
The Influence of Chlorhexidine Gluconate Dentine Pre-Treatment on Adhesive Interface and Marginal Sealing


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Preparation
2.2. Pulpal Pressure Simulation
2.3. Simulation of Cariogenic Attack
2.4. Samples Preparation for the Microleakage Study
2.5. Samples Preparation for the SEM Study
2.6. Statistical Analysis
3. Results
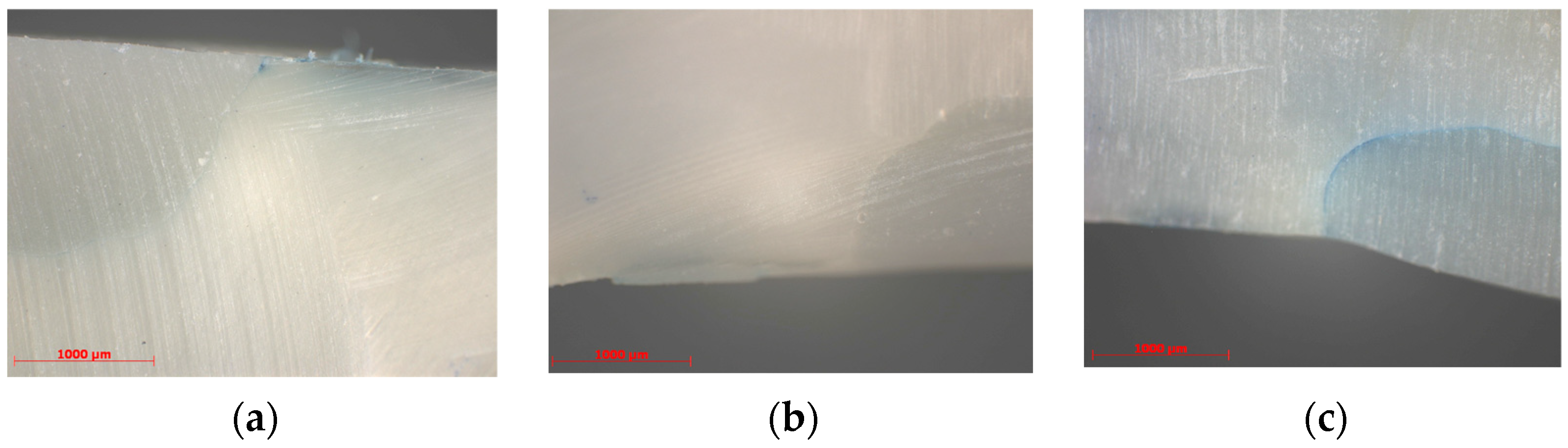
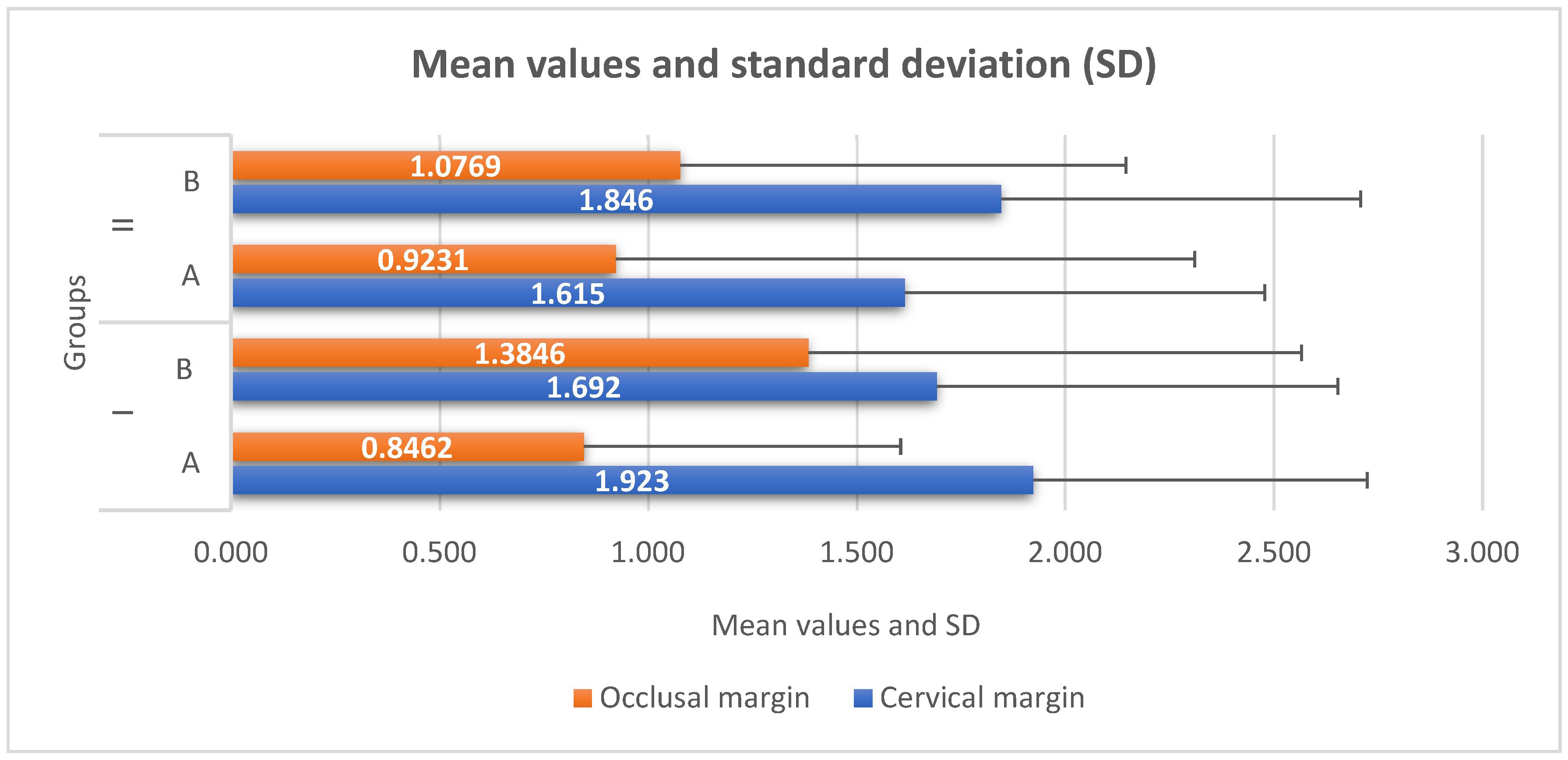
3.1. Microleakage Evaluation
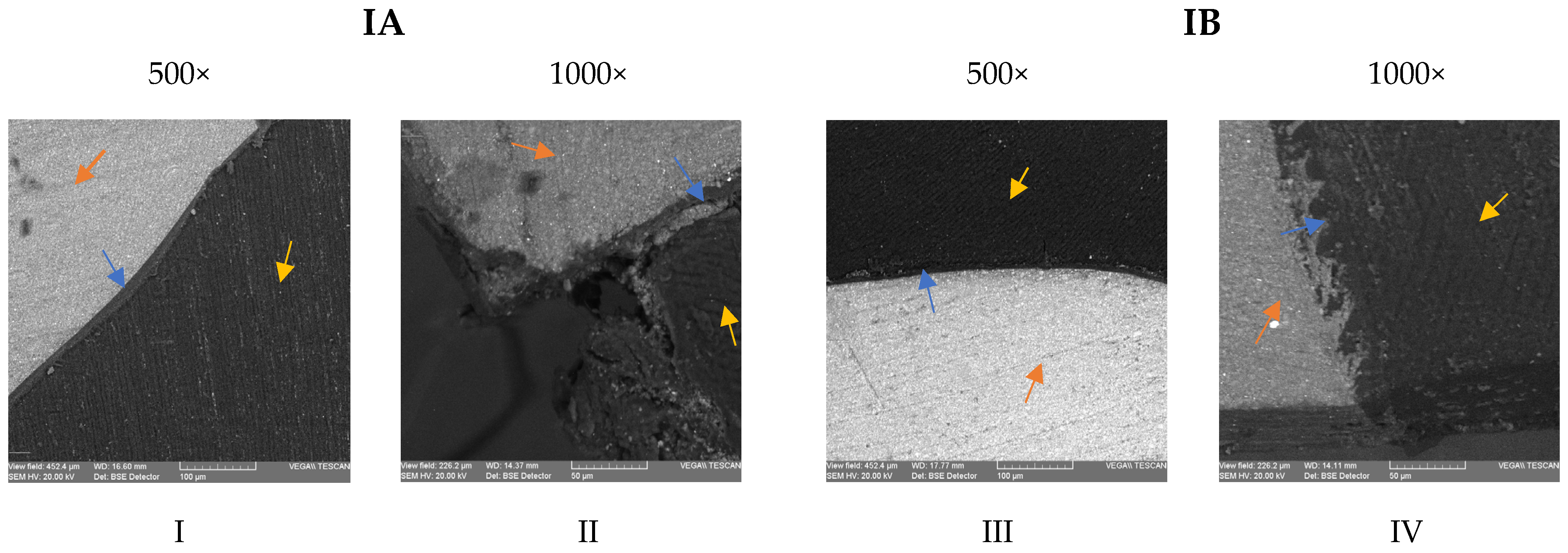
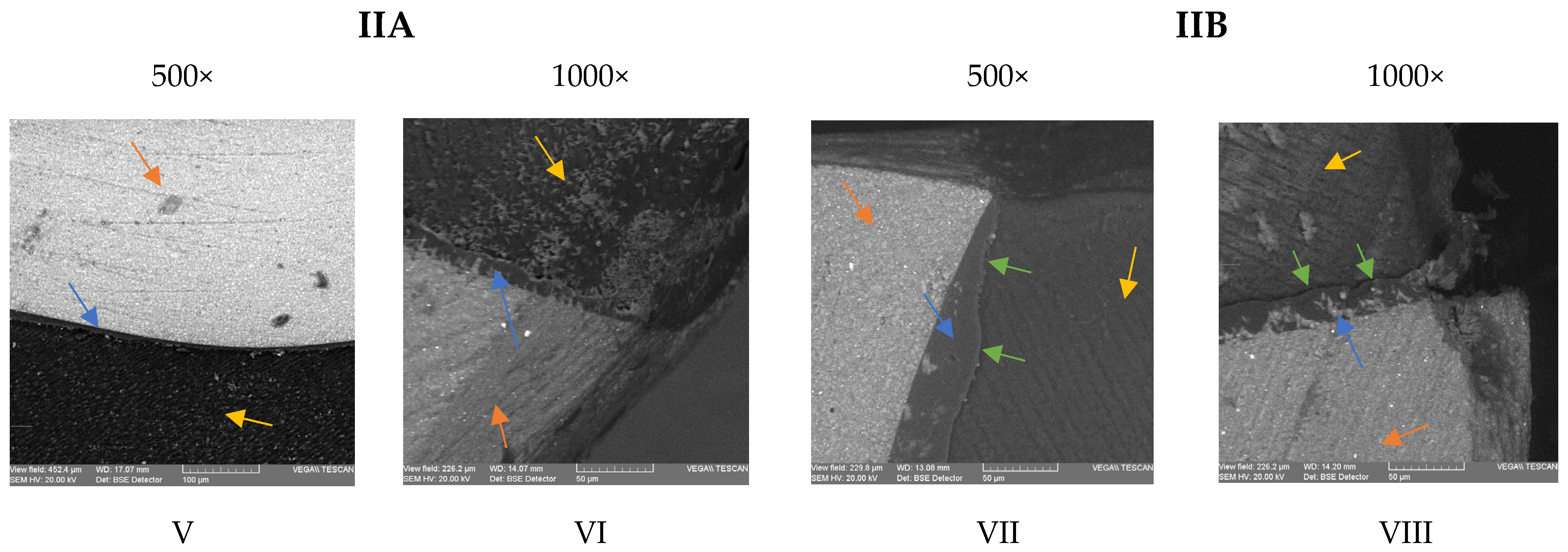
3.2. Scanning Electron Microscopy Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, L.; Chen, W.; Yu, Y.; Yang, J.; Jiang, Q.; Wu, W.; Yang, D. Effect of chlorhexidine-loaded poly (amido amine) dendrimer on matrix metalloproteinase activities and remineralization in etched human dentin in vitro. J. Mech. Behav. Biomed. Mater. 2021, 121, 104625. [Google Scholar] [CrossRef]
- Shen, J.; Xie, H.; Wang, Q.; Wu, X.; Yang, J.; Chen, C. Evaluation of the interaction of chlorhexidine and MDP and its effects on the durability of dentin bonding. Dent. Mater. 2020, 36, 1624–1634. [Google Scholar] [CrossRef] [PubMed]
- Iovan, G.; Ghiorghe, C.A.; Stoleriu, S.; Pancu, G.; Nica, I.; Taraboanta, I.; Andrian, S. Effect of Dental Bleaching on Marginal Sealing of Composite Resin Restorations Bonded with a Universal Adhesive. Mater. Plast. 2018, 55, 233. [Google Scholar] [CrossRef]
- Ástvaldsdóttir, Á.; Dagerhamn, J.; van Dijken, J.W.; Naimi-Akbar, A.; Sandborgh-Englund, G.; Tranæus, S. Longevity of posterior resin composite restorations in adults—A systematic review. J. Dent. 2015, 43, 934–954. [Google Scholar] [CrossRef]
- Nedeljkovic, I.; Teughels, W.; De Munck, J.; Van Meerbeek, B.; Van Landuyt, K.L. Is secondary caries with composites a material-based problem? Dent. Mater. 2015, 31, 247–277. [Google Scholar]
