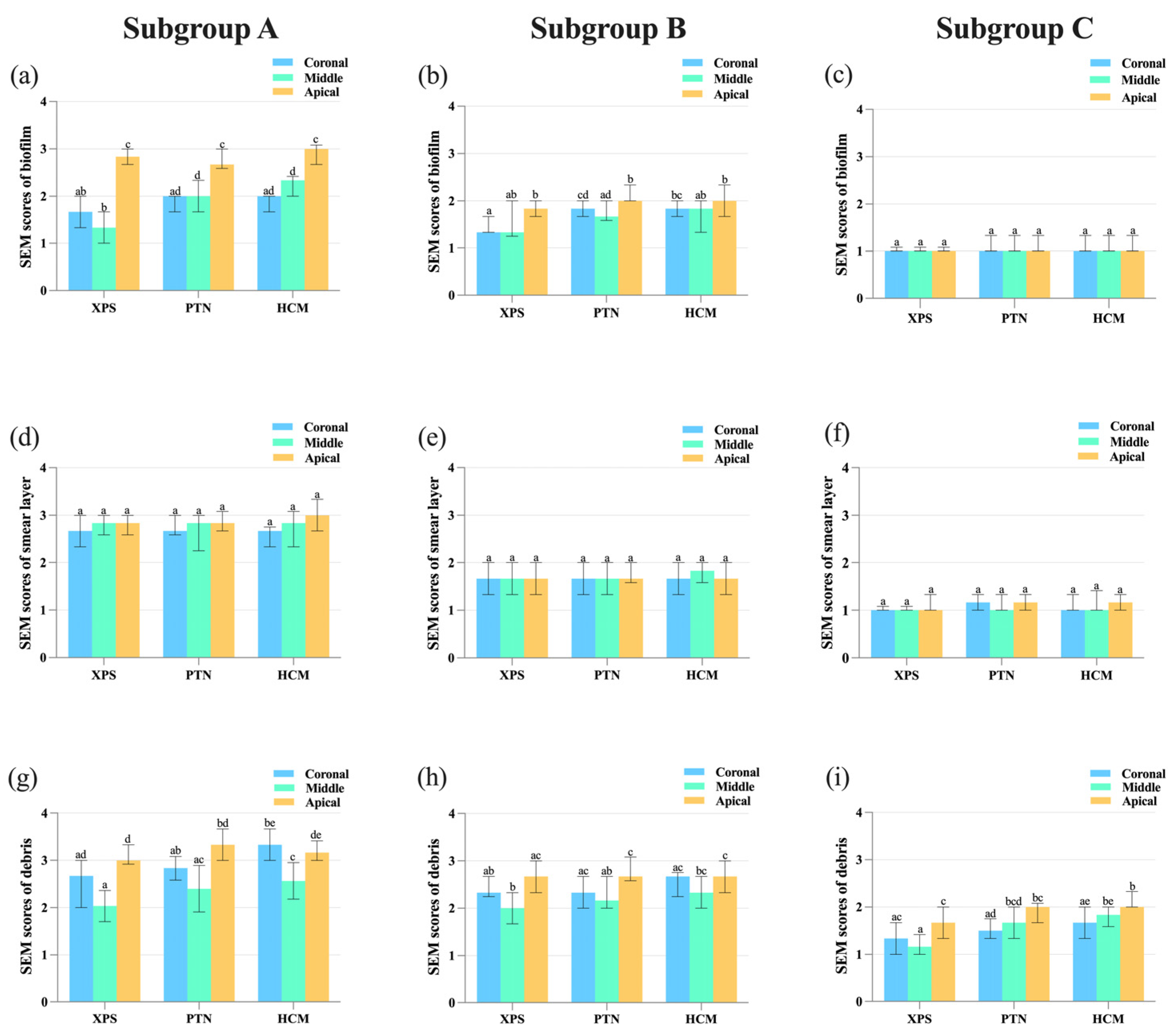
3.2. Assessment of the Effectiveness in Eliminating Bacterial Biofilm
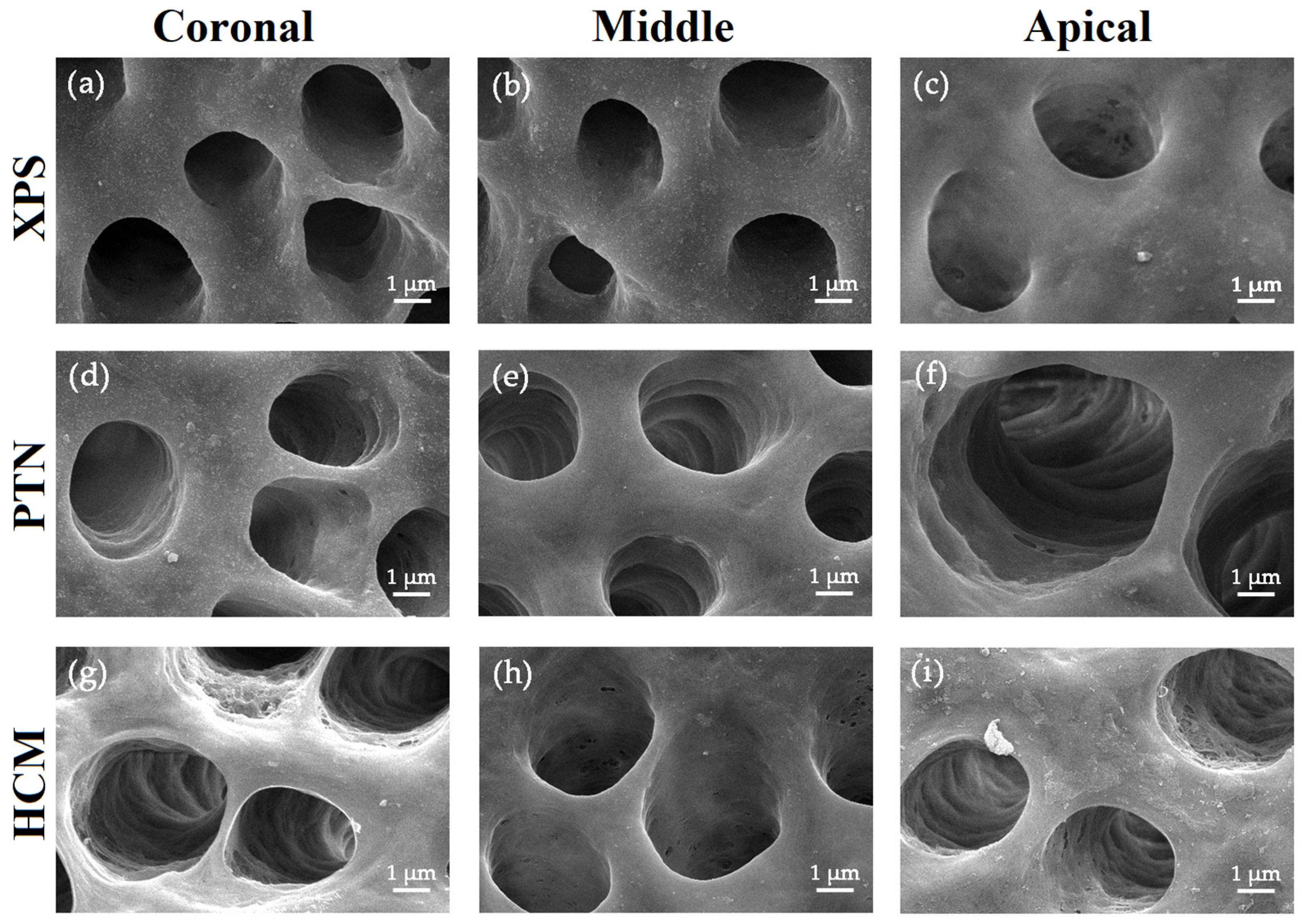
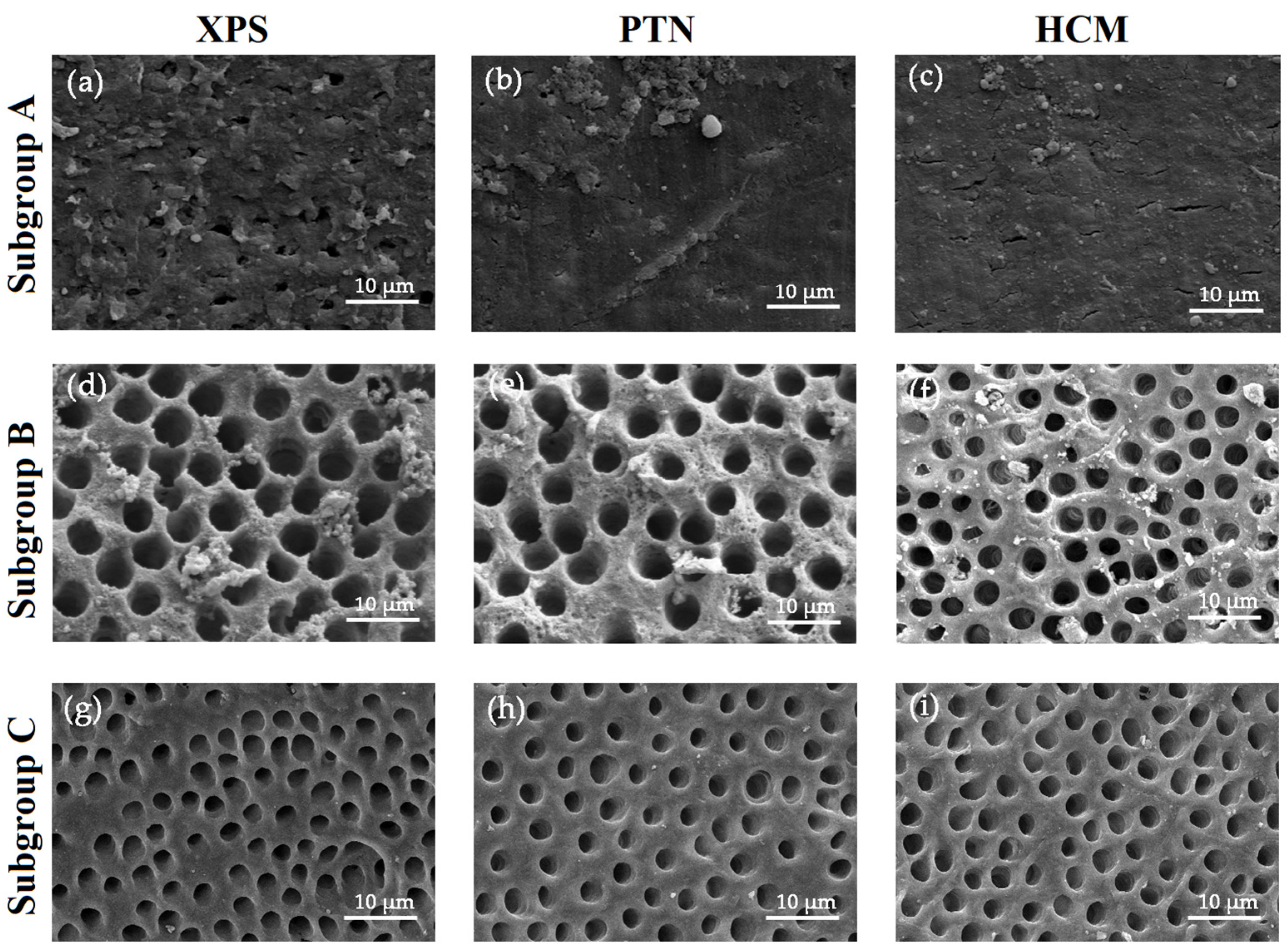
3.3. Assessment of the Effectiveness in Removing the Smear Layer
3.4. Assessment of the Effectiveness in Cleaning Hard Tissue Debris
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siqueira, J.F., Jr.; Pérez, A.R.; Marceliano-Alves, M.F.; Provenzano, J.C.; Silva, S.G.; Pires, F.R.; Vieira, G.C.S.; Rocas, I.N.; Alves, F.R.F. What happens to unprepared root canal walls: A correlative analysis using micro-computed tomography and histology/scanning electron microscopy. Int. Endod. J. 2018, 51, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, H.; Zhang, L.; Hieawy, A.; Shen, Y. Evaluation of extracellular polymeric substances matrix volume, surface roughness and bacterial adhesion property of oral biofilm. J. Dent. Sci. 2023, in press. [Google Scholar] [CrossRef]
- Liu, H.; Shen, Y.; Wang, Z.; Haapasalo, M. The ability of different irrigation methods to remove mixtures of calcium hydroxide and barium sulphate from isthmuses in 3D printed transparent root canal models. Odontology 2022, 110, 27–34. [Google Scholar] [CrossRef]
- Wu, M.K.; R'oris, A.; Barkis, D.; Wesselink, P.R. Prevalence and extent of long oval canals in the apical third. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2000, 89, 739–743. [Google Scholar] [CrossRef]
- Papic, M.; Papic, M.; Zivanovic, S.; Vuletic, M.; Zdravkovic, D.; Misic, A.; Miletic Kovacevic, M.; Popovic, M. The prevalence of oval-shaped root canals: A morphometric study using cone-beam computed tomography and image analysis software. Aust. Endod. J. 2022, 48, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Boschetti, E.; Silva-Sousa, Y.T.C.; Mazzi-Chaves, J.F.; Leoni, G.B.; Versiani, M.A.; Pécora, J.D.; Saquy, P.C.; Sousa-Neto, M.D. Micro-CT evaluation of root and canal morphology of mandibular first premolars with radicular grooves. Braz. Dent. J. 2017, 28, 597–603. [Google Scholar] [CrossRef]
