
Psychoanalysis of COVID-19 Patient Narratives: A Descriptive Study

Abstract
:1. Introduction
2. Lacanian Desire Theory
2.1. Desire as the Other’s Desire
2.2. Desire for the Other’s Desired Object
2.3. Desire as the Object of the Other’s Desire
3. Material and Methods
3.1. Research Design
3.2. Participants
3.3. Procedure of Interviews
3.4. Data Analysis
“I felt that I was in darkness when I saw the COVID-19 pandemic. I don’t know how to say it. I think that our society and national policy are good. The virus is horrible”(Patient 12, darkness and light metaphor)
“I felt my mind was blank. I could hear nothing whatever they said. …I was in panic when I could hear”.(Patient 4, emotional narratives of Fear)
“I felt that I liked to take medicines. I thought I could get recovery only if I kept taking medicines. The only thing I liked was to take medicines. So I tried my best to get medicines. I must take medicines. If the doctor did not give me medicines, I worried that there was no hope, but I thought there was a hope if he gave me medicines“(behavior narratives)
4. Results
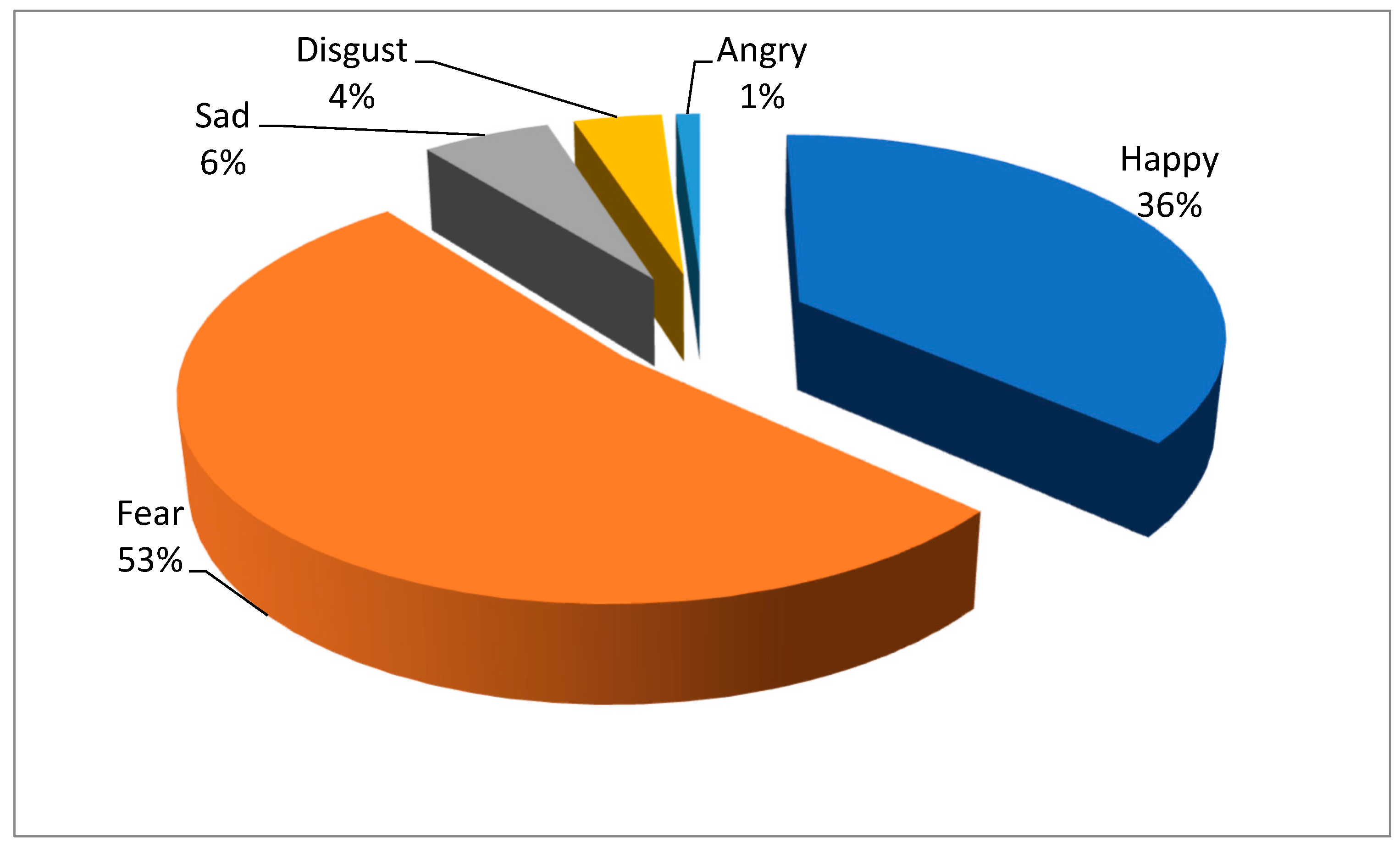
4.1. Quantitative Distribution of Patient Narratives
4.2. Qualitative Description of Patient Narratives
4.2.1. The Relationship between Lived-Experience Narratives and the Desire
“…during quarantine, the most thing I thought about was that I was serving a life sentence in prison. I had no idea when I could return home. Then, I got despaired. Everything in my mind was all about something like this.”(Patient 7, image metaphor and trials, law metaphor)
“Later, I told him about that. During the next day, the door wasn’t locked on. I felt different when the door wasn’t locked. I didn’t know. If the door was locked, I felt like I was in jail. Just felt like a jail. If the door was only closed but not locked, I felt…Er…My mood would be a little different. They locked the door, and that really made me scared, because you didn’t know how long you would be isolated”(Patient 10, image metaphor)
“When we were diagnosed with COVID-19, other people looked at us strangely…then they kept a long distance away us when we went for a COVID-19 test. They poked their head through the wall to check whether we were following up or not. …But I thought… I felt like a… a real… I noticed that, I mean, they were afraid of something like the plague. And I was the plague. The first time I had a feeling of being…the plague”(Patient 20, image metaphor)
“We are victims rather than prisoners. Some people looked at me strangely. Because I am a forthright man, I said that we are not criminals. We are the victims of the pandemic”(Patient 24, image metaphor)
“Because of my physical constitution, all I wanted was to sleep. I did not remember something which made me unhappy. If you say that, I was worried about my family. I contacted with my children at home. I was very, very, very worried about this, and I felt scary during the 14 days. So, I constantly asked about their physical states every day since I feared that others would be infected by me.”(Patient 2, specific behaviors, FEAR)
“…sometimes I could not fall asleep. If I failed to fall asleep, or I could not sleep at home, I feared that my brain would shut down when I was thinking too much. Then I always got up and ran around at home in the middle night, I wanted to end myself at that time. But I definitely could not do that because I have a child.”(Patient 7, obsessive behaviors, FEAR)
