
Intraoperative Blood Loss at Different Surgical-Procedure Stages during Posterior Spinal Fusion for Idiopathic Scoliosis
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Data Collection
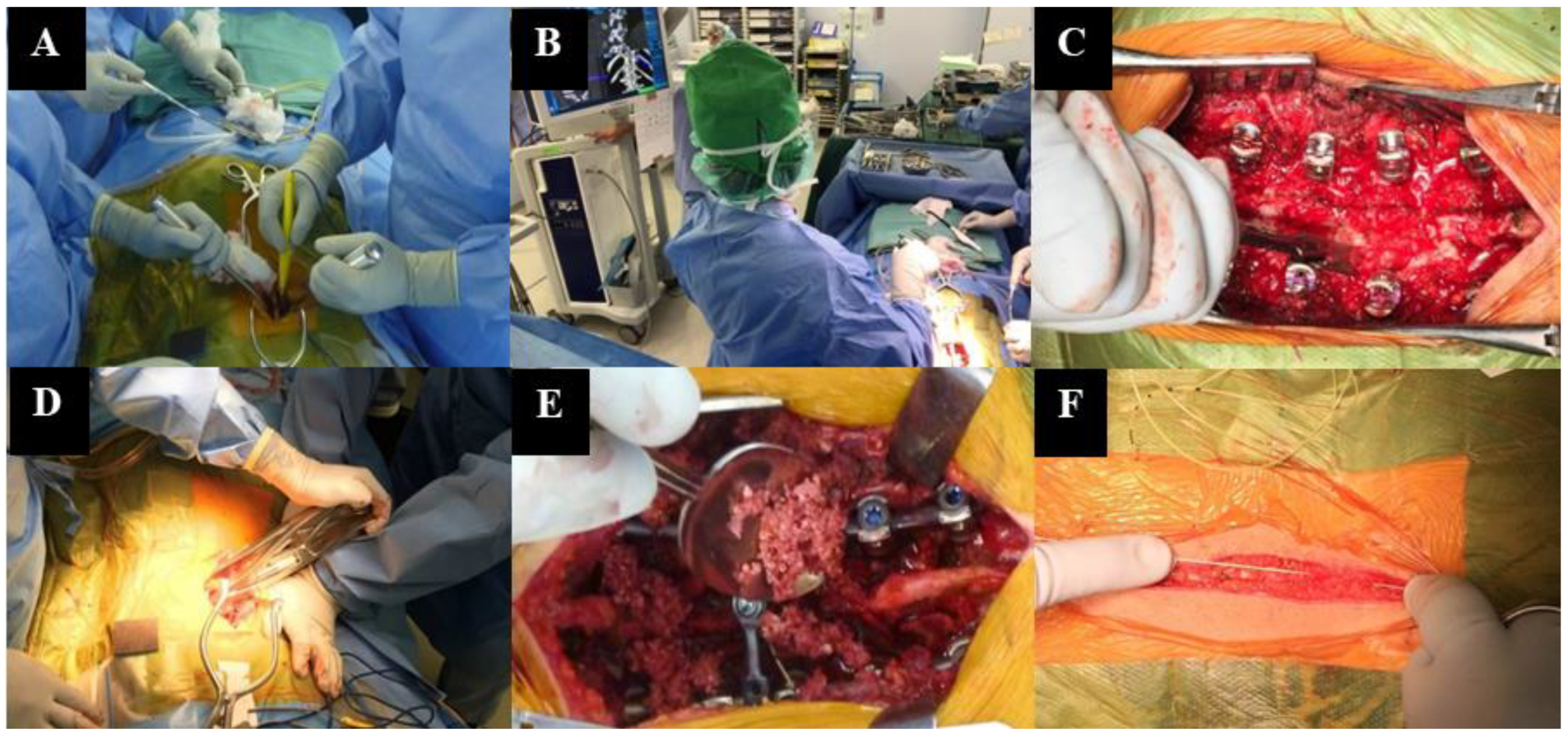
2.2. Surgical Procedure
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aiboshi, J.; Moore, E.E.; Ciesla, D.J.; Silliman, C.C. Blood transfusion and the two-insult model of post-injury multiple organ failure. Shock 2001, 15, 302–306. [Google Scholar] [CrossRef] [PubMed]
- Carreon, L.Y.; Puno, R.M.; Lenke, L.G.; Richards, B.S.; Sucato, D.J.; Emans, J.B.; Erickson, M.A. Non-neurologic complications following surgery for adolescent idiopathic scoliosis. J. Bone Jt. Surg. Am. 2007, 89, 2427–2432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, J.W.; Murray, D.J.; Snider, R.J.; Bassett, G.S.; Bridwell, K.H.; Lenke, L.G. Aprotinin reduces blood loss during spinal surgery in children. Spine 2003, 28, 2482–2485. [Google Scholar] [CrossRef] [PubMed]
- Dodd, R.Y. Current risk for transfusion transmitted infections. Curr. Opin. Hematol. 2007, 14, 671–676. [Google Scholar] [CrossRef] [PubMed]
- Kuklo, T.R.; Owens, B.D.; Polly, D.W., Jr. Perioperative blood and blood product management for spinal deformity surgery. Spine J. 2003, 3, 388–393. [Google Scholar] [CrossRef]
- Ridgeway, S.; Tai, C.; Alton, P.; Barnardo, P.; Harrison, D.J. Pre-donated autologous blood transfusion in scoliosis surgery. J. Bone Jt. Surg. Br. 2003, 85, 1032–1036. [Google Scholar] [CrossRef] [Green Version]
- Hassan, N.; Halanski, M.; Wincek, J.; Reischman, D.; Sanfilippo, D.; Rajasekaran, S.; Wells, C.; Tabert, D.; Kurt, B.; Mitchell, D.; et al. Blood management in pediatric spinal deformity surgery: Review of a 2-year experience. Transfusion 2011, 51, 2133–2141. [Google Scholar] [CrossRef]
- Ialenti, M.N.; Lonner, B.S.; Verma, K.; Dean, L.; Valdevit, A.; Errico, T. Predicting operative blood loss during spinal fusion for adolescent idiopathic scoliosis. J. Pediatr. Orthop. 2013, 33, 372–376. [Google Scholar] [CrossRef]
- Li, C.; Yang, M.; Wang, C.; Wang, C.; Fan, J.; Chen, Z.; Wei, X.; Zhang, G.; Bai, Y.; Zhu, X.; et al. Preoperative factors predicting intraoperative blood loss in female patients with adolescent idiopathic scoliosis. Medicine 2015, 94, e359. [Google Scholar] [CrossRef]
- Shah, S.A.; Ramirez-Garnica, G.; Ye, G.; Stanton, R.P.; Celerin, L. What factors are important in determining intraoperative blood loss during scoliosis surgery? In Proceedings of the Annual Meeting of the American Academy of Orthopaedic Surgeons, Las Vegas, NV, USA, 25–27 February 2009. [Google Scholar]
- Yu, X.; Xiao, H.; Wang, R.; Huang, Y. Prediction of massive blood loss in scoliosis surgery from preoperative variables. Spine 2013, 38, 350–355. [Google Scholar] [CrossRef]