- Lui, K.; Liu, H.; Wang, H.; Yang, X.; Huang, D.; Zhou, X.; Gao, Y.; Shen, Y. An application framework of 3D assessment image registration accuracy and untouched surface area in canal instrumentation laboratory research with micro-computed tomography. Clin. Oral. Investig. 2023, 27, 715–725. [Google Scholar] [CrossRef]
- Versiani, M.A.; Carvalho, K.K.T.; Mazzi-Chaves, J.F.; Sousa-Neto, M.D. Micro-computed tomographic evaluation of the shaping ability of XP-endo Shaper, iRaCe, and EdgeFile systems in long oval-shaped canals. J. Endod. 2018, 44, 489–495. [Google Scholar] [CrossRef]
- Liu, H.; Lai, W.W.M.; Hieawy, A.; Gao, Y.; Haapasalo, M.; Tay, F.R.; Shen, Y. Efficacy of XP-endo instruments in removing 54 month-aged root canal filling material from mandibular molars. J. Dent. 2021, 112, 103734. [Google Scholar] [CrossRef]
- Liu, H.; Shabehpour, K.; Wang, Z.; Sobotkiewicz, T.; Kwak, S.W.; Haapasalo, M.; Ruse, N.D.; Coil, J.M.; Tay, F.R.; Shen, Y. Characterisation of deformed or separated nickel-titanium retreatment instruments after clinical use—A multicentre experience: Defect profiles of clinically-used retreatment instruments. J. Dent. 2022, 117, 103939. [Google Scholar] [CrossRef]
- Azim, A.A.; Piasecki, L.; da Silva Neto, U.X.; Cruz, A.T.G.; Azim, K.A. XP Shaper, a novel adaptive core rotary instrument: Micro-computed tomographic analysis of its shaping abilities. J. Endod. 2017, 43, 1532–1538. [Google Scholar] [CrossRef]
- Wang, L.X.; Chen, H.; Lin, R.T.; Gu, L.S. Influence of pecking frequency at working length on the volume of apically extruded debris: A micro-computed tomography analysis. J. Dent. Sci. 2022, 17, 1274–1280. [Google Scholar] [CrossRef]
