
Significant Association between Subclinical Left Cardiac Dysfunction and Liver Stiffness in Metabolic Syndrome Patients with Diabetes Mellitus and Non-Alcoholic Fatty Liver Disease
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Vibration Controlled Transient Elastography (VCTE) and Controlled Attenuation Parameter (CAP) Determinations
2.1.1. Ethics
2.1.2. Statistical Analysis
2.1.3. Reproducibility
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef]
- Guembe, M.J.; Fernandez-Lazaro, C.I.; Sayon-Orea, C.; Sayon-Orea, C.; Toledo, E.; Moreno-Iribas, C. Risk for cardiovascular disease associated with metabolic syndrome and its components: A 13-year prospective study in the RIVANA cohort. Cardiovasc. Diabetol. 2020, 19, 195–204. [Google Scholar] [CrossRef]
- Kazlauskiene, L.; Butnoriene, J.; Norkus, A. Metabolic syndrome related to cardiovascular events in a 10-year prospective study. Diabetol. Metab. Syndr. 2015, 7, 102–109. [Google Scholar] [CrossRef]
- Simonova, G.I.; Mustafina, S.V.; Rymar, O.D.; Scherbacova, L.V.; Nikitenko, T.I.; Bobak, M.; Malyutina, S.K. Metabolic syndrome and the risk of cardiovascular and all-cause mortality: Data of 14-year prospective cohort study in Siberia. Russ. J. Cardiol. 2020, 25, 3821–3835. [Google Scholar] [CrossRef]
- Von Bibra, H.; St John Sutton, M. Diastolic dysfunction in diabetes and the metabolic syndrome: Promising potential for diagnosis and prognosis. Diabetologia 2010, 53, 1033–1045. [Google Scholar] [CrossRef]
- Purwowiyoto, S.L.; Prawara, A.S. Metabolic syndrome and heart failure: Mechanism and management. Med. Pharm. Rep. 2021, 9, 15–21. [Google Scholar] [CrossRef]
- Voigt, J.U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/industry task force to standardize tion imaging. J. Am. Soc. Echocardiogr. 2015, 28, 183–193. [Google Scholar] [CrossRef]
- Tan, Y.; Zhang, Z.; Zheng, C.; Wintergerst, K.A.; Keller, B.B.; Cai, L. Mechanisms of diabetic cardiomyopathy and potential therapeutic strategies: Preclinical and clinical evidence. Nat. Rev. Cardiol. 2020, 17, 585–607. [Google Scholar] [CrossRef]