“I could not sleep when I was waiting for the result of my COVID-19 test. I just wanted to get the report as soon as possible. I was so worried that I could not fall asleep. I worried about my family and my children, and myself. I think that maybe I was lucky and not infected at that time. It was just anxiety. Very anxious. I was anxious, and anxiety made me suffer from insomnia. Later, two hours later, I called them, asking about my result. Then I kept asking the same question for every two hours”(Patient 8, obsessive behaviors, FEAR)
“I never thought that my result was negative. Then the doctor told me it was negative. (laughing) I was tested negative. So I asked the doctor when I could leave the hospital. He told me how I could ask this question since I received treatment in the hospital for just a few days. He said that I must take COVID-19 test twice or more if I wanted to leave hospital. Then I fell on the bed and told them to exam. 24 h later I took the COVID-19 test again. The result was negative again. Then I asked the doctor when I could leave the hospital. I said that I heard from others that I could leave hospital only with one negative result of COVID-19 test. But some people were in the hospital and some people said I needed to take the COVID-19 test twice. It was just…I must go out because I fear the COVID-19 test. Then I frequently asked the doctor: ‘Can I go out?’.”(Patient 13, specific behaviors, FEAR)
“…We feared of the risk of infecting others. It seemed that our body got ill due to the COVID-19 infection, which made us fear of contact with others. If we wouldn’t infect others, everything was fine. But if we made others infected, we would feel guilty about this. We dared not contact others outside, or we would greet our neighbors in a long distance. We were afraid of contacting people. No contact. We feared of transmitting”(Patient 26, specific behaviors, FEAR)
“Some psychologists called me when I was discharged from the hospital because I couldn’t fall asleep at that time. I felt that the virus was everywhere”(Patient 2, presence, accompanying, and absence)
“I felt that the virus was everywhere. That was my feeling at that time.”(Patient 6, presence, accompanying, and absence)
4.2.2. The Effects of External Factors on Patients’ Mental Health and their Responses for Desire
“They would complain. Some people complained. But they didn’t think that you were a bane of others, or you gave them troubles deliberately. However, they wouldn’t look at the thing with an objective perspective”(Patient 9, behavior of others)
“…we walked on the way. We took a walk at night. We walked on the same road…he came to us. Then he saw us when we were walking on the left side. Thump, this man rushed to the right side. Just like this. Then as he saw me, he covered his mouth immediately, and his nose. He ran away”(Patient 18, behavior of others)
“Those residents quarreled with us. One of them said that he would beat me to death if we walked in (the community). I was angry then. For those healthy people, they rejected us extremely.”(Patient 27, behavior of others)
“…of course, I was in a bad mood. Many local people bought houses in Yun Ji town. Although some people knew us, they dared not greet us. They just took us as strangers. No greetings. Just, scary.”(Patient 27, behavior of others)
