
The Predictive Value of Monocyte/High-Density Lipoprotein Ratio (MHR) and Positive Symptom Scores for Aggression in Patients with Schizophrenia

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Statistical Analysis
2.3. Ethics Statement
3. Results
3.1. Comparison of Demographical and Clinical Characteristics between Groups
3.2. Comparison of Hematological Parameters in the Two Groups
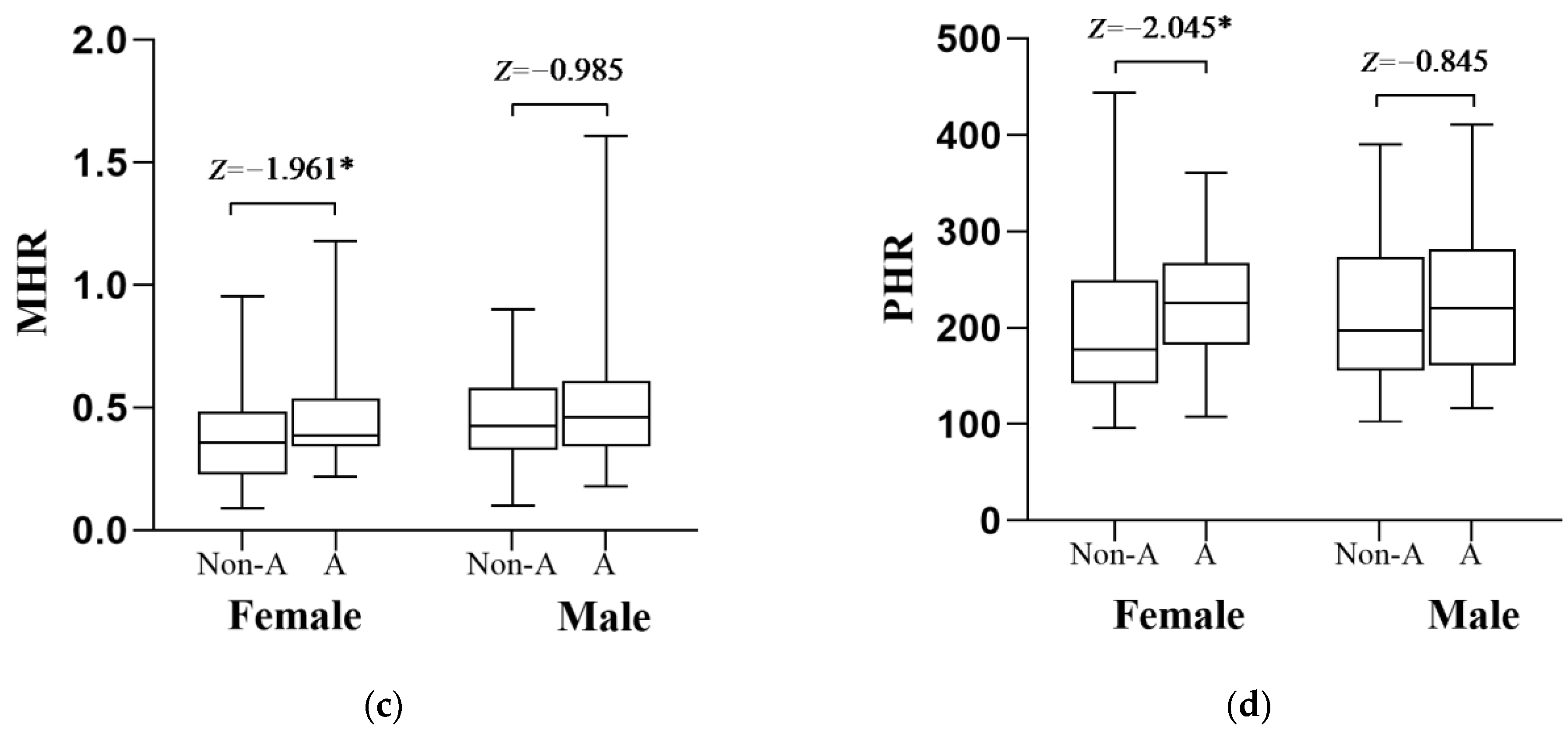
3.3. Serum Concentration, (a) PLT, (b) MON, (c) MHR and (d) PHR in Schizophrenia Patients by Sex, with and without Aggression
3.4. Correlations among the NHR, LHR, MHR, PHR and the MOAS in the Aggressive Group
3.5. The Related Factors for Aggression in Schizophrenia
4. Discussion
Study Limitations and Future Prospects
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pillinger, T.; D’Ambrosio, E.; McCutcheon, R.; Howes, O.D. Correction to: Is psychosis a multisystem disorder? A meta-review of central nervous system, immune, cardiometabolic, and endocrine alterations in first-episode psychosis and perspective on potential models. Mol. Psychiatry 2019, 24, 928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, Y.; Tanaka, A.; Kishi, T.; Li, Y.; Matsunaga, M.; Tanihara, S.; Iwata, N.; Ota, A. Recent findings on subjective well-being and physical, psychiatric, and social comorbidities in individuals with schizophrenia: A literature review. Neuropsychopharmacol. Rep. 2022, 42, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Kustner, B.; Martin, C.; Pastor, L. Prevalence of psychotic disorders and its association with methodological issues. A systematic review and meta-analyses. PLoS ONE 2018, 13, e0195687. [Google Scholar] [CrossRef] [Green Version]
- Battle, D.E. Diagnostic and Statistical Manual of Mental Disorders (DSM). Codas 2013, 25, 191–192. [Google Scholar]
- Jauhar, S.; Johnstone, M.; McKenna, P.J. Schizophrenia. Lancet 2022, 399, 473–486. [Google Scholar] [CrossRef]
- Swanson, J.W.; Swartz, M.S.; Van Dorn, R.A.; Elbogen, E.B.; Wagner, H.R.; Rosenheck, R.A.; Stroup, T.S.; McEvoy, J.P.; Lieberman, J.A. A national study of violent behavior in persons with schizophrenia. Arch. Gen. Psychiatry 2006, 63, 490–499. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.; Zhong, B.; Xiang, Y.; Chen, Q.; Cao, X.; Correll, C.; Ungvari, G.; Chiu, H.; Lai, K.; Wang, X. Prevalence of aggression in hospitalized patients with schizophrenia in China: A meta-analysis. Asia-Pac. Psychiatry Off. J. Pac. Rim Coll. Psychiatr. 2016, 8, 60–69. [Google Scholar] [CrossRef]
- Mohr, P.; Pecenák, J.; Svestka, J.; Swingler, D.; Treuer, T. Treatment of acute agitation in psychotic disorders. Neuro Endocrinol. Lett. 2005, 26, 327–335. [Google Scholar]
- Iozzino, L.; Ferrari, C.; Large, M.; Nielssen, O.; De Girolamo, G. Prevalence and Risk Factors of Violence by Psychiatric Acute Inpatients: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0128536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volavka, J. Violence in schizophrenia and bipolar disorder. Psychiatr. Danub. 2013, 25, 24–33. [Google Scholar]
