
A Systematic Review of Randomized Clinical Trials Evaluating the Efficacy of Minimally Invasive Surgery for Soft Tissue Management: Aesthetics, Postoperative Morbidity, and Clinical Results




Abstract
:1. Introduction
2. Materials and Methods
2.1. Questions
- P = patients requiring soft tissue management;
- I = MIST protocol;
- C = non-MIST protocol;
- O = clinical outcomes, aesthetic results, postoperative morbidity.
2.2. Review Process
2.3. Data Collection
2.4. Risk of Bias
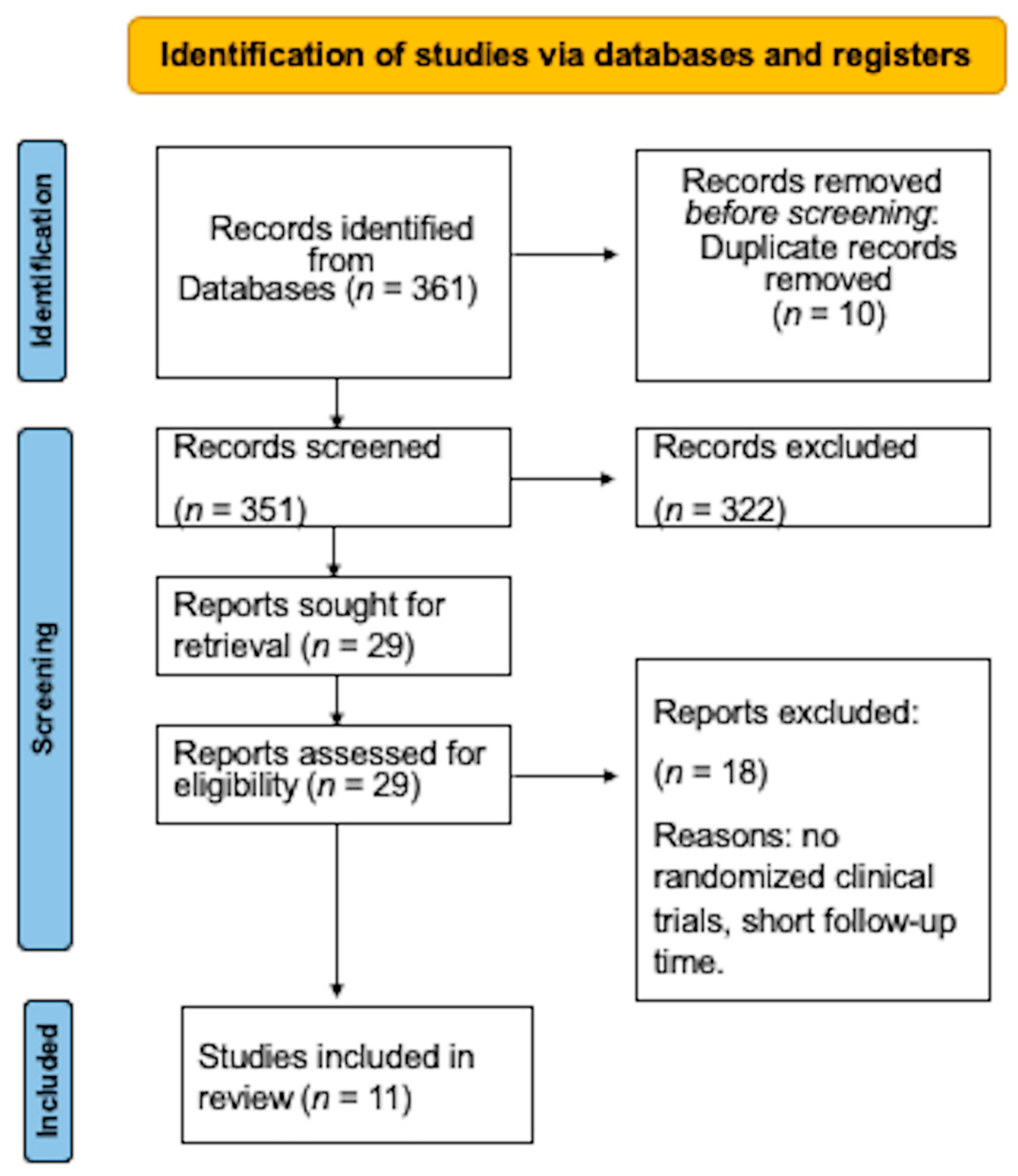
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kaya, K.S.; Türk, B.; Cankaya, M.; Seyhun, N.; Coşkun, B.U. Assessment of facial analysis measurements by golden proportion. Braz. J. Otorhinolaryngol. 2019, 85, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Harrar, H.; Myers, S.; Ghanem, A.M. Art or Science? An Evidence-Based Approach to Human Facial Beauty a Quantitative Analysis Towards an Informed Clinical Aesthetic Practice. Aesthetic Plast. Surg. 2018, 42, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, F.V.; Hirata, D.Y.; Reis, A.F.; Santos, V.R.; Miranda, T.S.; Faveri, M.; Duarte, P.M. Open-flap versus flapless esthetic crown lengthening: 12-month clinical outcomes of a randomized controlled clinical trial. J. Periodontol. 2014, 85, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Cairo, F.; Pagliaro, U.; Nieri, M. Treatment of gingival recession with coronally advanced flap procedures: A systematic review. J. Clin. Periodontol. 2008, 35, 136–162. [Google Scholar] [CrossRef] [PubMed]
- Harrel, S.K. A minimally invasive surgical approach for periodontal bone grafting. Int. J. Periodontics Restor. Dent. 1998, 18, 161–169. [Google Scholar]
- Harrel, S.K. A minimally invasive surgical approach for periodontal regeneration: Surgical technique and observations. J. Periodontol. 1999, 70, 1547–1557. [Google Scholar] [CrossRef]
- Wang, F.; Huang, W.; Zhang, Z.; Wang, H.; Monje, A.; Wu, Y. Minimally invasive flapless vs. flapped approach for single implant placement: A 2-year randomized controlled clinical trial. Clin. Oral Implant. Res. 2017, 28, 757–764. [Google Scholar] [CrossRef]
- Sunitha, R.V.; Sapthagiri, E. Flapless implant surgery: A 2-year follow-up study of 40 implants. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, e237–e243. [Google Scholar] [CrossRef]
- Nevins, M.L.; Camelo, M.; Nevins, M.; Schupbach, P.; Friedland, B.; Camelo, J.M.; Kim, D. Minimally invasive alveolar ridge augmentation procedure (tunneling technique) using rhPDGF-BB in combination with three matrices: A case series. Int. J. Periodontics. Restor. Dent. 2009, 29, 371–383. [Google Scholar]
- Bittencourt, S.; Del Peloso Ribeiro, E.; Sallum, E.A.; Nociti, F.H., Jr.; Casati, M.Z. Surgical microscope may enhance root coverage with subepithelial connective tissue graft: A randomized-controlled clinical trial. J. Periodontol. 2012, 83, 721–730. [Google Scholar] [CrossRef]
- de Campos, G.V.; Bittencourt, S.; Sallum, A.W.; Nociti, F.H., Jr.; Sallum, E.A.; Casati, M.Z. Achieving primary closure and enhancing aesthetics with periodontal microsurgery. Pract. Proced. Aesthetic Dent. 2006, 18, 449–454. [Google Scholar]
- Iglhaut, G.; Allen, E.P.; Sculean, A.; Iglhaut, T.; Nahles, S.; Fretwurst, T. Root Coverage Using a Novel Porcine Acellular Dermal Matrix: Case Reports of Different Minimally Invasive Techniques with a 3-Year Follow-up. Int. J. Periodontics Restor. Dent. 2023, 43, 47–54. [Google Scholar] [CrossRef]
- Cortellini, P.; Tonetti, M.S. Improved wound stability with a modified minimally invasive surgical technique in the regenerative treatment of isolated interdental intrabony defects. J. Clin. Periodontol. 2009, 36, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Trombelli, L.; Farina, R.; Franceschetti, G.; Calura, G. Single-flap approach with buccal access in periodontal reconstructive procedures. J. Periodontol. 2009, 80, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Duffy, J.M.; Latimer, J.M.; Fried, R.M.; Dragan, I.F. Minimally Invasive Coronally Advanced Flap Techniques for Correction of Gingival Recession Defects: A Review. Compend. Contin. Educ. Dent. 2023, 44, 36–41. [Google Scholar]
