
Computer Vision Syndrome: An Ophthalmic Pathology of the Modern Era
 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
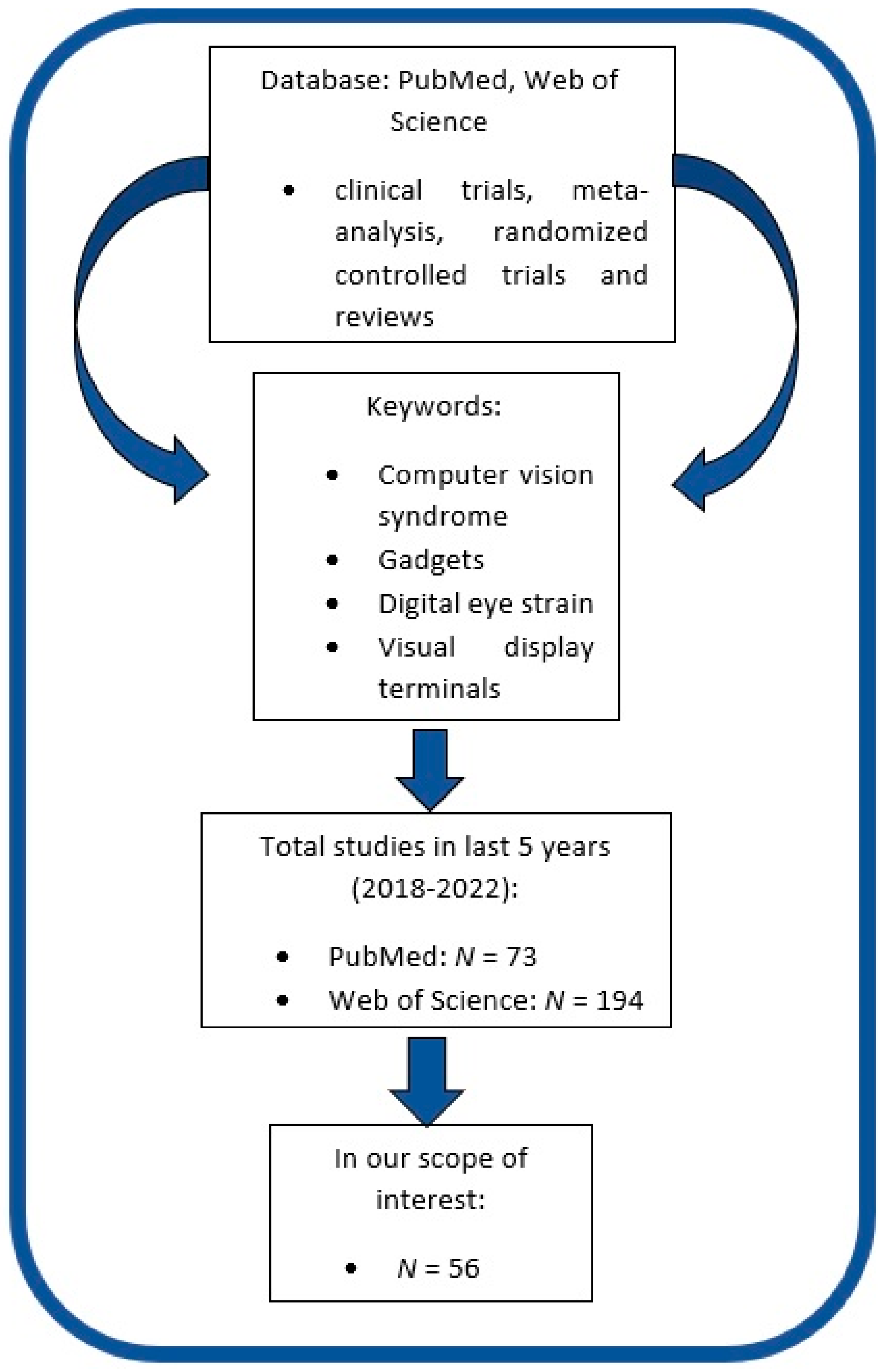
2. Paper Selection
3. Asthenopia, Visual Disturbances, and Intraocular Pressure Modification
3.1. Asthenopia
3.2. Accommodation and Vergence Anomalies and Amblyopia
3.3. Temporary Gadget-Induced Myopia
3.4. Intraocular Pressure Changes Secondary to the Use of Digital Screens
4. Environmental and Work Factors
4.1. Surrounding Light
4.2. Working Hours
4.3. Microenvironment
5. Personal Factors
5.1. Ametropia
5.2. Nicotine Use
6. Device-Related Factors
6.1. Angle of VDT
6.2. Screen Resolution and Text Size
6.3. 3D Stereoscopic Display
7. Ocular Surface Disorder
7.1. Spontaneous Blink Impairment
7.2. Dry Eye Disease and Tear Film Quality Prevention of Digital Screen-Induced Dry Eye
8. Extraocular Symptoms
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bogdănici, C.M.; Săndulache, D.E.; Nechita, C.A. Eyesight quality and Computer Vision Syndrome. Rom. J. Ophthalmol. 2017, 61, 112–116. [Google Scholar] [CrossRef]
- Sheppard, A.L.; Wolffsohn, J.S. Digital eye strain: Prevalence, measurement and amelioration. BMJ Open Ophthalmol. 2018, 3, e000146. [Google Scholar] [CrossRef] [Green Version]
- Rosenfield, M. Computer vision syndrome: A review of ocular causes and potential treatments. Ophthalmic Physiol. Opt. 2011, 31, 502–515. [Google Scholar] [CrossRef]
- Fenga, C.; Di pietro, R.; Di Nola, C.; Spinella, R.; Cacciola, A.; Germano, A.P. Asthenopia in VDT users: Our experience. G. Ital. Med. Lav. Ergon. 2007, 29, 500–501. [Google Scholar] [PubMed]
- Hayes, J.R.; Sheedy, J.E.; Stelmack, J.A.; Heaney, C.A. Computer use, symptoms, and quality of life. Optom. Vis. Sci. 2007, 84, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Rocha, L.E.; Debert-Ribeiro, M. Working conditions, visual fatigue and mental health among systems analysts in Sao Paulo, Brazil. Occup. Environ. Med. 2004, 61, 24–32. [Google Scholar] [PubMed]
- Bhanderi, D.J.; Choudhary, S.; Doshi, V.G. A community-based study of asthenopia in computer operators. Indian J. Ophthalmol. 2008, 56, 51–55. [Google Scholar] [CrossRef]
- Uchino, M.; Yokoi, N.; Uchino, Y.; Dogru, M.; Kawashima, M.; Komuro, A.; Sonomura, Y.; Kato, H.; Kinoshita, S.; Schaumberg, D.A.; et al. Prevalence of dry eye disease and its risk factors in visual display terminal users: The Osaka study. Am. J. Ophthalmol. 2013, 156, 759–766. [Google Scholar] [CrossRef]
- Toomingas, A.; Hagberg, M.; Heiden, M.; Richter, H.; Westergren, K.E.; Tornqvist, E.W. Risk factors, incidence and persistence of symptoms from the eyes among professional computer users. Work 2014, 47, 291–301. [Google Scholar] [CrossRef]
