
Optimization of Therapy and the Risk of Probiotic Use during Antibiotherapy in Septic Critically Ill Patients: A Narrative Review
 ,
,
Abstract
:1. Introduction
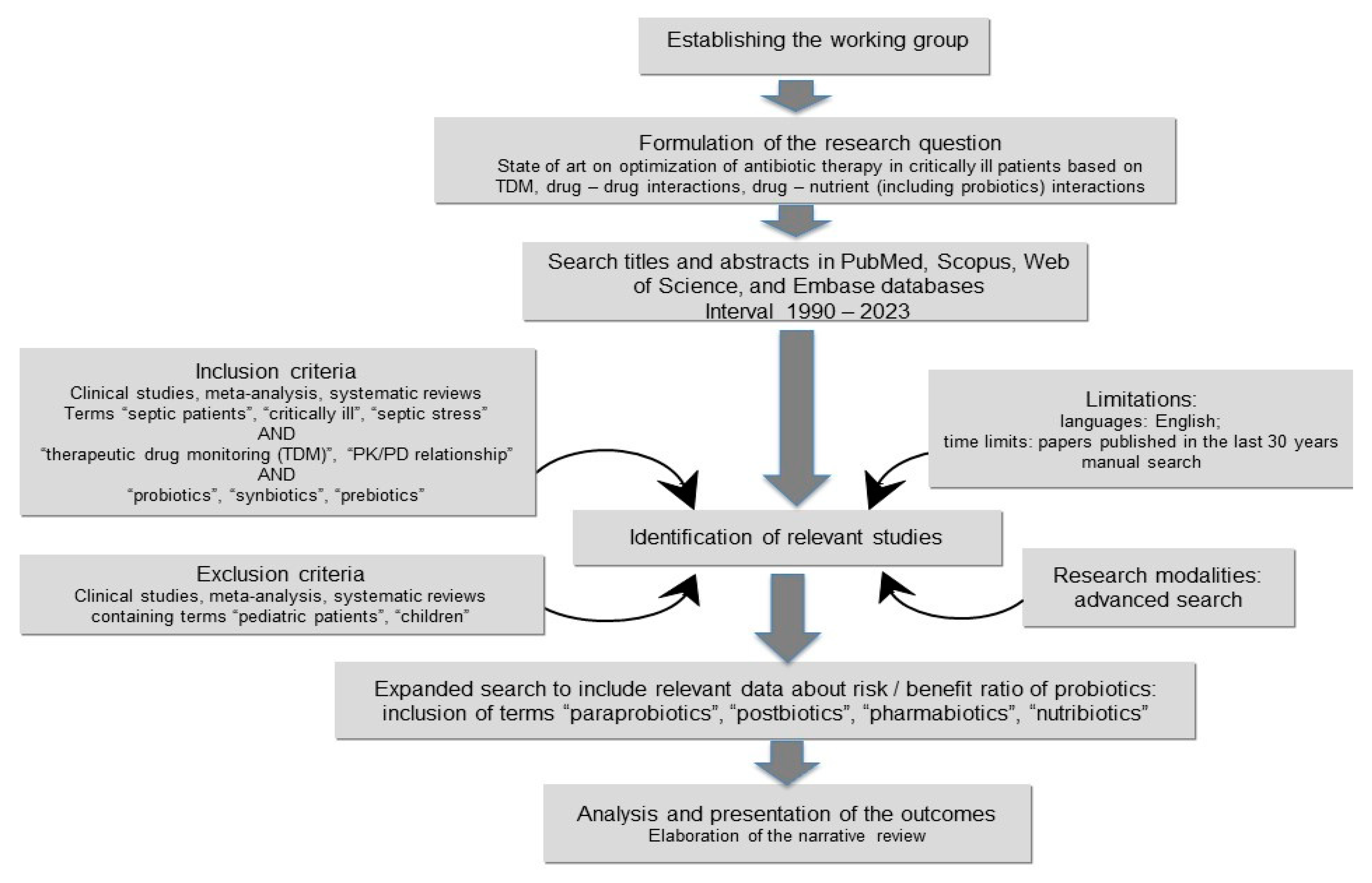
2. Materials and Methods
3. Results
3.1. TDM-Guided Recommendations in Septic Critically Ill Patients
3.1.1. Beta-Lactams TDM-Guided Recommendations
3.1.2. Beta-Lactam and Beta-Lactamase Inhibitor Combinations TDM-Guided Recommendations
3.1.3. Aminoglycosides TDM-Guided Recommendations
3.1.4. Oxazolidinones TDM-Guided Recommendations
3.1.5. Polymyxins TDM-Guided Recommendations
3.2. Antibiotic–Drug Interactions of High Interest in Critically Ill Patients
3.3. The Risk of Probiotic Use in Critically Ill Patients
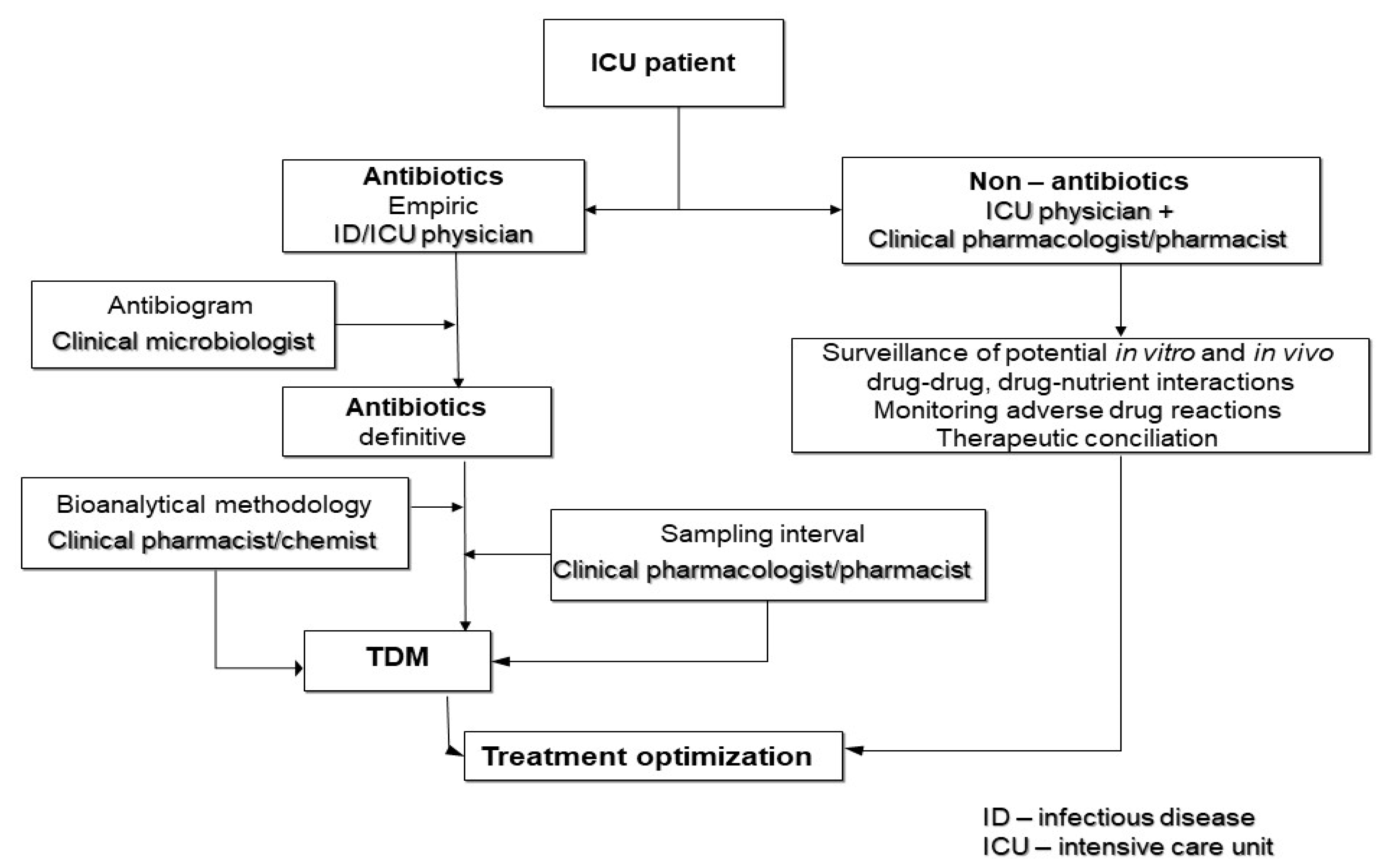
3.4. Multidisciplinary Approach Therapy Optimization in Septic Critically Ill Patients
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tosi, M.; Roat, E.; Biasi, S.D.; Munari, E.; Venturelli, S.; Coloretti, I.; Biagioni, E.; Cossarizza, A.; Girardis, M. Multidrug resistant bacteria in critically ill patients: A step further antibiotic therapy. J. Emerg. Crit. Care Med. 2018, 2, 103. [Google Scholar] [CrossRef]
- Pasero, D.; Cossu, A.P.; Terragni, P. Multi-Drug Resistance Bacterial Infections in Critically Ill Patients Admitted with COVID-19. Microorganisms 2021, 20, 1773. [Google Scholar] [CrossRef] [PubMed]
- Tabah, A.; Koulenti, D.; Laupland, K.; Misset, B.; Valles, J.; Bruzzi de Carvalho, F.; Paiva, J.A.; Cakar, N.; Ma, X.; Eggimann, P.; et al. Characteristics and determinants of outcome of hospital-acquired bloodstream infections in intensive care units: The EUROBACT International Cohort Study. Intensive Care Med. 2012, 38, 1930–1945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lat, I.; Daley, M.J.; Shewale, A.; Pangrazzi, M.H.; Hammond, D.; Olsen, K.M.; DEFINE study group and the Discovery Research Network. A Multicenter, Prospective, Observational Study to Determine Predictive Factors for Multidrug-Resistant Pneumonia in Critically Ill Adults: The DEFINE Study. Pharmacotherapy 2019, 39, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Pilmis, B.; Le Monnier, A.; Zahar, J.R. Gut Microbiota, Antibiotic Therapy and Antimicrobial Resistance: A Narrative Review. Microorganisms 2020, 8, 269. [Google Scholar] [CrossRef] [Green Version]
- Wei, B.W.; Wiersinga, W.J. The role of the gut microbiota in sepsis. Lancet Gastroenterol. Hepatol. 2017, 2, 135–143. [Google Scholar]
- Klingensmith, N.J.; Coopersmith, C.M. The Gut as the Motor of Multiple Organ Dysfunction in Critical Illness. Crit. Care Clin. 2016, 32, 203–212. [Google Scholar] [CrossRef] [Green Version]
- Luyt, C.E.; Bréchot, N.; Trouillet, J.L.; Chastre, J. Antibiotic stewardship in the intensive care unit. Crit. Care 2014, 18, 480. [Google Scholar] [CrossRef] [Green Version]
- Lanckohr, C.; Boeing, C.; De Waele, J.J.; de Lange, D.W.; Schouten, J.; Prins, M.; Nijsten, M.; Povoa, P.; Morris, A.C.; Bracht, H. Antimicrobial stewardship, therapeutic drug monitoring and infection management in the ICU: Results from the international A- TEAMICU survey. Ann. Intensive Care 2021, 11, 131. [Google Scholar] [CrossRef]
- Bassetti, M.; De Waele, J.J.; Eggimann, P.; Garnacho-Montero, J.; Kahlmeter, G.; Menichetti, F.; Nicolau, D.P.; Paiva, J.A.; Tumbarello, M.; Welte, T.; et al. Preventive and therapeutic strategies in critically ill patients with highly resistant bacteria. Intensive Care Med. 2015, 41, 776–795. [Google Scholar] [CrossRef]