- Hunter, M.; Carmel, H. The cost of staff injuries from inpatient violence. Hosp. Community Psychiatry 1992, 43, 586–588. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.; Siegel, A. Potentiating role of interleukin 2 (IL-2) receptors in the midbrain periaqueductal gray (PAG) upon defensive rage behavior in the cat: Role of neurokinin NK(1) receptors. Behav. Brain Res. 2006, 167, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Zalcman, S.S.; Siegel, A. The neurobiology of aggression and rage: Role of cytokines. Brain Behav. Immun. 2006, 20, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.; Zalcman, S.; Hassanain, M.; Siegel, A. Cytokine modulation of defensive rage behavior in the cat: Role of GABAA and interleukin-2 receptors in the medial hypothalamus. Neuroscience 2005, 133, 17–28. [Google Scholar] [CrossRef]
- Bhatt, S.; Bhatt, R.; Zalcman, S.S.; Siegel, A. Role of IL-1 beta and 5-HT2 receptors in midbrain periaqueductal gray (PAG) in potentiating defensive rage behavior in cat. Brain Behav. Immun. 2008, 22, 224–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahrén-Moonga, J.; Lekander, M.; Von Blixen, N.; Rönnelid, J.; Holmgren, S.; af Klinteberg, B. Levels of tumour necrosis factor-alpha and interleukin-6 in severely ill patients with eating disorders. Neuropsychobiology 2011, 63, 8–14. [Google Scholar] [CrossRef]
- Cushman, M.; Roux, A.D.; Ranjit, N.; Shea, S.; Ni, H.; Seeman, T. Socioeconomic Position, Race/Ethnicity, and Inflammation in the Multi-Ethnic Study of Atherosclerosis. Circulation 2008, 117, e344. [Google Scholar]
- Poletti, S.; Mazza, M.G.; Calesella, F.; Vai, B.; Lorenzi, C.; Manfredi, E.; Colombo, C.; Zanardi, R.; Benedetti, F. Circulating inflammatory markers impact cognitive functions in bipolar depression. J. Psychiatr. Res. 2021, 140, 110–116. [Google Scholar] [CrossRef]
- Fanning, J.R.; Lee, R.; Gozal, D.; Coussons-Read, M.; Coccaro, E.F. Childhood trauma and parental style: Relationship with markers of inflammation, oxidative stress, and aggression in healthy and personality disordered subjects. Biol. Psychol. 2015, 112, 56–65. [Google Scholar] [CrossRef]
- O’Brien, J.R.; Loi, E.C.; Byrne, M.L.; Zalewski, M.; Casement, M.D. The Link Between Positive and Negative Parenting Behaviors and Child Inflammation: A Systematic Review. Child Psychiatry Hum. Dev. 2021, 54, 51–65. [Google Scholar] [CrossRef]
- Jackson, A.J.; Miller, B.J. Meta-analysis of total and differential white blood cell counts in schizophrenia. Acta Psychiatr. Scand. 2020, 142, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Özdin, S.; Böke, Ö. Neutrophil/lymphocyte, platelet/lymphocyte and monocyte/lymphocyte ratios in different stages of schizophrenia. Psychiatry Res. 2019, 271, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Zhou, J.; Zhu, Y.; Yan, F.; Han, X.; Tan, Y.; Li, R. Neutrophil/lymphocyte, platelet/lymphocyte and monocyte/lymphocyte ratios in schizophrenia. Australas Psychiatry 2022, 30, 95–99. [Google Scholar] [CrossRef]