- Tadic, M.; Ilic, S.; Cuspidi, C.; Stojcevski, B.; Ivanovic, B.; Bukarica, L.; Jozika, L.; Celic, V. Left ventricular mechanics in untreated normotensive patients with type 2 diabetes mellitus: A two- and three-dimensional speckle tracking study. Echocardiography 2015, 32, 947–955. [Google Scholar] [CrossRef]
- Saraiva, R.M.; Demirkol, S.; Buakhamsri, A.; Greenberg, N.; Popovic, Z.B.; Thomas, J.D.; Klein, A.L. Left atrial strain measured by two-dimensional speckle tracking represents a new tool to evaluate left atrial function. J. Am. Soc. Echocardiogr. 2010, 23, 172–180. [Google Scholar] [CrossRef]
- Gong, H.P.H.; Tan, H.W.; Fang, N.-N.; Song, T.; Li, S.-H.; Zhong, M.; Zhang, W.; Zhang, Y. Impaired left ventricular systolic and diastolic function in patients with metabolic syndrome as assessed by strain and strain rate imaging. Diabetes Res. Clin. Pr. 2009, 83, 300–307. [Google Scholar] [CrossRef]
- Hwang, J.W.; Kang, S.J.; Lim, H.S.; Choi, B.-J.; Choi, S.-Y.; Hwang, G.-S.; Yoon, M.-H.; Shin, J.-H.; Tahk, S.-J. Impact of arterial stiffness on regional myocardial function assessed by speckle tracking echocardiography in patients with hypertension. J. Cardiovasc. Ultrasound. 2012, 20, 90–96. [Google Scholar] [CrossRef]
- Younossi, Z.; Koenig, A.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Peak epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef]
- Duell, P.B.; Welty, F.K.; Miller, M.; Chait, A.; Hammond, G.; Ahmad, Z.; Cohen, D.E.; Horton, J.D.; Pressman, G.S.; Toth, P.P.; et al. Nonalcoholic Fatty Liver Disease and Cardiovascular Risk: A Scientific Statement From the American Heart Association. Arterioscler. Thromb. Vasc. Biol. 2022, 42, e168–e185. [Google Scholar] [CrossRef]
- Azzam, H.; Malnick, S. Non-alcoholic fatty liver disease—The heart of the matter. World J. Hepatol. 2015, 7, 1369–1376. [Google Scholar] [CrossRef]
- Pieske, B.; Tschöpe, C.; De Boer, R.A.; Frase, A.G.; Anker, S.D.; Donal, E.; Edelmann, F.; Fu, M.; Guazzi, M.; Lam, C.; et al. How to diagnose heart failure with preserved ejection fraction: The HFA–PEFF diagnostic algorithm: A consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2020, 22, 391–412. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A consensus statement from the international diabetes federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.F.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heat J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- EASL-ALEH. Clinical practice guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. J. Hepatol. 2015, 63, 237–264. [Google Scholar] [CrossRef]
- Eddowes, P.J.; Sasso, M.; Allison, M.; Tsochatzis, E.; Anstee, Q.M.; Sheridan, D.; Guha, I.N.; Cobbold, J.F.; Deeks, J.J.; Paradis, V.; et al. Accuracy of FibroScan Controlled Attenuation Parameter and Liver Stiffness Measurement in Assessing Steatosis and Fibrosis in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 56, 1717–1730. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Bamber, J.; Berzigotti, A.; Bota, S.; Cantisani, V.; Castera, L.; Cosgrove, D.; Ferraioli, G.; Friedrich-Rust, M.; Gilja, O.H.; et al. EFSUMB guidelines and recommendations on the clinical use of liver ultrasound elastography, update 2017 (long version). Eur. J. Ultrasound 2017, 38, e16–e47. [Google Scholar]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- Fabiani, I.; Pugliese, N.R.; Santini, V.; Lorenzo Conte, L.; Bello, V.D. Speckle-Tracking Imaging, Principles and Clinical Applications: A Review for Clinical Cardiologists. In Echocardiography in Heart Failure and Cardiac Electrophysiology; Lakshmanadoss, U., Ed.; IntechOpen: London, UK, 2016; Available online: https://www.intechopen.com/chapters/51931 (accessed on 10 January 2023).
- Cottrell, C.; Kirkpatrick, J.N. Echocardiographic strain imaging and its use in the clinical setting. Expert Rev. Cardiovasc. Ther. 2010, 8, 93–102. [Google Scholar] [CrossRef]
- Brecht, A.; Oertelt-Prigione, S.; Seeland, U.; Rücke, M.; Hättasch, R.; Wagelöhner, T.; Regitz-Zagrosek, V.; Baumann, G.; Knebel, F.; Stangl, V. Left atrial function in preclinical diastolic dysfunction: Two-dimensional speckle tracking echocardiography-derived results from the BEFRI trial. J. Am. Soc. Echocardiogr. 2016, 29, 750–758. [Google Scholar] [CrossRef]