“I quarreled with the disease control professionals. Their work is to take a blood sample. Why did I quarrel with them? Because it was not long that I left the hospital, and I lived in hotel for a day after de-isolation. But they brought me to have a COVID-19 test three days later. I said to them that I was not tested positive. What did you think? I said that I just felt better for discharging from hospital. I just felt better when I lived in hotel. You guys took a sample every six or seven days. Was it anything different about my sample? Why did you take the sample every day? This made me upset. Didn’t you have other things to do? You were wasting the government finance. Did you think that there was too much money? They said that they were unwilling to do this. I didn’t think so. I complained: “why did not you stand in my shoes to think about what I thought. I quarreled with them that day. But I had no choice, and COVID-19 test was necessary. So, I still supported their work”(Patient 16, specific behavior, ANGRY/FEAR)
“…I felt upset. I would not take phone calls or video call on wechat. My friends and family sent me messages: “we hear that you are retested positive.” “how does it happen?” Nobody had the patience to respond. In the hospital, I felt…I was a person who had a good attitude. But then, I…uh, I wanted to curse.”(Patient 18, specific behavior, SAD)
“I was crushed when I was isolated for the past ten days. I couldn’t sleep. I feared that I couldn’t sleep at night, too.”(Patient 7, metaphor of crumbling, breaking, and falling apart)
“When I started my isolation, I felt the atmosphere was something like that I had been isolated from the outside world.”(Patient 10, link metaphor)
“I had been told that I was cured when I went back home. But a few days later I was sent back to the hospital and my family was forced to isolate. I think that is a little nonsense. Of course, it proved that the virus was very cunning. And our health systems had not prepared for this yet”(Patient 14, animacy metaphor)
“I had to isolate in a long period where I was isolated from my families and friends even when I went back home. I could not bring people around me the danger of infection, because I was not sure when I would be retested positive.”(Patient 29, carrying metaphor)
“Nobody in my hometown in village didn’t know my infection yet. Because you know that villagers, villagers are so, they have many mouths. If you say that you are fine, those people will exaggerate the details. I just don’t want to make villagers know my thing.”(Patient 5, image metaphor)
“Many people discriminated against us. They kept off when they saw us. The gossip was really…unbelievable. I felt disgusted. But I could not live in others people’ eyes. Now we live in our own house other than theirs.”(Patient 16, image metaphor)
4.2.3. The Efforts of Self-Construction for the Sense of Broken
“I was so happy when I was discharged from hospital. I couldn’t breathe the air outside because I was isolated in the hospital. I could not go outside as both doors and windows were closed. When I was discharged from the hospital, I thought that the air was clean, and humans were free.”(Patient 7, image metaphor)
“Yes, I felt I was free from the jail. The air was clean. Words could hardly describe my happiness. I relaxed finally.”(Patient 22, image metaphor)
“Patients were not allowed to go out because each ward was locked. We had limited space of activity. …I think it was like a prison.”(Patient 3, image metaphor)
“That means some managers with power felt uncomfortable. I think at that time what should I do was to change their mind and to make them not identify me as a sensitive object but a normal person. And I supposed that was what I thought most. My trouble was to find the way of solution.”(Patient 1, image metaphor)
“The doctor was nervous when the result was positive. Then I was kept in a big room. No one answered me when I called them or asked them for treatment. They put the dinner at the door and ran away soon. I felt a sense of discrimination. I was discriminated, and I was locked in a room in which nobody took some measures to deal with it.”(Patient 14, behavior of others)