- Velozo, C.; Silva, S.; Almeida, A.; Romeiro, K.; Vieira, B.; Dantas, H.; Sousa, F.; De Albuquerque, D.S. Shaping ability of XP-endo Shaper and ProTaper Next in long oval-shaped canals: A micro-computed tomography study. Int. Endod. J. 2020, 53, 998–1006. [Google Scholar] [CrossRef]
- Dantas, W.C.F.; Marceliano-Alves, M.F.V.; Marceliano, E.F.V.; Marques, E.F.; de Carvalho Coutinho, T.M.; Alves, F.R.F.; Martin, A.S.; Pelegrine, R.A.; Lopes, R.T.; Bueno, C. Microtomographic assessment of the shaping ability of the Hyflex CM and XP-endo Shaper systems in curved root canals. Eur. J. Dent. 2022, in press. [Google Scholar] [CrossRef]
- Martins, J.N.R.; Silva, E.J.N.L.; Marques, D.; Belladonna, F.; Simões-Carvalho, M.; Camacho, E.; Braz Fernandes, F.M.; Versiani, M.A. Comparison of design, metallurgy, mechanical performance and shaping ability of replica-like and counterfeit instruments of the ProTaper Next system. Int. Endod. J. 2021, 54, 780–792. [Google Scholar] [CrossRef] [PubMed]
- Poly, A.; Marques, F.; Moura Sassone, L.; Karabucak, B. The shaping ability of WaveOne Gold, TRUShape and XP-endo Shaper systems in oval-shaped distal canals of mandibular molars: A microcomputed tomographic analysis. Int. Endod. J. 2021, 54, 2300–2306. [Google Scholar] [CrossRef] [PubMed]
- Vieira, G.C.S.; Pérez, A.R.; Alves, F.R.F.; Provenzano, J.C.; Mdala, I.; Siqueira, J.F., Jr.; Rocas, I.N. Impact of contracted endodontic cavities on root canal disinfection and shaping. J. Endod. 2020, 46, 655–661. [Google Scholar] [CrossRef]
- Lacerda, M.; Marceliano-Alves, M.F.; Pérez, A.R.; Provenzano, J.C.; Neves, M.A.S.; Pires, F.R.; Goncalves, L.S.; Rocas, I.N.; Siqueira, J.F., Jr. Cleaning and shaping oval canals with 3 instrumentation systems: A correlative micro-computed tomographic and histologic study. J. Endod. 2017, 43, 1878–1884. [Google Scholar] [CrossRef] [PubMed]
- Poly, A.; Tseng, W.L.; Marques, F.; Setzer, F.C.; Karabucak, B. Micro-computed tomographic analysis of the shaping ability of XP-Endo Shaper in oval-shaped distal root canals of mandibular molars. Eur. Endod. J. 2021, 6, 271–277. [Google Scholar]