- Miljković, T.; Ilić, A.; Milovančev, A.; Bjelobrk, M.; Stefanović, M.; Stojšić-Milosavljević, A.; Tadić, S.; Golubović, M.; Popov, T.; Petrović, M. Left Atrial Strain as a Predictor of Left Ventricular Diastolic Dysfunction in Patients with Arterial Hypertension. Medicina 2022, 58, 156. [Google Scholar] [CrossRef]
- Potter, E.; Marwick, T.H. Assessment of Left Ventricular Function by Echocardiography: The Case for Routinely Adding Global Longitudinal Strain to Ejection Fraction. JACC Cardiovasc. Imaging 2018, 11, 260–274. [Google Scholar] [CrossRef]
- Pathan, F.; D’Elia, N.; Nolan, M.T.; Marwick, T.H.; Negishi, K. Normal Ranges of Left Atrial Strain by Speckle-Tracking Echocardiography: A Systematic Review and Meta-Analysis. J. Am. Soc. Echocardiogr. 2017, 30, 59–70.e8. [Google Scholar] [CrossRef]
- Parvanescu, T.; Vitel, A.; Sporea, I.; Mare, R.; Buz, B.; Bordejevic, D.A.; Tomescu, M.C.; Arnautu, S.F.; Morariu, V.I.; Citu, I.M. Significant Association between Left Ventricular Diastolic Dysfunction, Left Atrial Performance and Liver Stiffness in Patients with Metabolic Syndrome and Non-Alcoholic Fatty Liver Disease. Diabetes Metab. Syndr. Obes. 2021, 14, 1535–1545. [Google Scholar] [CrossRef]
- Kosmalski, M.; Ziółkowska, S.; Czarny, P.; Szemraj, J.; Pietras, T. The Coexistence of Nonalcoholic Fatty Liver Disease and Type 2 Diabetes Mellitus. J. Clin. Med. 2022, 11, 1375. [Google Scholar] [CrossRef]
- Fotbolcu, H.; Yakar, T.; Duman, D.; Karaahmet, T.; Tigen, K.; Cevik, C.; Kurtoglu, U.; Dindar, I. Impairment of the left ventricular systolic and diastolic function in patients with non-alcoholic fatty liver disease. Cardiol. J. 2010, 17, 457–463. [Google Scholar]
- Muranaka, A.; Yuda, S.; Tsuchihashi, K.; Hashimoto, A.; Nakata, T.; Miura, T.; Tsuzuki, M.; Wakabayashi, C.; Watanabe, N.; Shimamoto, K. Quantitative assessment of left ventricular and left atrial functions by strain rate imaging in diabetic patients with and without hypertension. Echocardiography 2009, 26, 262–271. [Google Scholar] [CrossRef]