- Cohen, Y.; Segal, O.; Barkana, Y.; Lederman, R.; Zadok, D.; Pras, E.; Morad, Y. Correlation between asthenopic symptoms and different measurements of convergence and reading comprehension and saccadic fixation eye movements. Optometry 2010, 81, 28–34. [Google Scholar] [CrossRef]
- Qu, X.-M.; Chu, R.-Y.; Wang, L.; Yao, P.-J.; Liu, J.-R. Effects of short-term VDT usage on visual functions. Zhonghua Yan Ke Za Zhi 2005, 41, 986–989. [Google Scholar]
- Rosenfield, M.; Gurevich, R.; Wickware, E.; Lay, M. Computer vision syndrome: Accommodative & vergence facility. J. Behav. Optom. 2010, 21, 119–122. [Google Scholar]
- Mohan, A.; Sen, P.; Mujumdar, D.; Shah, C.; Jain, E. Series of cases of acute acquired comitant esotropia in children associated with excessive online classes on smartphone during COVID-19 pandemic; digital eye strain among kids (DESK) study-3. Strabismus 2021, 29, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Neena, R.; Remya, S.; Anantharaman, G. Acute acquired comitant esotropia precipitated by excessive near work during the COVID-19-induced home confinement. Indian J. Ophthalmol. 2022, 70, 1359–1364. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.S.; Park, S.W.; Heo, H. Acute acquired comitant esotropia related to excessive Smartphone use. BMC Ophthalmol. 2016, 16, 37. [Google Scholar] [CrossRef] [Green Version]
- Kaur, S.; Sukhija, J.; Khanna, R.; Takkar, A.; Singh, M. Diplopia after Excessive Smart Phone Usage. Neuroophthalmology 2018, 43, 323–326. [Google Scholar] [CrossRef]
- Bogdanici, S.T.; Martinescu, G.; Sandulache, C.M.; Bogdanici, C.M. Socio-professional Integration for Amblyopic Patients. Rev. De Cercet. Si Interv. Soc. 2016, 52, 187–194. [Google Scholar]
- Liu, S.; Ye, S.; Xi, W.; Zhang, X. Electronic devices and myopic refraction among children aged 6–14 years in urban areas of Tianjin, China. Ophthalmic Physiol. Opt. 2019, 39, 282–293. [Google Scholar] [CrossRef]
- Lee, E.J.; Kim, H. Effect of Smartphone Use on Intraocular Pressure. Sci. Rep. 2019, 11, 18802. [Google Scholar] [CrossRef] [Green Version]
- Ha, A.; Kim, Y.K.; Park, Y.J.; Jeoung, J.W.; Park, K.H. Intraocular pressure change during reading or writing on smartphone. PLoS ONE 2018, 13, e0206061. [Google Scholar] [CrossRef] [Green Version]