- Kelly, C.R.; Fischer, M.; Allegretti, J.R.; LaPlante, K.; Stewart, D.B.; Limketkai, B.N.; Stollman, N.H. ACG Clinical Guidelines: Prevention, Diagnosis, and Treatment of Clostridioides difficile Infections. Am. J. Gastroenterol. 2021, 116, 1124–1147. [Google Scholar] [CrossRef]
- Roberts, J.A.; Abdul-Aziz, M.H.; Lipman, J.; Mouton, J.W.; Vinks, A.A.; Felton, T.W.; Hope, W.W.; Farkas, A.; Neely, M.N.; Schentag, J.J.; et al. Individualised antibiotic dosing for patients who are critically ill: Challenges and potential solutions. Lancet Infect. Dis. 2014, 14, 498–509. [Google Scholar] [CrossRef] [Green Version]
- Neely, M.; Jelliffe, R. Optimizing single-drug antibacterial and antifungal therapy. In Individualized Drug Therapy of Patients. BASIC Foundations, Relevant Software and Clinical Applications; Jelliffe, R., Neely, M., Eds.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 157–179. [Google Scholar]
- Li, J.; Xie, S.; Ahmed, S.; Wang, F.; Gu, Y.; Zhang, C.; Chai, X.; Wu, Y.; Cai, J.; Cheng, G. Antimicrobial Activity and Resistance: Influencing Factors. Front. Pharm. 2017, 8, 364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landersdorfer, C.B.; Nation, R.L. Limitations of Antibiotic MIC-Based PK-PD Metrics: Looking Back to Move Forward. Front. Pharmacol. 2021, 12, 770518. [Google Scholar] [CrossRef] [PubMed]
- Jager, N.G.; van Hest, R.M.; Lipman, J.; Taccone, F.S.; Roberts, J.A. Therapeutic drug monitoring of anti-infective agents in critically ill patients. Expert Rev Clin. Pharmacol. 2016, 9, 961–979. [Google Scholar] [CrossRef]
- Rodríguez-Gascón, A.; Solinís, M.Á.; Isla, A. The Role of PK/PD Analysis in the Development and Evaluation of Antimicrobials. Pharmaceutics. 2021, 13, 833. [Google Scholar] [CrossRef]
- Dhaese, S.A.M.; Hoste, E.A.; De Waele, J.J. Why We May Need Higher Doses of Beta-Lactam Antibiotics: Introducing the ‘Maximum Tolerable Dose’. Antibiotics 2022, 11, 889. [Google Scholar] [CrossRef]
- del Mar Fernández de Gatta, M.; Martin-Suarez, A.; Lanao, J.M. Approaches for dosage individualisation in critically ill patients. Expert. Opin. Drug Metab. Toxicol. 2013, 9, 1481–1493. [Google Scholar] [CrossRef]
- Chai, M.G.; Cotta, M.O.; Abdul-Aziz, M.H.; Roberts, J.A. What Are the Current Approaches to Optimising Antimicrobial Dosing in the Intensive Care Unit? Pharmaceutics 2020, 12, 638. [Google Scholar] [CrossRef]
- Jager, N.G.L.; Chai, M.G.; van Hest, R.M.; Lipman, J.; Roberts, J.A.; Cotta, M.O. Precision dosing software to optimize antimicrobial dosing: A systematic search and follow-up survey of available programs. Clin. Microbiol. Infect. 2022, 28, 1211–1224. [Google Scholar] [CrossRef] [PubMed]
- Cotta, M.O.; Lipman, J.; De Waele, J. Advancing precision-based antimicrobial dosing in critically ill patients. Intensive Care Med. 2023, 1–3. [Google Scholar] [CrossRef]
- Abdul-Aziz, M.H.; Alffenaar, J.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.A.; Pea, F.; Sjovall, F.; et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: A Position Paper. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.; Cotta, M.O.; Roberts, J.A. Pharmacokinetics/Pharmacodynamics of beta-Lactams and Therapeutic Drug Monitoring: From Theory to Practical Issues in the Intensive Care Unit. Semin. Respir. Crit. Care Med. 2019, 40, 476–487. [Google Scholar] [PubMed]