“The doctor told me how to do this, and I would follow his demands. I would follow his way for treatment. I won when the doctor pronounced his victory.”(Patient 28, fighting or battling)
“Our country is very strong. I’m touched so much because doctors and nurses took good care of me and treated my illness carefully. They did not take me as a patient in the hospital where I felt the warmness of home”(Patient 11, temperature, family)
“When I was transferred to another hospital, I…I didn’t know what happened. The transfer let me have no bottom in the heart. I was really afraid. I went there to be an experimental object, for real.”(Patient 10, container)
“Because I had never experienced such things, I had a feeling of fear. I feared of losing everything, and I feared of leaving the beautiful world.”(Patient 3, closeness and distance)
“You know that we left and came back for a long time. We were always shouting. Our hearts were shouting that we were not patients. We did not get ill. But we were diagnosed as patients because we matched the condition of COVID-19 test and diagnosis under the system and policies.”(Patient 30, animacy)
5. Discussion
Limitations and Future Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Interview Questions [23]
- 1.
- Could you please recollect how you were infected COVID-19? How did you feel when you were confirmed as a COVID-19 patient?
- 2.
- Could you please recollect the process of medical examination? How did you see or hear on the way to hospital and in the hospital? Could you narrate the whole process of seeing a doctor and nucleic acid testing (NAT)? How did you feel when you knew the results?
- 3.
- Could you please introduce the medical treatment in the hospital? What did you feel in the hospital? And what was the most impressive thing in the hospital?
- 4.
- What support did the doctors and nurses gave to you? Were there any impressive things that happened between you and these medical personnel?
- 5.
- What symptoms did you have since you got infected? Did you have any severe symptoms after infection? If you had, what did you feel when you knew your symptoms got severe?
- 6.
- What was the thing you thought about the most at that time? When you were infected and felt unhappy, what did you do to shift your attention out of these troubles?
- 7.
- Was someone nearby infected because of you?
- 8.
- Could you please narrate the scene of your discharge from hospital in detail?
- 9.
- Would you mention your infection to other people? How did you deal with the relationship between you and your family, relatives, friends, or neighbor? What did you think when people keep distance from you because your experiences? What support did your family give you when this happened to you?
- 10.
- Did you have dreams during the isolation?
- 11.
- Did you think about future when you knew that you were infected by COVID-19? What did you think about life and death? What was in your mind about death after your infection?
- 12.
- As to COVID-19, what kind of scene did you associate with? Why?
- 13.
- When you were recovered, did you ever think to help others in the way of sharing your experiences?
- 14.
- What was your opinion about the role of Chinese government for pandemic prevention and control? Could you please describe the image of nation in your mind?
- 15.
- How did you evaluate what doctors and nurses do during the epidemic? Why? And what was image of these medical personnel in your mind?