- Ha, A.; Kim, Y.K.; Kim, J.-S.; Jeoung, J.W.; Park, K.H. Changes in intraocular pressure during reading or writing on smartphones in patients with normal-tension glaucoma. Br. J. Ophthalmol. 2020, 104, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Parihar, J.K.S.; Jain, V.K.; Chaturvedi, P.; Kaushik, J.; Jain, G.; Parihar, A.K.S. Computer and visual display terminals (VDT) vision syndrome (CVDTS). Med. J. Armed Forces India 2016, 72, 270–276. [Google Scholar] [CrossRef] [Green Version]
- Joines, S.; James, T.; Liu, S.; Wang, W.; Dunn, R.; Cohen, S. Adjustable task lighting: Field study assesses the benefits in an office environment. Work 2015, 51, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Hua, W.; Wu, X.; Jiang, X.; Wan, Y.; Zhang, J.; Jin, J.; Liu, H.; Gao, G.; Fang, Y.; Pei, C.; et al. Association between elevated light levels in classrooms and change in vision acuity among elementary and secondary students. Chin. J. Prev. Med. 2015, 49, 147–151. [Google Scholar]
- Janosik, E.; Grzesik, J. Influence of different lighting levels at workstations with video display terminals on operators’ work efficiency. Med. Pract. 2003, 54, 123–132. [Google Scholar]
- Christensen, M.A.; Bettencourt, L.; Kaye, L.; Moturu, S.T.; Nguyen, K.T.; Olgin, J.E.; Pletcher, M.J.; Marcus, G.M. Direct Measurements of Smartphone Screen-Time: Relationships with Demographics and Sleep. PLoS ONE 2016, 11, e0165331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arshad, D.; Joyia, U.M.; Fatima, S.; Khalid, N.; Rishi, A.I.; Rahim, N.U.A.; Bukhari, S.F.; Shairwani, G.K.; Salmaan, A. The adverse impact of excessive smartphone screen-time on sleep quality among young adults: A prospective cohort. Sleep Sci. 2021, 14, 337–341. [Google Scholar] [CrossRef]
- Patil, A.; Bhavya; Chaudhury, S.; Srivastava, S. Eyeing computer vision syndrome: Awareness, knowledge, and its impact on sleep quality among medical students. Ind. Psychiatry J. 2019, 28, 68–74. [Google Scholar] [CrossRef]
- Grimaldi-Puyana, M.; Fernández-Batanero, J.M.; Fennell, C.; Sañudo, B. Associations of Objectively-Assessed Smartphone Use with Physical Activity, Sedentary Behavior, Mood, and Sleep Quality in Young Adults: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 3499. [Google Scholar] [CrossRef]
- Auffret, E.; Mielcarek, M.; Bourcier, T.; Delhommais, A.; Speeg-Schatz, C.; Sauer, A. Stress oculaire induit par les écrans. Analyses des symptômes fonctionnels et de l’équilibre binoculaire chez des utilisateurs intensifs [Digital eye strain. Functional symptoms and binocular balance analysis in intensive digital users]. J. Fr. Ophtalmol. 2022, 45, 438–445. [Google Scholar] [CrossRef]
- Rossi, G.C.M.; Scudeller, L.; Bettio, F.; Pasinetti, G.M.; Bianchi, P.E. Prevalence of dry eye in video display terminal users: A cross-sectional Caucasian study in Italy. Int. Ophthalmol. 2019, 39, 1315–1322. [Google Scholar] [CrossRef] [PubMed]