- Grégoire, G.; Sharrock, P.; Prigent, Y. Performance of a universal adhesive on etched and non-etched surfaces: Do the results match the expectations? Mater. Sci. Eng. C. Mater. Biol. Appl. 2016, 66, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Abrar, E.; Naseem, M.; Baig, Q.A.; Vohra, F.; Maawadh, A.M.; Almohareb, T.; AlRifaiy, M.Q.; Abduljabbar, T. Antimicrobial efficacy of silver diamine fluoride in comparison to photodynamic therapy and chlorhexidine on canal disinfection and bond strength to radicular dentin. Photodiagn. Photodyn. Ther. 2020, 32, 102066. [Google Scholar] [CrossRef]
- Albaladejo, A.; Osorio, R.; Toledano, M.; Ferrari, M. Hybrid layers of etch-and-rinse versus self-etching adhesive systems. Med. Oral Patol. Oral. Cir. Bucal. 2010, 15, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Carrilho, M.R.; Tay, F.R.; Donnelly, A.M.; Agee, K.A.; Tjäderhane, L.; Mazzoni, A.; Breschi, L.; Foulger, S.; Pashley, D.H. Host-derived loss of dentin matrix stiffness associated with solubilization of collagen. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 90, 373–380. [Google Scholar] [CrossRef] [Green Version]
- Makishi, P.; Pacheco, R.R.; Sadr, A.; Shimada, Y.; Sumi, Y.; Tagami, J. Assessment of self-adhesive resin composites: Nondestructive imaging of resin-dentin interfacial adaptation and shear bond strength. Microsc. Microanal. 2015, 21, 1523–1529. [Google Scholar] [CrossRef] [PubMed]
- Tay, F.R.; Pashley, D.H.; Suh, B.I.; Hiraishi, N.; You, C.K. Water treeing in simplified dentin adhesives—Deja vu? Oper. Dent. 2005, 30, 561–579. [Google Scholar] [PubMed]
- Belli, R.; Sartori, N.; Peruchi, L.D.; Guimarães, J.C.; Araújo, É.; Monteiro, S., Jr.; Baratieri, L.N.; Lohbauer, U. Slow progression of dentin bond degradation during one-year water storage under simulated pulpal pressure. J. Dent. 2010, 38, 802–810. [Google Scholar] [CrossRef]