- Imamura, K.; Suzuki, E.; Takeuchi, T.; Saito, A. Clinical Outcomes of Periodontal Regenerative Therapy Using rhFGF-2 with a Modified Minimally Invasive Surgical Technique for Intrabony Defects: Case Series with a 12-Month Follow-up. Int. J. Periodontics Restor. Dent. 2022, 42, 507–513. [Google Scholar] [CrossRef]
- Windisch, P.; Iorio-Siciliano, V.; Palkovics, D.; Ramaglia, L.; Blasi, A.; Sculean, A. The role of surgical flap design (minimally invasive flap vs. extended flap with papilla preservation) on the healing of intrabony defects treated with an enamel matrix derivative: A 12-month two-center randomized controlled clinical trial. Clin. Oral Investig. 2022, 26, 1811–1821. [Google Scholar] [CrossRef]
- Priyanka, M.; Reddy, K.; Pradeep, K. Efficacy of rh-PDGF-BB and Emdogain with or without DFDBA using M-MIST in the treatment of intrabony defects. Niger. J. Clin. Pract. 2023, 26, 116–124. [Google Scholar]
- Rajendran, V.; Uppoor, A.; Kadakampally, D.; Mannava, Y. Comparison of minimally invasive coronally advanced flap and modified coronally advanced flap for the management of multiple adjacent gingival recession defects: A split mouth randomized control trial. J. Esthet. Restor. Dent. 2018, 30, 509–515. [Google Scholar] [CrossRef]
- Anoixiadou, S.; Parashis, A.; Vouros, I. Minimally Invasive Non-Surgical Technique in the Treatment of Intrabony Defects-A Narrative Review. Dent. J. 2023, 11, 25. [Google Scholar] [CrossRef]
- Richardson, C.R.; Allen, E.P.; Chambrone, L.; Langer, B.; McGuire, M.K.; Zabalegui, I. Periodontal Soft Tissue Root Coverage Procedures: Practical Applications from the AAP Regeneration Workshop. Clin. Adv. Periodontics 2015, 5, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Barbato, L.; Selvaggi, F.; Kalemaj, Z.; Buti, J.; Bendinelli, E.; Marca, M.; Cairo, F. Clinical efficacy of minimally invasive surgical (MIS) and non-surgical (MINST) treatments of periodontal intra-bony defect: A systematic review and network meta-analysis of RCT’s. Clin. Oral Investig. 2020, 24, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Hu, B.; Zhang, Y.; Li, W.; Song, J. Minimally Invasive Surgery Combined with Regenerative Biomaterials in Treating Intra-Bony Defects: A Meta-Analysis. PLoS ONE 2016, 19, e0147001. [Google Scholar] [CrossRef]
- Di Gianfilippo, R.; Wang, I.C.; Steigmann, L.; Velasquez, D.; Wang, H.L.; Chan, H.L. Efficacy of microsurgery and comparison to macrosurgery for gingival recession treatment: A systematic review with meta-analysis. Clin. Oral Investig. 2021, 25, 4269–4280. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Çankaya, Z.T.; Ünsal, B.; Gürbüz, S.; Bakirarar, B.; Tamam, E. Efficiency of Concentrated Growth Factor in the Surgical Treatment of Multiple Adjacent Papillary Losses: A Randomized, Controlled, Examiner-Blinded Clinical Trial Using CAD/CAM. Int. J. Periodontics Restor. Dent. 2020, 40, e73–e83. [Google Scholar] [CrossRef]
- McGuire, M.K.; Scheyer, E.T. A randomized, double-blind, placebo-controlled study to determine the safety and efficacy of cultured and expanded autologous fibroblast injections for the treatment of interdental papillary insufficiency associated with the papilla priming procedure. J. Periodontol. 2007, 78, 4–17. [Google Scholar] [CrossRef]
- Karmakar, S.; Kamath, D.S.G.; Shetty, N.J.; Natarajan, S. Treatment of Multiple Adjacent Class I and Class II Gingival Recessions by Modified Microsurgical Tunnel Technique and Modified Coronally Advanced Flap Using Connective Tissue Graft: A Randomized Mono-center Clinical Trial. J. Int. Soc. Prev. Community Dent. 2022, 12, 38–48. [Google Scholar]
- Srivastava, R.; Mohan, R.; Saravana Balaji, M.D.; Vijay, V.K.; Srinivasan, S.; Navarasu, M. Randomized Controlled Trial on a Minimally Invasive Microsurgical Versus Conventional Procedure for the Management of Localized Gingival Recession in Esthetic Zone using Alloderm. J. Pharm. Bioallied Sci. 2021, 13, S476–S483. [Google Scholar] [PubMed]