- Mercado, C.P.; Kilic, F. Molecular mechanisms of SERT in platelets: Regulation of plasma serotonin levels. Mol. Interv. 2010, 10, 231–241. [Google Scholar] [CrossRef]
- Thomas, M.R.; Storey, R.F. The role of platelets in inflammation. Thromb. Haemost. 2015, 114, 449–458. [Google Scholar] [PubMed]
- Tong, Z.; Zhu, J.; Wang, J.-J.; Yang, Y.-J.; Hu, W. The Neutrophil-Lymphocyte Ratio Is Positively Correlated with Aggression in Schizophrenia. Biomed Res. Int. 2022, 2022, 4040974. [Google Scholar] [CrossRef]
- Nazir, S.; Jankowski, V.; Bender, G.; Zewinger, S.; Rye, K.A.; van der Vorst, E.P. Interaction between high-density lipoproteins and inflammation: Function matters more than concentration! Adv. Drug Deliv. Rev. 2020, 159, 94–119. [Google Scholar] [CrossRef]
- Goossens, J.; Morrens, M.; Coppens, V. The Potential Use of Peripheral Blood Mononuclear Cells as Biomarkers for Treatment Response and Outcome Prediction in Psychiatry: A Systematic Review. Mol. Diagn. Ther. 2021, 25, 283–299. [Google Scholar] [CrossRef]
- Toledo, A.; Huang, Z.; Benach, J.L.; London, E. Analysis of Lipids and Lipid Rafts in Borrelia. Methods Mol. Biol. 2017, 1690, 69–82. [Google Scholar]
- Bukrinsky, M.I.; Mukhamedova, N.; Sviridov, D. Lipid rafts and pathogens: The art of deception and exploitation. J. Lipid Res. 2020, 61, 601–610. [Google Scholar] [CrossRef] [Green Version]
- Wei, L.; Xie, H.; Yan, P. Prognostic value of the systemic inflammation response index in human malignancy: A meta-analysis. Medicine 2020, 99, e23486. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Fan, Q.; Wu, S.; Wan, Y.; Lei, Y. Compared with the monocyte to high-density lipoprotein ratio (MHR) and the neutrophil to lymphocyte ratio (NLR), the neutrophil to high-density lipoprotein ratio (NHR) is more valuable for assessing the inflammatory process in Parkinson’s disease. Lipids Health Dis. 2021, 20, 35. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.-B.; Chen, Y.-S.; Ji, H.-Y.; Xie, W.-M.; Jiang, J.; Ran, L.-S.; Zhang, C.-T.; Quan, X.-Q. Neutrophil to high-density lipoprotein ratio has a superior prognostic value in elderly patients with acute myocardial infarction: A comparison study. Lipids Health Dis. 2020, 19, 59. [Google Scholar] [CrossRef] [Green Version]
- Kadihasanoglu, M.; Karabay, E.; Yucetas, U.; Erkan, E.; Ozbek, E. Relation between Monocyte to High-Density Lipoprotein Cholesterol Ratio and Presence and Severity of Erectile Dysfunction. Aktuelle Urol. 2018, 49, 256–261. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, M.; Xue, M.; Liu, D.; Sun, J. Elevated monocyte-to-HDL cholesterol ratio predicts post-stroke depression. Front. Psychiatry 2022, 13, 902022. [Google Scholar] [CrossRef]
- Uyar, B.; Budak, E.A. Effects of Major Depressive Disorder on Monocytes, High-Density Lipoprotein (HDL) and Monocyte to HDL Ratio: A Case-Control Study. Psychiatr. Danub. 2022, 34, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Sahpolat, M.; Ayar, D.; Ari, M.; Karaman, M.A. Elevated Monocyte to High-density Lipoprotein Ratios as an Inflammation Markers for Schizophrenia Patients. Clin. Psychopharmacol. Neurosci. 2021, 19, 112–116. [Google Scholar] [CrossRef]