- Erdinest, N.; Berkow, D. Computer Vision Syndrome. Harefuah 2021, 160, 386–392. [Google Scholar] [PubMed]
- Wiggins, N.P.; Daum, K.M. Visual discomfort and astigmatic refractive errors in VDT use. J. Am. Optom. Assoc. 1991, 62, 680–684. [Google Scholar] [PubMed]
- Wiggins, N.P.; Daum, K.M.; Snyder, C.A. Effects of residual astigmatism in contact lens wear on visual discomfort in VDT use. J. Am. Optom. Assoc. 1992, 63, 177–181. [Google Scholar] [PubMed]
- Harris, C.; Straker, L. Survey of physical ergonomics issues associated with school childrens’ use of laptop computers. Int. J. Ind. Ergon. 2000, 26, 337–346. [Google Scholar] [CrossRef]
- Makrynioti, D.; Zagoriti, Z.; Koutsojannis, C.; Morgan, P.B.; Lagoumintzis, G. Ocular conditions and dry eye due to traditional and new forms of smoking: A review. Contact Lens Anterior Eye 2020, 43, 277–284. [Google Scholar] [CrossRef]
- Ranasinghe, P.; Wathurapatha, W.S.; Perera, Y.S.; Lamabadusuriya, D.A.; Kulatunga, S.; Jayawardana, N.; Katulanda, P. Computer vision syndrome among computer office workers in a developing country: An evaluation of prevalence and risk factors. BMC Res. Notes 2016, 9, 150. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, M.; Said, O.; Ibrahim, O.; Soliman, A. Visual Sequelae of Computer Vision Syndrome: A Cross-Sectional Case-Control Study. J. Ophthalmol. 2021, 2021, 6630286. [Google Scholar] [CrossRef]
- Kim, D.J.; Lim, C.Y.; Gu, N.; Park, C.Y. Visual Fatigue Induced by Viewing a Tablet Computer with a High-resolution Display. Korean J. Ophthalmol. 2017, 31, 388–393. [Google Scholar] [CrossRef] [Green Version]
- Yum, H.R.; Park, S.H.; Kang, H.-B.; Shin, S.Y. Changes in ocular factors according to depth variation and viewer age after watching a three-dimensional display. Br. J. Ophthalmol. 2014, 98, 684–690. [Google Scholar] [CrossRef]
- Yum, H.R.; Park, S.H.; Kang, H.-B.; Shin, S.Y. Changes in ocular parameters depending on the motion-in-depth of a three-dimensional display. Br. J. Ophthalmol. 2015, 99, 1706–1712. [Google Scholar] [CrossRef] [PubMed]
- Wee, S.W.; Moon, N.J. Clinical evaluation of accommodation and ocular surface stability relevant to visual asthenopia with 3D displays. BMC Ophthalmol. 2014, 14, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tychsen, L.; Foeller, P. Effects of immersive virtual reality headset viewing on young children: Visuomotor function, postural stability, and motion sickness. Am. J. Ophthalmol. 2020, 209, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Munsamy, A.J.; Paruk, H.; Gopichunder, B.; Luggya, A.; Majola, T.; Khulu, S. The effect of gaming on accommodative and vergence facilities after exposure to virtual reality head-mounted display. J. Optom. 2020, 13, 163–170. [Google Scholar] [CrossRef]
