1. Introduction
Cardiac arrhythmia in pregnant women is a major therapeutic challenge. Due to a combination of hormonal, hemodynamic, and autonomic changes, an increased incidence of cardiac arrhythmias has been observed in pregnant women [
1]. Compared with other arrhythmias, supraventricular tachycardia (SVT) is the most common sustained arrhythmia with a reported incidence of 13 to 24 per 1000 pregnancies [
2]. In consideration of the potential risk of radiation exposure to the fetus, catheter ablation is an alternative strategy, whereas antiarrhythmic medicines, including beta-blockers, adenosine triphosphate, and non-dihydropyridine calcium antagonists, used to be the first-choice therapeutic option for pregnant patients with symptomatic SVT [
3]. In recent years, however, using real-time intracardiac echocardiographic imaging, three-dimensional (3D) electroanatomical mapping and contact force-sensing catheters, zero-fluoroscopy catheter ablation gradually is preferred in those patients [
4].
Focal atrial tachycardias (AT) comprise a distinct subset of SVT and are characterized by centrifugal spread of activation wave fronts from an atrial point source [
5]. Using high-density mapping, radiofrequency (RF) catheter ablation can now be effective for curing most focal AT with the three-dimensional mapping technique. However, focal ATs originating from the right atrial appendage (RAA), which constitute an estimated 3.8% of all focal ATs [
6,
7], may pose big challenges to RF ablation because the atrial appendage (AA) wall is extremely thin and vulnerable. RF ablation here is likely to result in cardiac perforation and a potentially fatal outcome for the mother and fetus. The extremely thin appendage wall can easily become deformed when touched by a catheter, which hinders an accurate location. Additionally, the unusual complex structure can increase the difficulty of catheter ablation.
Thus, it should be a priority to introduce an effective and safe strategy in this situation, especially with continuous and refractory arrhythmia. With limited effect on hemodynamics and tiny wounds, thoracoscopic ectomy of atrial appendage appears to be a prospective method, which only needs to make several apertures at the right third and sixth intercostal spaces for excising the lesion site.
