
How Accurate Is the Diagnosis of “Chronic Obstructive Pulmonary Disease” in Patients Hospitalized with an Acute Exacerbation?
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Retrospective Data Collection
2.3. Follow Up Visit
2.4. Comparison of Patients Groups Based on Spirometry
2.5. Data Analysis
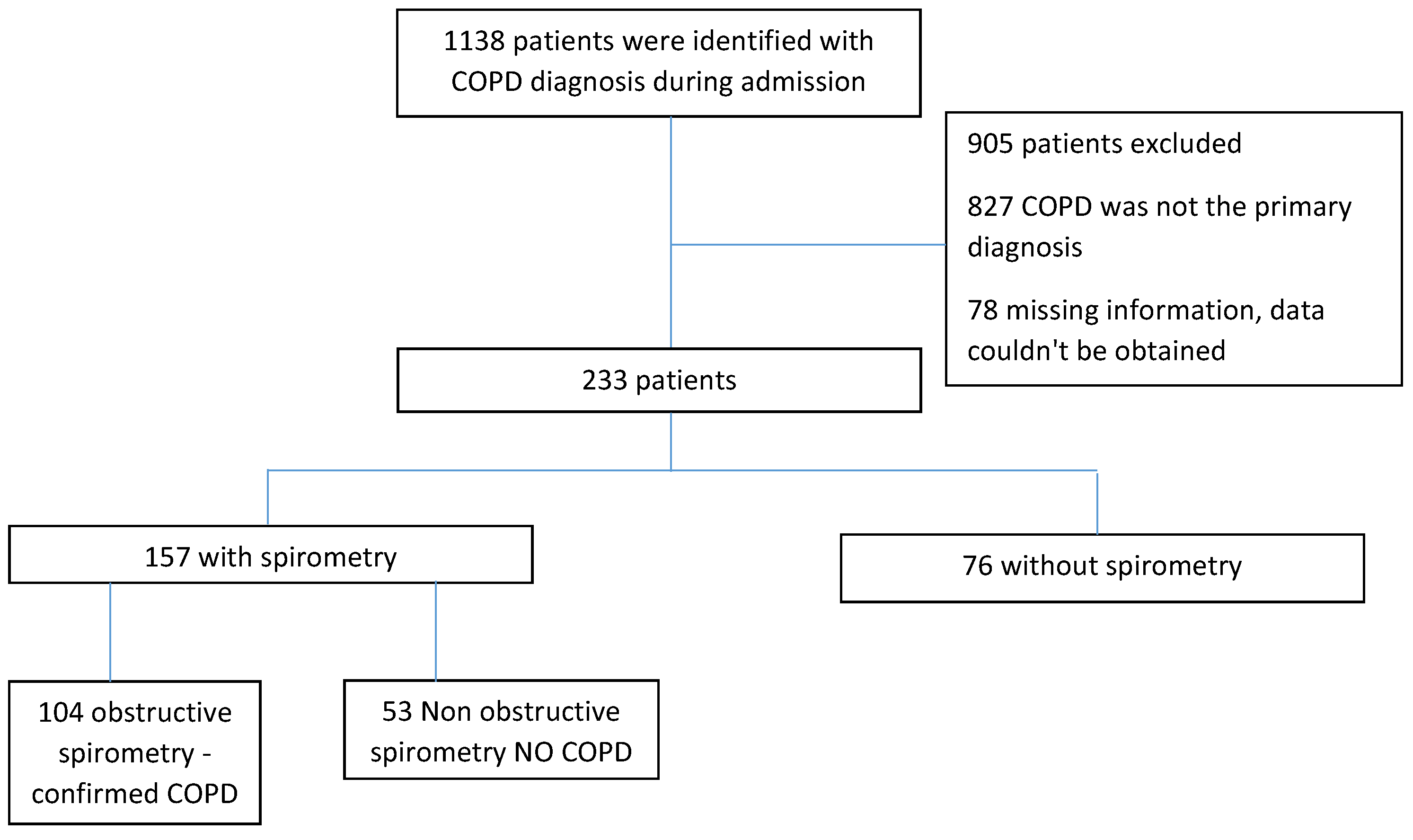
3. Results
3.1. Patients’ Characteristics
3.2. Differences between the Patient Groups
3.3. Admission Course
3.4. Laboratory Results
3.5. Factors Associated with Having a Confirmed COPD Diagnosis (Table 3)

{kind=link}
| OR | CI | p-Value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Age | 1.03 | 0.95 | 1.12 | 0.49 |
| Origin | 1.66 | 0.34 | 8.18 | 0.53 |
| Smoking | 0.93 | 0.17 | 5.06 | 0.93 |
| Past Smoker | 1.5 | 0.04 | 52 | 0.82 |
| Chronic Oxygen Therapy | 1.13 | 0.23 | 5.63 | 0.88 |
| CT before admission | 0.37 | 0.08 | 1.69 | 0.20 |
| Emphysema on CT before admission | 2.44 | 0.6 | 9.99 | 0.21 |
| Pulmonologist follow up before admission | 0.25 | 0.01 | 4.88 | 0.36 |
| Inhaler therapy | 1.81 | 0.23 | 14.18 | 0.57 |
| WBC | 1.02 | 0.97 | 1.07 | 0.52 |
| PCO2 | 1.05 | 0.99 | 1.11 | 0.08 |
| Pulmonologist consultation during admission | 4.78 | 0.55 | 41.47 | 0.16 |
| Pulmonologist consultation following admission | 14.59 | 2.41 | 88.22 | <0.001 |
| Recurrent admission due to COPD | 7.1 | 1.25 | 40.51 | 0.03 |
| Number of Hospitalization days | 1.05 | 0.99 | 1.13 | 0.13 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, C.; Xu, J.; Yang, L.; Xu, Y.; Zhang, X.; Bai, C.; Kang, J.; Ran, P.; Shen, H.; Wen, F.; et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): A national cross-sectional study. Lancet 2018, 391, 1706–1717. [Google Scholar] [CrossRef] [PubMed]
- Ntritsos, G.; Franek, J.; Belbasis, L.; A Christou, M.; Markozannes, G.; Altman, P.; Fogel, R.; Sayre, T.; E Ntzani, E.; Evangelou, E. Gender-specific estimates of COPD prevalence: A systematic review and meta-analysis. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 1507–1514. [Google Scholar] [CrossRef] [Green Version]
- Mathers, C.D.; Loncar, D. Projections of Global Mortality and Burden of Disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz-Guzman, E.; Mannino, D.M. Epidemiology and Prevalence of Chronic Obstructive Pulmonary Disease. Clin. Chest Med. 2014, 35, 7–16. [Google Scholar] [CrossRef] [PubMed]
- GOLD Report. Global Initiative for Chronic Obstructive Lung Disease 2020 Report. Global Initiative for Chronic Obstructive Lung Disease. 2020. Available online: https://goldcopd.org/wp-content/uploads/2019/12/GOLD-2020-FINAL-ver1.2-03Dec19_WMV.pdf (accessed on 26 January 2023).