- Ciążyńska, J.; Janowski, M.; Maciaszek, J. Effects of a Modern Virtual Reality 3D Head-Mounted Display Exergame on Simulator Sickness and Immersion Under Specific Conditions in Young Women and Men: Experimental Study. JMIR Serious Games 2022, 10, e41234. [Google Scholar] [CrossRef]
- Yin, Z.; Liu, B.; Hao, D.; Yang, L.; Feng, Y. Evaluation of VDT-Induced Visual Fatigue by Automatic Detection of Blink Features. Sensors 2022, 22, 916. [Google Scholar] [CrossRef]
- Li, S.; Hao, D.; Liu, B.; Yin, Z.; Yang, L.; Yu, J. Evaluation of eyestrain with vertical electrooculogram. Comput. Methods Programs Biomed. 2021, 208, 106171. [Google Scholar] [CrossRef]
- Akkaya, S.; Atakan, T.; Acikalin, B.; Aksoy, S.; Ozkurt, Y. Effects of long-term computer use on eye dryness. North. Clin. Istanb. 2018, 5, 319–322. [Google Scholar] [CrossRef]
- Hanyuda, A.; Sawada, N.; Uchino, M.; Kawashima, M.; Yuki, K.; Tsubota, K.; Yamagishi, K.; Iso, H.; Yasuda, N.; Saito, I.; et al. Physical inactivity, prolonged sedentary behaviors, and use of visual display terminals as potential risk factors for dry eye disease: JPHC-NEXT study. Ocul. Surf. 2020, 18, 56–63. [Google Scholar] [CrossRef]
- Wang, M.T.M.; Muntz, A.; Mamidi, B.; Wolffsohn, J.S.; Craig, J.P. Modifiable lifestyle risk factors for dry eye disease. Contact Lens Anterior Eye 2021, 44, 101409. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Wang, M.T.M.; Vidal-Rohr, M.; Menduni, F.; Dhallu, S.; Ipek, T.; Acar, D.; Recchioni, A.; France, A.; Kingsnorth, A.; et al. Demographic and lifestyle risk factors of dry eye disease subtypes: A cross-sectional study. Ocul. Surf. 2021, 21, 58–63. [Google Scholar] [CrossRef]
- Inomata, T.; Iwagami, M.; Nakamura, M.; Shiang, T.; Yoshimura, Y.; Fujimoto, K.; Okumura, Y.; Eguchi, A.; Iwata, N.; Miura, M.; et al. Characteristics and Risk Factors Associated with Diagnosed and Undiagnosed Symptomatic Dry Eye Using a Smartphone Application. JAMA Ophthalmol. 2020, 138, 58–68. [Google Scholar] [CrossRef]
- Moon, J.H.; Lee, M.Y.; Moon, N.J. Association between video display terminal use and dry eye disease in school children. J. Pediatr. Ophthalmol. Strabismus 2014, 51, 87–92. [Google Scholar] [CrossRef]
- Moon, J.H.; Kim, K.W.; Moon, N.J. Smartphone use is a risk factor for pediatric dry eye disease according to region and age: A case control study. BMC Ophthalmol. 2016, 16, 188. [Google Scholar] [CrossRef] [Green Version]