We report a pregnant patient with severe focal atrial tachycardia. The patient successfully underwent thoracoscopic ectomy of the atrial appendage without fluoroscopy using a three-dimensional mapping system.
2. Case Presentation
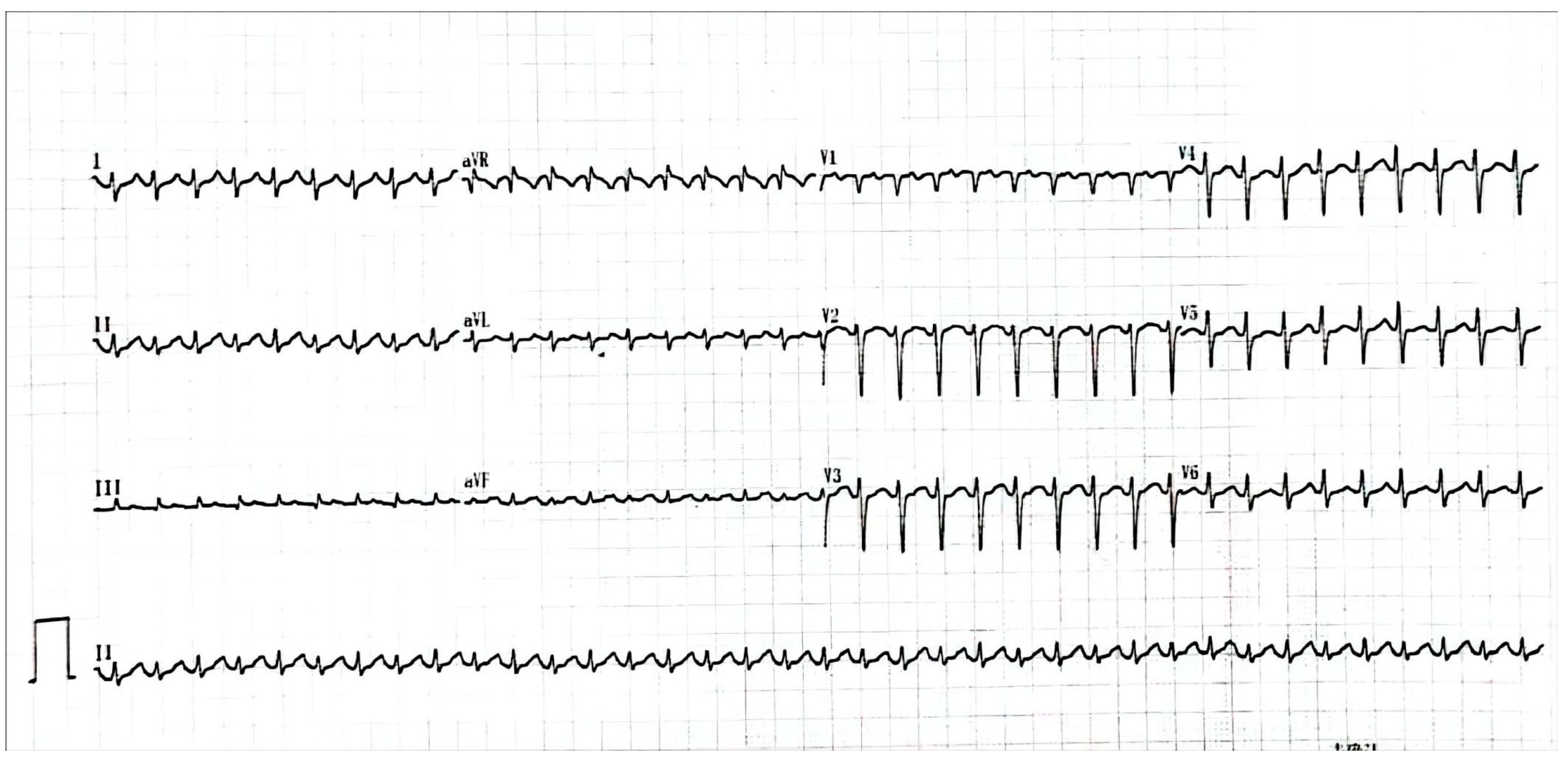
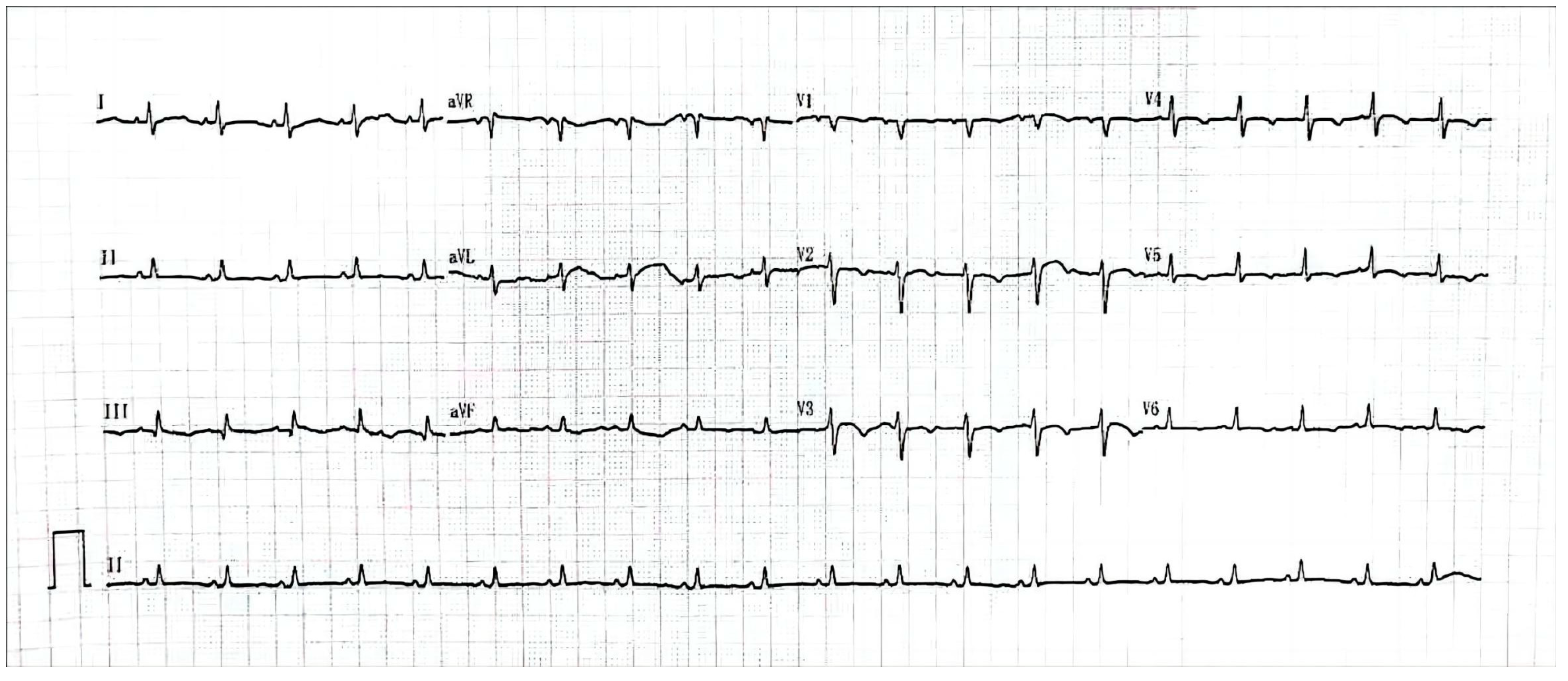
A 26-year-old pregnant woman with rapid and refractory tachycardia, at 21 weeks of gestation, was transferred for urgent management. She had arrhythmia episodes one year before pregnancy, and the arrhythmia became persistent and severe during pregnancy. This patient had a structurally normal heart. The 12-lead electrocardiogram revealed tachycardia of up to 220 beats per minute (
Figure 1).
2.1. Initial Medication
Adenosine triphosphate administration was given, and then transesophageal overdrive suppression was performed. The tachycardia continued without intermittence and the woman felt dizzy, a little dyspnea, and had mild hypotension.
An immediate and brief multidisciplinary consultation, which comprised electrophysiologists, a cardiac surgeon, an obstetrician, and a medical physicist, agreed that the rapid and persistent tachycardia would be fatal both to the fetus and the mother if it continued. Routinely, the risk of fluoroscopic radiation is often concerned with catheter ablation in pregnancy. It was recommended for the patient since we had carried nearly two thousands cases of zero-fluoroscopy ablation and the success rate of was over 99%.
The patient finally chose to take zero-fluoroscopy catheter ablation using the Carto 3TM system. The study was urgently approved by the Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, China. Written informed consent was acquired.
2.2. The First Mapping and Ablation
Antiarrhythmic medications had discontinued for at least five half-lives before the procedure in the primary hospital. Three patches attached to the sensor cables were placed on the back skin of the patient. The location pad was slid under the patient’s table, such that the three back patches were in the center of the location pad. Infiltrated with 1% lidocaine, the femoral vein was punctured. The ablation catheter (NaviStar® 4 mm TC, Biosense Webster Inc., Irvine, CA, USA) was placed via an eight-French sheath; a mapping catheter was placed in the coronary sinus (CS) via a six-French sheath. An electrophysiological study was performed using standard pacing protocols. The entire procedure was performed with zero-fluoroscopy.