- Tay, F.R.; King, N.M.; Chan, K.M.; Pashley, D.H. How can nanoleakage occur in self-etching adhesive systems that demineralize and infiltrate simultaneously? J. Adhes. Dent. 2002, 4, 255–269. [Google Scholar]
- Taraboanta, I.; Stoleriu, S.; Iovan, G.I.; Moldovanu, A.; Georgescu, A.; Negraia, M.; Andrian, S. Evaluation of pre-heating effects on marginal adaptation of resin-based materials. Mater. Plast. 2018, 55, 238–242. [Google Scholar] [CrossRef]
- Liu, Y.; Tj¨aderhane, L.; Breschi, L.; Mazzoni, A.; Li, N.; Mao, J.; Pashley, D.H.; Tay, F.R. Limitations in bonding to dentin and experimental strategies to prevent bond degradation. J. Dent. Res. 2011, 90, 953–968. [Google Scholar] [CrossRef] [PubMed]
- Frassetto, A.; Breschi, L.; Turco, G.; Marchesi, G.; Di Lenarda, R.; Tay, F.R. Mechanisms of degradation of the hybrid layer in adhesive dentistry and therapeutic agents to improve bond durability—A literature review. Dent. Mater. 2016, 32, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Tan, J.; Chen, L.; Li, D.; Tan, Y. The incorporation of chlorhexidine in a two-step self-etching adhesive preserves dentin bond in vitro. J. Dent. 2009, 37, 807–812. [Google Scholar] [CrossRef]
- Toledano, M.; Yamauti, M.; Osorio, E.; Osorio, R. Zinc-inhibited MMP-mediated collagen degradation after different dentine demineralization procedures. Caries. Res. 2012, 46, 201–207. [Google Scholar] [CrossRef]
- Santiago, S.L.; Osorio, R.; Neri, J.R.; Carvalho, R.M.; Toledano, M. Effect of the flavonoid epigallocatechin-3-gallate on resin-dentin bond strength. J. Adhes. Dent. 2013, 15, 535–540. [Google Scholar]
- Carrilho, M.R.; Carvalho, R.M.; Sousa, E.N.; Nicolau, J.; Breschi, L.; Mazzoni, A.; Tj¨aderhane, L.; Tay, F.R.; Agee, K.; Pashley, D.H. Substantivity of chlorhexidine to human dentin. Dent. Mater. 2010, 26, 779–785. [Google Scholar] [CrossRef] [Green Version]
