
A Placebo-Controlled Trial to Evaluate Two Locally Delivered Antibiotic Gels (Piperacillin Plus Tazobactam vs. Doxycycline) in Stage III–IV Periodontitis Patients
 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
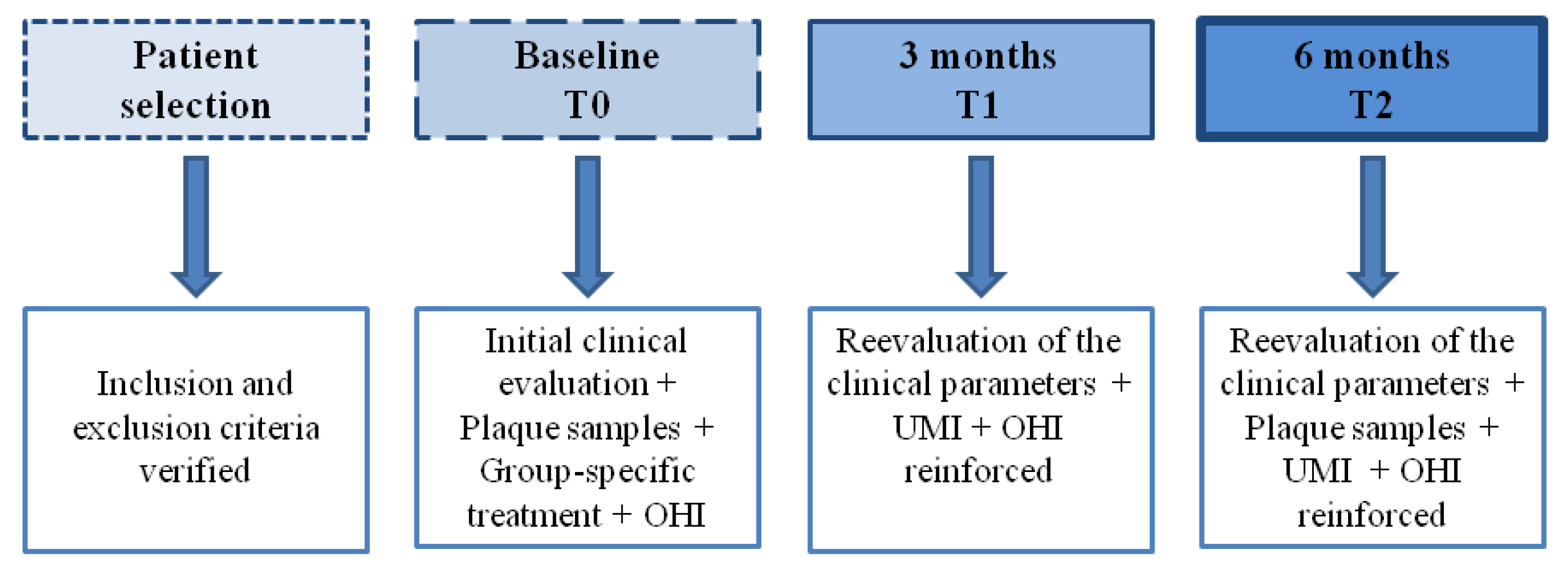
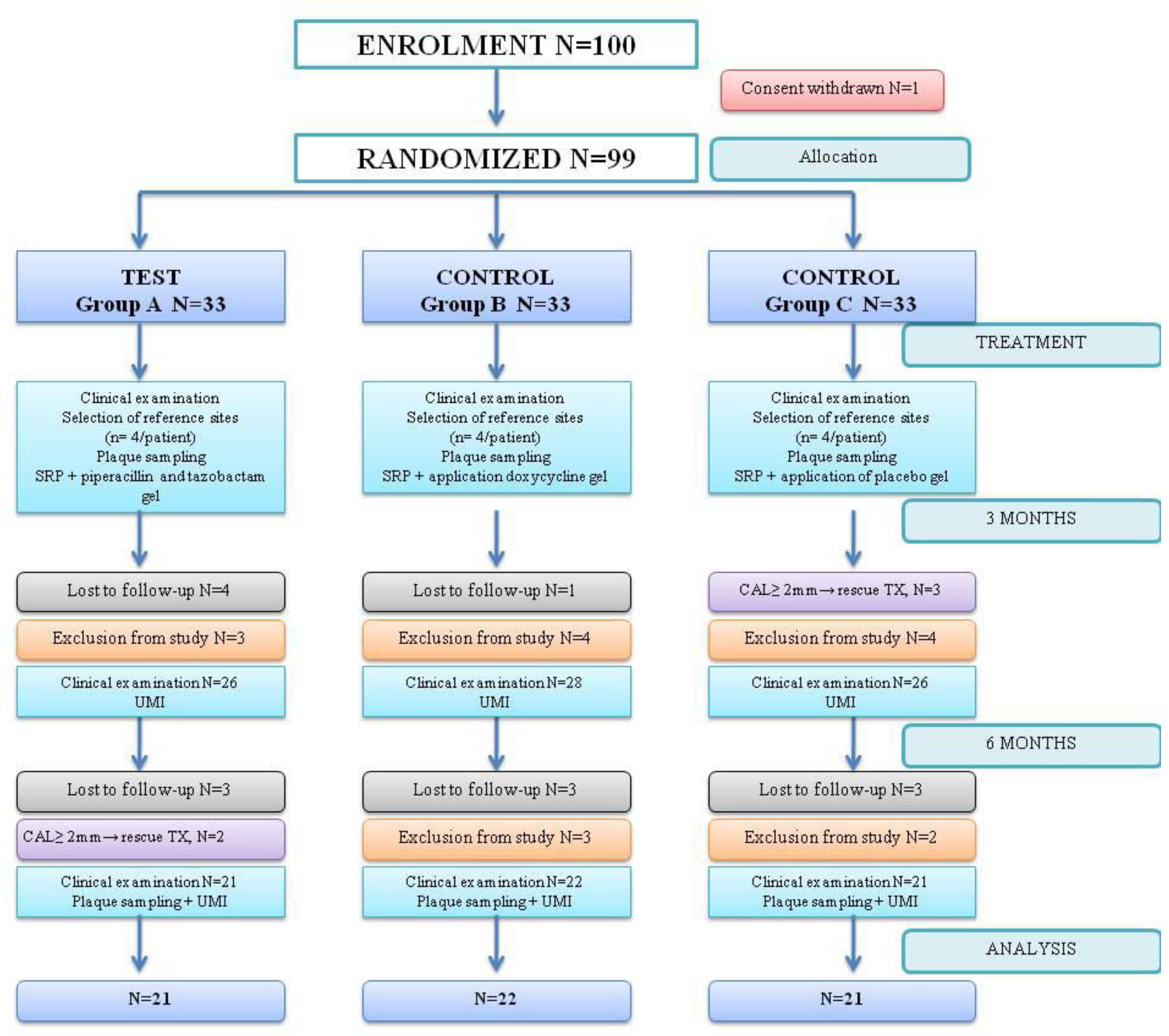
2.1. Study Design
2.2. Clinical Examination
2.3. Microbiological Examination
2.4. Randomization
2.5. Treatment Procedures
2.6. Statistical Analysis
3. Results
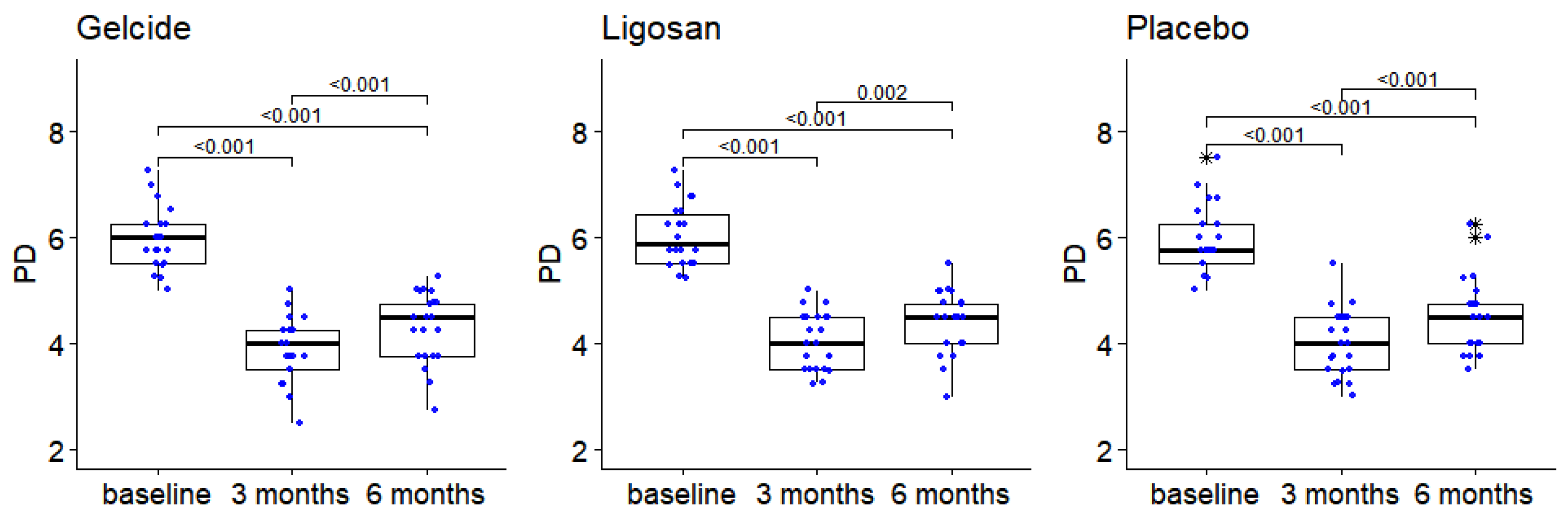
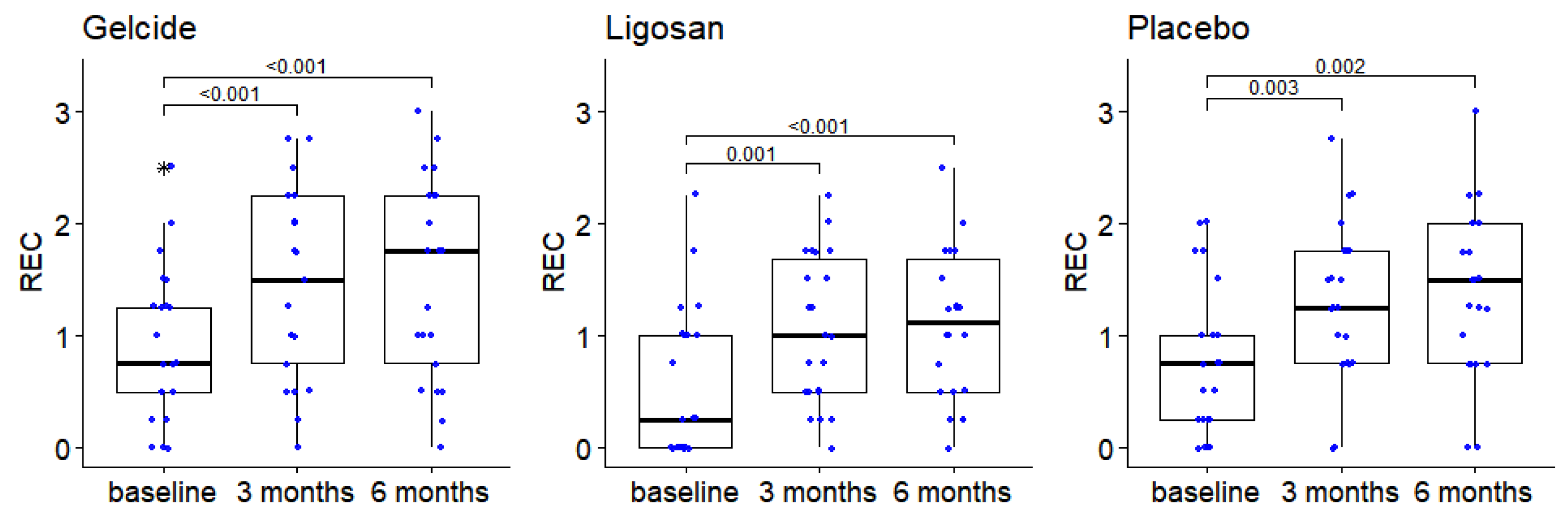
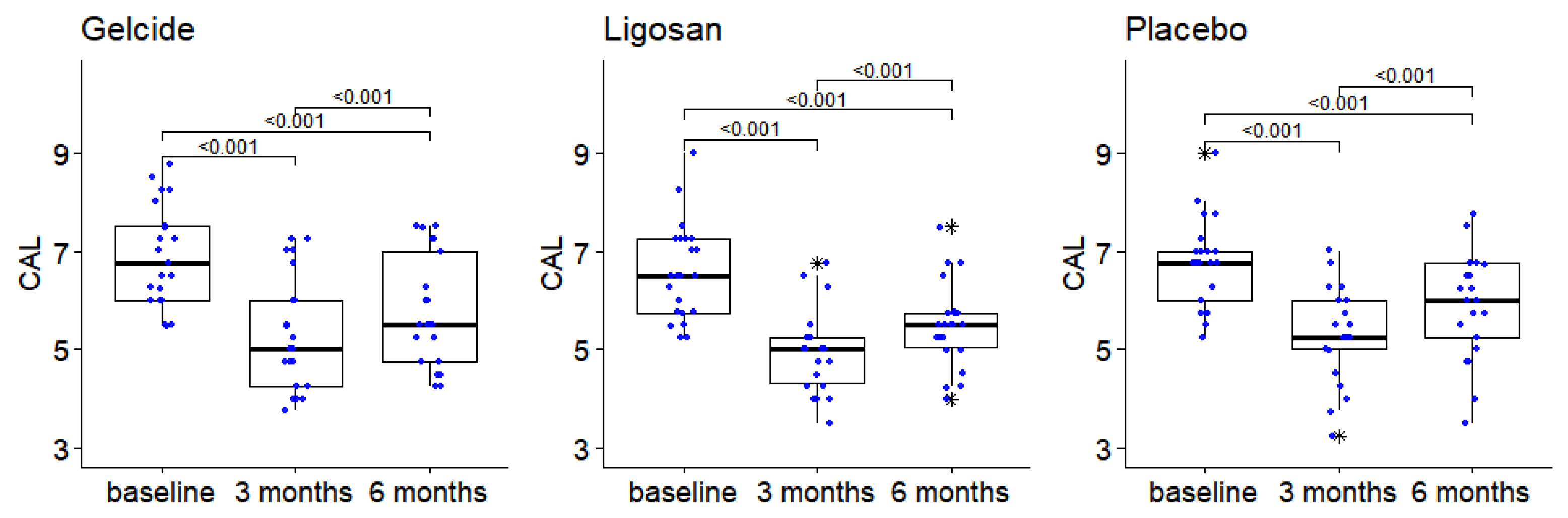
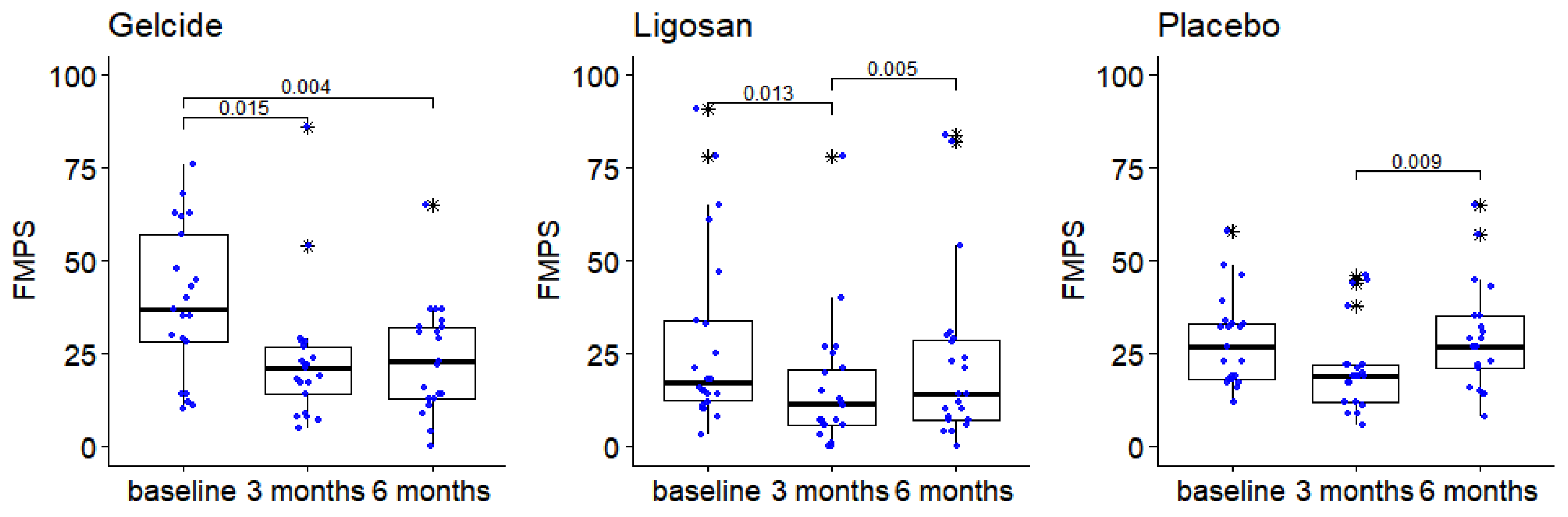
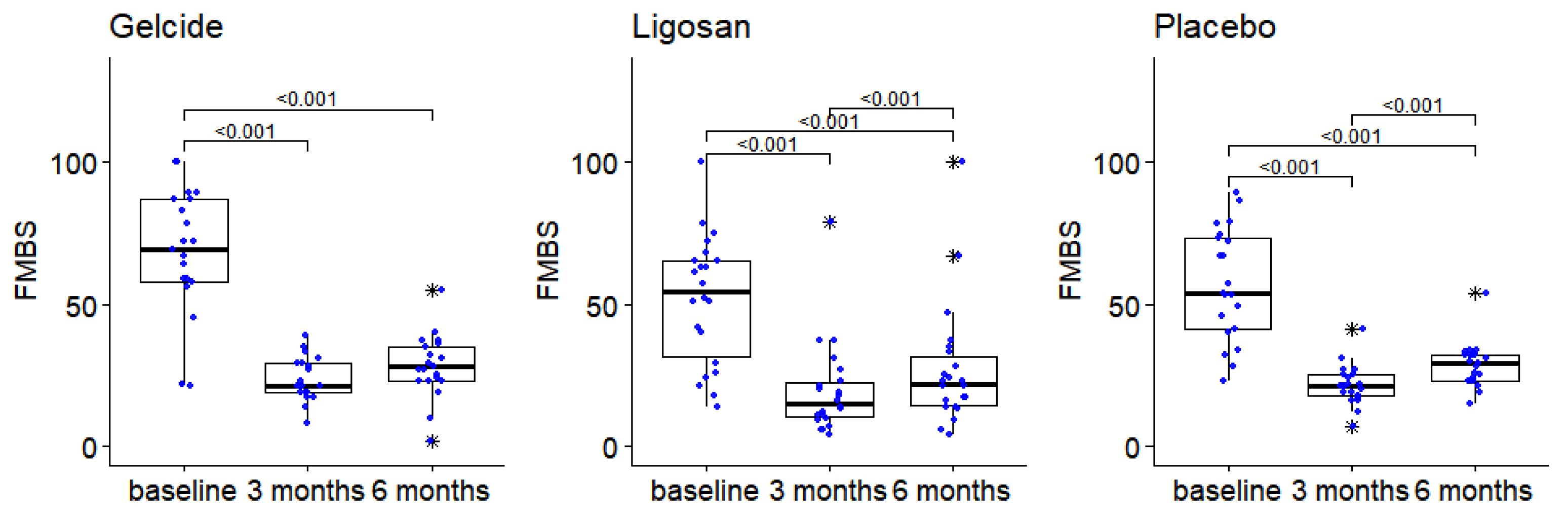
3.1. Clinical Results
3.2. Results of Microbiological Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zambon, J.J. Periodontal Diseases: Microbial Factors. Ann. Periodontol. 1996, 1, 879–925. [Google Scholar] [CrossRef] [PubMed]
- Offenbacher, S. Periodontal Diseases: Pathogenesis. Ann. Periodontol. 1996, 1, 821–878. [Google Scholar] [CrossRef] [PubMed]
- Van Winkelhoff, A.J.; Loos, B.G.; Van Der Reijden, W.A.; Van Der Velden, U. Porphyromonas gingivalis, Bacteroides forsythus and other putative periodontal pathogens in subjects with and without periodontal destruction. J. Clin. Periodontol. 2002, 29, 1023–1028. [Google Scholar] [CrossRef] [PubMed]
- Badersten, A.; Nilvéus, R.; Egelberg, J. Effect of nonsurgical periodontal therapy. J. Clin. Periodontol. 1981, 8, 57–72. [Google Scholar] [CrossRef]
- Kaldahl, W.B.; Kalkwarf, K.L.; Patil, K.D.; Molvar, M.P.; Dyer, J.K. Long-Term Evaluation of Periodontal Therapy: II. Incidence of Sites Breaking Down. J. Periodontol. 1996, 67, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Cobb, C.M. Non-Surgical Pocket Therapy: Mechanical. Ann. Periodontol. 1996, 1, 443–490. [Google Scholar] [CrossRef] [PubMed]
- Palcanis, K.G. Surgical Pocket Therapy. Ann. Periodontol. 1996, 1, 589–617. [Google Scholar] [CrossRef]
- Drisko, C.H. Non-Surgical Pocket Therapy: Pharmacotherapeutics. Ann. Periodontol. 1996, 1, 491–566. [Google Scholar] [CrossRef]
- Drisko, C.H. The use of locally-delivered doxycycline in the treatment of periodontitis. Clinical results. J. Clin. Periodontol. 1998, 25, 947–952. [Google Scholar] [CrossRef]
- Tonetti, M.S. The use of topical antibiotics in periodontal pockets. In Proceedings of the 2nd European Workshop on Periodontology, Thurgau, Switzerland, February 1996; Lang, N.P., Karring, T., Lindhe, J., Eds.; Quintessence Publishing: Berlin, Germany, 1997; pp. 78–109. [Google Scholar]
- Greenstein, G.; Polson, A. The Role of Local Drug Delivery in the Management of Periodontal Diseases: A Comprehensive Review. J. Periodontol. 1998, 69, 507–520. [Google Scholar] [CrossRef]