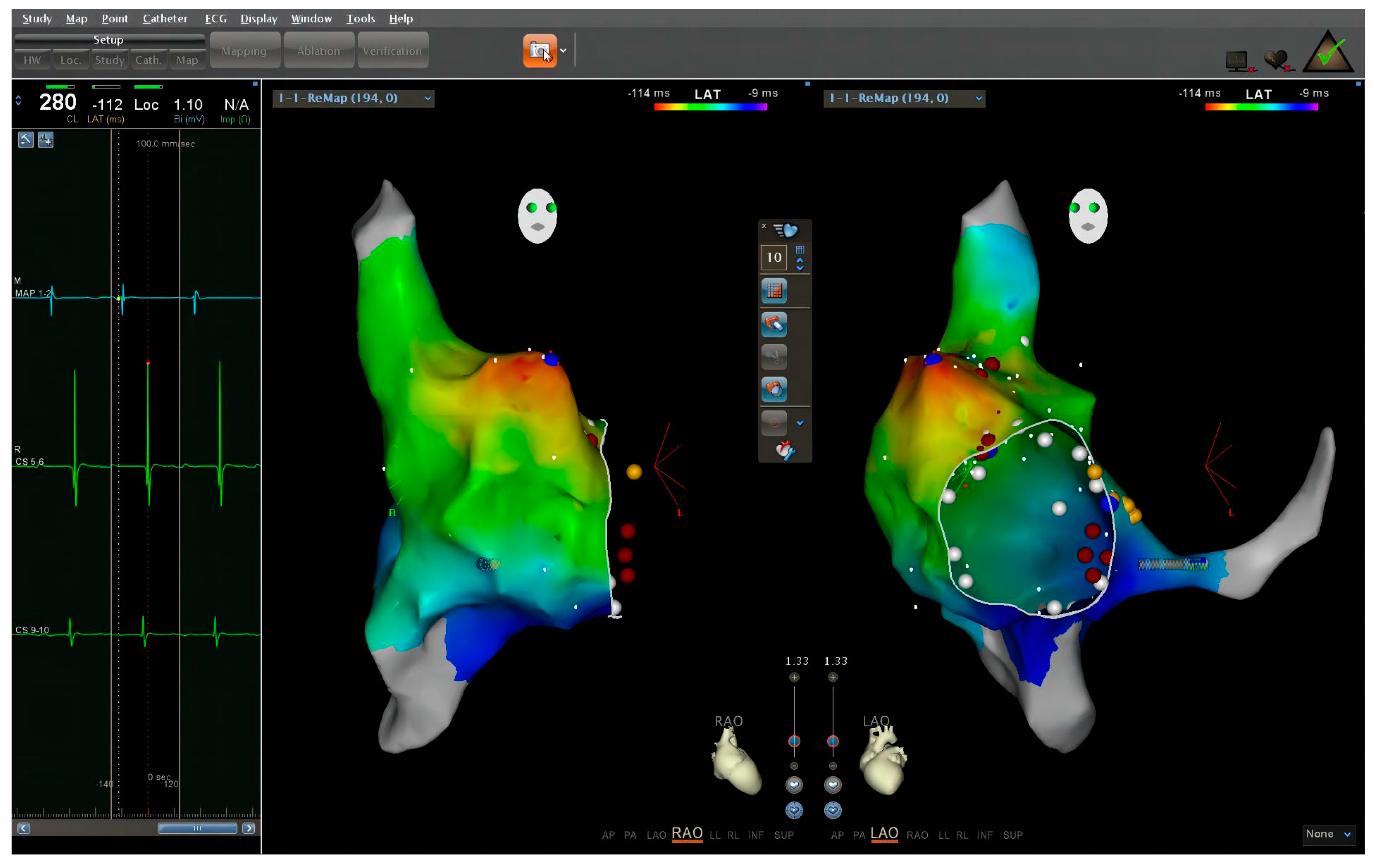
Intracardiac electrogram revealed an SVT at a cycle length of 260 milliseconds. Electrogram from CS electrode showed an activation pattern from proximal to distal. Adenosine triphosphate administration led to an atrium-ventricle conduction ratio of two or three to one. The virtual geometry of the right cardiac chamber was reconstructed by the ablation catheter. Further mapping with the ablation catheter revealed that the tachycardia originated from the apex of right atrial appendage (
Figure 2). Ablation with low power, ten to fifteen watts, was applied at the earliest site and had no effect. Higher power and longer ablation strategies were rejected by the expert group due to safety concerns for the pregnant woman and the fetus.
2.3. Burst Pacing and Medication
Repetitive burst pacing was applied at three hundred to four hundred beats per minute after the mapping. However, the tachycardia still could not only be terminated but also needed to be converted into atrial fibrillation, a status more applicable to medicine.
Other anti-arrhythmic drugs, including verapamil, propafenone, cedilanid, and esmolol, were administered with the aim of temporally terminating the tachycardia, but they all failed and the tachycardia became more rapid.
Electric cardioversion was not performed due to the automatic property of the tachycardia.
2.4. The Second Mapping and Thoracoscopic Ectomy
The patient was then sent to the Cardiac Care Unit. The tachycardia became more rapid, and her hemodynamics worsened. Hence, another urgent multidisciplinary consultation with the electrophysiologist, cardiac surgeon, obstetrician, and medical physicist was carried out. Plans for additional radiofrequency ablation for the atrial tachycardia were rejected by the expert group. Then, thoracoscopic ectomy of the atrial appendage was recommended and simultaneous three-dimensional mapping was considered accurate for the real-time location.
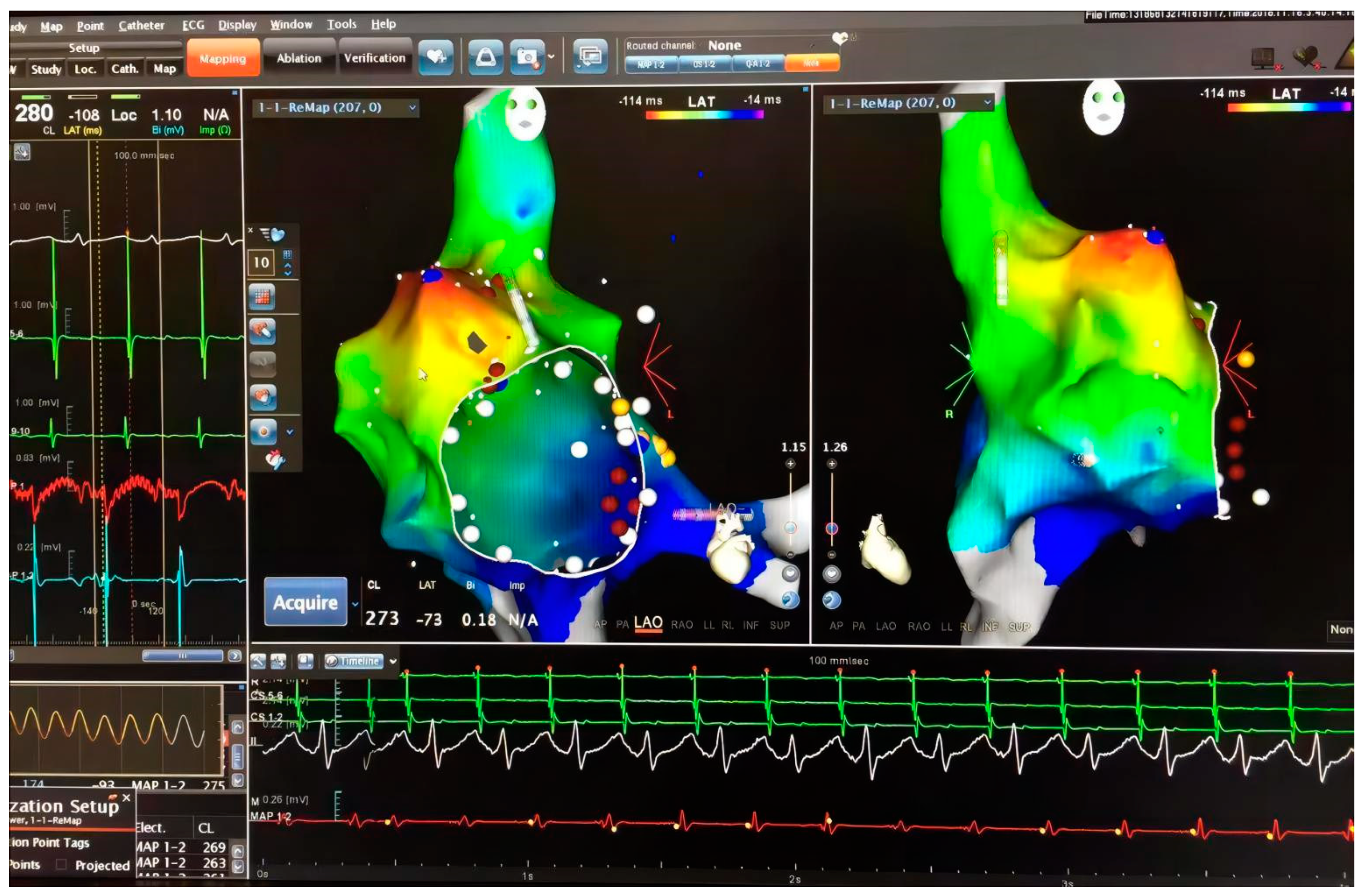
The patient was sent to the operating room immediately. Three-dimensional mapping guiding by Ensite
TM system was performed with zero-fluoroscopy, which also confirmed the same origin. (
Figure 3). To avoid surgery, low-power, short-course ablation was performed again, and the results remained ineffective. Attempts to convert atrial fibrillation and terminate tachycardia by high-frequency stimulation also failed. Based on the failure of these attempts, surgical removal of the appendage became inevitable.