- Talens-Estarelles, C.; Sanchis-Jurado, V.; Esteve-Taboada, J.J.; Pons, Á.M.; García-Lázaro, S. How Do Different Digital Displays Affect the Ocular Surface? Optom. Vis. Sci. 2020, 97, 1070–1079. [Google Scholar] [CrossRef]
- Kim, A.D.; Muntz, A.; Lee, J.; Wang, M.T.M.; Craig, J.P. Therapeutic benefits of blinking exercises in dry eye disease. Contact Lens Anterior Eye 2021, 44, 101329. [Google Scholar] [CrossRef]
- Fujita, H.; Sano, K.; Baba, T.; Tanaka, T.; Ohno-Matsui, K. Blind working time in visual display terminal users. J. Occup. Health 2019, 61, 175–181. [Google Scholar] [CrossRef] [Green Version]
- American Optometric Association. Computer Vision Syndrome. Available online: https://www.aoa.org/healthy-eyes/eye-and-vision-conditions/computer-vision-syndrome?sso=y (accessed on 13 August 2022).
- Wang, M.T.M.; Chan, E.; Ea, L.; Kam, C.; Lu, Y.; Misra, S.L.; Craig, J.P. Randomized Trial of Desktop Humidifier for Dry Eye Relief in Computer Users. Optom. Vis. Sci. 2017, 94, 1052–1057. [Google Scholar] [CrossRef] [PubMed]
- Vaz, F.T.; Henriques, S.P.; Silva, D.S.; Roque, J.; Lopes, A.S.; Mota, M. Digital Asthenopia: Portuguese Group of Ergophthalmology Survey. Acta Med. Port. 2019, 32, 260–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, S.F.; McDermott, K.C.; Burge, W.K.; Ahmed, I.I.K.; Varma, D.K.; Liao, Y.J.; Crandall, A.S.; Khaderi, S.K.R. Visual function, digital behavior and the vision performance index. Clin. Ophthalmol. 2018, 12, 2553–2561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stringham, J.M.; Stringham, N.T.; O’Brien, K.J. Macular Carotenoid Supplementation Improves Visual Performance, Sleep Quality, and Adverse Physical Symptoms in Those with High Screen Time Exposure. Foods 2017, 6, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esaki, Y.; Kitajima, T.; Takeuchi, I.; Tsuboi, S.; Furukawa, O.; Moriwaki, M.; Fujita, K.; Iwata, N. Effect of blue-blocking glasses in major depressive disorder with sleep onset insomnia: A randomized, double-blind, placebo-controlled study. Chronobiol. Int. 2017, 34, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Dhar-Munshi, S.; Amed, S.; Munshi, S. Computer vision syndrome: An update. Br. J. Neurosci. Nurs. 2019, 15, S10–S11. [Google Scholar] [CrossRef]
- OnHealth. Smartphone dangers: Could Your Cell Phone Be Bad for Your Health? Available online: https://www.onhealth.com/content/1/dangers_cell_phone_health (accessed on 15 August 2022).
- Experience Life. Are Smartphones Causing Thumb Tendonitis? Available online: https://experiencelife.com/article/smartphones-thumb-tendonitis (accessed on 15 August 2022).