- Abdulla, A.; Ewoldt, T.M.J.; Purmer, I.M.; Muller, A.E.; Gommers, D.; Endeman, H.; Koch, B.C.P. A narrative review of predictors for beta-lactam antibiotic exposure during empirical treatment in critically ill patients. Expert. Opin. Drug Metab. Toxicol. 2021, 17, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Gatti, M.; Bartoletti, M.; Cojutti, P.G.; Gaibani, P.; Conti, M.; Giannella, M.; Viale, P.; Pea, F. A descriptive case series of pharmacokinetic/pharmacodynamic target attainment and microbiological outcome in critically ill patients with documented severe extensively drug-resistant Acinetobacter baumannii bloodstream infection and/or ventilator-associated pneumonia treated with cefiderocol. J. Glob. Antimicrob. Resist. 2021, 27, 294–298. [Google Scholar]
- Scharf, C.; Paal, M.; Schroeder, I.; Vogeser, M.; Draenert, R.; Irlbeck, M.; Zoller, M.; Liebchen, U. Therapeutic Drug Monitoring of Meropenem and Piperacillin in Critical Illness-Experience and Recommendations from One Year in Routine Clinical Practice. Antibiotics 2020, 9, 131. [Google Scholar] [CrossRef] [Green Version]
- Steffens, N.A.; Zimmermann, E.S.; Nichelle, S.M.; Brucker, N. Meropenem use and therapeutic drug monitoring in clinical practice: A literature review. J. Clin. Pharm. 2021, 46, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Lechtig-Wasserman, S.; Liebisch-Rey, H.; Diaz-Pinilla, N.; Blanco, J.; Fuentes-Barreiro, Y.V.; Bustos, R.H. Carbapenem Therapeutic Drug Monitoring in Critically Ill Adult Patients and Clinical Outcomes: A Systematic Review with Meta-Analysis. Antibiotics 2021, 10, 177. [Google Scholar] [CrossRef]
- Richter, D.C.; Frey, O.; Röhr, A.; Roberts, J.A.; Köberer, A.; Fuchs, T.; Papadimas, N.; Heinzel-Gutenbrunner, M.; Brenner, T.; Lichtenstern, C.; et al. Therapeutic drug monitoring-guided continuous infusion of piperacillin/tazobactam significantly improves pharmacokinetic target attainment in critically ill patients: A retrospective analysis of four years of clinical experience. Infection 2019, 47, 1001–1011. [Google Scholar] [CrossRef] [Green Version]
- Hagel, S.; Bach, F.; Brenner, T.; Bracht, H.; Brinkmann, A.; Annecke, T.; Hohn, A.; Weigand, M.; Michels, G.; Kluge, S.; et al. Effect of therapeutic drug monitoring-based dose optimization of piperacillin/tazobactam on sepsis-related organ dysfunction in patients with sepsis: A randomized controlled trial. Intensive Care Med. 2022, 48, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Goncette, V.; Layios, N.; Descy, J.; Frippiat, F. Continuous infusion, therapeutic drug monitoring and outpatient parenteral antimicrobial therapy with ceftazidime/avibactam: A retrospective cohort study. J. Glob. Antimicrob. Resist. 2021, 26, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Castaldo, N.; Cattelan, A.; Mussini, C.; Righi, E.; Tascini, C.; Menichetti, F.; Mastroianni, C.M.; Tumbarello, M.; Grossi, P.; et al. Ceftolozane/tazobactam for the treatment of serious Pseudomonas aeruginosa infections: A multicentre nationwide clinical experience. Int. J. Antimicrob. Agents 2019, 53, 408–415. [Google Scholar] [CrossRef]
- Navarrete-Rouco, M.E.; Luque, S.; Sorlí, L.; Benítez-Cano, A.; Roberts, J.A.; Grau, S. Therapeutic Drug Monitoring and Prolonged Infusions of Ceftolozane/Tazobactam for MDR/XDR Pseudomonas aeruginosa Infections: An Observational Study. Eur. J. Drug Metab. Pharm. 2022, 47, 561–566. [Google Scholar] [CrossRef]
- Clark, J.A.; Burgess, D.S. Plazomicin: A new aminoglycoside in the fight against antimicrobial resistance. Adv. Infect. Dis. 2020, 7, 2049936120952604. [Google Scholar] [CrossRef]