- Wei, Y.; Wang, T.; Li, G.; Feng, J.; Deng, L.; Xu, H.; Yin, L.; Ma, J.; Chen, D.; Chen, J. Investigation of systemic immune-inflammation index, neutrophil/high-density lipoprotein ratio, lymphocyte/high-density lipoprotein ratio, and monocyte/high-density lipoprotein ratio as indicators of inflammation in patients with schizophrenia and bipolar disorder. Front. Psychiatry 2022, 13, 941728. [Google Scholar]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Knoedler, D.W. The Modified Overt Aggression Scale. Am. J. Psychiatry 1989, 146, 1081–1082. [Google Scholar]
- Rosales, C. Neutrophil: A Cell with Many Roles in Inflammation or Several Cell Types? Front. Physiol. 2018, 9, 113. [Google Scholar] [CrossRef]
- Melo, M.C.A.; Garcia, R.F.; de Araújo, C.F.C.; Abreu, R.L.C.; de Bruin, P.F.C.; de Bruin, V.M.S. Clinical significance of neutrophil-lymphocyte and platelet-lymphocyte ratios in bipolar patients: An 18-month prospective study. Psychiatry Res. 2019, 271, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.; Petzold, T.; Ishikawa-Ankerhold, H. Macrophage Regulation of Granulopoiesis and Neutrophil Functions. Antioxid. Redox Signal. 2021, 35, 182–191. [Google Scholar] [CrossRef]
- Mongirdienė, A.; Laukaitienė, J.; Skipskis, V.; Kuršvietienė, L.; Liobikas, J. The Difference of Cholesterol, Platelet and Cortisol Levels in Patients Diagnosed with Chronic Heart Failure with Reduced Ejection Fraction Groups According to Neutrophil Count. Medicina 2021, 57, 557. [Google Scholar] [CrossRef] [PubMed]
- Pillay, J.; Braber, I.D.; Vrisekoop, N.; Kwast, L.M.; de Boer, R.J.; Borghans, J.A.M.; Tesselaar, K.; Koenderman, L. In vivo labeling with 2H2O reveals a human neutrophil lifespan of 5.4 days. Blood 2010, 116, 625–627. [Google Scholar] [CrossRef] [Green Version]
- Huang, W.; Ren, F.; Luo, L.; Zhou, J.; Huang, D.; Pan, Z.; Tang, L. The characteristics of lymphocytes in patients positive for anti-MDA5 antibodies in interstitial lung disease. Rheumatology 2020, 59, 3886–3891. [Google Scholar] [CrossRef] [PubMed]
- Pfau, M.L.; Ménard, C.; Russo, S.J. Inflammatory Mediators in Mood Disorders: Therapeutic Opportunities. Annu. Rev. Pharmacol. Toxicol. 2018, 58, 411–428. [Google Scholar] [CrossRef]
- Yin, W.; Gallagher, N.R.; Sawicki, C.M.; McKim, D.B.; Godbout, J.P.; Sheridan, J.F. Repeated social defeat in female mice induces anxiety-like behavior associated with enhanced myelopoiesis and increased monocyte accumulation in the brain. Brain Behav. Immun. 2019, 78, 131–142. [Google Scholar] [CrossRef]
- Pogorzelska, K.; Krętowska, A.; Krawczuk-Rybak, M.; Sawicka-Żukowska, M. Characteristics of platelet indices and their prognostic significance in selected medical condition—A systematic review. Adv. Med. Sci. 2020, 65, 310–315. [Google Scholar] [CrossRef]