References
- Fawaz, M.; Samaha, A. The Psychosocial Effects of Being Quarantined Following Exposure to COVID-19: A Qualitative Study of Lebanese Health Care Workers. Int. J. Soc. Psychiatry 2020, 66, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Norful, A.A.; Rosenfeld, A.; Schroeder, K.; Travers, J.L.; Aliyu, S. Primary Drivers and Psychological Manifestations of Stress in Frontline Healthcare Workforce during the Initial COVID-19 Outbreak in the United States. Gen. Hosp. Psychiatry 2021, 69, 20–26. [Google Scholar] [CrossRef]
- Sarabia-Cobo, C.; Pérez, V.; Lorena, P.; Hermosilla-Grijalbo, C.; Alconero-amarero, A.R. Experiences of Geriatric Nurses in Nursing Home Settings Across Four Countries in the Face of the COVID-19 Pandemic. J. Adv. Nurs. 2021, 77, 869–878. [Google Scholar] [CrossRef]
- Wankowicz, P.; Szylinska, A.; Rotter, I. Assessment of Mental Health Factors among Health Professionals Depending on Their Contact with COVID-19 Patients. Int. J. Environ. Res. Public Health 2020, 17, 5849. [Google Scholar] [CrossRef]
- Yang, L.; Zhou, M.; Li, L.L.; Luo, P.; Fan, W.L.; Xu, J.J.; Chen, Q.; Pan, F.; Lei, P.; Zheng, C.S.; et al. Characteristics of Mental Health Implications and Plasma Metabolomics in Patients Recently Recovered from COVID-19. Transl. Psychiatry 2021, 11, 307. [Google Scholar] [CrossRef]
- Yue, L.; Wang, J.Y.; Ju, M.L.; Zhu, Y.; Chen, L.H.; Shi, L.; Shi, B.H.; Chen, J.; Shen, Y.F. How Psychiatrists Coordinate Treatment for COVID-19: A Retrospective Study and Experience from China. Gen. Psychiatry 2020, 33, 174–178. [Google Scholar] [CrossRef]
- Parikh, N.C.; Balchandani, A.D.; Nakum, D.H.; Patel, B.S.; Bhowmick, S.S.; Shah, N.D.; Darji, V.K. Study of Screening of Mental Health Status of Coronavirus Disease-19 Confirmed Noncritical Patients Admitted at a Tertiary Care Hospital and a Coronavirus Disease Care Center in Ahmedabad. Indian J. Psychiatry 2021, 63, 584–587. [Google Scholar] [CrossRef]
- Alamri, H.S.; Mousa, W.F.; Algarni, A.; Megahid, S.F.; Bshabshe, A.A.; Alshehri, N.N.; Bashah, D.M.; Alosaimi, R.; Alshehri, A.; Alsamghan, A.; et al. Mental Health of COVID-19 Patients—A Cross-Sectional Survey in Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 4758. [Google Scholar] [CrossRef]
- Kang, E.E.; Lee, S.Y.; Kim, M.S.; Jung, H.; Kim, K.H.; Kim, K.N.; Park, H.Y.; Lee, Y.J.; Cho, B.; Sohn, J.H. The Psychological Burden of COVID-19 Stigma: Evaluation of the Mental Health of Isolated Mild Condition COVID-19 Patients. J. Korean Med. Sci. 2021, 36, e33. [Google Scholar] [CrossRef]
- Gu, Y.Q.; Zhu, Y.; Xu, F.Z.; Xi, J.Z.; Xu, G.X. Factors Associated with Mental Health Outcomes among Patients with COVID-19 Treated in the Fangcang Shelter Hospital in China. Asia-Pac. Psychiatry 2021, 13, e12443. [Google Scholar] [CrossRef]
- Sahoo, S.; Mehra, A.; Suri, V.; Malhotra, P.; Yaddanapudi, L.N.; Puri, G.D.; Grover, S. Lived Experiences of the Corona Survivors (Patients Admitted in COVID Wards): A Narrative Real-life Documented Summaries of Internalized Guilt, Shame, Stigma, Anger. Asian J. Psychiatry 2020, 53, 102187. [Google Scholar] [CrossRef] [PubMed]