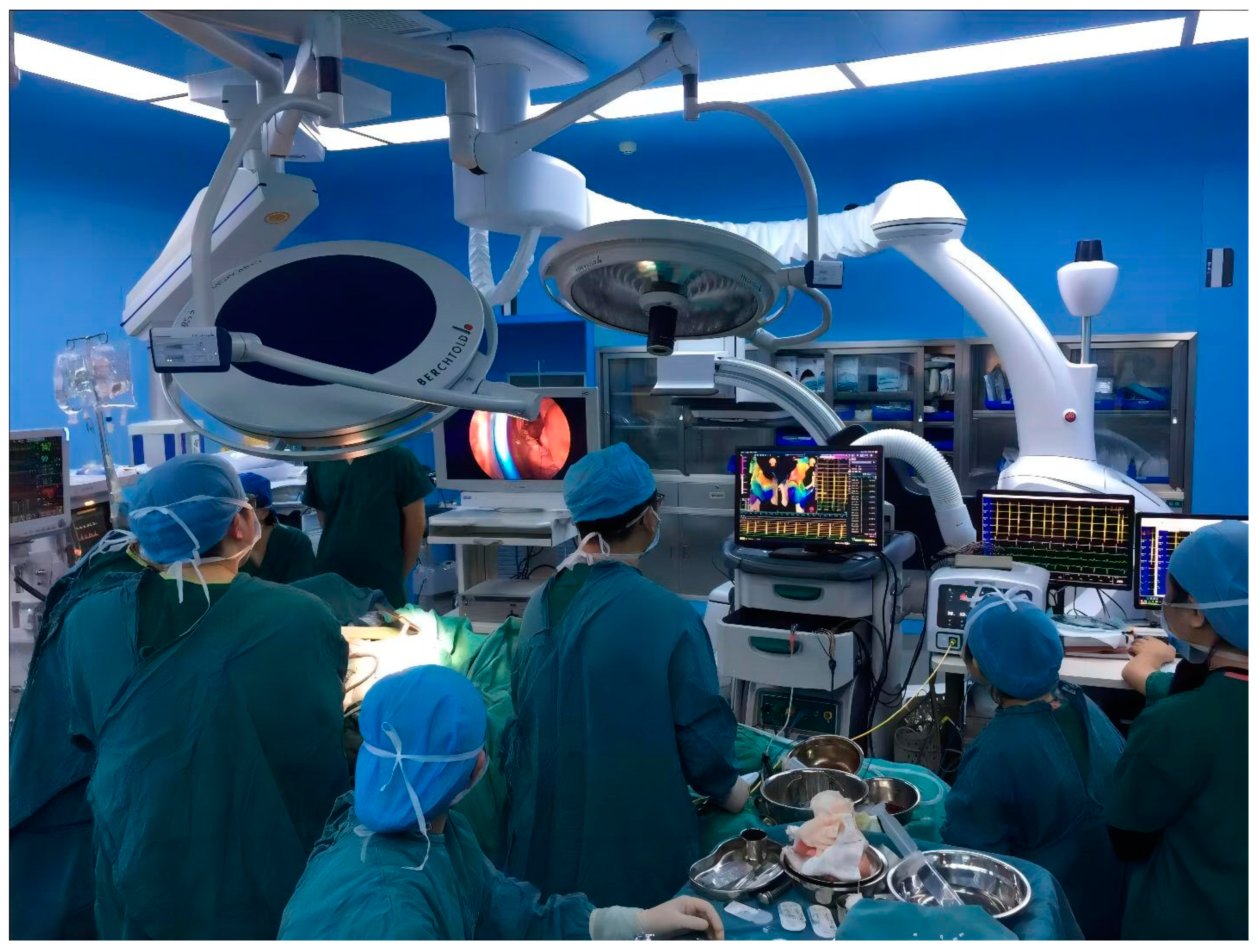
Under general anesthesia, after surgical disinfection and surgical drape, with the accessing ports at the right third and sixth intercostal space, the right atrium was on display in front of us (
Figure 4). Because of severe volume overload and increased filling pressure, the thin appendage distended and lost contour of its neck, making the right atrium almost like a ball. The surgeon could not stably clamp the appendage through the aperture. Urgent bloodletting, of an estimated 1500 milliliters, had to be performed from the sheath in the femoral vein, which finally helped the surgeon to clamp the shrunken appendage. The blood was infused with an autotransfusion system at last. After excision of RAA by a minimally invasive thoracoscopic approach (
Figure 5), her heart rate dropped to 120 beats per minute (bpm) (
Figure 6), being confirmed by sinus origin after mapping. The patient received invasive blood pressure monitoring throughout the procedure, which displayed acceptable hemodynamics for the patient and her fetus.
2.5. Literature Review
We performed a literature search on PubMed using the following search terms: “pregnancy” AND “atrial tachycardia” AND “catheter ablation”. Studies were reviewed for case reports on catheter ablation being performed in pregnant patients with atrial tachycardia. After screening titles and corresponding content, six published studies met the criteria.