- Erjavec, G.N.; Tudor, L.; Perkovic, M.N.; Podobnik, J.; Curkovic, K.D.; Curkovic, M.; Strac, D.S.; Cusek, M.; Bortolato, M.; Pivac, N. Serotonin 5-HT(2A) receptor polymorphisms are associated with irritability and aggression in conduct disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2022, 117, 110542. [Google Scholar] [CrossRef]
- Yu, Q.; Weng, W.; Zhou, H.; Tang, Y.; Ding, S.; Huang, K.; Liu, Y. Elevated Platelet Parameter in First-Episode Schizophrenia Patients: A Cross-Sectional Study. J. Interf. Cytokine Res. 2020, 40, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Coccaro, E.F. Association of C-reactive protein elevation with trait aggression and hostility in personality disordered subjects: A pilot study. J. Psychiatr. Res. 2006, 40, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Graham, J.E.; Robles, T.F.; Kiecolt-Glaser, J.K.; Malarkey, W.B.; Bissell, M.G.; Glaser, R. Hostility and pain are related to inflammation in older adults. Brain Behav. Immun. 2006, 20, 389–400. [Google Scholar] [CrossRef] [PubMed]
- Coccaro, E.F.; Lee, R.; Coussons-Read, M. Elevated plasma inflammatory markers in individuals with intermittent explosive disorder and correlation with aggression in humans. JAMA Psychiatry 2014, 71, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Coccaro, E.F.; Lee, R. Cerebrospinal fluid 5-hydroxyindolacetic acid and homovanillic acid: Reciprocal relationships with impulsive aggression in human subjects. J. Neural Transm. 2010, 117, 241–248. [Google Scholar] [CrossRef]
- Carrillo, M.; Ricci, L.A.; Coppersmith, G.A.; Melloni, R.H. The effect of increased serotonergic neurotransmission on aggression: A critical meta-analytical review of preclinical studies. Psychopharmacology 2009, 205, 349–368. [Google Scholar] [CrossRef]
- Coccaro, E.F.; Lee, R.; Gozal, D. Elevated Plasma Oxidative Stress Markers in Individuals with Intermittent Explosive Disorder and Correlation With Aggression in Humans. Biol. Psychiatry 2016, 79, 127–135. [Google Scholar] [CrossRef]
- Tang, H.; Xiang, Z.; Li, L.; Shao, X.; Zhou, Q.; You, X.; Xiong, C.; Ning, J.; Chen, T.; Deng, D.; et al. Potential role of anti-inflammatory HDL subclasses in metabolic unhealth/obesity. Artif. Cells Nanomed. Biotechnol. 2021, 49, 565–575. [Google Scholar] [CrossRef]
- Soran, H.; Hama, S.; Yadav, R.; Durrington, P.N. HDL functionality. Curr. Opin. Lipidol. 2012, 23, 353–366. [Google Scholar] [CrossRef]
- Tomson-Johanson, K.; Harro, J. Low cholesterol, impulsivity and violence revisited. Curr. Opin. Endocrinol. Diabetes Obes. 2018, 25, 103–107. [Google Scholar] [CrossRef]
- Eriksen, B.M.S.; Bjørkly, S.; Lockertsen, Ø.; Færden, A.; Roaldset, J.O. Low cholesterol level as a risk marker of inpatient and post-discharge violence in acute psychiatry—A prospective study with a focus on gender differences. Psychiatry Res. 2017, 255, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aydın, F.Y.; Eynel, E.; Oruç, I.; Ince, H.; Yüksel, E.; Aydın, E. The Role of Monocyte to High-Density Lipoprotein Cholesterol Ratio in Predicting the Severity of Proteinuria and Renal Dysfunction in Primary Nephrotic Syndrome. Cureus 2021, 13, e20345. [Google Scholar]