- Lin, B.; Hu, Y.; Xu, P.; Xu, T.; Chen, C.; He, L.; Zhou, M.; Chen, Z.; Zhang, C.; Yu, X.; et al. Expert consensus statement on therapeutic drug monitoring and individualization of linezolid. Front. Public Health 2022, 10, 967311. [Google Scholar] [CrossRef]
- Yang, M.; Zhao, L.; Wang, X.; Sun, C.; Gao, H.; Wang, X.; Qian, S. Population Pharmacokinetics and Dosage Optimization of Linezolid in Critically Ill Pediatric Patients. Antimicrob. Agents Chemother. 2021, 65, e02504-20. [Google Scholar] [CrossRef]
- Sazdanovic, P.; Jankovic, S.M.; Kostic, M.; Dimitrijevic, A.; Stefanovic, S. Pharmacokinetics of linezolid in critically ill patients. Expert. Opin. Drug Metab. Toxicol. 2016, 12, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Bandín-Vilar, E.; García-Quintanilla, L.; Castro-Balado, A.; Zarra-Ferro, I.; González-Barcia, M.; Campos-Toimil, M.; Mangas-Sanjuan, V.; Mondelo-García, C.; Fernández-Ferreiro, A. A Review of Population Pharmacokinetic Analyses of Linezolid. Clin. Pharm. 2022, 61, 789–817. [Google Scholar] [CrossRef] [PubMed]
- Dudhani, R.V.; Turnidge, J.D.; Nation, R.L.; Li, J. fAUC/MIC is the most predictive pharmacokinetic/pharmacodynamic index of colistin against Acinetobacter baumannii in murine thigh and lung infection models. J. Antimicrob. Chemother. 2010, 65, 1984–1990. [Google Scholar] [CrossRef] [Green Version]
- Yu, X.B.; Zhang, X.S.; Wang, Y.X.; Wang, Y.Z.; Zhou, H.M.; Xu, F.M.; Yu, J.H.; Zhang, L.W.; Dai, Y.; Zhou, Z.Y.; et al. Population Pharmacokinetics of Colistin Sulfate in Critically Ill Patients: Exposure and Clinical Efficacy. Front. Pharm. 2022, 13, 915958. [Google Scholar] [CrossRef]
- Ehrentraut, S.F.; Muenster, S.; Kreyer, S.; Theuerkauf, N.U.; Bode, C.; Steinhagen, F.; Ehrentraut, H.; Schewe, J.C.; Weber, M.; Putensen, C.; et al. Extensive Therapeutic Drug Monitoring of Colistin in Critically Ill Patients Reveals Undetected Risks. Microorganisms 2020, 8, 415. [Google Scholar] [CrossRef] [Green Version]
- Tran, T.B.; Velkov, T.; Nation, R.L.; Forrest, A.; Tsuji, B.T.; Bergen, P.; Li, J. Pharmacokinetics/pharmacodynamics of colistin and polymyxin B: Are we there yet? Int. J. Antimicrob. Agents 2016, 48, 592–597. [Google Scholar] [CrossRef] [Green Version]
- Couet, W.; Grégoire, N.; Marchand, S.; Mimoz, O. Colistin pharmacokinetics: The fog is lifting. Clin. Microbiol. Infect. 2012, 18, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reis, A.M.; Cassiani, S.H. Prevalence of potential drug interactions in patients in an intensive care unit of a university hospital in Brazil. Clinics 2011, 66, 9–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baniasadi, S.; Farzanegan, B.; Alehashem, M. Important drug classes associated with potential drug-drug interactions in critically ill patients: Highlights for cardiothoracic intensivists. Ann. Intensive Care 2015, 5, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kheshti, R.; Aalipour, M.; Namazi, S. A comparison of five common drug-drug interaction software programs regarding accuracy and comprehensiveness. J. Res. Pharm Pract. 2016, 5, 257–263. [Google Scholar] [PubMed]
- Morte-Romea, E.; Luque-Gómez, P.; Arenere-Mendoza, M.; Sierra-Monzón, J.L.; Camón Pueyo, A.; Pellejero Sagastizabal, G.; Verdejo Muñoz, G.; Sánchez Fabra, D.; Paño-Pardo, J.R. Performance Assessment of Software to Detect and Assist Prescribers with Antimicrobial Drug Interactions: Are all of them Created Equal? Antibiotics 2020, 9, 19. [Google Scholar] [CrossRef] [Green Version]