- Press, D.; Kotsiou, O.S.; Deskata, K.; Gourgoulianis, K.I. Missed diagnosis and overtreatment of COPD among smoking primary care population in Central Greece: Old problems persist. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 487–498. [Google Scholar]
- Simon, P.M.; Schwartzstein, R.M.; Weiss, J.W.; Fencl, V.; Teghtsoonian, M.; Weinberger, S.E. Distinguishable Types of Dyspnea in Patients with Shortness of Breath. Am. Rev. Respir. Dis. 1990, 142, 1009–1014. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.; Partridge, M.R.; Miravitlles, M.; Cazzola, M.; Vogelmeier, C.; Leynaud, D.; Ostinelli, J. Symptom variability in patients with severe COPD: A pan-European cross-sectional study. Eur. Respir. J. 2011, 37, 264–272. [Google Scholar] [CrossRef] [Green Version]
- de los Monteros, M.J.E.; Pena, C.; Hurtado, E.J.S.; Jareno, J.; Miravitlles, M. Variability of respiratory symptoms in severe COPD. Arch. Bronconeumol. 2012, 48, 3–7. [Google Scholar] [CrossRef]
- Lopez, A.D.; Shibuya, K.; Rao, C.; Mathers, C.D.; Hansell, A.L.; Held, L.S.; Schmid, V.; Buist, S. Chronic obstructive pulmonary disease: Current burden and future projections. Eur. Respir. J. 2006, 27, 397–412. [Google Scholar] [CrossRef] [Green Version]
- Mannino, D.M.; Etzel, R.A.; Flanders, W.D. Do the Medical History and Physical Examination Predict Low Lung Function? Arch. Intern. Medi. 1993, 153, 1892–1897. [Google Scholar] [CrossRef]
- Holleman, D.R.; Simel, D.L. Does the Clinical Examination Predict Airflow Limitation? JAMA 1995, 273, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Spero, K.; Bayasi, G.; Beaudry, L.; Barber, K.R.; Khorfan, F. Overdiagnosis of COPD in hospitalized patients. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 2417–2423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghattas, C.; Dai, A.; Gemmel, D.J.; Awad, M.H. Over diagnosis of chronic obstructive pulmonary disease in an underserved patient population. Int. J. Chronic Obstr. Pulm. Dis. 2013, 8, 545–549. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Wise, R.A.; Medinger, A.E. Do Patients Hospitalized with COPD Have Airflow Obstruction? Chest 2017, 151, 1263–1271. [Google Scholar] [CrossRef]
- Yeatts, K.B.; Lippmann, S.J.; Waller, A.E.; Lich, K.H.; Travers, D.; Weinberger, M.; Donohue, J.F. Population-based burden of COPD-related visits in the ED: Return ED visits, hospital admissions, and comorbidity risks. Chest 2013, 144, 784–793. [Google Scholar] [CrossRef] [Green Version]
- Lash, T.L.; Johansen, M.B.; Christensen, S.; Baron, J.A.; Rothman, K.J.; Hansen, J.G.; Sørensen, H.T. Hospitalization Rates and Survival Associated with COPD: A Nationwide Danish Cohort Study. Lung 2010, 189, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Larrañaga, A.; Carney, L.; Soljak, M.; Bottle, A.; Partridge, M.; Bell, D.; Abi-Aad, G.; Aylin, P.; Majeed, A. Association of population and primary healthcare factors with hospital admission rates for chronic obstructive pulmonary disease in England: National cross-sectional study. Thorax 2011, 66, 191–196. [Google Scholar] [CrossRef] [Green Version]