- Killoy, W.J. Chemical treatment of periodontitis: Local delivery of antimicrobials. Int Dent. J. 1998, 48 (Suppl. 1), 305–315. [Google Scholar] [CrossRef]
- Garrett, S.; Johnson, L.; Drisko, C.H.; Adams, D.F.; Bandt, C.; Beiswanger, B.; Bogle, G.; Donly, K.; Hallmon, W.W.; Hancock, E.B.; et al. Two multi-center studies evaluating locally delivered doxycycline hyclate, placebo control, oral hygiene, and scaling and root planing in the treatment of periodontitis. J. Periodontol. 1999, 70, 490–503. [Google Scholar] [CrossRef]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Berglundh, T.; Sculean, A.; Tonetti, M.S.; Aass, A.M.; Aimetti, M.; et al. EFP Workshop Participants and Methodological Consultants. Treatment of stage I-III periodontitis-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. 22), 4–60, Erratum in J. Clin. Periodontol. 2021, 48, 163. [Google Scholar] [CrossRef]
- Sanz, I.; Alonso, B.; Carasol, M.; Herrera, D.; Sanz, M. Nonsurgical treatment of periodontitis. J. Évid. Based Dent. Pract. 2012, 12 (Suppl. 3), 76–86. [Google Scholar] [CrossRef] [PubMed]
- Sender-Janeczek, A.; Zborowski, J.; Szulc, M.; Konopka, T. New Local Drug Delivery with Antibiotic in the Nonsurgical Treatment of Periodontitis—Pilot Study. Appl. Sci. 2019, 9, 5077. [Google Scholar] [CrossRef]
- Jervøe-Storm, P.M.; Al Ahdab, H.; Semaan, E.; Fimmers, R.; Jepsen, S. Microbiological outcomes of quadrant versus full-mouth root planning as monitored by real-time PCR. J. Clin. Periodontol. 2007, 34, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Roman-Torres, C.V.G.; Bryington, M.S.; Kussaba, S.T.; Pimentel, A.C.; Jimbo, R.; Cortelli, J.R.; Romito, G.A. Comparison of Full-Mouth Scaling and Quadrant-Wise Scaling in the Treatment of Adult Chronic Periodontitis. Braz. Dent. J. 2018, 29, 296–300. [Google Scholar] [CrossRef]
- Tomasi, C.; Koutouzis, T.; Wennström, J.L. Locally delivered doxycycline as an adjunct to mechanical debridement at retreatment of periodontal pockets. J. Periodontol. 2008, 79, 431–439. [Google Scholar]
- Rabbani, G.M.; Ash MMJr Caffesse, R.G. The effectiveness of subgingival scaling and root planing in calculus removal. J. Periodontol. 1981, 52, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Caffesse, R.G.; Sweeney, P.L.; Smith, B.A. Scaling and root planing with and without periodontal flap surgery. J. Clin. Periodontol. 1986, 13, 205–210. [Google Scholar] [CrossRef]
- Fleischer, H.C.; Mellonig, J.T.; Brayer, W.K.; Gray, J.L.; Barnett, J.D. Scaling and Root Planing Efficacy in Multirooted Teeth. J. Periodontol. 1989, 60, 402–409. [Google Scholar] [CrossRef]