- Azaripour, A.; Kissinger, M.; Farina, V.S.; Van Noorden, C.J.; Gerhold-Ay, A.; Willershausen, B. Root coverage with connective tissue graft associated with coronally advanced flap or tunnel technique: A randomized, double-blind, mono-centre clinical trial. J. Clin. Periodontol. 2016, 43, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Nizam, N.; Bengisu, O.; Sönmez, Ş. Micro and macrosurgical techniques in the coverage of gingival recession using connective tissue graft: 2 years follow-up. J. Esthet. Restor. Dent 2015, 27, 71–83. [Google Scholar] [CrossRef] [PubMed]
- Burkhardt, R.; Lang, N.P. Coverage of localized gingival recessions: Comparison of micro- and macrosurgical techniques. J. Clin. Periodontol. 2005, 32, 287–293. [Google Scholar] [CrossRef]
- Ucak, O.; Ozcan, M.; Seydaoglu, G.; Haytac, M.C. Microsurgical instruments in laterally moved, coronally advanced flap for Miller Class III isolated recession defects: A randomized controlled clinical trial. Int. J. Periodontics Restor. Dent. 2017, 37, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, A.; Pk, P.; Jhamb, K.; Chaurasia, V.R.; Masamatti, V.S.; Dk, S.; Dk, S.; Babaji, P. Clinical evaluation of papilla reconstruction using subepithelial connective tissue graft. J. Clin. Diagn. Res. 2014, 8, ZC77–ZC81. [Google Scholar] [PubMed]
- Brägger, U.; Lauchenauer, D.; Lang, N.P. Surgical lengthening of the clinical crown. J. Clin. Periodontol. 1992, 19, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Francetti, L.; Del Fabbro, M.; Calace, S.; Testori, T.; Weinstein, R.L. Microsurgical treatment of gingival recession: A controlled clinical study. Int. J. Periodontics Restor. Dent. 2005, 25, 181–188. [Google Scholar]
- Shanelec, D.A. Periodontal microsurgery. J. Esthet. Restor. Dent. 2003, 15, 402–407. [Google Scholar] [CrossRef]
- Cortellini, P.; Tonetti, M.S. Microsurgical approach to periodontal regeneration. Initial evaluation in a case cohort. J. Periodontol. 2001, 72, 559–569. [Google Scholar] [CrossRef]
- Zucchelli, G.; Mele, M.; Mazzotti, C.; Marzadori, M.; Montebugnoli, L.; De Sanctis, M. Coronally advanced flap with and without vertical releasing incisions for the treatment of multiple gingival recessions: A comparative controlled randomized clinical trial. J. Periodontol. 2009, 80, 1083–1094. [Google Scholar] [CrossRef]
- De Sanctis, M.; Zucchelli, G. Coronally advanced flap: A modified surgical approach for isolated recession-type defects: Three-year results. J. Clin. Periodontol. 2007, 34, 262–268. [Google Scholar] [CrossRef]
- Zucchelli, G.; Amore, C.; Sforza, N.M.; Montebugnoli, L.; De Sanctis, M. Bilaminar techniques for the treatment of recession-type defects. A comparative clinical study. J. Clin. Periodontol. 2003, 30, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Tavelli, L.; Barootchi, S. A Minimally Invasive Approach for the Treatment of Multiple Adjacent Gingival Recessions with a Volume-Stable Collagen Matrix: A Case Series. Int. J. Periodontics Restor. Dent. 2022, 42, 155–162. [Google Scholar] [CrossRef]
- Cortellini, P.; Cortellini, S.; Bonaccini, D.; Stalpers, G.; Mollo, A. Treatment of Teeth with Insufficient Clinical Crown. Part 1: One-Year Clinical Outcomes of a Minimally Invasive Crown-Lengthening Approach. Int. J. Periodontics Restor. Dent. 2021, 41, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Griffin, T.J.; Cheung, W.S.; Zavras, A.I.; Damoulis, P.D. Postoperative complications following gingival augmentation procedures. J. Periodontol. 2006, 77, 2070–2079. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, P.; Malet, J.; Borghetti, A. Decision-making in aesthetics: Root coverage revisited. Periodontology 2000 2001, 27, 97–120. [Google Scholar] [CrossRef]
- Ardila, C.M.; Vivares-Builes, A.M. Antibiotic Resistance in Patients with Peri-Implantitis: A Systematic Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 15609. [Google Scholar] [CrossRef]
- Ardila, C.M.; Bedoya-García, J.A.; González-Arroyave, D. Antimicrobial resistance in patients with endodontic infections: A systematic scoping review of observational studies. Aust. Endod. J. 2022. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Randomized clinical trials (containing experimental group versus control group). Clinical trials with at least 3 months of follow-up. Persons without systemic diseases. MIST to treat different soft tissue conditions. | Patients with any disorder that can disturb healing. Patients who underwent periodontal surgical therapy in the preceding 12 months. Smokers. Continued traumatic tooth brushing. Deficient plaque control procedures. Bruxism and/or parafunctional habits. Patients with orthodontic appliances. Duplicate publications. In vitro experimentations and investigations implemented on animals. |