- Pavel, I.A.; Savu, B.; Chiriac, C.P.; Bogdănici, C.M. Ocular and musculoskeletal changes in the pediatric population using gadgets. Rom. J. Ophthalmol. 2022, 66, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Shantakumari, N.; Eldeeb, R.; Sreedharan, J.; Gopal, K. Computer use and vision-related problems among university students in ajman, United arab emirate. Ann. Med. Health Sci. Res. 2014, 4, 258–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Choi, Y.-H.; Kim, J. Effects of the cervical flexion angle during smartphone use on muscle fatigue and pain in the cervical erector spinae and upper trapezius in normal adults in their 20s. J. Phys. Ther. Sci. 2017, 29, 921–923. [Google Scholar] [CrossRef] [Green Version]
- Turkistani, A.N.; Al-Romaih, A.; Alrayes, M.M.; Al Ojan, A.; Al-Issawi, W. Computer vision syndrome among Saudi population: An evaluation of prevalence and risk factors. J. Fam. Med. Prim. Care 2021, 10, 2313–2318. [Google Scholar] [CrossRef]
- Arumugam, S.; Kumar, K.; Subramani, R.; Kumar, S. Prevalence of computer vision syndrome among information technology professionals working in Chennai. World J. Med. Sci. 2014, 11, 312–314. [Google Scholar]
- Xie, Y.; Szeto, G.; Dai, J. Prevalence and risk factors associated with musculoskeletal complaints among users of mobile handheld devices: A systematic review. Appl. Ergon. 2017, 59, 132–142. [Google Scholar] [CrossRef]
- Werth, A.; Babski-Reeves, K. Effects of portable computing devices on posture, muscle activation levels and efficiency. Appl. Ergon. 2014, 45, 1603–1609. [Google Scholar] [CrossRef]
- Young, J.G.; Trudeau, M.B.; Odell, D.; Marinelli, K.; Dennerlein, J.T. Wrist and shoulder posture and muscle activity during touch-screen tablet use: Effects of usage configuration, tablet type, and interacting hand. Work 2013, 45, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Elghomati, A.; Mackieh, A.; Babaqi, T. Weaknesses of research methodologies on musculoskeletal disorders associated with mobile touch-screen devices. J. Occup. Health 2022, 64, e12337. [Google Scholar] [CrossRef] [PubMed]
- Toosi, K.K.; Hogaboom, N.S.; Oyster, M.L.; Boninger, M.L. Computer keyboarding biomechanics and acute changes in median nerve indicative of carpal tunnel syndrome. Clin. Biomech. 2015, 30, 546–550. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author and Year | Participants and Methods | Key Findings |
|---|---|---|
| Christensen et al., 2016 [26] | Cross-sectional analysis of 653 participants enrolled in a longitudinal cohort study conducted via the Internet, which could be accessed by any interested adult; | Long-term use of VTDs has been shown to be associated with shorter sleep times and lower sleep efficiency; |
| Arshad et al., 2021 [27] | Descriptive cohort study conducted on 280 students at Rawalpindi Medical University for a period of 1 month; | Excessive smartphone use affects sleep quality and has various physical and psychological side effects; |
| Patil et al., 2019 [28] | Questionnaire-based research conducted on 463 medical students; | Prolonged use of digital screens can affect the quality of sleep; |
| Grimaldi et al., 2020 [29] | Study conducted on 306 college students from various universities from Seville; | Young adults’ prolonged exposure to smartphones is significant associated with reduced physical activity, sedentary lifestyle, disturbed mood, and low sleep quality; |
| Auffret et al., 2022 [30] | Cross-sectional, prospective, monocentric pilot study conducted on 52 participants; | Chronic use of screens had a negative influence on binocular balance; |
| Rossi et al., 2019 [31] | Cross-sectional study conducted on 194 subjects; the participants were divided in two groups: VDT workers and control group; | Older participants and those who spend more than 4 h a day using VDTs are at major risk of developing dry eye syndrome; |
| Author and Year | Participants and Methods | Key Findings |
|---|---|---|