- Claffey, N.; Loos, B.; Gantes, B.; Martin, M.; Egelberg, J. Probing depth at re-evaluation following initial periodontal therapy to indicate the initial response to treatment. J. Clin. Periodontol. 1989, 16, 229–233. [Google Scholar] [CrossRef]
- Claffey, N.; Egelberg, J. Clinical characteristics of periodontal sites with probing attachment loss following initial periodontal treatment. J. Clin. Periodontol. 1994, 21, 670–679. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89 (Suppl. 1), S159–S172, Erratum in J. Periodontol. 2018, 89, 1475. [Google Scholar] [CrossRef]
- Brown, M.; Gilbert, P. Sensitivity of biofilms to antimicrobial agents. J. Appl. Bacteriol. 1993, 74, 87S–97S. [Google Scholar] [CrossRef]
- Ashby, M.J.; Neale, J.E.; Knott, S.J.; Critchley, I.A. Effect of antibiotics on non-growing planktonic cells and biofilms of Escherichia coli. J. Antimicrob. Chemother. 1994, 33, 443–452. [Google Scholar] [CrossRef]
- Goodson, J.M. Pharmacokinetic principles controlling efficacy of oral therapy. J. Dent. Res. 1989, 68, 1625–1632. [Google Scholar]
- Greenstein, G.; Tonetti, M. The role of controlled drug delivery for periodontitis. The Research, Science and Therapy Committee of the American Academy of Periodontology. J. Periodontol. 2000, 71, 125–140. [Google Scholar] [CrossRef]
- Rams, T.E.; Slots, J. Local delivery of antimicrobial agents in the periodontal pocket. Periodontology 2000 1996, 10, 139–159. [Google Scholar] [CrossRef]
- Bonito, A.J.; Lux, L.; Lohr, K.N. Impact of Local Adjuncts to Scaling and Root Planing in Periodontal Disease Therapy: A Systematic Review. J. Periodontol. 2005, 76, 1227–1236. [Google Scholar] [CrossRef]
- Hanes, P.J.; Purvis, J.P. Local Anti-Infective Therapy: Pharmacological Agents. A Systematic Review. Ann. Periodontol. 2003, 8, 79–98. [Google Scholar] [CrossRef]
- Matesanz-Pérez, P.; García-Gargallo, M.; Figuero, E.; Bascones-Martínez, A.; Sanz, M.; Herrera, D. A systematic review on the effects of local antimicrobials as adjuncts to subgingival debridement, compared with subgingival debridement alone, in the treatment of chronic periodontitis. J. Clin. Periodontol. 2013, 40, 227–241. [Google Scholar] [CrossRef]
- Smiley, C.J.; Tracy, S.L.; Abt, E.; Michalowicz, B.S.; John, M.T.; Gunsolley, J.; Cobb, C.M.; Rossmann, J.; Harrel, S.K.; Forrest, J.L.; et al. Evidence-based clinical practice guideline on the nonsurgical treatment of chronic periodontitis by means of scaling and root planing with or without adjuncts. J. Am. Dent. Assoc. 2015, 146, 525–535. [Google Scholar] [CrossRef]