- Vitel, A.; Sporea, I.; Mare, R.; Banciu, C.; Bordejevic, D.A.; Parvanescu, T.; Citu, I.M.; Tomescu, M.C. Association between Subclinical Left Ventricular Myocardial Systolic Dysfunction Detected by Strain and Strain-Rate Imaging and Liver Steatosis and Fibrosis Detected by Elastography and Controlled Attenuation Parameter in Patients with Metabolic Syndrome. Diabetes Metab. Syndr. Obes. 2020, 13, 3749–3759. [Google Scholar] [CrossRef]
- Li, S.; Wang, J.; Zhang, B.; Li, X.; Liu, Y. Diabetes Mellitus and Cause-Specific Mortality: A Population-Based Study. Diabetes Metab. J. 2019, 43, 319–341. [Google Scholar] [CrossRef]
- Tanaka, H.; Tatsumi, K.; Matsuzoe, H.; Matsumoto, K.; Hirata, K.-I. Impact of diabetes mellitus on left ventricular longitudinal function of patients with non-ischemic dilated cardiomyopathy. Cardiovasc. Diabetol. 2020, 19, 84–94. [Google Scholar] [CrossRef]
- Targher, G.; Byrne, C.D.; Tilg, H. NAFLD and increased risk of cardiovascular disease: Clinical associations, pathophysiological mechanisms and pharmacological implications. Gut 2020, 69, 1691–1705. [Google Scholar] [CrossRef]
- Zhu, L.; Wang, Y.; Zhao, S.; Lu, M. Detection of myocardial fibrosis. Where we stand. Front. Cardiovasc. Med. 2022, 9, 1–13. [Google Scholar] [CrossRef]
- Hallsworth, K.; Hollingsworth, K.G.; Thoma, C.; Jakovljevic, D.; MacGowan, G.A.; Anstee, Q.M.; Taylor, R.; Day, C.P.; Trenell, M.I. Cardiac structure and function are altered in adults with non-alcoholic fatty liver disease. J. Hepatol. 2013, 58, 757–762. [Google Scholar] [CrossRef]
- Sporea, I.; Mare, R.; Popescu, A.; Nistorescu, S.; Baldea, V.; Sirli, R.; Braha, A.; Sima, A.; Timar, R.; Lupusoru, R. Screening for Liver Fibrosis and Steatosis in a Large Cohort of Patients with Type 2 Diabetes Using Vibration Controlled Transient Elastography and Controlled Attenuation Parameter in a Single-Center Real-Life Experience. J. Clin. Med. 2020, 9, 1032. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| With DM (n = 72) | Without DM (n = 78) | p Value | |
|---|---|---|---|
| Age (years) | 62.8 ± 8.7 | 60.2 ± 10.7 | 0.31 |
| Male sex n (%) | 38 (53) | 44 (56) | 0.71 |
| Systemic hypertension (n, %) | 62 (80%) | 58 (84%) | 0.52 |
| Smoking (current, %) | 7 (9%) | 8 (10%) | 0.83 |
| Systolic BP (mmHg) | 142.9 ± 15 | 140.1 ± 19 | 0.32 |
| Diastolic BP (mmHg) | 85.4 ± 11 | 83.7 ± 11 | 0.34 |