- Kohsari, M.; Moradinazar, M.; Rahimi, Z.; Najafi, F.; Pasdar, Y.; Shakiba, E. New inflammatory biomarkers (lymphocyte and monocyte percentage to high-density lipoprotein cholesterol ratio and lymphocyte to monocyte percentage ratio) and their association with some cardiometabolic diseases: Results from a large Kurdish cohort study in Iran. Wien. Klin. Wochenschr. 2022, 134, 626–635. [Google Scholar]
- Jialal, I.; Jialal, G.; Ms, B.A. The platelet to high density lipoprotein -cholesterol ratio is a valid biomarker of nascent metabolic syndrome. Diabetes Metab. Res. Rev. 2021, 37, e3403. [Google Scholar] [CrossRef] [PubMed]
- Reichenberg, A.; Yirmiya, R.; Schuld, A.; Kraus, T.; Haack, M.; Morag, A.; Pollmächer, T. Cytokine-associated emotional and cognitive disturbances in humans. Arch. Gen. Psychiatry 2001, 58, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Pesce, M.; Speranza, L.; Franceschelli, S.; Ialenti, V.; Iezzi, I.; Patruno, A.; Rizzuto, A.; Robazza, C.; De Lutiis, M.A.; Felaco, M.; et al. Positive correlation between serum interleukin-1β and state anger in rugby athletes. Aggress. Behav. 2013, 39, 141–148. [Google Scholar] [CrossRef]
- Zhang, Q.; Hong, W.; Li, H.; Peng, F.; Wang, F.; Li, N.; Xiang, H.; Zhang, Z.; Su, Y.; Huang, Y.; et al. Increased ratio of high sensitivity C-reactive protein to interleukin-10 as a potential peripheral biomarker of schizophrenia and aggression. Int. J. Psychophysiol. 2017, 114, 9–15. [Google Scholar] [CrossRef]
- Quan, N.; Herkenham, M. Connecting cytokines and brain: A review of current issues. Histol. Histopathol. 2002, 17, 273–288. [Google Scholar] [PubMed]
- Das, S.; Deuri, S.K.; Sarmah, A.; Pathak, K.; Baruah, A.; Sengupta, S.; Mehta, S.; Avinash, P.R.; Kalita, K.N.; Hazarika, J. Aggression as an independent entity even in psychosis- the role of inflammatory cytokines. J. Neuroimmunol. 2016, 292, 45–51. [Google Scholar] [CrossRef]
- Pan, Y.-Z.; Xie, X.-M.; Tang, Y.-L.; Ng, C.H.; Wang, G.; Xiang, Y.-T. A comparison of aggression between patients with acute schizophrenia and mania presenting to psychiatric emergency services. J. Affect. Disord. 2022, 296, 493–497. [Google Scholar] [CrossRef]
- Araya, T.; Ebnemelek, E.; Getachew, R. Prevalence and Associated Factors of Aggressive Behavior among Patients with Schizophrenia at Ayder Comprehensive Specialized Hospital, Ethiopia. Biomed Res. Int. 2020, 2020, 7571939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shor, E.; Golriz, G. Gender, Race, and Aggression in Mainstream Pornography. Arch. Sex. Behav. 2018, 48, 739–751. [Google Scholar] [CrossRef] [PubMed]
- Zaborskis, A.; Ilionsky, G.; Tesler, R.; Heinz, A. The Association Between Cyberbullying, School Bullying, and Suicidality Among Adolescents. Crisis 2019, 40, 100–114. [Google Scholar] [CrossRef]
- Göttlich, M.; Buades-Rotger, M.; Wiechert, J.; Beyer, F.; Krämer, U.M. Structural covariance of amygdala subregions is associated with trait aggression and endogenous testosterone in healthy individuals. Neuropsychologia 2022, 165, 108113. [Google Scholar] [CrossRef]