- Imperial, I.C.; Ibana, J.A. Addressing the Antibiotic Resistance Problem with Probiotics: Reducing the Risk of Its Double-Edged Sword Effect. Front. Microbiol. 2016, 7, 1983. [Google Scholar] [CrossRef] [Green Version]
- Morrow, L.E.; Gogineni, V.; Malesker, M.A. Probiotics in the intensive care unit. Nutr. Clin. Pract. 2012, 27, 235–241. [Google Scholar] [CrossRef]
- Chaudhari, A.; Dwivedi, M.K. The concept of probiotics, prebiotics, postbiotics, synbiotics, nutribiotics, and pharmabiotics. In Probiotics in the Prevention and Management of Human Diseases: A Scientific Perspective; Dwivedi, M., Amaresan, N., Sankaranaryanan, A., and Kemp, H., Eds.; Elsevier: Amsterdam, The Netherlands, 2022; pp. 7–9, 37. [Google Scholar]
- Teame, T.; Wang, A.; Xie, M.; Zhang, Z.; Yang, Y.; Ding, Q.; Gao, C.; Olsen, R.E.; Ran, C.; Zhou, Z. Paraprobiotics and Postbiotics of Probiotic Lactobacilli, Their Positive Effects on the Host and Action Mechanisms: A Review. Front Nutr. 2020, 7, 570344. [Google Scholar] [CrossRef] [PubMed]
- Vyas, U.; Ranganathan, N. Probiotics, prebiotics, and synbiotics: Gut and beyond. Gastroenterol. Res Pract. 2012, 872716, 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarpellini, E.; Rinninella, E.; Basilico, M.; Colomier, E.; Rasetti, C.; Larussa, T.; Santori, P.; Abenavoli, L. From Pre- and Probiotics to Post-Biotics: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 19, 37. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Faliva, M.A.; Perna, S.; Giacosa, A.; Peroni, G.; Castellazzi, A.M. Using probiotics in clinical practice: Where are we now? A review of existing meta-analyses. Gut Microbes 2017, 8, 521–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guarner, F.; Khan, A.G.; Garisch, J.; Eliakim, R.; Gangl, A.; Thomson, A.; Krabshuis, J.; Lemair, T.; Kaufmann, P.; de Paula, J.A.; et al. World Gastroenterology Organisation Global Guidelines: Probiotics and prebiotics. J. Clin. Gastroenterol. 2012, 46, 468–481. [Google Scholar] [CrossRef]
- Su, G.L.; Ko, C.W.; Bercik, P.; Falck-Ytter, Y.; Sultan, S.; Weizman, A.V.; Morgan, R.L. AGA Clinical Practice Guidelines on the Role of Probiotics in the Management of Gastrointestinal Disorders. Gastroenterology 2020, 159, 697–705. [Google Scholar] [CrossRef]
- Lerner, A.; Shoenfeld, Y.; Matthias, T. Probiotics: If It Does Not Help It Does Not Do Any Harm. Really? Microorganisms 2019, 7, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, C.; Lu, F.; Chen, J.; Ma, J.; Xu, N. Probiotic Supplementation Prevents the Development of Ventilator-Associated Pneumonia for Mechanically Ventilated ICU Patients: A Systematic Review and Network Meta-analysis of Randomized Controlled Trials. Front. Nutr. 2022, 9, 919156. [Google Scholar] [CrossRef]
- Naseri, A.; Seyedi-Sahebari, S.; Mahmoodpoor, A.; Sanaie, S. Probiotics in Critically Ill Patients: An Umbrella Review. Indian, J. Crit. Care Med. 2022, 26, 339–360. [Google Scholar]
- Sun, Y.C.; Wang, C.Y.; Wang, H.L.; Yuan, Y.; Lu, J.H.; Zhong, L. Probiotic in the prevention of ventilator-associated pneumonia in critically ill patients: Evidence from meta-analysis and trial sequential analysis of randomized clinical trials. BMC Pulm. Med. 2022, 22, 168. [Google Scholar] [CrossRef]
- Weng, H.; Li, J.G.; Mao, Z.; Feng, Y.; Wang, C.Y.; Ren, X.Q.; Zeng, X.T. Probiotics for Preventing Ventilator-Associated Pneumonia in Mechanically Ventilated Patients: A Meta-Analysis with Trial Sequential Analysis. Front. Pharmacol. 2017, 8, 717. [Google Scholar] [CrossRef] [Green Version]