| Yum et al., 2014 [40] | A total of 38 participants were included; before and after viewing a 3D screen, the near point of accommodation, near point of convergence and the tear break-up time were analyzed; | Watching a 3D display has negative effects on accommodation, convergence and tear dynamics; |
| Yum et al., 2015 [41] | A total of 30 participants were included; before and after viewing a 3D screen, the near point of accommodation, near point of convergence, and the tear break-up time were analyzed; | Motion-in-depth has an important influence on ocular parameters when a 3D display is watched; |
| Wee et al., 2014 [42] | Conducted on 15 adults without ophthalmological pathology; before and after viewing 3D and 2D screens, accommodative capacity, ocular protection index, and total ocular symptom scores were analyzed; | Impairment of accommodative capacity and stability of the ocular surface may be causative factors of visual asthenopia in participants viewing 3D displays; |
| Tychsen et al., 2020 [43] | Conducted on 50 children; this study aimed to assess the safety of VR 3D headset (Virtual Reality three-dimensional binocular–stereoscopic near-eye display) in young children; | Watching a 3D display can cause subjective symptoms such as asthenopia, motion sickness, fatigue, head or neck pain; |
| Munsamy et al., 2020 [44] | Conducted on 62 participants with ages between 18 and 30 years; the paper investigated the modifications between accommodative and vergence facilities before and after exposure to VR device; | Binocular accommodative and vergence facilities increased after 25 min of VR gaming in emmetropic participants under 30 years of age; |
| Ciążyńska et al., 2022 [45] | Conducted on 45 participants; the study investigated the effects of VR 3D HMD gaming in terms of immersion, simulator sickness, breathing, and heart rates and energy expenditure during two sessions of playing on males and females; | The second game session caused sickness in both groups, more noticeably in women; |
| Author and Year | Participants and Methods | Key Findings |
|---|---|---|
| Hanyuda et al., 2020 [49] | Cross-sectional study which included a total of 102,582 participants aged 40–74 years; | Physical inactivity, prolonged sedentary behaviors, and use of VDT were related to increased susceptibility to DED among middle-aged to older Japanese adults; |
| Wang et al., 2021 [50] | Conducted on 322 participants; a questionnaire regarding lifestyle was administered, and dry eye symptomology, ocular surface characteristics, and tear film quality were evaluated; | Prolonged use of digital screens and reduced caffeine consumption were factors associated with higher chances of dry eye disease; |
| Wolffsohn et al., 2021 [51] | A total of 1125 participants; a demographic and lifestyle questionnaire was administered, and dry eye symptomology, ocular surface characteristics and tear film parameters were evaluated; | Risk factors associated with evaporative type DED were older age, East and South Asian ethnicity, contact lens wear, increased exposure to the digital device screen, higher psychological stress, and poorer health; |
| Inomata et al., 2020 [52] | Cross-sectional study including individuals in Japan who completed a questionnaire; | Extended screen exposure (>8 h per day) was positively associated with symptomatic dry eye; |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavel, I.A.; Bogdanici, C.M.; Donica, V.C.; Anton, N.; Savu, B.; Chiriac, C.P.; Pavel, C.D.; Salavastru, S.C. Computer Vision Syndrome: An Ophthalmic Pathology of the Modern Era. Medicina 2023, 59, 412. https://doi.org/10.3390/medicina59020412
Pavel IA, Bogdanici CM, Donica VC, Anton N, Savu B, Chiriac CP, Pavel CD, Salavastru SC. Computer Vision Syndrome: An Ophthalmic Pathology of the Modern Era. Medicina. 2023; 59(2):412. https://doi.org/10.3390/medicina59020412
Chicago/Turabian StylePavel, Irina Andreea, Camelia Margareta Bogdanici, Vlad Constantin Donica, Nicoleta Anton, Bogdan Savu, Cristina Petronela Chiriac, Cristian Dan Pavel, and Silvia Cristina Salavastru. 2023. "Computer Vision Syndrome: An Ophthalmic Pathology of the Modern Era" Medicina 59, no. 2: 412. https://doi.org/10.3390/medicina59020412