- Nardini, S.; Annesi-Maesano, I.; Simoni, M.; del Ponte, A.; Sanguinetti, C.M.; De Benedetto, F. Accuracy of diagnosis of COPD and factors associated with misdiagnosis in primary care setting. E-DIAL (Early DIAgnosis of obstructive lung disease) study group. Respir. Med. 2018, 143, 61–66. [Google Scholar] [CrossRef] [PubMed]
- López-Campos, J.L.; Hartl, S.; Pozo-Rodriguez, F.; Roberts, C.M. European COPD Audit: Design, organisation of work and methodology. Eur. Respir. J. 2012, 41, 270–276. [Google Scholar] [CrossRef] [Green Version]
- Price, L.C.; Lowe, D.; Hosker, H.S.R.; Anstey, K.; Pearson, M.G.; Roberts, C.M. UK National COPD Audit 2003: Impact of hospital resources and organisation of care on patient outcome following admission for acute COPD exacerbation. Thorax 2006, 61, 837–842. [Google Scholar] [CrossRef] [Green Version]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.; Coates, A.; Van Der Grinten, C.P.M.; Gustafsson, P.; Hankinson, J.; et al. Interpretative strategies for lung function tests. Eur. Respir. J. 2005, 26, 948–968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef] [PubMed]
- Loh, C.H.; Genese, F.A.; Kannan, K.K.; Lovings, T.M.; Peters, S.P.; Ohar, J.A. Spirometry in Hospitalized Patients with Acute Exacerbation of COPD Accurately Predicts Post Discharge Airflow Obstruction. Chronic Obstr. Pulm. Dis. J. COPD Found. 2018, 5, 124–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Villar, A.; Represas-Represas, C.; Mouronte-Roibás, C.; Ramos-Hernández, C.; Priegue-Carrera, A.; Fernández-García, S.; López-Campos, J.L. Reliability and usefulness of spirometry performed during admission for COPD exacerbation. PLoS ONE 2018, 13, e0194983. [Google Scholar] [CrossRef] [PubMed]
- Daoud, N.; Soskolne, V.; Mindell, J.S.; Roth, M.A.; Manor, O. Ethnic inequalities in health between Arabs and Jews in Israel: The relative contribution of individual-level factors and the living environment. Int. J. Public Health 2018, 63, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Wan, E.S.; Fortis, S.; Regan, E.A.; Hokanson, J.; Han, M.K.; Casaburi, R.; Make, B.J.; Crapo, J.D.; DeMeo, D.L.; Silverman, E.K.; et al. Longitudinal Phenotypes and Mortality in Preserved Ratio Impaired Spirometry in the COPDGene Study. Am. J. Respir. Crit. Care Med. 2018, 198, 1397–1405. [Google Scholar] [CrossRef]