- Jepsen, K.; Jepsen, S. Antibiotics/antimicrobials: Systemic and local administration in the therapy of mild to moderately advanced periodontitis. Periodontology 2000 2016, 71, 82–112. [Google Scholar] [CrossRef]
- Soskolne, W.A.; Heasman, P.A.; Stabholz, A.; Smart, G.J.; Palmer, M.; Flashner, M.; Newman, H.N. Sustained local delivery of chlorhexidine in the treatment of periodontitis: A multi-center study. J. Periodontol. 1997, 68, 32–38. [Google Scholar] [CrossRef]
- Paquette, D.W.; Ryan, M.E.; Wilder, R.S. Locally delivered antimicrobials: Clinical evidence and relevance. J. Dent. Hyg. 2008, 82 (Suppl. 3), 10–15. [Google Scholar]
- Hamp, S.-E.; Nyman, S.; Lindhe, J. Periodontal treatment of multi rooted teeth. J. Clin. Periodontol. 1975, 2, 126–135. [Google Scholar] [CrossRef]
- Polson, A.M. The Research Team, Calibration, and Quality Assurance in Clinical Trials in Periodontics. Ann. Periodontol. 1997, 2, 75–82. [Google Scholar] [CrossRef]
- Miller, P.D., Jr. A classification of marginal tissue recession. Int. J. Periodontics Restor. Dent. 1985, 5, 8–13. [Google Scholar]
- Mühlemann, H.R.; Zander, H.A. Tooth Mobility (III): The Mechanism of Tooth Mobility. J. Periodontol. 1954, 25, 128–153. [Google Scholar] [CrossRef]
- Rusu, D.; Stratul, S.-I.; Sarbu, C.; Roman, A.; Anghel, A.; Didilescu, A.; Jentsch, H. Evaluation of a hydrophobic gel adhering to the gingiva in comparison with a standard water-soluble 1% chlorhexidine gel after scaling and root planing in patients with moderate chronic periodontitis. A randomized clinical trial. Int. J. Dent. Hyg. 2017, 15, 53–64. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 1 October 2021).
- Lauenstein, M.; Kaufmann, M.; Persson, G.R. Clinical and microbiological results following nonsurgical periodontal therapy with or without local administration of piperacillin/tazobactam. Clin. Oral Investig. 2013, 17, 1645–1660. [Google Scholar] [CrossRef]
- Joyston-Bechal, S.; Smales, F.C.; Duckworth, R. Effect of metronidazole on chronic periodontal disease in subjects using a topically applied chlorhexidine gel. J. Clin. Periodontol. 1984, 11, 53–62. [Google Scholar] [CrossRef]
- Goodson, J.M.; Holborow, D.; Dunn, R.L.; Hogan, P.; Dunham, S. Monolithic tetracycline-containing fibers for controlled delivery to periodontal pockets. J. Periodontol. 1983, 54, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Greenstein, G. Clinical significance of bacterial resistance to tetracyclines in the treatment of periodontal diseases. J. Periodontol. 1995, 66, 925–932. [Google Scholar] [CrossRef]
- Tan, O.L.; Safii, S.H.; Razali, M. Commercial local pharmacotherapeutics and adjunctive agents for nonsurgical treatment of periodontitis: A contemporary review of clinical efficacies and challenges. Antibiotics 2020, 9, 11. [Google Scholar] [CrossRef]