| Authors, Place, Publication Date | Patients /Mean Age | Diagnosis/ Condition | Trial Design/ Experimental versus Control Group | Methods of Clinical Evaluation | Clinical Results | Methods of Aesthetic Evaluation and Postoperative Morbidity | Aesthetic Outcomes | Postoperative Morbidity | Limitations Presented by the Authors | Follow-Up Period |
|---|---|---|---|---|---|---|---|---|---|---|
| Çankaya et al., Turkey 2020 [27] | 40 32 years | Papillary losses in maxillary anterior teeth | Parallel experimental group: 20 patients with 60 multiple adjacent papillary losses receiving minimally invasive surgery with concentrated growth factor. Control group: 20 patients with 60 multiple adjacent papillary losses without surgery. | Plaque index, probing depth, bleeding on probing, measurement of the width of the keratinized gingiva, and papillary thickness were evaluated before surgery and at 3, 6, and 12 months after surgery. Changes in the interproximal papilla and papilla filling were evaluated at 3, 6, and 12 months after surgery. Digital impression images were taken and transferred to software. Three separate images were taken at each session at baseline and 3, 6, and 12 months. | The papillary area at 3, 6, and 12 months showed statistically significant differences from baseline values in the test group (p < 0.001) but not in the control group. | NR | NR | NR | MIST is not recommended in cases of insufficient keratinized gingival width, shallow vestibular depth, presence of a high frenulum. | 12 months |
| McGuirre & Scheyer, USA 2007 [28] | 20 Age NR | Interdental papillary recession defects | Crossover experimental and control groups: Each subject (20 patients) served as his/her own control by receiving test and placebo therapy (cell culture media). Two primary sites were designated and randomized to receive autologous fibroblast or placebo injections beginning 1 week following the papilla priming method; two additional injections were completed 7 to 14 days following the initial injections. | Percentage changes in papillary height of the primary treatment areas from baseline to the 4-month visit. Changes in the following parameters from baseline to the 4-month visit: distance from the tip of the papilla to the alveolar crest and from the base of the contact area to the alveolar crest, probing depth, interproximal width of papilla, and plaque index. Photographs were taken at a standard magnification. Radiographs and study impressions of sites were taken at baseline and 4 months. | The management zones presented a statistically significant mean percentage increase from baseline in papillary height (p = 0.0067) at 2 months. The difference between test and placebo sites in papillary height at 2 months approached statistical significance (p = 0.006), recommending that the test therapy was greater than placebo management. | Inflammation score, tissue texture and color, and patient and clinician perception of change in the Nordland Class Score. A visual analog scale was used by the examiner and subject to assess the defect change from baseline to 2, 3, and 4 months. Assessment of subject safety included an analysis of the incidence of adverse events. | The examiner and subject’s visual scale scores were statistically significantly different from baseline for both treatment groups and superior for the test sites over the placebo (p = 0.01). | The fact that there were no significant changes in inflammation nor tissue texture, and color following treatment indicated that the therapy was well tolerated and yielded no adverse effects. The treatment was pain-free for both groups. | Small sample size. Angulation for digital photographs was not standardized. Volumetric increase in papilla following treatment was not measured. | 4 months |