| Heart rate (beats/min) | 77.4 ± 11.3 | 73.9 ± 11.1 | 0.05 |
| BMI (kg/m2) | 33.6 ± 5.3 | 32.0 ± 4.8 | 0.05 |
| Waist circumference (cm) | 114 ± 12 | 110 ± 13 | 0.05 |
| Total cholesterol (mg/dL) | 174 ± 40 | 183 ± 62 | 0.24 |
| HDL (mg/dL) | 44.4 ± 13.7 | 45.7 ± 11.8 | 0.53 |
| LDL (mg/dL) | 129.4 ± 31 | 130.5 ± 30 | 0.82 |
| Triglyceride (mgl/dL) | 172.7 ± 109 | 134.4 ± 80.4 | 0.01 |
| FPG (mg/dL) | 153 ± 50 | 108 ± 11 | <0.0001 |
| HbA1c (%) | 7.1 ± 0.9 | 5.2 ± 0.7 | <0.0001 |
| ASAT (U/L) | 24 ± 9 | 23 ± 5 | 0.39 |
| ALAT (U/L) | 37 ± 7 | 36 ± 5 | 0.31 |
| NT-proBNP (pg/mL) | 144 ± 66 | 129 ± 65 | 0.16 |
| Number of MetS components | 3.9 ± 0.8 | 3.7 ± 0.6 | 0.08 |
| Number of components ≥ 4 | 39 (54%) | 34 (44%) | 0.22 |
| Duration of diabetes (years) | 6.5 ± 4 | - | - |
| Diabetes treatment Oral antidiabetics Insulin | 51 (70%) 18 (25%) | - | - |
| Statins | 49 (68%) | 57 (73%) | 0.50 |
| Fibrates | 21 (29%) | 17 (21%) | 0.25 |
| ACEI/ARB | 35 (49%) | 43 (55%) | 0.46 |
| Beta-blockers | 55 (76%) | 58 (74%) | 0.77 |
| Calcium antagonists | 40 (56%) | 43 (55%) | 0.90 |
| Diuretics | 52 (72%) | 55 (70%) | 0.79 |
| With DM (n = 72) | Without DM (n = 78) | p Value | |
|---|---|---|---|
| CAP, dB/m | 292.42 ± 43.6 | 299.36 ± 60.7 | <0.0001 |
| Steatosis stage | |||
| S0 | 0 (0%) | 0 (0%) | 1 |
| S1 | 8 (11%) | 37 (47%) | <0.0001 |
| S2 | 25 (35%) | 14 (18%) | <0.02 |
| S3 | 39 (54%) | 27 (35%) | <0.02 |
| LSM, kPa | 11.53 ± 5.94 | 8.00 ± 3.58 | <0.0001 |
| Fibrosis stage | |||
| F0-1 | 27 (38%) | 57 (73%) | <0.0001 |
| F2 | 28 (39%) | 17 (22%) | 0.02 |
| F3 | 15 (21%) | 3 (4%) | 0.001 |
| F4 | 2 (2%) | 1 (1%) | 0.61 |
| With DM (n = 72) | Without DM (n = 78) | p Value | |
|---|---|---|---|
| Traditional echocardiography | |||
| LV End DD (mm) | 49.14 ± 3.22 | 48.73 ± 2.97 | 0.41 |
| LV End SD (mm) | 30.37 ± 2.54 | 29.87 ± 2.72 | 0.24 |
| LA diameter (mm) | 3.14 ± 0.33 | 3.24 ± 0.35 | 0.07 |
| LVEF (%) | 51.5 ± 0.6 | 51.6 ± 0.5 | 0.26 |
| LVFS (%) | 37.99 ± 2.93 | 38.10 ± 3.55 | 0.83 |
| LV diastolic dysfunction (n, %) | 38 (52%) | 28 (36%) | 0.04 |
| LA volumes (mL) | |||
| Maxim | 27.4 ± 5.3 | 26.9 ± 5.5 | 0.57 |