3. Results
3.1. Results of Operation
The techniques of catheter introduction, mapping, and ablation were carried out according to established criteria. The patient was able to lie down for the time required to complete the procedure. Catheter mapping was successfully performed on the pregnant woman under the guidance of the Carto 3TM system and EnsiteTM system with the zero-fluoroscopy approach. The AT was observed to originate in the apex of the RAA. After a minimally invasive thoracoscopic procedure for RAA excision, the patient restored her sinus rhythm, and the hemodynamics became stable. After surgery, fetal heart monitoring showed that the fetus was in good health. Finally, after several wound dressing changes, the patient’s stitches were successfully removed and she and was discharged.
3.2. Follow-Up
This patient delivered a healthy boy by cesarean section. Both mother and child had an uneventful postoperative course. During 6 to 12 months of follow-up, complications related to the ablation and operation were observed neither in the mother nor the child.
3.3. Literature Review
A summary of the cases reported previously and our case are shown in
Table 1. Seven pregnant patients, undergoing RF catheter ablation for atrial tachycardia, were reported in six published studies [
8,
9,
10,
11,
12,
13]. Focal ATs originating from the AA or other sites were noted in three patients and four patients, respectively. The mean maternal age was 31 years old (range: 20–48), and RF catheter ablation was performed at a mean gestational age of 19.6 weeks (range: 27–30).
All ablations were successfully completed, except one case reported by Mizukami et al. [
8]. This was a 26-year-old woman in her first pregnancy presenting with persistent AT, which was also resistant to medication and cardioversion. The first attempt of catheter ablation failed. With the persistent AT, two months after the failed ablation, she developed severe systolic dysfunction and circulatory collapse. The second emergent RF catheter ablation was performed, revealing that the AT originated in the apex of the RAA. Nevertheless, the second attempt of ablation failed again. At last, she also received surgical RAA resection, leading to resolution of the tachycardia and improvement of cardiac function. Pathological examination of the resected RAA revealed a complex AA wall, including diverticulum formation and intramural hematoma, which explained the difficulty of RF catheter ablation. A subsequent pregnancy two years after treatment was uncomplicated.
It is worth noticing that all women and fetuses were in good condition and had an uneventful postoperative course, even for the patient who received surgical RAA resection. However, one patient’s baby, as reported by Yang et al., died during the process and her focal AT also originated from the RAA [
11].
4. Discussion
The present study reported a pregnant woman presenting with severe, extremely rapid, persistent, and refractory atrial tachycardia originating from RAA. She was suffering from continuous palpitation and hypotension at admission. Initial treatment with adenosine triphosphate failed. Zero-fluoroscopy mapping and ablation was recommended immediately. Three-dimensional mapping revealed an origination of RAA. Then, the planned ablation was canceled for fears of the high risk of cardiac perforation, which might be fatal both to the fetus and woman in this severe situation. Even repetitive burst pacing also could not stop the arrhythmia.
The following measures including repetitive burst pacing and various anti-arrhythmic drugs could not stop the arrhythmia. Electric cardioversion was not performed because of the automatic property of the tachycardia. Thus, thoracoscopic ectomy of the atrial appendage was recommended by an urgent multidisciplinary consultation. Simultaneous three-dimensional mapping was considered for guiding an accurate ectomy.
Of note, the manipulation of the ectomy was quite more difficult in this overweight pregnant woman than in general patients. Furthermore, the thin appendage distended and lost contour of its neck due to severe volume overload and increased filling pressure, making the right atrium almost like a ball; the surgeon could not stably clamp the appendage through the aperture. Urgent bloodletting, of an estimated 1500 milliliters, was performed from the sheath in the femoral vein, which finally helped the surgeon to clamp the shrunken appendage. The blood was infused with an autotransfusion system at last.
4.1. Focal AT of Pregnant Women
Pregnant women have a higher risk of arrhythmia than non-pregnant women due to increased blood volume, altered hormone levels, and increased myocardial automaticity [
1]. Abnormal automaticity during pregnancy has been found to be the main mechanism for maternal focal AT, and they often manifest around a gestation age of 24–25 weeks. Although recurrent episodes of focal AT may cause tachycardia-induced cardiomyopathy, its prognosis is acceptable with the improvement of left ventricular function and spontaneous resolution of the arrhythmia after delivery in the majority of patients. However, the biological basis for the manifestation of focal AT due to automaticity during pregnancy is still unclear [
14].
The underlying reasons may be multi-factorial. First, autonomic adaptations to hemodynamic changes during pregnancy may stimulate some myocardial cells, which have already been vulnerable to arrhythmogenesis. It has been found that these abnormal cells have nodal-like electrophysiological properties with spontaneous automaticity (Phase 4 depolarization) and adenosine sensitivity. Their proarrhythmogenic potential may be unmasked by the increased β-2 adrenergic sensitivity and β adrenergic agonists associated with normal pregnancy. Second, plasma volume markedly increases during normal pregnancy, and the subsequent mechanical stress and stretch of the atrial walls may also facilitate the occurrence of arrhythmias. Third, animal studies found that pregnancy increased the density of the hyperpolarization-activated current (If), which contributed to the normal increase in heart rate in pregnancy but possibly also predisposing for automatic focal AT [
14].
4.2. Limitation of Conventional Catheter Ablation for Pregnant Women
Despite the safety of medicines and catheter ablation applications, managing pregnant women with SVT has been challenging in clinical practice for a long time [
15]. Recently, RF catheter ablation has been recommended as Class IIa for this situation with a level of evidence of C [
16]. It is often applied for patients who are suffering from medication failure and experience frequent episodes or present hemodynamic changes. However, conventional RF catheter ablation highly relies on fluoroscopic guidance, which can put both the pregnant women and fetuses at high risk of radiation exposure. Therefore, there is no ideal strategy for curing those arrhythmias in pregnant women [
17]. Therefore, it is necessary to develop an effective and safer therapeutic method.
As for conventional catheter ablation, fluoroscopy is necessary for guiding catheter manipulation and visualizing cardiac anatomy, making radiation exposure inevitable. The awareness of radiation doses and risks is essential today in order to apply the risk–benefit assessment and to reinforce the principles of justification and optimization in clinical practice [
18]. Radiation exposure related to conventional catheter ablation carries small but non-negligible stochastic and deterministic effects on health, especially for the developing fetus [
18]. Andreassi et al. confirmed a definite relationship between long-term exposure in a catheterization laboratory and chromosome breaks [
19]. Such radiation exposure is particularly harmful to pregnant women, potentially causing side effects such as fetal death, major organ malformations, intrauterine growth restriction, microcephaly, and cognitive impairment [
20]. Previous studies have shown that prenatal radiation at 10 mGy also increases the risk of tumor development in children [
21].