- Wennström, J.L.; Newman, H.N.; MacNeill, S.R.; Killoy, W.J.; Griffiths, G.S.; Gillam, D.G.; Krok, L.; Needleman, I.G.; Weiss, G.; Garrett, S. Utilisation of locally delivered doxycycline in non-surgical treatment of chronic periodontitis. A comparative multi-centre trial of 2 treatment approaches. J. Clin. Periodontol. 2001, 28, 753–761. [Google Scholar] [CrossRef]
- Badersten, A.; Nilveus, R.; Egelberg, J. Effect of nonsurgical periodontal therapy. III. Single versus repeated instrumentation. J. Clin. Periodontol. 1984, 11, 114–124. [Google Scholar] [CrossRef]
- Anderson, G.B.; Palmer, J.A.; Bye, F.L.; Smith, B.A.; Caffesse, R.G. Effectiveness of subgingival scaling and root planing: Single versus multiple episodes of instrumentation. J. Periodontol. 1996, 67, 367–373. [Google Scholar] [CrossRef]
- Kinane, D.F.; Radvar, M. A six-month comparison of three periodontal local antimicrobial therapies in persistent periodontal pockets. J. Periodontol. 1999, 70, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Van Steenberghe, D.; Rosling, B.; Söder, P.Ö.; Landry, R.G.; Van der Velden, U.; Timmerman, M.F.T.; McCarthy, E.; Vandenhoven, G.; Wouters, C.; Wilson, M.; et al. A 15-month evaluation of the effects of repeated subgingival minocycline in chronic adult periodontitis. J. Periodontol. 1999, 70, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.C.; Paquette, D.W.; Offenbacher, S.; Adams, D.F.; Armitage, G.C.; Bray, K.; Caton, J.; Cochran, D.L.; Drisko, C.H.; Fiorellini, J.P.; et al. Treatment of periodontitis by local administration of minocycline microspheres: A controlled trial. J. Periodontol. 2001, 72, 1535–1544. [Google Scholar] [CrossRef]
- Ahamed, S.; Jalaluddin, M.; Khalid, I.; Moon, N.; Shafi, T.K.; Ali, F.M. The use of controlled release locally delivered 10% doxycycline hyclate gel as an adjunct to scaling and root planing in the treatment of chronic periodontitis: Clinical and microbiological results. J. Contemp. Dent. Pract. 2013, 14, 1080–1086. [Google Scholar]
- Sandhya, Y.P.; Prabhuji, M.L.; Chandra, R.V. Comparative evaluation of the efficacy of 10% doxycycline hyclate in the periodontal treatment of smokers—A clinical and microbiological study. Oral Health Prev. Dent. 2011, 9, 59–65. [Google Scholar] [PubMed]