- Missel, M.; Bernild, C.; Christensen, S.W.; Dagyaran, I.; Berg, S.K. It’s Not Just a Virus! Lived Experiences of People Diagnosed with COVID-19 Infection in Denmark. Qual. Health Res. 2021, 31, 822–834. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Wang, L.; Yang, J.; Xie, L.; Chen, Y. How COVID-19 Patient Narratives Concerning Reinfection Mirror Their Mental Health: A Case Series. Psychiatr. Danub. 2021, 33, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Yang, J. Psychological Status of Frontline Healthcare Professionals at the Outbreak of COVID-19 in Wuhan: A Narrative Case Series. Psychiatr Clin. Psychopharmacol. 2021, 31, 233–237. [Google Scholar] [CrossRef]
- Sahoo, S.; Mehra, A.; Suri, V.; Malhotra, P.; Grover, S. Handling Children in COVID Wards: A Narrative Experience and Suggestions for Providing Psychological Support. Asian J. Psychiatry 2020, 53, 102207. [Google Scholar] [CrossRef]
- Velykodna, M. Psychoanalysis during the COVID-19 Pandemic: Several Reflections on Countertransference. Psychodyn. Pract. 2021, 27, 10–28. [Google Scholar] [CrossRef]
- Haber, D. Reflections in the Fog: Transferential Challenges and COVID-19. Psychoanal. Self Context 2021, 16, 253–263. [Google Scholar]
- Gairola, V. COVID-19 Turned Upside Down: A Psychological Perspective. Eur. Psychiatry 2021, 64, S677–S678. [Google Scholar] [CrossRef]
- Lacan, J.; Fink, B. Ecrits: The First Complete Edition in English; W.W. Norton & Company: New York, NY, USA, 1956–2006; p. 231. [Google Scholar]
- Lacan, J.; Tomaselli, S. The Seminar of Jacques Lacan Book II: The Ego in Freud’s Theory and in the Technique of Psychoanalysis; Translator; W.W. Norton & Company: New York, NY, USA, 1954–1955; pp. 223–224. [Google Scholar]
- Littlemore, J.; Turner, S. Metaphors in Communication about Pregnancy Loss. Metaphor. Soc. World 2020, 10, 45–75. [Google Scholar] [CrossRef]
- Deng, Y.; Yang, J.; Wan, W. Embodied Metaphor in Communication about Lived Experiences of the COVID-19 Pandemic in Wuhan, China. PLoS ONE 2021, 16, e0261968. [Google Scholar] [CrossRef]
- Deng, Y.; Yang, J.; Wang, L.; Chen, Y. The Road Less Traveled: How COVID-19 Patients Use Metaphors to Frame Their Lived Experiences. Int. J. Environ. Res. Public Health 2022, 19, 15979. [Google Scholar] [CrossRef]
- Deng, Y.; Park, M.; Chen, J.; Yang, J.; Xie, L.; Li, H.; Wang, L.; Chen, Y. Emotional Discourse Analysis of COVID-19 Patients and Their Mental Health: A Text Mining Study. PLoS ONE 2022, 17, e0274247. [Google Scholar] [CrossRef]
- Deng, Y.; Li, H.; Park, M. Emotional Experiences of COVID-19 Patients in China: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 9491. [Google Scholar] [CrossRef]
- Wallerstein, R. Metaphor in Psychoanalysis and Clinical Data. In Metaphor and Fields: Common Ground, Common Language, and the Future of Psychoanalysis, 1st ed.; Katz, S.M., Ed.; Routledge: New York, NY, USA, 2012. [Google Scholar]
- Peirce, C.S. Essential Peirce; Indiana University Press: Bloomington, IN, USA, 1998; p. 478. [Google Scholar]