| Ribeiro et al., Brazil 2014 [3] | 28 28 years | Altered passive eruption | Split-mouth experimental and control groups: Contralateral quadrants received aesthetic crown lengthening using open-flap (28 sides, 105 teeth) or MIST techniques (28 sides, 105 teeth) for the treatment of excessive gingival display. | Plaque index, probing depth, bleeding on probing, gingival margin, clinical attachment level, and keratinized gingiva height were evaluated at baseline and 3, 6, and 12 months post-surgery. Bone level was noted before and after the surgical techniques. The gingival crevicular fluid levels of receptor activator of nuclear factor-kB ligand and osteoprotegerin were assessed at baseline and 3 months post-surgery. To assess the hard and soft tissues, soft-tissue cone beam computed tomography was performed at baseline. | Probing depths were reduced for both groups at all time points, compared with baseline (p < 0.05). There were no differences between groups for gingival margin reduction at any time point. | Patient perceptions regarding morbidity and aesthetic satisfaction were evaluated with a questionnaire and the responses were quantified with a visual analog scale. The questionnaire was obtained upon completion of the procedure (pain), at 7 days post-surgery (pain/discomfort, swelling, hematoma, aesthetic appearance), and at 6 months post-surgery (esthetic appearance). | Patients reported high satisfaction with the aesthetic appearance of both procedures. | Patients reported low morbidity for both procedures. | MIST is not recommended in cases of insufficient keratinized gingival width. The reduction of bone in the buccal-palatal direction in cases of thick bone is not possible using MIST. | 12 months |
| Wang et al., China 2017 [7] | 40 39 years | Lost mandibular first molar at least 3 months of post-extraction healing. | Parallel experimental group: 20 patients intervened with minimally invasive flapless method for single implant placement. Control group: 20 patients intervened with flapped implant surgery. | Cone beam computerized tomography was taken at the day of implant installation. Modified sulcus bleeding index and plaque index were evaluated at 1, 2, and 4 weeks post-surgery and 3, 6, 12, and 24 months post-crown delivery. Probing depth was assessed at 4 weeks post-implant insertion surgery, on the day of crown delivery and at 3, 6, 12, and 24 months following intervention. The width of keratinized mucosa was measured between the soft tissue margin and the mucogingival junction at the facial aspects of the abutment on the day of crown delivery and at 12- and 24-month follow-up. Periapical radiographs were completed on the day after implant insertion, crown delivery and at 3-, 12-, and 24-month recall. All images were scanned and transferred to a computer with an image analysis package. | At each appointment, no changes in probing depth and marginal bone loss were observed between groups (p < 0.05). | Wound healing index was evaluated at 1, 2, and 4 weeks post-surgery. At 2 weeks post-surgery, post-surgical pain was measured on a visual analog scale by questioning the patient to evaluate their pain after surgery. | NR | Patients in the MIST group described significantly less post-surgical pain (p< 0.01) and significantly lower wound healing index scores at 1-week follow-up. | Computer-guided template was not performed for patients. Large sample size and histological analysis are required to confirm the findings. | 24 months |
| Bittecourt et al., Brazil 2012 [10] | 24 34 years | Gingival recessions | Split-mouth experimental and control groups: 24 patients in which subepithelial connective tissue graft was performed with a microscope or without a microscope or any type of magnification in the treatment of gingival recessions. | Recession height, weight of keratinized tissue, recession width, probing depth, clinical attachment level, and thickness of the keratinized tissue were registered at baseline and 6 and 12 months post-surgery. | The mean proportions of root coverage for test and control groups after 12 months were 98.0% and 88.3%, correspondingly (p < 0.05). | Overall postoperative pain was also assessed using