- Tonetti, M.S.; Cortellini, P.; Carnevale, G.; Cattabriga, M.; de Sanctis, M.; Pini Prato, G.P. A controlled multicenter study of adjunctive use of tetracycline periodontal fibers in mandibular class II furcations with persistent bleeding. J. Clin. Periodontol. 1998, 25, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Mestnik, M.J.; Feres, M.; Figueiredo, L.C.; Duarte, P.M.; Lira, E.A.; Faveri, M. Short-term benefits of the adjunctive use of metronidazole plus amoxicillin in the microbial profile and in the clinical parameters of subjects with generalized aggressive periodontitis. J. Clin. Periodontol. 2010, 37, 353–365. [Google Scholar] [CrossRef]
- Lazar, V. Quorum sensing in biofilms—How to destroy the bacterial citadels or their cohesion/power? Anaerobe 2011, 17, 280–285. [Google Scholar] [CrossRef]
- Badersten, A.; Niveus, R.; Egelberg, J. 4-year observations of basic periodontal therapy. J. Clin. Periodontol. 1987, 14, 438–444. [Google Scholar] [CrossRef]
- Ramfjord, S.P.; Caffesse, R.G.; Morrison, E.C.; Hill, R.W.; Kerry, G.J.; Appleberry, E.A.; Nissle, R.R.; Stults, D.L. 4 modalities of periodontal treatment compared over 5 years. J. Clin. Periodontol. 1987, 14, 445–452. [Google Scholar] [CrossRef]
- Rosén, B.; Olavi, G.; Badersten, A.; Rönström, A.; Söderholm, G.; Egelberg, J. Effect of different frequencies of preventive maintenance treatment on periodontal conditions. 5-Year observations in general dentistry patients. J. Clin. Periodontol. 1999, 26, 225–233. [Google Scholar] [CrossRef]
- Goodson, J.M.; Gunsolley, J.C.; Grossi, S.G.; Bland, P.S.; Otomo-Corgel, J.; Doherty, F.; Comiskey, J. Minocycline HCl microspheres reduce red-complex bacteria in periodontal disease therapy. J. Periodontol. 2007, 78, 1568–1579. [Google Scholar] [CrossRef] [PubMed]
- Flemmig, T.F.; Petersilka, G.; Völp, A.; Gravemeier, M.; Zilly, M.; Mross, D.; Prior, K.; Yamamoto, J.; Beikler, T. Efficacy and safety of adjunctive local moxifloxacin delivery in the treatment of periodontitis. J. Periodontol. 2011, 82, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Eickholz, P.; Kim, T.-S.; Bürklin, T.; Schacher, B.; Renggli, H.H.; Schaecken, M.T.; Holle, R.; Kübler, A.; Ratka-Krüger, P. Non-surgical periodontal therapy with adjunctive topical doxycycline: A double-blind randomized controlled multicenter study. J. Clin. Periodontol. 2002, 29, 108–117. [Google Scholar] [CrossRef]
- Wennström, J.L.; Tomasi, C.; Bertelle, A.; Dellasega, E. Fullmouth ultrasonic debridement versus quadrant scaling and root planing as an initial approach in the treatment of chronic periodontitis. J. Clin. Periodontol. 2005, 32, 851–859. [Google Scholar] [CrossRef] [PubMed]
- Feres, M.; Gursky, L.C.; Faveri, M.; Tsuzuki, C.O.; Figueiredo, L.C. Clinical and microbiological benefits of strict supragingival plaque control as part of the active phase of periodontal therapy. J. Clin. Periodontol. 2009, 36, 857–867. [Google Scholar] [CrossRef] [PubMed]