- Carvalho, K.K.T.; Petean, I.B.F.; Silva-Sousa, A.C.; Camargo, R.V.; Mazzi-Chaves, J.F.; Silva-Sousa, Y.T.C.; Sousa-Neto, M.D. Heat-treated NiTi instruments and final irrigation protocols for biomechanical preparation of flattened canals. Braz. Oral. Res. 2022, 36, e115. [Google Scholar] [CrossRef]
- Orlowski, N.B.; Schimdt, T.F.; Teixeira, C.D.S.; Garcia, L.; Savaris, J.M.; Tay, F.R.; Bortoluzzi, E.A. Smear layer removal using passive ultrasonic irrigation and different concentrations of sodium hypochlorite. J. Endod. 2020, 46, 1738–1744. [Google Scholar] [CrossRef] [PubMed]
- Cai, M.; Cai, Y.; Yang, R.; Xu, Z.; Neelakantan, P.; Wei, X. Impact of agitation/activation strategies on the antibiofilm potential of sodium hypochlorite/etidronate mixture in vitro. BMC Oral. Health 2022, 22, 201. [Google Scholar] [CrossRef] [PubMed]
- Al-Zuhair, H.; Su, Z.; Liu, H.; Wang, Z.; Haapasalo, M.; Hieawy, A.; Gao, Y.; Shen, Y. Antimicrobial effects of agitational irrigation on single- and multispecies biofilms in dentin canals. Odontology 2023, 111, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Fan, W.; Xu, T.; Tay, F.R.; Gutmann, J.L.; Fan, B. Evaluation of several instrumentation techniques and irrigation methods on the percentage of untouched canal wall and accumulated dentine debris in C-shaped canals. Int. Endod. J. 2019, 52, 1354–1365. [Google Scholar] [CrossRef]
- Paranjpe, A.; de Gregorio, C.; Gonzalez, A.M.; Gomez, A.; Silva Herzog, D.; Pina, A.A.; Cohenca, N. Efficacy of the self-adjusting file system on cleaning and shaping oval canals: A microbiological and microscopic evaluation. J. Endod. 2012, 38, 226–231. [Google Scholar] [CrossRef]
- Hulsmann, M.; Rummelin, C.; Schafers, F. Root canal cleanliness after preparation with different endodontic handpieces and hand instruments: A comparative SEM investigation. J. Endod. 1997, 23, 301–306. [Google Scholar] [CrossRef]