- Gunaydin, Z.; Yazici, A.R.; Cehreli, Z.C. In Vivo and In Vitro Effects of Chlorhexidine Pretreatment on Immediate and Aged Dentin Bond Strengths. Oper. Dent. 2016, 41, 258–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, D.; Huang, X.; Huang, C.; Yang, T.; Du, X.; Wang, Y. Effects of chlorhexidine on bonding durability of different adhesive systems using a novel thermocycling method. Aust. Dent. J. 2013, 58, 148–155. [Google Scholar] [CrossRef]
- Shadman, N.; Farzin-Ebrahimi, S.; Mortazavi-Lahijani, E.; Jalali, Z. Effect of chlorhexidine on the durability of a new universal adhesive system. J. Clin. Exp. Dent. 2018, 10, 921. [Google Scholar] [CrossRef] [PubMed]
- Jacomine, J.C.; Giacomini, M.; Agulhari, M.A.; Zabeu, G.; Honório, H.; Wang, L. Performance of a Universal Bonding System Associated With 2% Digluconate Chlorhexidine in Carious and Eroded Dentin. Oper. Dent. 2021, 46, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Agulhari, M.A.S.; Froio, N.L.; Jacomine, J.C.; Giacomini, M.C.; Borges, A.F.S.; Honório, H.M.; Wang, L. Profile of MDP-chlorhexidine for universal dentin bonding systems: A calcium-competition interference? Int. J. Adhes. Adhes. 2022, 116, 103140. [Google Scholar] [CrossRef]
- Gwinnett, A.J. Acid etching for composite resins. Dent. Clin. N. Am. 1981, 25, 271–289. [Google Scholar] [CrossRef] [PubMed]
- Osorio, R.; Yamauti, M.; Osorio, E.; Ruiz-Requena, M.E.; Pashley, D.; Tay, F.; Toledano, M. Effect of dentin etching and chlorhexidine application on metalloproteinase-mediated collagen degradation. Eur. J. Oral Sci. 2011, 119, 79–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sai, K.; Takamizawa, T.; Imai, A.; Tsujimoto, A.; Ishii, R.; Barkmeier, W.W.; Latta, M.A.; Miyazaki, M. Influence of application time and etching mode of universal adhesives on enamel adhesion. J. Adhes. Dent. 2018, 20, 65–77. [Google Scholar] [PubMed]