- Occhipinti, M.; Paoletti, M.; Bartholmai, B.J.; Rajagopalan, S.; Karwoski, R.A.; Nardi, C.; Inchingolo, R.; Larici, A.R.; Camiciottoli, G.; Lavorini, F.; et al. Spirometric assessment of emphysema presence and severity as measured by quantitative CT and CT-based radiomics in COPD. Respir. Res. 2019, 20, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowe, K.; Regan, E.A.; Anzueto, A.; Austin, E.; Austin, J.H.M.; Beaty, T.H.; Benos, P.V.; Benway, C.; Bhatt, S.P.; Bleecker, E.R.; et al. COPDGene® 2019: Redefining the Diagnosis of Chronic Obstructive Pulmonary Disease. Chronic Obstr. Pulm. Dis. J. COPD Found. 2019, 6, 384–399. [Google Scholar] [CrossRef] [Green Version]

| N (%) or Mean ± SD | |||||
|---|---|---|---|---|---|
| Total (N = 233) | Confirmed COPD (N = 104) | No COPD (N = 53) | Never had Spirometry (N = 76) | p-Value | |
| Sex | 0.58 | ||||
| Male | 167 (71.7) | 78 (75) | 36 (67.9) | 53 (69.7) | |
| Female | 66 (28.3) | 26 (25) | 17 (32.1) | 23 (30.3) | |
| Age (years) | 70 ± 11.9 | 71.5 ± 10.3 | 65.5 ± 11.9 | 71 ± 13.0 | <0.01 |
| Origin | <0.01 | ||||
| Arab | 78 (33.5) | 26 (25) | 15 (28.3) | 37 (48.7) | |
| Jew | 155 (66.5) | 78 (75) | 38 (71.7) | 39 (51.3) | |
| Past Medical History | |||||
| Hypertension | 129 (55.4) | 54 (51.9) | 30 (56.6) | 45 (59.2) | 0.91 |
| Heart Disease | 97 (41.6) | 39 (37.5) | 22 (41.5) | 36 (47.4) | 0.41 |
| Asthma | 22 (9.4) | 10 (9.6) | 6 (11.3) | 6 (7.9) | 0.94 |
| CKD # | 30 (12.9) | 15 (14.4) | 4 (7.5) | 11 (14.5) | 0.42 |
| Sleep Apnea | 19 (8.2) | 11 (10.6) | 4 (7.5) | 4 (5.3) | 0.43 |
| Smoking | <0.01 | ||||
| Current | 132 (56.7) | 52 (50) | 26 (49.1) | 54 (71) | |
| Never | 16 (6.9) | 4 (3.8) | 6 (11.3) | 6 (7.9) | |
| Past | 85 (36.5) | 48 (46.2) | 21 (39.6) | 16 (21.1) | |
| Emphysema (by CT) | 68 (29.2) | 44 (42.3) | 11 (20.8) | 13 (17.1) | 0.01 |
| Length of Stay (Days) | 4.3 ± 5.3 | 3 ± 3.0 | 4 ± 5.4 | 7.4 ± 7.4 | 0.04 |
| Diagnosis Made by | < 0.01 | ||||
| Unknown | 38 (16.3) | 4 (3.8) | 6 (11.4) | 28 (36.8) | |
| Pulmonologist | 126 (54.1) | 86 (82.7) | 31 (58.4) | 9 (11.9) | |
| Other * | 69 (29.6) | 14 (13.5) | 16 (30.2) | 39 (51.3) | |
| Recurrent Admission | 136 | 70 | 25 | 41 | 0.03 |
| (58.4) | (67.3) | (47.2) | (53.9) | ||
| Recurrent Admission due to COPD | 41 (17.6) | 29 (27.9) | 3 (5.6) | 9 (11.8) | <0.01 |
| FEV1 (L) | 2.2 ± 0.7 | 1.1 ± 0.4 | 1.8 ± 0.6 | - | <0.001 |
| FEV1, (% of predicted) | 48.6 ± 12.1 | 45.1 ± 16.9 | 49.3 ± 18.3 | - | 0.12 |
| FEV1 < LLN # | 79 (34) | 61 (58.6) | 22 (41.5) | - | <0.001 |
| FEV1 (Z-score) # | −2.85 (−3.7; −2.15) | −2.99 (−4.05; −2.6) | −2.15 (−2.85; −1.29) | - | <0.001 |
| FVC (L) | 2.2 ± 0.7 | 2.1 ± 0.7 | 2.4 ± 0.8 | - | <0.001 |
| FVC (% of predicted) | 69.6 ± 21.3 | 66.5 ± 19.9 | 75.1 ± 22.4 | - | <0.001 |
| FVC < LLN # | 61 (65.5%) | 42 (40.4) | 19 (35.9) | - | 0.36 |
| FVC (Z-score) # | −2.31 (−2.9; −1.36) | −2.34 (−2.8; −1.21) | −2.08 (−3; −2.08) | - | <0.001 |