- Duramaz, A.; Bilgili, M.G.; Bayram, B.; Ziroglu, N.; Edipoglu, E.; Ones, H.N.; Kural, C.; Avkan, M.C. The role of intraoperative cell salvage system on blood management in major orthopedic surgeries: A cost-benefit analysis. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Nadler, S.B.; Hidalgo, J.H.; Bloch, T. Prediction of blood volume in normal human adults. Surgery 1962, 51, 224–232. [Google Scholar] [PubMed]
- Chiu, C.K.; Chan, C.Y.; Aziz, I.; Hasan, M.S.; Kwan, M.K. Assessment of Intraoperative Blood Loss at Different Surgical Stages During Posterior Spinal Fusion Surgery in the Treatment of Adolescent Idiopathic Scoliosis. Spine 2016, 41, E566–E573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modi, H.N.; Suh, S.W.; Hong, J.Y.; Song, S.H.; Yang, J.H. Intraoperative blood loss during different stages of scoliosis surgery: A prospective study. Scoliosis 2010, 5, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helenius, I.; Keskinen, H.; Syvanen, J.; Lukkarinen, H.; Mattila, M.; Valipakka, J.; Pajulo, O. Gelatine matrix with human thrombin decreases blood loss in adolescents undergoing posterior spinal fusion for idiopathic scoliosis: A multicentre, randomised clinical trial. Bone Jt. J. 2016, 98-B, 395–401. [Google Scholar] [CrossRef] [Green Version]
- Alamanda, V.K.; Massengill, D.L.; Rozario, N.; Moore, C.G.; Scannell, B.; Brighton, B.; Vanderhave, K.L. Blood Loss Trends and Financial Implications in Adolescent Idiopathic Scoliosis. Clin. Spine Surg. 2018, 31, E418–E421. [Google Scholar] [CrossRef]
- Nugent, M.; Tarrant, R.C.; Queally, J.M.; Sheeran, P.; Moore, D.P.; Kiely, P.J. Influence of curve magnitude and other variables on operative time, blood loss and transfusion requirements in adolescent idiopathic scoliosis. Ir. J. Basic Med. Sci. 2016, 185, 513–520. [Google Scholar] [CrossRef]
- Meert, K.L.; Kannan, S.; Mooney, J.F. Predictors of red cell transfusion in children and adolescents undergoing spinal fusion surgery. Spine 2002, 27, 2137–2142. [Google Scholar] [CrossRef]
- Abousamra, O.; Sponseller, P.D.; Lonner, B.S.; Shah, S.A.; Marks, M.C.; Cahill, P.J.; Pahys, J.M.; Newton, P.O.; Harms Study, G. Thoracic Lordosis, Especially in Males, Increases Blood Loss in Adolescent Idiopathic Scoliosis. J. Pediatr. Orthop. 2019, 39, e201–e204. [Google Scholar] [CrossRef]
- Yoshihara, H.; Yoneoka, D. Predictors of allogeneic blood transfusion in spinal fusion for pediatric patients with idiopathic scoliosis in the United States, 2004–2009. Spine 2014, 39, 1860–1867. [Google Scholar] [CrossRef]
- Goobie, S.M.; Zurakowski, D.; Glotzbecker, M.P.; McCann, M.E.; Hedequist, D.; Brustowicz, R.M.; Sethna, N.F.; Karlin, L.I.; Emans, J.B.; Hresko, M.T. Tranexamic Acid Is Efficacious at Decreasing the Rate of Blood Loss in Adolescent Scoliosis Surgery: A Randomized Placebo-Controlled Trial. J. Bone Jt. Surg. Am. 2018, 100, 2024–2032. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.H.; Bhandarkar, A.W.; Suh, S.W.; Hong, J.Y.; Hwang, J.H.; Ham, C.H. Evaluation of accuracy of plain radiography in determining the Risser stage and identification of common sources of errors. J. Orthop. Surg. Res. 2014, 9, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| n = 45 | ||