4.3. Catheter Ablation for Pregnant Women with Zero Fluoroscopy
Advances in electroanatomic mapping (EAM) have made zero-fluoroscopy the goal of many, if not most, catheter ablation procedures. In addition to the reduction in radiation exposure, an EAM system could also offer several benefits. For example, these mapping systems are able to locate the correct position of any electrode at any time and allow an accurate reconstruction of the geometry of both heart chambers and vessels, simplifying navigation and reducing the procedure time [
22]. It is also helpful to understand the relationship between bipoles and cardiac anatomy, and between different structures and facilitating complex anatomy cases, continuously visualizing two projections at the same time. EAM systems allow visualization of the catheters from the beginning to the end of the procedure [
23].
The advantage of RF catheter ablation utilizing the EAM system has been increasingly acknowledged by healthcare professionals due to the advantage of minimal or even no radiation exposure, making it an ideal choice for pregnant women undergoing catheter ablation [
4]. Szumowski et al. reported that nine pregnant women with arrhythmias underwent successful ablation without complications, receiving minimum or no X-ray exposure [
4]. Intracardiac echo and electroanatomical mapping systems have also been described to be critical in limiting maternal and fetal radiation exposure [
24]. Our center confirmed that the medical staff using the zero-fluoroscopy approach felt less fatigue [
25]. We also demonstrated that RF catheter ablation of SVT or PVC/VT in pregnant patients can be safely and effectively performed with a completely zero-fluoroscopy approach [
26,
27]. Depending on all of these, the European Society for Cardiology recommended that zero-fluoroscopy catheter ablation should be considered in cases of drug-refractory or poorly tolerated SVT in experienced centers [
16].
In this case, zero-fluoroscopy mapping and ablation were initially planned since adenosine triphosphate failed to terminate the tachycardia. Carto
® system was chosen for the primary mapping because it would be less easy for a cardiac anatomy reconstructed by a magnetic field to become deformed compared with that by an electric field. As a special type of SVT, focal AT is derived from specific sites of the atrium [
3,
5]. Clinically, the common sites include the crista terminalis, tricuspid annulus, CS ostium, pulmonary veins, mitral annulus, para-Hisian region, and interatrial septum [
28,
29,
30,
31,
32,
33,
34,
35]. Accurate location of the origin is critical for a successful ablation.
4.4. Atrial Tachycardia Originating from Atrial Appendage
Atrial tachycardia originating from AA accounts for 3.8% of the SVT [
6,
7] and is usually persistent and drug-resistant [
36]. It can even cause tachycardia-induced cardiomyopathy [
32]. The apex of an atrial appendage is extremely thin and vulnerable, and catheter ablation applied here would be at risk and have higher recurrence despite the use of fluoroscopic guidance; thus, it is often treated by surgical resection [
7]. Apart from endocardial access, percutaneous epicardial ablation [
37] is an alternative option. However, the reported complications, such as pericardial effusion, phrenic nerve injury, and collateral damage to the coronary artery, make it less favorable [
38]. Additionally, further surgery might become more difficult because of the pericarditis when epicardial ablation fails.
Although the atrial appendage possesses endocrine function and can act as a blood buffer to some extent [
39], the ectomy appears to have no impact on sinus rhythm, normal cardiac function, and long-term hemodynamic effects, which has been confirmed by previous studies [
40]. Ohtsuka et al. proved that removing the atrial appendage was safe [
41]. Similarly, left atrial appendage occlusion employed in patients with atrial fibrillation also demonstrated safe outcomes except for low incidences of complications regarding device-related thrombus or catheter manipulation [
41,
42].
Atrial appendage is relatively complex and comprises thick pectinate muscle bands with intervening thin-walled myocardium, elongated morphology with a multilobulated apex, and a comparatively narrow orifice [
7]. Catheter ablation could be far more challenging at the apex of the atrial appendage. About seven years ago, our team evidenced that one woman had cardiac perforation and pericardial perfusion, and the wound had been covered by a thrombus clot due to the catheter ablation, which was performed before the surgical ectomy of appendage. The patient in this study had had severe palpitation, obvious dyspnea, and hemodynamic changes. Prolonged procedure, multiple attempts, and possible recurrence doubtlessly would greatly increase the risk of complications, such as cardiogenic shock or tamponade, which could be fatal both for the mother and the fetus. Therefore, the MDT method, which combined video-assisted thoracoscopic ectomy with three-dimensional and zero-fluoroscopy guidance, a thorough radical measure, was finally taken after consultation. The rapid arrhythmia terminated at once during the clamping and did not occur after the ectomy.
5. Conclusions
We presented here a pregnant woman who had severe palpitation, dyspnea, and hypotension due to persistent, refractory, and extremely rapid tachycardia. As adenosine triphosphate could not terminate the arrhythmia, a zero-fluoroscopy catheter ablation was arranged immediately. Three-dimensional mapping with a magnetic field demonstrated an origin from the distal part of RAA. Burst pacing at high rates, ablation with low power, and administration of various drugs, such as verapamil, propafenone, cedilanid, and esmolol, all failed. Considering the risk of ablation using high power and that possible recurrence might be fatal in this situation, video-assisted thoracoscopic ectomy was considered after consultation; three-dimensional electric field mapping was used for accurate location during the ectomy because the X-ray machine in the hybrid operating room was occupied. After 1500 mL of bloodletting, being performed to shrink the bulgy appendage, the surgeon was able to clamp the apex of the appendage. The patient remained stable with autotransfusion and recovered soon after appendage ectomy. She had a healthy baby and had no recurrence during follow-up. MDT measures, using thoracoscopic ectomy and the three-dimensional and zero-fluoroscopy electroanatomical mapping technique, is minimally invasive and a promising strategy.
Author Contributions
Conceptualization, Y.B. and G.C.; methodology, J.Q.; software, J.Q.; validation, Y.B., J.Q. and M.H.; formal analysis, M.H.; investigation, Y.B. and J.Q.; resources, G.C.; data curation, J.Q.; writing—original draft preparation, Y.B.; writing—review and editing, J.Q.; visualization, M.H.; supervision, G.C.; project administration, G.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (TJ-IRB2021084), approval on 4 August 2021.
Informed Consent Statement
Informed consent was obtained from this subject involved in the study.
Data Availability Statement
The data is unavailable due to privacy restrictions now.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
AA = atrial appendage, AT = atrial tachycardia, CS = coronary sinus, LAA = left atrial appendage, LAO = left anterior oblique view, MDT = multidisciplinary treatment, RAA = right atrial appendage, RAO = right anterior oblique view, RF = radiofrequency, SVT = supraventricular tachycardia.