a horizontal visual analog scale. At 6 months, a questionnaire was given to each patient. The questionnaire recorded the results of the procedures relative to aesthetics, root sensitivity (before and after surgery), and the postoperative period. | In the test group, all patients were pleased with the aesthetics achieved, and 19 patients (79.1%) were satisfied in the control group. | For postoperative morbidity, 14 patients in each of the two therapy groups did not take analgesics for pain control. | A longer follow-up period is necessary to verify the stability of MIST. The randomization method and impossibility of masking patients to the use of the microscope. | 12 months |
| Rajendran et al., India 2018 [19] | 7 30–48 years | Gingival recessions | Split-mouth experimental and control groups: 7 patients were treated with a minimally invasive coronally advanced flap or with modified coronally advanced flap for the treatment of multiple adjacent gingival recessions. | Recession heigh, recession width, probing depth, clinical attachment level, width of keratinized tissue, and gingival tissue thickness were recorded at baseline and 6 months post-operation. | No disparities were presented among minimally invasive coronally advanced and modified coronally advanced flap places, in the change in gingival recession depth, gingival recession width, clinical attachment level, width of the keratinized tissue, mean, and complete root coverage after 6 months (p > 0.05). | For patient-reported outcomes, a questionnaire and visual analogue scale were used. The questionnaire consisted of 2 parts: the first part was regarding aesthetic concerns about the recession, and the second part was regarding the preferred method of treatment among the 2 techniques used in the study. Patient satisfaction with aesthetics was evaluated at 3- and 6-month follow-up visits. The postoperative morbidity was evaluated 1 week after surgery. | The patient-reported aesthetic result was statistically significant (p < 0.001) between the minimally invasive coronally advanced flap and the modified coronally advanced flap arms, with better results for the minimally invasive coronally advanced flap arm. | The patient-reported outcome of postoperative morbidity was statistically significant (p < 0.001) between the minimally invasive coronally advanced flap and the modified coronally advanced flap sides, with better results on the minimally invasive coronally advanced flap side. | Small sample size. Studying various classes of Miller recession defects was recommended. | 6 months |
| Karmakar et al., India 2022 [29] | 10 44 years | Gingival recessions | Parallel experimental group: 5 patients treated with modified microsurgical tunnel technique utilizing connective tissue graft in the coverage of multiple adjacent recessions. Control group: 5 patients treated with modified coronally advanced flap utilizing connective tissue graft in the coverage of multiple adjacent recessions. | Sulcular bleeding index, recession depth, probing depth, clinical attachment level, keratinized tissue width, and gingival biotype were recorded at baseline and 1, 3, and 6 months post-surgery. | Mean root coverage and complete root coverage for the experimental group were 92.01% and 80% (p = 0.703) and for the control group were 87.39% and 60% (p = 0.545). | At baseline and 1, 3, and 6 months post-surgery, patients were provided with a questionnaire to subjectively evaluate their dentinal hypersensitivity. Quantitative evaluation was performed using a visual analog scale. Patient morbidity was assessed by subjective evaluation from the patient regarding pain, bleeding, and swelling 7 days after the surgery. The aesthetic evaluation was performed using the Root Coverage Aesthetic Score by comparing the digital images taken at baseline and 6 months by the operator. | Both therapies described high aesthetic outcomes. | Patients in the control group presented more morbidity (p < 0.05). | A longer follow-up period is necessary. | 6 months |