- Cheema, H.A.; Shahid, A.; Ayyan, M.; Mustafa, B.; Zahid, A.; Fatima, M.; Ehsan, M.; Athar, F.; Duric, N.; Szakmany, T. Probiotics for the Prevention of Ventilator-Associated Pneumonia: An Updated Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients 2022, 14, 1600. [Google Scholar] [CrossRef]
- Su, M.; Jia, Y.; Li, Y.; Zhou, D.; Jia, J. Probiotics for the Prevention of Ventilator-Associated Pneumonia: A Meta-Analysis of Randomized Controlled Trials. Respir. Care 2020, 65, 673–685. [Google Scholar] [CrossRef] [PubMed]
- Bo, L.; Li, J.; Tao, T.; Bai, Y.; Ye, X.; Hotchkiss, R.S.; Kollef, M.H.; Crooks, N.H.; Deng, X. Probiotics for preventing ventilator-associated pneumonia. Cochrane Database Syst. Rev. 2014, 10, CD009066. [Google Scholar] [CrossRef]
- Manzanares, W.; Lemieux, M.; Langlois, P.L.; Wischmeyer, P.E. Probiotic and synbiotic therapy in critical illness: A systematic review and meta-analysis. Crit. Care 2016, 19, 262, Erratum in: Crit. Care 2017, 21, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barraud, D.; Bollaert, P.E.; Gibot, S. Impact of the administration of probiotics on mortality in critically ill adult patients: A meta-analysis of randomized controlled trials. Chest 2013, 143, 646–655. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Zeng, Q.; Li, K.X.; Wang, Y.; Wang, L.; Sun, M.W.; Zeng, J.; Jiang, H. Efficacy of probiotics or synbiotics for critically ill adult patients: A systematic review and meta-analysis of randomized controlled trials. Burn. Trauma. 2022, 10, tkac004. [Google Scholar] [CrossRef]
- Johnstone, J.; Meade, M.; Lauzier, F.; Marshall, J.; Duan, E.; Dionne, J.; Arabi, Y.M.; Heels-Ansdell, D.; Thabane, L.; Lamarche, D.; et al. Effect of Probiotics on Incident Ventilator-Associated Pneumonia in Critically Ill Patients: A Randomized Clinical Trial. JAMA 2021, 326, 1024–1033. [Google Scholar] [CrossRef] [PubMed]
- EFSA BIOHAZ Panel (EFSA Panel on Biological Hazards); Koutsoumanis, K.; Allende, A.; Alvarez-Ordonez, A.; Bolton, D.; Bover-Cid, S.; Chemaly, M.; Davies, R.; De Cesare, A.; Hilbert, F.; et al. Update of the List of QPS-Recommended Biological Agents Intentionally Added to Food or Feed as Notified to EFSA 12: Suitability of Taxonomic Units Notified to EFSA until March 2020. EFSA J. 2020, 18, 6174. [Google Scholar]
- Sotoudegan, F.; Daniali, M.; Hassani, S.; Nikfar, S.; Abdollahi, M. Reappraisal of probiotics’ safety in human. Food Chem. Toxicol. 2019, 129, 22–29. [Google Scholar] [CrossRef]
- Doron, S.; Snydman, D.R. Risk and safety of probiotics. Clin. Infect. Dis. 2015, 60, S129–S134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yelin, I.; Flett, K.B.; Merakou, C.; Mehrotra, P.; Stam, J.; Snesrud, E.; Hinkle, M.; Lesho, E.; McGann, P.; McAdam, A.J.; et al. Genomic and epidemiological evidence of bacterial transmission from probiotic capsule to blood in ICU patients. Nat. Med. 2019, 25, 1728–1732. [Google Scholar] [CrossRef]
- Daniali, M.; Nikfar, S.; Abdollahi, M. Antibiotic resistance propagation through probiotics. Expert Opin. Drug Metab. Toxicol. 2020, 16, 1207–1215. [Google Scholar] [CrossRef] [PubMed]
- Cassir, N.; Benamar, S.; La Scola, B. Clostridium butyricum: From beneficial to a new emerging pathogen. Clin. Microbiol. Infect. 2016, 22, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Hanchi, H.; Mottawea, W.; Sebei, K.; Hammami, R. The Genus Enterococcus: Between Probiotic Potential and Safety Concerns-An Update. Front. Microbiol. 2018, 9, 1791. [Google Scholar] [CrossRef]