|---|---|---|
| Sex | Male (n = 7); Female (n = 38) | |
| Age (SD), years | 17.6 (5.0) | |
| Height (SD), m | 1.6 (0.1) | |
| Weight (SD), kg | 47.7 (7.6) | |
| BMI (SD), kg/m2 | 19.0 (2.5) | |
| Hb (SD), g/dL | 13.7 (1.6) | |
| Plt (SD), ×104/μL | 26.2 (5.2) | |
| PT (SD), s | 12.6 (0.9) | |
| aPTT (SD), s | 32.7 (8.9) | |
| Fib (SD), mg/dL | 251 (44.4) | |
| Preoperative Cobb angle (SD), ° | 55.3 (11.5) | |
| Preoperative thoracic kyphosis (SD), ° | 21.1 (10.4) | |
| Lenke type, number of patients | 1 | 22 |
| 2 | 5 | |
| 3 | 2 | |
| 4 | 1 | |
| 5 | 11 | |
| 6 | 4 | |
| Main Curve Flexibility (SD), % | 43.9 (20.4) | |
| Number of fused vertebrae | 9.7 (3.1) |
| Postoperative Cobb angle (SD), ° | 15.9 (8.6) |
| Correction rate (SD), % | 72.2 (12.1) |
| Operative time (SD), min | 287.9 (68.2) |
| Total blood loss (SD), mL | 756.5 (504.7) |
| Unstandardized | Standardized | t | Significance p | ||
|---|---|---|---|---|---|
| B | SE | β | |||
| Intercept | −1167.3 | 314.2 | |||
| aPTT | 15.2 | 6.0 | 0.3 | 2.5 | 0.02 * |
| Preoperative Cobb angle | 13.4 | 5.6 | 0.3 | 2.4 | 0.02 * |
| Fused vertebrae | 70.9 | 21.2 | 0.4 | 3.3 | <0.01 * |
| Unstandardized | Standardized | t | Significance p | ||
| B | SE | β | |||
| Intercept | −968.3 | 293.5 | |||
| A aPTT | 12.2 | 5.6 | 0.2 | 2.2 | 0.04 * |
| Preoperative Cobb angle | 10.8 | 5.2 | 0.2 | 2.1 | 0.04 * |
| Fused vertebrae | 54.2 | 20.1 | 0.3 | 2.7 | 0.01 * |
| Blood loss during exposure stage | 1.6 | 0.5 | 0.3 | 3.1 | <0.01 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shirasawa, E.; Saito, W.; Miyagi, M.; Imura, T.; Nakazawa, T.; Mimura, Y.; Yokozeki, Y.; Kuroda, A.; Kawakubo, A.; Uchida, K.; et al. Intraoperative Blood Loss at Different Surgical-Procedure Stages during Posterior Spinal Fusion for Idiopathic Scoliosis. Medicina 2023, 59, 387. https://doi.org/10.3390/medicina59020387
Shirasawa E, Saito W, Miyagi M, Imura T, Nakazawa T, Mimura Y, Yokozeki Y, Kuroda A, Kawakubo A, Uchida K, et al. Intraoperative Blood Loss at Different Surgical-Procedure Stages during Posterior Spinal Fusion for Idiopathic Scoliosis. Medicina. 2023; 59(2):387. https://doi.org/10.3390/medicina59020387
Chicago/Turabian StyleShirasawa, Eiki, Wataru Saito, Masayuki Miyagi, Takayuki Imura, Toshiyuki Nakazawa, Yusuke Mimura, Yuji Yokozeki, Akiyoshi Kuroda, Ayumu Kawakubo, Kentaro Uchida, and et al. 2023. "Intraoperative Blood Loss at Different Surgical-Procedure Stages during Posterior Spinal Fusion for Idiopathic Scoliosis" Medicina 59, no. 2: 387. https://doi.org/10.3390/medicina59020387