- Paque, F.; Balmer, M.; Attin, T.; Peters, O.A. Preparation of oval-shaped root canals in mandibular molars using nickel-titanium rotary instruments: A micro-computed tomography study. J. Endod. 2010, 36, 703–707. [Google Scholar] [CrossRef]
- Chinchiyanont, P.; Yanpiset, K.; Banomyong, D.; Thongbai-On, N. Shaping ability of non-adaptive and adaptive core nickel-titanium single-file systems with supplementary file in ribbon-shaped canals analysed by micro-computed tomography. Aust. Endod. J. 2022, in press. [Google Scholar] [CrossRef]
- Siqueira, J.F., Jr.; Rôças, I.N.; Santos, S.R.; Lima, K.C.; Magalhaes, F.A.; de Uzeda, M. Efficacy of instrumentation techniques and irrigation regimens in reducing the bacterial population within root canals. J. Endod. 2002, 28, 181–184. [Google Scholar] [CrossRef]
- Alves, F.R.F.; Paiva, P.L.; Marceliano-Alves, M.F.; Cabreira, L.J.; Lima, K.C.; Siqueira, J.F., Jr.; Rocas, I.N.; Provenzano, J.C. Bacteria and hard tissue debris extrusion and intracanal bacterial reduction promoted by XP-endo Shaper and Reciproc instruments. J. Endod. 2018, 44, 1173–1178. [Google Scholar] [CrossRef]
- Üreyen Kaya, B.; Erik, C.E.; Sesli Çetin, E.; Köle, M.; Maden, M. Mechanical reduction in intracanal Enterococcus faecalis when using three different single-file systems: An ex vivo comparative study. Int. Endod. J. 2019, 52, 77–85. [Google Scholar] [CrossRef]
- Pawar, A.M.; Pawar, M.; Metzger, Z.; Thakur, B. Apical extrusion of debris by supplementary files used for retreatment: An ex vivo comparative study. J. Conserv. Dent. 2016, 19, 125–129. [Google Scholar] [CrossRef]
- Thomas, A.R.; Velmurugan, N.; Smita, S.; Jothilatha, S. Comparative evaluation of canal isthmus debridement efficacy of modified EndoVac technique with different irrigation systems. J. Endod. 2014, 40, 1676–1680. [Google Scholar] [CrossRef]