- Guthman, E.M.; Falkner, A.L. Neural mechanisms of persistent aggression. Curr. Opin. Neurobiol. 2022, 73, 102526. [Google Scholar] [CrossRef]
- Kelly, A.M.; Abreu, J.A.G.; Thompson, R.R. Beyond sex and aggression: Testosterone rapidly matches behavioural responses to social context and tries to predict the future. Proc. Biol. Sci. 2022, 289, 20220453. [Google Scholar] [CrossRef]
- Dack, C.R.J.P.C.S.D.B.L.; Ross, J.; Papadopoulos, C.; Stewart, D.; Bowers, L. A review and meta-analysis of the patient factors associated with psychiatric in-patient aggression. Acta Psychiatr. Scand. 2013, 127, 255–268. [Google Scholar] [CrossRef]
- Krakowski, M.; Czobor, P.; Chou, J.C.-Y. Course of violence in patients with schizophrenia: Relationship to clinical symptoms. Schizophr. Bull. 1999, 25, 505–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weltens, I.; Bak, M.; Verhagen, S.; Vandenberk, E.; Domen, P.; van Amelsvoort, T.; Drukker, M. Aggression on the psychiatric ward: Prevalence and risk factors. A systematic review of the literature. PLoS ONE 2021, 16, e0258346. [Google Scholar] [CrossRef]
- Cho, W.; Shin, W.-S.; An, I.; Bang, M.; Cho, D.-Y.; Lee, S.-H. Biological Aspects of Aggression and Violence in Schizophrenia. Clin. Psychopharmacol. Neurosci. 2019, 17, 475–486. [Google Scholar] [CrossRef] [PubMed]
- Meyer, J.M.; Koro, C.E. The effects of antipsychotic therapy on serum lipids: A comprehensive review. Schizophr. Res. 2004, 70, 1–17. [Google Scholar] [CrossRef]
- Hermans, R.A.; Ringeling, L.T.; Liang, K.; Kloosterboer, S.M.; de Winter, B.C.M.; Hillegers, M.H.J.; Koch, B.C.P.; Dierckx, B. The effect of therapeutic drug monitoring of risperidone and aripiprazole on weight gain in children and adolescents: The SPACe 2: STAR (trial) protocol of an international multicentre randomised controlled trial. BMC Psychiatry 2022, 22, 814. [Google Scholar] [CrossRef]
- Buckley, P.F.; Kausch, O.; Gardner, G. Clozapine treatment of schizophrenia: Implications for forensic psychiatry. J. Clin. Forensic Med. 1995, 2, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Krakowski, M.I.; Czobor, P.; Citrome, L.; Bark, N.; Cooper, T.B. Atypical antipsychotic agents in the treatment of violent patients with schizophrenia and schizoaffective disorder. Arch. Gen. Psychiatry 2006, 63, 622–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Kang, R.; Yan, Y.; Gao, K.; Li, Z.; Jiang, J.; Chi, X.; Xia, L. Epidemiology of schizophrenia and risk factors of schizophrenia-associated aggression from 2011 to 2015. J. Int. Med. Res. 2018, 46, 4039–4049. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Parameters | All Patients (n = 214) | Non-Aggressive (n = 120) | Aggressive (n = 94) | p Value |
|---|---|---|---|---|
| Gender, n (%) | 0.028 | |||
| Female | 107 (50.00) | 68 (56.70) | 39 (41.20) | |
| Male | 107 (50.00) | 52 (43.30) | 55 (51.40) | |
| Marriage, n (%) | 0.433 | |||
| Unmarried | 96 (44.9) | 51 (42.50) | 45 (47.90) | |
| Married | 118 (55.10) | 69 (57.50) | 49 (52.10) | |