- Gerald, M. I Wish That You Could Stay a Little Longer: Seeing the Image in Psychoanalysis. Psychoanal. Inq. 2016, 36, 644–652. [Google Scholar] [CrossRef]
- Saltzman, L.Y.; Lesen, A.E.; Henry, V.; Hansel, T.C.; Bordnick, P.S. COVID-19 Mental Health Disparities. Health Secur. 2021, 19, S5–S13. [Google Scholar] [CrossRef]
- Gasparyan, D. Mirror for the Other: Problem of the Self in Continental Philosophy (from Hegel to Lacan). Integr. Psychol. Behav. Sci. 2014, 48, 1–17. [Google Scholar] [CrossRef]
- Brown, T. Desire and Drive in Researcher Subjectivity—The Broken Mirror of Lacan. Qual. Inq. 2008, 14, 402–423. [Google Scholar] [CrossRef]
- Drummond, J.J. Self-Identity and Personal Identity. Phenomenol. Cogn. Sci. 2021, 20, 235–247. [Google Scholar] [CrossRef]
- Mo, G.H.; Wang, Z.X.; Chen, X.S.; Jiang, Q. The Prognosis and Prevention Measures for Mental Health in COVID-19 Patients: Through the Experience of SARS. Biopsychosoc. Med. 2020, 14, 22. [Google Scholar] [CrossRef]
- Guo, L.; Lin, J.; Ying, W.; Zheng, C.; Hu, B. Correlation Study of Short-Term Mental Health in Patients Discharged after Coronavirus Disease 2019 (COVID-19) Infection without Comorbidities: A Prospective Study. Neuropsychiatr. Dis. Treat. 2020, 16, 2661–2667. [Google Scholar] [CrossRef]
- Epstein, D.; Andrawis, W.; Lipsky, A.M.; Ziad, H.A.; Matan, M. Anxiety and Suicidality in a Hospitalized Patient with COVID-19 Infection. Eur. J. Case Rep. Intern. Med. 2020, 7, 001651. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Cao, L.; Li, X.; Jia, Y.; Xia, H. Awareness of Mental Health Problems in Patients with Coronavirus Disease 19 (COVID-19): A Lesson from an Adult Man Attempting Suicide. Asian J. Psychiatry 2020, 51, 102106. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Zhou, J.; Zong, C. Two Cases Report of Epidemic Stress Disorder to Novel Coronavirus Pneumonia. Asian J. Psychiatry 2020, 51, 102070. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Wang, S. The Cognitive Power of Deliberate Metaphors in the Reports of COVID-19 Outbreak. J. Tianjin Foreign Stud. Univ. 2020, 27, 114–127+161. [Google Scholar]
- Gok, A.; Kara, A. Individuals’ Conceptions of COVID-19 Pandemic through Metaphor Analysis. Curr. Psychol. 2021, 41, 449–458. [Google Scholar] [CrossRef]
- Menon, V.; Padhy, S.K. Mental Health among COVID-19 Survivors: Are We Overlooking the Biological Links? Asian J. Psychiatry 2020, 53, 102217. [Google Scholar] [CrossRef]
- Bryon, D. Processing Trauma in Psychoanalysis in ‘Real’ Time and in Dreams: The Convergence of Past, Present and Future during COVID-19. J. Anal. Psychol. 2021, 66, 399–410. [Google Scholar] [CrossRef]
- Hurley, J. Perceptual Shifts of Priority: A Qualitative Study Bringing Emotional Intelligence to the Foreground for Nurses in Talk-based Therapy Roles. J. Psychiatr. Ment. Health Nurs. 2013, 20, 97–104. [Google Scholar] [CrossRef]
- Browne, G.; Hurley, J. Mental Health Nurses as Therapists in a Rehabilitation Setting: A Phenomenological Study. Int. J. Ment. Health Nurs. 2018, 27, 1109–1117. [Google Scholar] [CrossRef]