- Versiani, M.A.; Alves, F.R.; Andrade-Junior, C.V.; Marceliano-Alves, M.F.; Provenzano, J.C.; Rocas, I.N.; Sousa-Neto, M.D.; Siqueira, J.F., Jr. Micro-CT evaluation of the efficacy of hard-tissue removal from the root canal and isthmus area by positive and negative pressure irrigation systems. Int. Endod. J. 2016, 49, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Curtis, T.O.; Sedgley, C.M. Comparison of a continuous ultrasonic irrigation device and conventional needle irrigation in the removal of root canal debris. J. Endod. 2012, 38, 1261–1264. [Google Scholar] [CrossRef]
- Chan, R.; Versiani, M.A.; Friedman, S.; Malkhassian, G.; Sousa-Neto, M.D.; Leoni, G.B.; Silva-Sousa, Y.T.C.; Basrani, B. Efficacy of 3 supplementary irrigation protocols in the removal of hard tissue debris from the mesial root canal system of mandibular molars. J. Endod. 2019, 45, 923–929. [Google Scholar] [CrossRef]
- Shi, L.; Wan, J.; Yang, Y.; Yao, Y.; Yang, R.; Xie, W. Evolution of the combined effect of different irrigation solutions and activation techniques on the removal of smear layer and dentin microhardness in oval-shaped root canal: An in-vitro study. Biomol. Biomed. 2023, 23, 126–136. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Mu, Y.; Deng, X.; Zhang, S.; Zhou, D. Comparison of the effect of four decalcifying agents combined with 60 °C 3% sodium hypochlorite on smear layer removal. J. Endod. 2012, 38, 381–384. [Google Scholar] [CrossRef]
- Schmidt, T.F.; Teixeira, C.S.; Felippe, M.C.; Felippe, W.T.; Pashley, D.H.; Bortoluzzi, E.A. Effect of ultrasonic activation of irrigants on smear layer removal. J. Endod. 2015, 41, 1359–1363. [Google Scholar] [CrossRef]
- Violich, D.R.; Chandler, N.P. The smear layer in endodontics—A review. Int. Endod. J. 2010, 43, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Martins, J.N.R.; Martins, R.F.; Braz Fernandes, F.M.; Silva, E.J.N.L. What meaningful information are the instruments mechanical testing giving us? A comprehensive review. J. Endod. 2022, 48, 985–1004. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Sterile Saline | 3% NaOCl + 17% EDTA | 3% NaOCl + 17% EDTA + PUI | |||