| Srivastava et al., India 2021 [30] | 30 Age NR | Gingival recessions | Parallel experimental group: 15 patients with recession defects were managed with a coronally positioned flap and acellular dermal matrix utilizing microsurgery. Control group: 15 patients with recessions were managed with a coronally positioned flap and acellular dermal matrix applying a conventional method. | Height of gingival recession, probing depth, clinical attachment level, gingival thickness, and width of the attached gingiva were documented at baseline and 3 and 6 months. | The MIST technique exhibited a significant change in the ultrasonographic thickness of gingiva (p < 0.003). | At 10 days and 1 and 6 months post-operation, patient satisfaction was recorded on a scale of 1–10. The satisfaction criteria included intra-operative experience at 10th day (pain during surgery and discomfort experience related to the duration of procedure and handling by the operator), postoperative experience at 1 month (for pain, swelling and postoperative complications), hypersensitivity at 6 months, recession coverage at 6 months, and appearance (color and form) at 6 months. | The MIST technique confirmed an improved patient satisfaction result (p < 0.005). | Postoperative morbidity was better in the experimental group (p < 0.005). | NR | 6 months |
| Azaripour et al., Germany 2016 [31] | 40 39 years | Gingival recessions | Parallel experimental group: 20 patients were treated with the coronally advanced flap and the modified microsurgical tunnel technique for the management of recessions. Control group: 20 patients were treated with the coronally advanced flap for the management of recessions. | Clinical measurements and volumetric evaluation of the soft tissue and digital photographs were performed at baseline and 1, 3, 6, and 12 months after surgery. The following clinical measurements were performed: probing depth, recession of the gingival margin, and width of keratinized tissue. The evaluation based on the Root Coverage Aesthetic Score was performed by comparing the corresponding images that were taken at baseline and 6- and 12-month reevaluation appointments. | Root coverage was 98.3% for the coronally advanced flap and 97.2% for the modified microsurgical tunnel technique (p > 0.05) | The aesthetic outcomes were evaluated using the Root Coverage Aesthetic Score. The evaluation compared 3 corresponding images of each experimental unit taken at baseline and 6 and 12 months. Immediately after surgery and again after 2 weeks, a questionnaire was given to the patients for subjective evaluation of the treatment in terms of pain, fear, morbidity, overall satisfaction, and root sensitivity. The parameters were evaluated quantitatively using a visual analogue scale. At the 1-year evaluation, patient satisfaction and their willingness to undergo further periodontal surgery were explored. | Both treatments described high aesthetic results (9.2 ± 1.3 for the coronally advanced flap and 9.2 ± 1.1 for the modified microsurgical tunnel technique; p > 0.05). | Both therapies showed certain post-surgical pain. On a measure from 0 to 10, the noticed pain was 2.2 ± 2.9 for the the coronally advanced flap test group and 2.8 ±2.9 for the modified microsurgical tunnel technique group (p > 0.05). | NR | 12 months |
| Nizam et al., Turkey 2015 [32] | 24 27 years | Gingival recessions | Split-mouth experimental and control groups: 21 teeth in microsurgical technique (experimental group) and 21 teeth in macrosurgical treatment (control group) were managed by implementing coronally positioned flap and subgingival connective tissue graft in the coverage of gingival recessions | Silicone impressions were made, and stone models of each defect were obtained. Photographs were also taken (preoperative procedure). Plaque index, gingival index, and probing depths were recorded. Recession depth, recession width, keratinized tissue width, and root surface area of the recessions were calculated. All clinical measurements except probing depth were made on standardized photographs. Clinical attachment level was also measured. These parameters were evaluated at baseline, 1, 3, 6, and 24th months. | Recession depth and recession surface area at 24 months were significantly lower in the microsurgical group (p < 0.05). | Postoperative pain of the intervention was evaluated using a visual analog scale during the first week. The patients also assessed the aesthetic result at baseline and 3, 6, and 24 months using a visual analog scale. | Aesthetic results improved likewise in both treatments. | The pain results in the donor and recipient zone diminished earlier in the microsurgical group (p < 0.05). | The calculation of root coverage percentage based on recession depth may result in overestimation of root coverage percentage and therefore could also be validated using root surface area values. | 24 months |