- Santos, V.R.; Lima, J.A.; De Mendonça, A.C.; Braz Maximo, M.B.; Faveri, M.; Duarte, P.M. Effectiveness of full-mouth and partial-mouth scaling and root planing in treating chronic periodontitis in subjects with type 2 diabetes. J. Periodontol. 2009, 80, 1237–1245. [Google Scholar] [CrossRef]
- Saito, A.; Hosaka, Y.; Kikuchi, M.; Akamatsu, M.; Fukaya, C.; Matsumoto, S.; Ueshima, F.; Hayakawa, H.; Fujinami, K.; Nakagawa, T. Effect of initial periodontal therapy on oral health-related quality of life in patients with periodontitis in Japan. J. Periodontol. 2010, 81, 1001–1009. [Google Scholar] [CrossRef]
- Bland, P.S.; Goodson, J.M.; Gunsolley, J.C.; Grossi, S.G.; Otomo-Corgel, J.; Doherty, F.; Comiskey, J.L. Association of antimicrobial and clinical efficacy: Periodontitis therapy with minocycline microspheres. J. Int. Acad. Periodontol. 2010, 12, 11–19. [Google Scholar]
- John, M.T.; Michalowicz, B.S.; Kotsakis, G.A.; Chu, H. Network meta-analysis of studies included in the Clinical Practice Guideline on the nonsurgical treatment of chronic periodontitis. J. Clin. Periodontol. 2017, 44, 603–611. [Google Scholar] [CrossRef]
- Stoller, N.H.; Johnson, L.R.; Trapnell, S.; Harrold, C.Q.; Garrett, S. The pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline compared to systemically delivered doxycycline in gingival crevicular fluid, saliva, and serum. J. Periodontol. 1998, 69, 1085–1091, Erratum in J. Periodontol. 1999, 70, 238. [Google Scholar] [CrossRef]
- Renvert, S.; Wikström, M.; Dahlén, G.; Slots, J.; Egelberg, J. On the inability of root debridement and periodontal surgery to eliminate Actinobacillus actinomycetemcomitans from periodontal pockets. J. Clin. Periodontol. 1990, 17, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, I.; Dimitriadis, N.; Papadimitriou, K.; Sakellari, D.; Vouros, I.; Konstantinidis, A. Hand instrumentation versus ultrasonic debridement in the treatment of chronic periodontitis: A randomized clinical and microbiological trial. J. Clin. Periodonto.l 2009, 36, 132–241. [Google Scholar] [CrossRef] [PubMed]
- Jeffcoat, M.K.; Bray, K.S.; Ciancio, S.G.; Dentino, A.R.; Fine, D.H.; Gordon, J.M.; Gunsolley, J.C.; Killoy, W.J.; Lowenguth, R.A.; Magnusson, N.I.; et al. Adjunctive use of a subgingival controlled-release chlorhexidine chip reduces probing depth and improves attachment level compared with scaling and root planing alone. J. Periodontol. 1998, 69, 989–997. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Time Point | Group A (n = 21) | Group B (n = 22) | Group C (n = 21) | p-Values |
|---|---|---|---|---|---|
| Age (years, mean ± sd) | Baseline | 50.71 ± 9.56 | 0.489 a | ||