|---|---|---|---|---|---|---|
| S1 | S2 | S1 | S2 | S1 | S2 | |
| XPS | 6.29 ± 0.25 a | 3.43 ± 0.09 b | 6.00 ± 0.45 a | 1.73 ± 0.26 d | 6.50 ± 0.32 a | 0.34 ± 0.55 e |
| PTN | 6.33 ± 0.22 a | 4.02 ± 0.16 c | 6.12 ± 0.56 a | 2.09 ± 0.40 d | 6.32 ± 0.28 a | 0.75 ± 0.66 e |
| HCM | 6.17 ± 0.25 a | 3.99 ± 0.15 c | 6.46 ± 0.64 a | 2.22 ± 0.27 d | 6.60 ± 0.35 a | 0.62 ± 0.67 e |
| Groups | Sterile Saline | 3% NaOCl + 17% EDTA | 3% NaOCl + 17% EDTA + PUI | |||
|---|---|---|---|---|---|---|
| S1–S2 | Reduction (%) | S1–S2 | Reduction (%) | S1–S2 | Reduction (%) | |
| XPS | 2.87 ± 0.25 | 45.47 a | 4.27 ± 0.36 | 71.17 c | 6.16 ± 0.44 | 94.98 d |
| PTN | 2.31 ± 0.28 | 36.39 b | 4.04 ± 0.50 | 65.97 c | 5.57 ± 0.63 | 88.18 d |
| HCM | 2.18 ± 0.28 | 35.30 b | 4.24 ± 0.63 | 65.33 c | 5.97 ± 0.53 | 90.86 d |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Wang, Z.; Bao, P.; Meng, T.; Liu, M.; Li, H.; Shen, Y.; Liu, D.; Jia, Z.; Liu, H. Cleaning and Disinfecting Oval-Shaped Root Canals: Ex Vivo Evaluation of Three Rotary Instrumentation Systems with Passive Ultrasonic Irrigation. Medicina 2023, 59, 962. https://doi.org/10.3390/medicina59050962
Li Y, Wang Z, Bao P, Meng T, Liu M, Li H, Shen Y, Liu D, Jia Z, Liu H. Cleaning and Disinfecting Oval-Shaped Root Canals: Ex Vivo Evaluation of Three Rotary Instrumentation Systems with Passive Ultrasonic Irrigation. Medicina. 2023; 59(5):962. https://doi.org/10.3390/medicina59050962
Chicago/Turabian StyleLi, Ying, Zhengyang Wang, Pingping Bao, Tingting Meng, Meng Liu, Huixu Li, Ya Shen, Dayong Liu, Zhi Jia, and He Liu. 2023. "Cleaning and Disinfecting Oval-Shaped Root Canals: Ex Vivo Evaluation of Three Rotary Instrumentation Systems with Passive Ultrasonic Irrigation" Medicina 59, no. 5: 962. https://doi.org/10.3390/medicina59050962