References
- Moore, J.S.; Teefey, P.; Rao, K.; Berlowitz, M.S.; Chae, S.H.; Yankowitz, J. Maternal arrhythmia: A case report and review of the literature. Obstet. Gynecol. Surv. 2012, 67, 298–312. [Google Scholar] [CrossRef] [PubMed]
- Robins, K.; Lyons, G. Supraventricular tachycardia in pregnancy. Br. J. Anaesth. 2004, 92, 140–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, R.L.; Joglar, J.A.; Caldwell, M.A.; Calkins, H.; Conti, J.B.; Deal, B.J.; Estes, N.A., 3rd; Field, M.E.; Goldberger, Z.D.; Hammill, S.C.; et al. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients with Supraventricular Tachycardia: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2016, 67, e27–e115. [Google Scholar] [CrossRef] [PubMed]
- Szumowski, L.; Szufladowicz, E.; Orczykowski, M.; Bodalski, R.; Derejko, P.; Przybylski, A.; Urbanek, P.; Kuśmierczyk, M.; Koźluk, E.; Sacher, F.; et al. Ablation of severe drug-resistant tachyarrhythmia during pregnancy. J. Cardiovasc. Electrophysiol. 2010, 21, 877–882. [Google Scholar] [CrossRef]
- Taylor, C.M.; Samardhi, H.; Haqqani, H.M. Atrial tachycardias arising from the atrial appendages and aortic sinus of valsalva. Curr. Cardiol. Rev. 2015, 11, 118–126. [Google Scholar] [CrossRef] [Green Version]
- Roberts-Thomson, K.C.; Kistler, P.M.; Haqqani, H.M.; McGavigan, A.D.; Hillock, R.J.; Stevenson, I.H.; Morton, J.B.; Vohra, J.K.; Sparks, P.B.; Kalman, J.M. Focal atrial tachycardias arising from the right atrial appendage: Electrocardiographic and electrophysiologic characteristics and radiofrequency ablation. J. Cardiovasc. Electrophysiol. 2007, 18, 367–372. [Google Scholar] [CrossRef]
- Guo, X.-G.; Zhang, J.-L.; Ma, J.; Jia, Y.-H.; Zheng, Z.; Wang, H.-Y.; Su, X.; Zhang, S. Management of focal atrial tachycardias originating from the atrial appendage with the combination of radiofrequency catheter ablation and minimally invasive atrial appendectomy. Heart Rhythm 2014, 11, 17–25. [Google Scholar] [CrossRef]
- Mizukami, A.; Suzuki, M.; Nakamura, R.; Kuroda, S.; Ono, M.; Matsue, Y.; Iwatsuka, R.; Yonetsu, T.; Matsumura, A.; Hashimoto, Y. Histological examination of the right atrial appendage after failed catheter ablation for focal atrial tachycardia complicated by cardiogenic shock in a post-partum patient. J. Arrhythmia 2016, 32, 227–229. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, J.D.; Helms, A.; Mangrum, J.M.; DiMarco, J.P. Ablation of incessant left atrial tachycardia without fluoroscopy in a pregnant woman. J. Cardiovasc. Electrophysiol. 2011, 22, 346–349. [Google Scholar] [CrossRef]
- Zuberi, Z.; Silberbauer, J.; Murgatroyd, F. Successful Non-Fluoroscopic Radiofrequency Ablation of Incessant Atrial Tachycardia in a High Risk Twin Pregnancy. Indian Pacing Electrophysiol. J. 2014, 14, 26–31. [Google Scholar] [CrossRef] [Green Version]
- Yang, P.-S.; Park, J.; Pak, H.-N. Radiofrequency catheter ablation of incessant atrial tachycardia in pregnant women with minimal radiation exposure: Lessons from two case studies. J. Cardiol. Cases 2014, 9, 213–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barros, C.B.S.; Chokr, M.O.; Pisani, C.; Leite, T.S.B.; Avila, W.S.; Scanavacca, M.I. Catheter ablation of atrial tachycardia on the non-coronary aortic cusp during pregnancy without fluoroscopy. HeartRhythm Case Rep. 2018, 4, 566–569. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; Qi, S.; Cai, H.; Wang, D.; Ru, L. Non-Fluoroscopic Radiofrequency Ablation of Left Atrial Appendage Tachycardia during Early Pregnancy. Braz. J. Cardiovasc. Surg. 2019, 34, 495–498. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.C.; Shen, C.; McLaughlin, T.J.; Li, J.Z.; Hauspurg, A.; Berlacher, K.L.; Bhonsale, A.; Jain, S.K.; Kancharla, K.; Saba, S. Maternal focal atrial tachycardia during pregnancy: A systematic review. J. Cardiovasc. Electrophysiol. 2020, 31, 2982–2997. [Google Scholar] [CrossRef] [PubMed]
- Knotts, R.J.; Garan, H. Cardiac arrhythmias in pregnancy. Semin. Perinatol. 2014, 38, 285–288. [Google Scholar] [CrossRef]
- Calkins, H. The 2019 ESC Guidelines for the Management of Patients with Supraventricular Tachycardia. Eur. Heart J. 2019, 40, 3812–3813. [Google Scholar] [CrossRef] [Green Version]
- Bombelli, F.; Lagona, F.; Salvati, A.; Catalfamo, L.; Ferrari, A.G.; Pappone, C. Radiofrequency catheter ablation in drug refractory maternal supraventricular tachycardias in advanced pregnancy. Obstet. Gynecol. 2003, 102, 1171–1173. [Google Scholar] [CrossRef]
- Carpeggiani, C.; Kraft, G.; Caramella, D.; Semelka, R.; Picano, E. Radioprotection (un)awareness in cardiologists, and how to improve it. Int. J. Cardiovasc. Imaging 2012, 28, 1369–1374. [Google Scholar] [CrossRef]
- Andreassi, M.G.; Cioppa, A.; Botto, N.; Joksic, G.; Manfredi, S.; Federici, C.; Ostojic, M.; Rubino, P.; Picano, E. Somatic DNA damage in interventional cardiologists: A case-control study. FASEB J. 2005, 19, 998–999. [Google Scholar] [CrossRef]
- Williams, P.M.; Fletcher, S. Health effects of prenatal radiation exposure. Am. Fam. Physician 2010, 82, 488–493. [Google Scholar]
- Doll, R.; Wakeford, R. Risk of childhood cancer from fetal irradiation. Br. J. Radiol. 1997, 70, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Giaccardi, M.; Anselmino, M.; Del Greco, M.; Mascia, G.; Perini, A.P.; Mascia, P.; De Ferrari, G.M.; Picano, E. Radiation awareness in an Italian multispecialist sample assessed with a web-based survey. Acta Cardiol. 2021, 76, 307–311. [Google Scholar] [CrossRef]