- Gatti, M.; Cojutti, P.G.; Bartoletti, M.; Tonetti, T.; Bianchini, A.; Ramirez, S.; Pizzilli, G.; Ambretti, S.; Giannella, M.; Mancini, R.; et al. Expert clinical pharmacological advice may make an antimicrobial TDM program for emerging candidates more clinically useful in tailoring therapy of critically ill patients. Crit. Care 2022, 26, 178. [Google Scholar] [CrossRef]
- Veringa, A.; Sturkenboom, M.G.G.; Dekkers, B.G.J.; Koster, R.A.; Roberts, J.A.; Peloquin, C.A.; Touw, D.J.; Alffenaar, J.-W.C. LC-MS/MS for Therapeutic Drug Monitoring of anti-infective drugs. TrAC-Trends Anal. Chem. 2016, 84, 34–40. [Google Scholar] [CrossRef] [Green Version]
- Ortonobes, S.; Mujal-Martínez, A.; de Castro Julve, M.; González-Sánchez, A.; Jiménez-Pérez, R.; Hernández-Ávila, M.; De Alfonso, N.; Maye-Pérez, I.; Valle-Delmás, T.; Rodríguez-Sánchez, A.; et al. Successful Integration of Clinical Pharmacists in an OPAT Program: A Real-Life Multidisciplinary Circuit. Antibiotics 2022, 11, 1124. [Google Scholar] [CrossRef]
- ntimicrobial Resistance Collaborators; Wozniak, T. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations; HM Government and Wellcome Trust: London, UK, 2016; Review on Antimicrobial Resistance, chaired by Jim O’Neill; Available online: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf (accessed on 29 January 2023).
- Ya, K.; Win, P.T.N.; Bielicki, J.; Lambiris, M.; Fink, G. Association Between Antimicrobial Stewardship Programs and Antibiotic Use Globally: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2023, 6, e2253806. [Google Scholar]
- Mandelli, G.; Dore, F.; Langer, M.; Garbero, E.; Alagna, L.; Bianchin, A.; Ciceri, R.; Di Paolo, A.; Giani, T.; Giugni, A.; et al. Effectiveness of a Multifaced Antibiotic Stewardship Program: A Pre-Post Study in Seven Italian ICUs. J. Clin. Med. 2022, 11, 4409. [Google Scholar] [CrossRef]
- Cogan, R.C.; El-Matary, B.W.; El-Matary, W.M. Therapeutic drug monitoring for biological medications in inflammatory bowel disease. Saudi. J. Gastroenterol. 2022, 28, 322–331. [Google Scholar]
- Aonuma, K.; Shiga, T.; Atarashi, H.; Doki, K.; Echizen, H.; Hagiwara, N.; Hasegawa, J.; Hayashi, H.; Hirao, K.; Ichida, F.; et al. Guidelines for Therapeutic Drug Monitoring of Cardiovascular Drugs Clinical Use of Blood Drug Concentration Monitoring (JCS 2015)?-Digest Version. Circ. J. 2017, 81, 581–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiemke, C.; Bergemann, N.; Clement, H.W.; Conca, A.; Deckert, J.; Domschke, K.; Eckermann, G.; Egberts, K.; Gerlach, M.; Greiner, C.; et al. Consensus Guidelines for Therapeutic Drug Monitoring in Neuropsychopharmacology: Update 2017. Pharmacopsychiatry 2018, 51, 9–62, Erratum in: Pharmacopsychiatry 2018, 51, e1. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control. Antimicrobial consumption (AMC) reporting protocol 2020. In European Surveillance of Antimicrobial Consumption Network (ESAC-Net) Surveillance Data for 2019; ECDC: Stockholm, Sweden, 2020. [Google Scholar]
- Bakker, T.; Abu-Hanna, A.; Dongelmans, D.A.; Vermeijden, W.J.; Bosman, R.J.; de Lange, D.W.; Klopotowska, J.E.; de Keizer, N.F.; SIMPLIFY study group; Hendriks, S.; et al. Clinically relevant potential drug-drug interactions in intensive care patients: A large retrospective observational multicenter study. J. Crit. Care 2021, 62, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Roe, A.L.; Boyte, M.E.; Elkins, C.A.; Goldman, V.S.; Heimbach, J.; Madden, E.; Oketch-Rabah, H.; Sanders, M.E.; Sirois, J.; Smith, A. Considerations for determining safety of probiotics: A USP perspective. Regul. Toxicol. Pharmacol. 2022, 136, 105266. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| PK/PD Relationship | Antibacterial Class | PK, PD Parameters |