| Burkhardt & Lang, Switzerland 2005 [33] | 10 32–44 years | Gingival recessions | Split-mouth experimental and control groups: 10 patients with bilateral Class I and II recessions at maxillary canines were randomly selected for recession coverage either by a microsurgical (experimental group) or macrosurgical (control group) technique. | Clinical examinations at the recession sites were carried out before the surgical procedures and then after 1, 3, 6, and 12 months post-operation. The following parameters were assessed: gingival and plaque index, probing depth, clinical attachment level, and gingival recession. The percentage of vascularization was analyzed on the standardized angiographic images in defined areas of the gingival surfaces (obtained immediately after surgical intervention and 3 and 7 days post-operation). | The clinical lengths showed a mean recession coverage of 99.4% for the experimental and 90.8% for the control sites after the first month of healing (p < 0.05). The proportion of root coverage in both test and control sites persisted unchanging through the first year at 98% and 90%, correspondingly. The vascularization of the grafts was significantly improved by the microsurgical method (p < 0.05). | Subjective point of view | Complete root coverage was the ideal treatment outcome from an aesthetic and subjective standpoint. After one month, 90% of the test sites and 40% of the control sites had total root coverage, respectively (p < 0.05). | The microsurgically operated sites had greater vascularization than the macrosurgically treated sites, based on the angiographic study carried out immediately after the surgical procedure (p = 0.02). The distinction revealed proof that a minimally invasive method might result in less tissue trauma. | NR | 12 months |
| Randomized Clinical Trial | Randomization | Double Blinding | Withdraw | Proper Randomization | Proper Double Blinding | Score |
|---|---|---|---|---|---|---|
| Çankaya et al., 2020 [27] | 1 | 0 | 1 | 1 | 0 | 3 |
| McGuirre & Scheyer, 2007 [28] | 1 | 1 | 1 | 1 | 1 | 5 |
| Ribeiro et al., 2014 [3] | 1 | 0 | 1 | 1 | 0 | 3 |
| Wang et al., 2017 [7] | 1 | 0 | 1 | 1 | 0 | 3 |
| Bittencourt et al., 2012 [10] | 1 | 0 | 1 | 1 | 0 | 3 |
| Rajendran et al., 2018 [19] | 1 | 1 | 1 | 1 | 1 | 5 |
| Karmakar et al., 2022 [29] | 1 | 1 | 1 | 1 | 0 | 4 |
| Srivastava et al., 2021 [30] | 1 | 0 | 1 | 0 | 0 | 2 |
| Azaripour et al., 2016 [31] | 1 | 0 | 1 | 1 | 0 | 3 |
| Nizam et al., 2015 [32] | 1 | 0 | 1 | 0 | 0 | 2 |
| Burkhardt & Lang, 2005 [33] | 1 | 0 | 1 | 0 | 0 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ardila, C.M.; González-Arroyave, D.; Vivares-Builes, A.M. A Systematic Review of Randomized Clinical Trials Evaluating the Efficacy of Minimally Invasive Surgery for Soft Tissue Management: Aesthetics, Postoperative Morbidity, and Clinical Results. Medicina 2023, 59, 924. https://doi.org/10.3390/medicina59050924
Ardila CM, González-Arroyave D, Vivares-Builes AM. A Systematic Review of Randomized Clinical Trials Evaluating the Efficacy of Minimally Invasive Surgery for Soft Tissue Management: Aesthetics, Postoperative Morbidity, and Clinical Results. Medicina. 2023; 59(5):924. https://doi.org/10.3390/medicina59050924
Chicago/Turabian StyleArdila, Carlos M., Daniel González-Arroyave, and Annie Marcela Vivares-Builes. 2023. "A Systematic Review of Randomized Clinical Trials Evaluating the Efficacy of Minimally Invasive Surgery for Soft Tissue Management: Aesthetics, Postoperative Morbidity, and Clinical Results" Medicina 59, no. 5: 924. https://doi.org/10.3390/medicina59050924