| Age (years), median (IQR) | 38.00 (18.00) | 39.50 (18.00) | 37 (17.00) | 0.32 |
| Family history of psychosis, n (%) | 0.584 | |||
| No | 167 (78.00) | 92 (76.70) | 75 (79.80) | |
| Yes | 47 (22.00) | 28 (23.30) | 19 (20.20) | |
| Education (years), median (IQR) | 9.00 (3.00) | 9.00 (3.00) | 9.00 (6.00) | 0.565 |
| BMI (kg/m2), median (IQR) | 23.88 (5.06) | 24.01 (5.34) | 23.62 (4.70) | 0.664 |
| Length of illness (years), median (IQR) | 12.00 (11.00) | 13.00 (10.00) | 11.00 (9.00) | 0.149 |
| PANSS score, median (IQR) | ||||
| Total score | 104.00 (29.25) | 102.00 (27.00) | 105.50 (32.00) | 0.116 |
| Positive symptom score | 28.00 (8.00) | 27.00 (7.00) | 29.00 (7.00) | 0.002 |
| Negative symptom score | 25.00 (14.00) | 25.00 (14.00) | 24.50 (14.00) | 0.878 |
| General psychopathology score | 50.50 (14.00) | 50.00 (12.00) | 52.50 (17.00) | 0.350 |
| Non-Aggressive (n = 120) | Aggressive (n = 94) | Mann–Whitney U | ||
|---|---|---|---|---|
| Z | p | |||
| HDL (mmol/L) | 1.180 (0.420) | 1.145 (0.320) | −0.236 | 0.813 |
| NEU (×109/L) | 3.795 (2.160) | 4.165 (2.520) | −1.328 | 0.184 |
| LYM (×109/L) | 1.815 (1.050) | 1.990 (0.730) | −1.071 | 0.284 |
| MON (×109/L) | 0.450 (0.220) | 0.535 (0.200) | −3.088 | 0.002 |
| PLT (×109/L) | 221.500 (80.000) | 255.500 (82.000) | −2.731 | 0.006 |
| NHR | 3.336 (2.242) | 3.458 (2.218) | −1.332 | 0.183 |
| LHR | 1.526 (1.255) | 1.636 (0.890) | −0.888 | 0.375 |
| MHR | 0.394 (0.239) | 0.419 (0.244) | −2.355 | 0.019 |
| PHR | 191.301 (118.245) | 221.388 (110.130) | −2.234 | 0.025 |
| Total Weighted Scores | Verbal Aggression | Aggression against Property | Auto-Aggression | Physical Aggression | |
|---|---|---|---|---|---|
| NHR | 0.289 ** | −0.026 | −0.001 | 0.319 ** | 0.199 |
| LHR | 0.213 * | −0.084 | −0.036 | 0.134 | 0.215 * |
| PHR | 0.115 | −0.147 | 0.012 | 0.227 * | 0.056 |
| MHR | 0.238 * | 0.014 | −0.055 | 0.163 | 0.230 * |
| Aggression (Yes/No) | |||||
|---|---|---|---|---|---|
| Independent Variable | β | SE | Waldχ2 | p | OR (95%CI) |
| MHR | 1.529 | 0.687 | 4.953 | 0.026 | 4.616 (1.200, 17.750) |
| Positive symptom scores | 0.071 | 0.026 | 7.236 | 0.007 | 1.074 (1.019, 1.131) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, N.; Ma, H.; Zhang, K.; Zhang, C.; Geng, D. The Predictive Value of Monocyte/High-Density Lipoprotein Ratio (MHR) and Positive Symptom Scores for Aggression in Patients with Schizophrenia. Medicina 2023, 59, 503. https://doi.org/10.3390/medicina59030503
Cheng N, Ma H, Zhang K, Zhang C, Geng D. The Predictive Value of Monocyte/High-Density Lipoprotein Ratio (MHR) and Positive Symptom Scores for Aggression in Patients with Schizophrenia. Medicina. 2023; 59(3):503. https://doi.org/10.3390/medicina59030503
Chicago/Turabian StyleCheng, Ning, Huan Ma, Ke Zhang, Caiyi Zhang, and Deqin Geng. 2023. "The Predictive Value of Monocyte/High-Density Lipoprotein Ratio (MHR) and Positive Symptom Scores for Aggression in Patients with Schizophrenia" Medicina 59, no. 3: 503. https://doi.org/10.3390/medicina59030503