| FEV1/FVC | 0.6 ± 0.1 | 0.5 ± 0.1 | 0.8 ± 0.1 | - | <0.001 |
| FEV1/FVC < LLN # | 49 (21) | 49 (47.1) | 0 (0) | - | <0.001 |
| FEV1/FVC (Z-score) # | −2 (−3.5; −0.58) | −2.72 (−4.05; −1.99 | −1.3 (−0.83; 0.47) | - | <0.001 |
| Inhaler Therapy | <0.01 | ||||
| None | 96 (41.2) | 16 (15.4) | 24 (45.3) | 56 (73.7) | |
| LABA | 3 (1.3) | 2 (1.9) | 1 (1.9) | 0 (0) | |
| LAMA | 9 (3.8) | 6 (5.8) | 2 (3.8) | 1 (1.3) | |
| ICS | 15 (6.4) | 7 (6.7) | 3 (5.6) | 5 (6.6) | |
| LABA/LAMA | 13 (5.5) | 13 (12.5) | 0 (0) | 0 (0) | |
| ICS/LABA | 42 (18.1) | 16 (15.4) | 13 (24.5) | 13 (17.1) | |
| ICS/LABA/LAMA | 55 (23.7) | 44 (42.3) | 10 (18.9) | 1 (1.3) | |
| N (%) or Mean ± SD | |||||
|---|---|---|---|---|---|
| Total (N = 233) | Confirmed COPD (N = 104) | No COPD (N = 53) | Never had Spirometry (N = 76) | p-Value | |
| Antibiotics | 183 | 88 | 39 | 56 | 0.13 |
| (78.5) | (84.6) | (73.6) | (73.7) | ||
| Bronchodilators (Short acting) | 208 | 94 | 47 | 67 | 0.89 |
| (89.3) | (90.4) | (88.7) | (88.2) | ||
| Systemic steroids | 186 | 86 | 42 | 58 | 0.57 |
| (79.8) | (82.7) | (79.2) | (76.3) | ||
| Heart failure therapy | 39 (16.7) | 16 (15.4) | 8 (15.1) | 15 (19.7) | 0.25 |
| Respiratory support | 45 (19.4) | 27 (26) | 6 (11.5) | 12 (15.8) | 0.06 |
| Pulmonologist consultation during admission | 42 | 26 | 9 | 7 | 0.02 |
| (18.0) | (25.0) | (17.0) | (9.2) | ||
| Pulmonologist consultation following admission | 118 | 81 | 29 | 8 | <0.01 |
| (50.6) | (77.9) | (54.7) | (10.5) | ||
| COPD diagnosis remained after admission | 229 | 104 | 51 | 74 | 0.17 |
| (98.3) | (100.0) | (96.2) | (97.4) | ||
| Laboratory results | |||||
| WBC | 11.4 ± 7 | 12.3 ± 5.6 | 10.6 ± 11 | 10.7 ± 4.6 | <0.01 |
| CRP | 6.1 ± 9 | 6.5 ± 9 | 4.8 ± 7.8 | 6.4 ± 10.3 | 0.75 |
| PCO2 | 49.7 ± 15.2 | 53 ± 16 | 44.5 ± 13.8 | 48.4 ± 14 | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Darawshy, F.; Abu Rmeileh, A.; Kuint, R.; Goychmann-Cohen, P.; Fridlender, Z.G.; Berkman, N. How Accurate Is the Diagnosis of “Chronic Obstructive Pulmonary Disease” in Patients Hospitalized with an Acute Exacerbation? Medicina 2023, 59, 632. https://doi.org/10.3390/medicina59030632
Darawshy F, Abu Rmeileh A, Kuint R, Goychmann-Cohen P, Fridlender ZG, Berkman N. How Accurate Is the Diagnosis of “Chronic Obstructive Pulmonary Disease” in Patients Hospitalized with an Acute Exacerbation? Medicina. 2023; 59(3):632. https://doi.org/10.3390/medicina59030632
Chicago/Turabian StyleDarawshy, Fares, Ayman Abu Rmeileh, Rottem Kuint, Polina Goychmann-Cohen, Zvi G. Fridlender, and Neville Berkman. 2023. "How Accurate Is the Diagnosis of “Chronic Obstructive Pulmonary Disease” in Patients Hospitalized with an Acute Exacerbation?" Medicina 59, no. 3: 632. https://doi.org/10.3390/medicina59030632