| Sex = female (n, %) | Baseline | 8 (38.10%) | 13 (59.09%) | 14 (66.67%) | 0.156 b |
| Smokers (n, %) | Baseline | 9 (42.86%) | 8 (36.36%) | 9 (42.86%) | 0.881b |
| PPD (n, %) 5 mm 6 mm 7 mm 8 mm | Baseline Baseline Baseline Baseline | 28 (33.33%) 34 (40.48%) 18 (21.43%) 4 (4.76%) | 32 (36.36%) 29 (32.96%) 19 (21.59%) 8 (9.09%) | 28 (33.33%) 35 (41.67%) 16 (19.05%) 5 (5.95%) | 0.853 a |
| PPD (mm ± sd) | Baseline 3 months Difference to baseline 6 months Difference to baseline | 0.936 a 0.766 a 0.919 a 0.837 a 0.410 a | |||
| REC (mm ± sd) | Baseline 3 months Difference to baseline 6 months Difference to baseline | 0.119 a 0.216 a 0.926 a 0.231 a 0.955 a | |||
| CAL (mm ± sd) | Baseline 3 months Difference to baseline 6 months Difference to baseline | 0.575 a 0.475 a 0.573 a 0.315 a 0.203 a | |||
| FMPS (± sd) | Baseline 3 months Difference to baseline 6 months Difference to baseline | 0.074 a 0.045 a 0.396 a 0.072 a 0.093 a | |||
| FMBS (± sd) | Baseline 3 months Difference to baseline 6 months Difference to baseline | 0.077 a 0.057 a 0.188 a 0.152 a 0.113 a | |||
| BOP | Baseline 3 months 6 months | 83/84 (98.81%) 25/84 (29.76%) 27/84 (32.14%) | 88/88 (100%) 26/88 (29.55%) 30/88 (34.09%) | 82/84 (97.62%) 29/84 (34.52%) 35/84 (41.67%) | - 0.732 b 0.396 b |
| Pocket closure (%) | Baseline 3 months 6 months | 0/84 55/84 (65.48%) 39/84 (46.43%) | 0/88 53/88 (60.23%) 38/88 (43.18%) | 0/84 49/84 (58.33%) 31/84 (36.90%) | - 0.615 b 0.446 b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilyes, I.; Rusu, D.; Rădulescu, V.; Vela, O.; Boariu, M.I.; Roman, A.; Surlin, P.; Kardaras, G.; Boia, S.; Chinnici, S.; et al. A Placebo-Controlled Trial to Evaluate Two Locally Delivered Antibiotic Gels (Piperacillin Plus Tazobactam vs. Doxycycline) in Stage III–IV Periodontitis Patients. Medicina 2023, 59, 303. https://doi.org/10.3390/medicina59020303
Ilyes I, Rusu D, Rădulescu V, Vela O, Boariu MI, Roman A, Surlin P, Kardaras G, Boia S, Chinnici S, et al. A Placebo-Controlled Trial to Evaluate Two Locally Delivered Antibiotic Gels (Piperacillin Plus Tazobactam vs. Doxycycline) in Stage III–IV Periodontitis Patients. Medicina. 2023; 59(2):303. https://doi.org/10.3390/medicina59020303
Chicago/Turabian StyleIlyes, Ioana, Darian Rusu, Viorelia Rădulescu, Octavia Vela, Marius Ion Boariu, Alexandra Roman, Petra Surlin, Giorgios Kardaras, Simina Boia, Salvatore Chinnici, and et al. 2023. "A Placebo-Controlled Trial to Evaluate Two Locally Delivered Antibiotic Gels (Piperacillin Plus Tazobactam vs. Doxycycline) in Stage III–IV Periodontitis Patients" Medicina 59, no. 2: 303. https://doi.org/10.3390/medicina59020303