- Maybery, D.; Jaffe, I.C.; Cuff, R.; Duncan, Z.; Grant, A.; Kennelly, M.; Ruud, T.; Skogoy, B.E.; Weimand, B.; Reupert, A. Mental Health Service Engagement with Family and Carers: What Practices are Fundamental? BMC Health Serv. Res. 2021, 21, 1073. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number (%) |
|---|---|
| Gender | |
| Male | 20 (56%) |
| Age | |
| 20–30 | 10 (27.8%) |
| 31–40 | 12 (33.3%) |
| 41–50 | 8 (22.2%) |
| 51–60 | 6 (16.7%) |
| Occupation | |
| Individual business | 6 (16.7%) |
| Engineer | 5 (13.9%) |
| Factory Worker | 5 (13.9%) |
| Farmer | 4 (11.1%) |
| Unemployed | 4 (11.11%) |
| Waiter | 2 (5.5%) |
| College Student | 2 (5.5%) |
| Manager | 1 (2.7%) |
| Medical staff | 1 (2.7%) |
| E-commerce | 1 (2.7%) |
| Housewife | 1 (2.7%) |
| Retired | 1 (2.7%) |
| Designer | 1 (2.7%) |
| Finance staff | 1 (2.7%) |
| Teacher | 1 (2.7%) |
| Marital Status | |
| Married | 26 (72.2%) |
| Unmarried | 8 (22.2%) |
| Divorced | 2 (5.6%) |
| Mean Hospital Quarantine Time | 16 days |
| Category | Instances | Percentage | Category | Instances | Percentage |
|---|---|---|---|---|---|
| Image metaphor | 76 | 24.68% | Physical injury | 3 | 0.97% |
| Motion | 24 | 7.79% | Presence, accompanying and absence | 3 | 0.97% |
| Container | 16 | 5.19% | Journey | 3 | 0.97% |
| Family | 16 | 5.19% | Weight | 3 | 0.97% |
| Life and death | 15 | 4.87% | Depth | 2 | 0.65% |
| War | 14 | 4.55% | Liquid-based metaphors | 2 | 0.65% |
| Animacy | 11 | 3.57% | Different realities | 2 | 0.65% |
| Symbolic metaphorical enactment | 10 | 3.25% | Sense of touch | 2 | 0.65% |
| Integrative behavior | 10 | 3.25% | Size | 2 | 0.65% |
| Darkness and light | 9 | 2.92% | Spatialization | 2 | 0.65% |
| Pressure | 7 | 2.27% | Agency | 1 | 0.32% |
| Carrying | 7 | 2.27% | Balance | 1 | 0.32% |
| Color | 6 | 1.95% | Cleanliness, dirtiness | 1 | 0.32% |
| Violence and impact | 6 | 1.95% | Conduit metaphor | 1 | 0.32% |
| Animal | 6 | 1.95% | Divided self | 1 | 0.32% |
| Closeness and distance | 5 | 1.62% | Explosion | 1 | 0.32% |
| Different realities | 5 | 1.62% | Fighting or battling | 1 | 0.32% |
| Temperature | 5 | 1.62% | Finding and losing | 1 | 0.32% |
| Body-related metaphor | 4 | 1.30% | Going back and forth | 1 | 0.32% |
| Crumbling, breaking, falling apart | 4 | 1.30% | Inside and outside | 1 | 0.32% |
| Fairness, justice | 4 | 1.30% | Sense | 1 | 0.32% |
| Machine | 4 | 1.30% | Trials, law | 1 | 0.32% |
| Games, chance, sport | 3 | 0.97% | Pushing and pulling | 1 | 0.32% |
| Hiding | 3 | 0.97% | Seeing | 1 | 0.32% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deng, Y.; Xie, L.; Wang, L.; Chen, Y. Psychoanalysis of COVID-19 Patient Narratives: A Descriptive Study. Medicina 2023, 59, 712. https://doi.org/10.3390/medicina59040712
Deng Y, Xie L, Wang L, Chen Y. Psychoanalysis of COVID-19 Patient Narratives: A Descriptive Study. Medicina. 2023; 59(4):712. https://doi.org/10.3390/medicina59040712
Chicago/Turabian StyleDeng, Yu, Luxue Xie, Li Wang, and Yaokai Chen. 2023. "Psychoanalysis of COVID-19 Patient Narratives: A Descriptive Study" Medicina 59, no. 4: 712. https://doi.org/10.3390/medicina59040712