- Tonko, J.B.; Douglas, H.; Wright, M.J. Ivabradine-sensitive incessant atrial tachycardia during pregnancy: A case report. Eur. Heart J. Case Rep. 2021, 5, ytab367. [Google Scholar] [CrossRef] [PubMed]
- Driver, K.; Chisholm, C.A.; Darby, A.E.; Malhotra, R.; Dimarco, J.P.; Ferguson, J.D. Catheter Ablation of Arrhythmia during Pregnancy. J. Cardiovasc. Electrophysiol. 2015, 26, 698–702. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, G.Z.; Yao, Y.; Bai, Y.; Chu, H.M.; Ma, K.Z.; Liew, R.; Liu, H.; Zhong, G.Q.; Xue, Y.M.; et al. Ablation of idiopathic ventricular arrhythmia using zero-fluoroscopy approach with equivalent efficacy and less fatigue: A multicenter comparative study. Medicine 2017, 96, e6080. [Google Scholar] [CrossRef]
- Chen, G.; Sun, G.; Xu, R.; Chen, X.; Yang, L.; Bai, Y.; Yang, S.; Guo, P.; Zhang, Y.; Zhao, C.; et al. Zero-fluoroscopy catheter ablation of severe drug-resistant arrhythmia guided by Ensite NavX system during pregnancy: Two case reports and literature review. Medicine 2016, 95, e4487. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Wang, Y.; Proietti, R.; Wang, X.; Ouyang, F.; Ma, C.S.; Yu, R.H.; Zhao, C.; Ma, K.; Qiu, J.; et al. Zero-fluoroscopy approach for ablation of supraventricular tachycardia using the Ensite NavX system: A multicenter experience. BMC Cardiovasc. Disord. 2020, 20, 48. [Google Scholar] [CrossRef] [Green Version]
- Kalman, J.M.; E Olgin, J.; Karch, M.R.; Hamdan, M.; Lee, R.J.; Lesh, M.D. “Cristal tachycardias”: Origin of right atrial tachycardias from the crista terminalis identified by intracardiac echocardiography. J. Am. Coll. Cardiol. 1998, 31, 451–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morton, J.B.; Sanders, P.; Das, A.; Vohra, J.K.; Sparks, P.B.; Kalman, J.M. Focal atrial tachycardia arising from the tricuspid annulus: Electrophysiologic and electrocardiographic characteristics. J. Cardiovasc. Electrophysiol. 2001, 12, 653–659. [Google Scholar] [CrossRef]
- Kistler, P.M.; Fynn, S.P.; Haqqani, H.; Stevenson, I.H.; Vohra, J.K.; Morton, J.B.; Sparks, P.B.; Kalman, J.M. Focal atrial tachycardia from the ostium of the coronary sinus: Electrocardiographic and electrophysiological characterization and radiofrequency ablation. J. Am. Coll. Cardiol. 2005, 45, 1488–1493. [Google Scholar] [CrossRef] [Green Version]
- Yamada, T.; Lau, Y.R. Successful catheter ablation of a focal atrial tachycardia originating from the coronary sinus ostium in a patient with a history of Fontan conversion and dextrocardia. Europace 2018, 20, 1351. [Google Scholar] [CrossRef] [PubMed]
- Kistler, P.M.; Sanders, P.; Fynn, S.P.; Stevenson, I.H.; Hussin, A.; Vohra, J.K.; Sparks, P.B.; Kalman, J.M. Electrophysiological and electrocardiographic characteristics of focal atrial tachycardia originating from the pulmonary veins: Acute and long-term outcomes of radiofrequency ablation. Circulation 2003, 108, 1968–1975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kistler, P.M.; Sanders, P.; Hussin, A.; Morton, J.B.; Vohra, J.K.; Sparks, P.B.; Kalman, J.M. Focal atrial tachycardia arising from the mitral annulus: Electrocardiographic and electrophysiologic characterization. J. Am. Coll. Cardiol. 2003, 41, 2212–2219. [Google Scholar] [CrossRef]
- Iwai, S.; Badhwar, N.; Markowitz, S.M.; Stambler, B.S.; Keung, E.; Lee, R.J.; Chung, J.H.; Olgin, J.E.; Scheinman, M.M.; Lerman, B.B. Electrophysiologic properties of para-Hisian atrial tachycardia. Heart Rhythm 2011, 8, 1245–1253. [Google Scholar] [CrossRef]
- Wong, M.C.; Kalman, J.M.; Ling, L.H.; Medi, C.; The, A.; Lee, G.; Kumar, S.; Morton, J.B.; Kistler, P.M. Left septal atrial tachycardias: Electrocardiographic and electrophysiologic characterization of a paraseptal focus. J. Cardiovasc. Electrophysiol. 2013, 24, 413–418. [Google Scholar] [CrossRef]
- Freixa, X.; Berruezo, A.; Mont, L.; Magnani, S.; Benito, B.; Tolosana, J.M.; Perafan, P.; Tamborero, D.; Brugada, J. Characterization of focal right atrial appendage tachycardia. Europace 2008, 10, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Phillips, K.P.; Natale, A.; Sterba, R.; Saliba, W.I.; Burkhardt, J.D.; Wazni, O.; Liberman, L.; Schweikert, R.A. Percutaneous pericardial instrumentation for catheter ablation of focal atrial tachycardias arising from the left atrial appendage. J. Cardiovasc. Electrophysiol. 2008, 19, 430–433. [Google Scholar] [CrossRef]
- Yamada, T. Transthoracic epicardial catheter ablation: Indications, techniques, and complications. Circ. J. 2013, 77, 1672–1680. [Google Scholar] [CrossRef] [Green Version]
- Donal, E.; Yamada, H.; Leclercq, C.; Herpin, D. The left atrial appendage, a small, blind-ended structure: A review of its echocardiographic evaluation and its clinical role. Chest 2005, 128, 1853–1862. [Google Scholar] [CrossRef] [Green Version]
- Medi, C.; Kalman, J.M.; Haqqani, H.; Vohra, J.K.; Morton, J.B.; Sparks, P.B.; Kistler, P. Tachycardia-mediated cardiomyopathy secondary to focal atrial tachycardia: Long-term outcome after catheter ablation. J. Am. Coll. Cardiol. 2009, 53, 1791–1797. [Google Scholar] [CrossRef] [Green Version]
- Ohtsuka, T.; Ninomiya, M.; Nonaka, T.; Hisagi, M.; Ota, T.; Mizutani, T. Thoracoscopic stand-alone left atrial appendectomy for thromboembolism prevention in nonvalvular atrial fibrillation. J. Am. Coll. Cardiol. 2013, 62, 103–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, P.A.; Holmes, D.R. Non-surgical left atrial appendage closure for stroke prevention in atrial fibrillation. J. Cardiovasc. Electrophysiol. 2011, 22, 1184–1191. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}