- Feitosa, V.P.; Correr, A.B.; Correr-Sobrinho, L.; Sinhoreti, M.A. Effect of a new method to simulate pulpal pressure on bond strength and nanoleakage of dental adhesives to dentin. J. Adhes. Dent. 2012, 6, 517–524. [Google Scholar]
- Feitosa, V.P.; Sauro, S.; Watson, T.F.; Correr, A.B.; Osorio, R.; Toledano, M. Evaluation of the micro-mechanical strength of resin bonded-dentin interfaces submitted to short-term degradation strategies. J. Mech. Behav. Biomed. Mater. 2012, 15, 112–120. [Google Scholar] [CrossRef]
- Matsuda, Y.; Komatsu, H.; Murata, Y.; Tanaka, T.; Sano, H. A newly designed automatic pH-cycling system to simulate daily pH fluctuations. Dent. Mater. 2006, 25, 280–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Putzeys, E.; Duca, R.C.; Coppens, L.; Vanoirbeek, J.; Godderis, L.; Van Meerbeek, B.; Van Landuyt, K.L. In-vitro transdentinal diffusion of monomers from adhesives. J. Dent. 2018, 75, 91–97. [Google Scholar] [CrossRef]
- Feitosa, V.P.; Leme, A.A.; Sauro, S.; Correr-Sobrinho, L.; Watson, T.F.; Sinhoreti, M.A.; Correr, A.B. Hydrolytic degradation of the resin–dentine interface induced by the simulated pulpal pressure, direct and indirect water ageing. J. Dent. 2012, 40, 1134–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagi, K.; Yamamoto, H.; Uemura, R.; Matsuda, Y.; Okuyama, K.; Ishimoto, T.; Nakano, T.; Hayashi, M. Use of PIXE/PIGE for sequential Ca and F measurements in root carious model. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vachiramon, V.; Vargas, M.A.; Pashley, D.H.; Tay, F.R.; Geraldeli, S.; Qian, F.; Armstrong, S.R. Effects of oxalate on dentin bond after 3-month simulated pulpal pressure. J. Dent. 2008, 36, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Santana, V.B.; De Alexandre, R.S.; Rodrigues, J.A.; Ely, C.; Reis, A.F. Effects of immediate dentin sealing and pulpal