|---|---|---|
| Time-dependent | β-lactams, linezolid, lincosamides, macrolides | fT > MIC |
| Concentration-dependent | aminoglycosides, fluoroquinolones, daptomycin | fCmax/MIC |
| Co-dependent (concentration-dependent with time-dependence) | fluoroquinolones, tigecycline, linezolid, glycopeptides, macrolides, colistin | fAUC24/MIC |
| Product | Strain |
|---|---|
| Probiotics | Lactobacillus (e.g., L. acidophilus, L. rhamnosus, L. reuteri, L. bulgaricus, L. plantarum, L. casei, L. lactis, etc.), Bifidobacterium (B. bifidum, B. longum, B. breve, B. infantis, B. lactis, B. thermophilum, etc.), Saccharomyces spp. (S. cerevisiae, S. boulardii), lactic acid bacteria (LAB) including Lactococcus, Lactobacillus, Streptococcus, and Enterococcus or Clostridium spp. cluster IV |
| Prebiotics | galactooligosaccharides (GOS), fructooligosaccharides (FOS), xylooligosaccharides (XOS), isomaltooligosaccharides (IMO), inulin, lactulose, lactosucrose, lactitol |
| Synbiotics | L. rhamnosus + inulin, Lactobacillus + Bifidobacterium + Enterococcus + FOS, Saccharomyces boulardii + Lactobacillus sporogenes + FOS) |
| Paraprobiotics | peptidoglycans, teichoic acid, cell-wall polysaccharides, cell surface-associated proteins, proteinaceous filaments |
| Postbiotics | Exopolysaccharides, short chain fatty acids, enzymes, bacterial lysates, etc. |
| Author | Method | No. Studies/ No. Patients | Results | Conclusion/Limitations |
|---|---|---|---|---|
| Li et al., 2022 [59] | meta-analysis | 31 RCT 8339 patients |
|
|
| Naseri et al., 2022 [60] | umbrella review | 20 RCT |
|
|
| Sun et al., 2022 [61] | meta-analysis | 23 RCT 5543 patients |
|
|
| Weng et al., 2017 [62] | meta-analysis with trial sequential analysis | 13 studies 1969 patients |
|
|
| Cheema et al., 2022 [63] | systematic review and meta-analysis | 18 RCTs 4893 patients |
|
|
| Su et al., 2020 [64] | meta-analysis | 14 studies 1975 patients |
|
|
| Bo et al., 2014 [65] | Cochrane review | 8 RCTs 1083 patients. |
|
|
| Manzanares et al., 2016 [66] | systematic review and meta-analysis | 30 RCT 2972 patients |
|
|
| Barraud et al., 2013 [67] | meta-analysis | 13 trials 1439 patients |
|
|
| Wang et al., 2022 [68] | systematic review and meta-analysis | 25 RCT 5049 patients |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onofrei, M.I.; Ghiciuc, C.M.; Luca, C.M.; Postolache, P.; Sapaniuc, C.; Enache Leonte, G.; Rosu, F.M. Optimization of Therapy and the Risk of Probiotic Use during Antibiotherapy in Septic Critically Ill Patients: A Narrative Review. Medicina 2023, 59, 478. https://doi.org/10.3390/medicina59030478
Onofrei MI, Ghiciuc CM, Luca CM, Postolache P, Sapaniuc C, Enache Leonte G, Rosu FM. Optimization of Therapy and the Risk of Probiotic Use during Antibiotherapy in Septic Critically Ill Patients: A Narrative Review. Medicina. 2023; 59(3):478. https://doi.org/10.3390/medicina59030478
Chicago/Turabian StyleOnofrei, Maria Ioana, Cristina Mihaela Ghiciuc, Catalina Mihaela Luca, Paraschiva Postolache, Cristina Sapaniuc, Georgiana Enache Leonte, and Florin Manuel Rosu. 2023. "Optimization of Therapy and the Risk of Probiotic Use during Antibiotherapy in Septic Critically Ill Patients: A Narrative Review" Medicina 59, no. 3: 478. https://doi.org/10.3390/medicina59030478