| Minim | 11.55 ± 4.0 | 12.56 ± 3.7 | 0.11 |
| LA ejection fraction (%) | 56.2 ± 4.2 | 56.9 ± 3.8 | 0.28 |
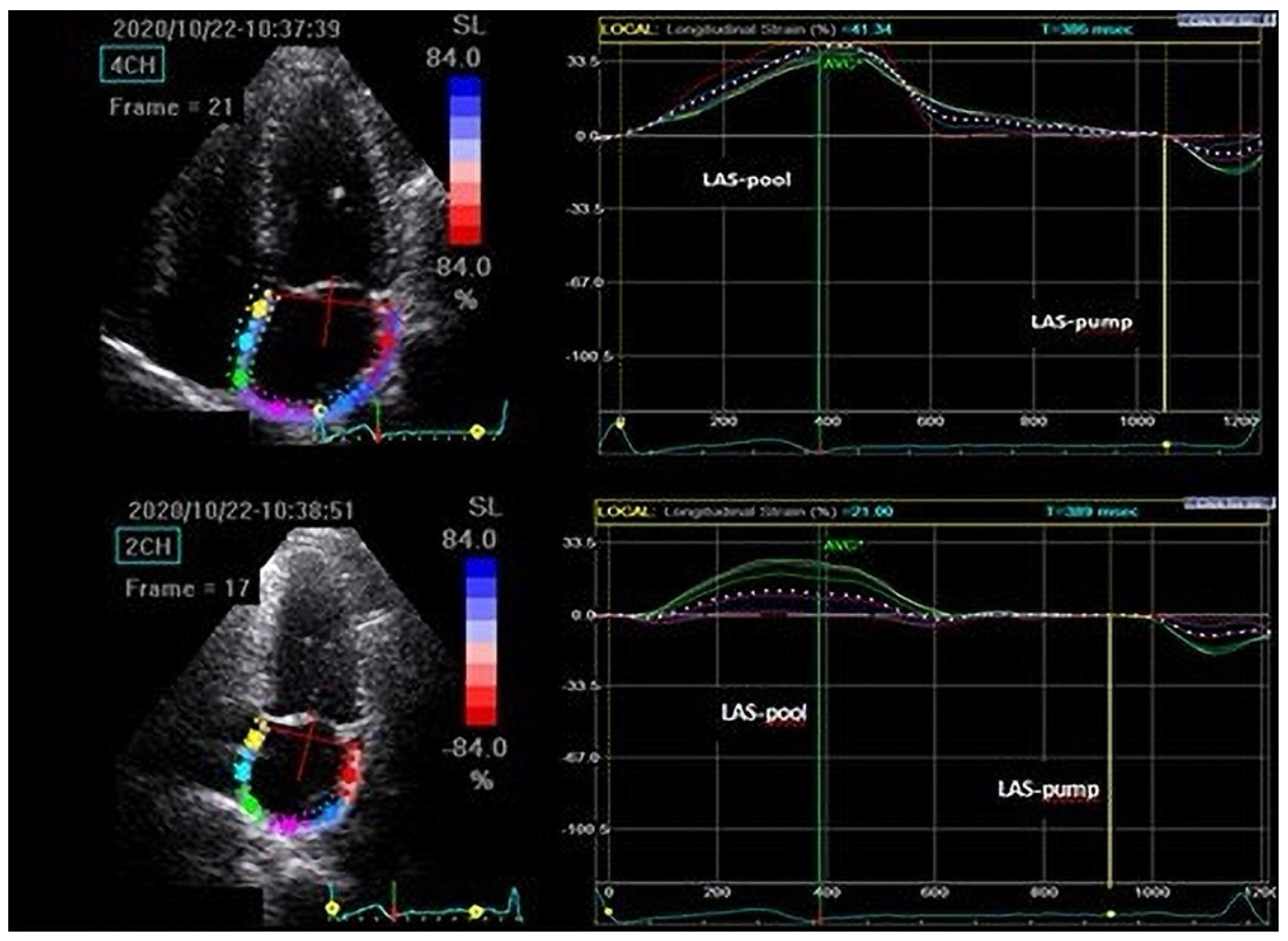
| 2D-STE | |||
| LAS-pool (%) | 43.9 ± 4.3 | 45.4 ± 3.7 | 0.02 |
| LAS-pump (%) | 17.4 ± 2.2 | 18.3 ± 1.8 | <0.01 |
| LA stiffness | 0.34 ± 0.12 | 0.28 ± 0.15 | <0.01 |
| LAsf ≥ 0.38 | 29 (40%) | 19 (24%) | 0.03 |
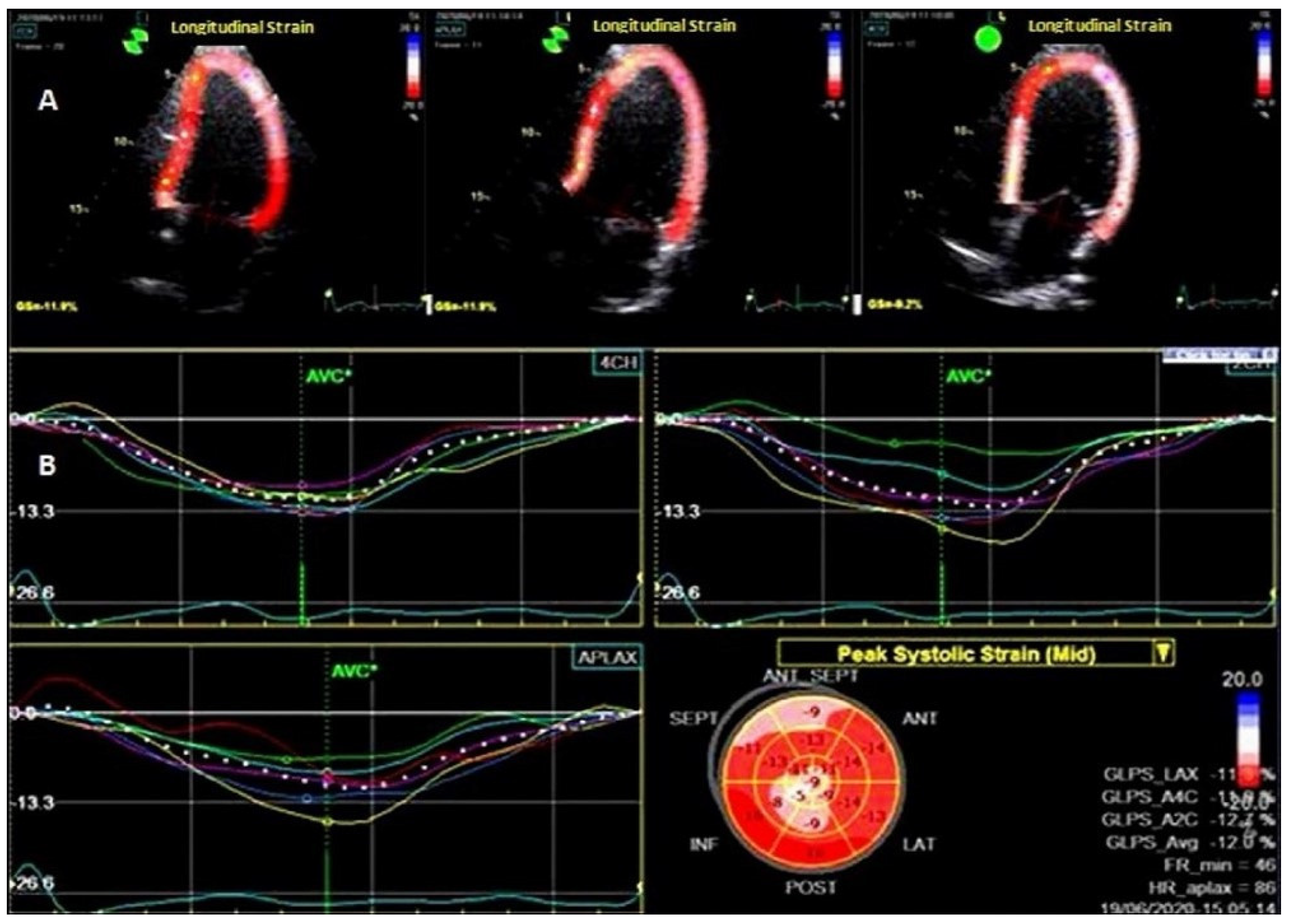
| GLS (%) | 20.1 ± 2.4 | 21.6 ± 2.1 | 0.0001 |
| GLS ≤ 18% | 34 (47%) | 13 (16%) | <0.0001 |
| Parameter | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| β | SE | p | β | SE | p | |
| Liver steatosis ≥ S2 | 2.17 | 0.62 | <0.001 | |||
| Liver fibrosis ≥ F2 | 3.60 | 0.81 | <0.0001 | 3.14 | 0.43 | <0.0001 |
| Independent predictors of LA stiffness ≥ 0.38 in MetS patients with DM | ||||||
| Parameter | Univariate analysis | Multivariate analysis | ||||
| β | SE | β | SE | |||
| Liver fibrosis ≥ F2 | 3.60 | 0.81 | <0.0001 | 3.14 | 0.43 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Apostu, A.; Malita, D.; Arnautu, S.-F.; Tomescu, M.-C.; Gaiță, D.; Popescu, A.; Mare, R.; Gidea, R.; Arnautu, D.-A. Significant Association between Subclinical Left Cardiac Dysfunction and Liver Stiffness in Metabolic Syndrome Patients with Diabetes Mellitus and Non-Alcoholic Fatty Liver Disease. Medicina 2023, 59, 328. https://doi.org/10.3390/medicina59020328
Apostu A, Malita D, Arnautu S-F, Tomescu M-C, Gaiță D, Popescu A, Mare R, Gidea R, Arnautu D-A. Significant Association between Subclinical Left Cardiac Dysfunction and Liver Stiffness in Metabolic Syndrome Patients with Diabetes Mellitus and Non-Alcoholic Fatty Liver Disease. Medicina. 2023; 59(2):328. https://doi.org/10.3390/medicina59020328
Chicago/Turabian StyleApostu, Alexandru, Daniel Malita, Sergiu-Florin Arnautu, Mirela-Cleopatra Tomescu, Dan Gaiță, Alina Popescu, Ruxandra Mare, Ramona Gidea, and Diana-Aurora Arnautu. 2023. "Significant Association between Subclinical Left Cardiac Dysfunction and Liver Stiffness in Metabolic Syndrome Patients with Diabetes Mellitus and Non-Alcoholic Fatty Liver Disease" Medicina 59, no. 2: 328. https://doi.org/10.3390/medicina59020328