pressure on resin cement bond strength and nanoleakage. Oper. Dent. 2016, 41, 189–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breschi, L.; Maravic, T.; Comba, A.; Cunha, S.R.; Loguercio, A.D.; Reis, A.; Hass, V.; Cadenaro, M.; Mancuso, E.; Mayer-Santos, E.; et al. Chlorhexidine preserves the hybrid layer in vitro after 10-years aging. Dent. Mater. 2020, 36, 672–680. [Google Scholar] [CrossRef]
- Kharouf, N.; Eid, A.; Hardan, L.; Bourgi, R.; Arntz, Y.; Jmal, H.; Foschi, F.; Sauro, S.; Ball, V.; Haikel, Y.; et al. Antibacterial and bonding properties of universal adhesive dental polymers doped with pyrogallol. Polymers 2021, 13, 1538. [Google Scholar] [CrossRef]
- Vivanco, R.G.; Cardoso, R.S.; Sousa, A.B.; Chinelatti, M.A.; de Freitas Vincenti, S.A.; Tonani-Torrieri, R.; Pires-de, F.D. Effect of thermo-mechanical cycling and chlorhexidine on the bond strength of universal adhesive system to dentin. Heliyon 2020, 6, e03871. [Google Scholar] [CrossRef] [PubMed]
- Kimyai, S.; Mohammadi, N.; Bahari, M.; Pesyanian, E.; Pesyanian, F. Effect of Cavity Disinfection with Chlorhexidine on Marginal Gap of Class V Composite Restorations Bonded with a Universal Adhesive Using Self-Etch and Etch-and-Rinse Bonding Strategy. Front. Dent. 2020, 17, 1. [Google Scholar] [CrossRef] [PubMed]
- Hosaka, K.; Nakajima, M.; Monticelli, F.; Carrilho, M.; Yamauti, M.; Aksornmuang, J. Influence of hydrostatic pulpal pressure on the microtensile bond strength of all-in-one self-etching adhesives. J. Adhes. Dent. 2007, 9, 437–442. [Google Scholar] [PubMed]
- Guan, R.; Takagaki, T.; Matsui, N.; Sato, T.; Burrow, M.F.; Palamara, J.; Nikaido, T.; Tagami, J. Dentin bonding performance using Weibull statistics and evaluation of acid-base-resistant zone formation of recently introduced adhesives. Dent. Mater. J. 2016, 35, 684–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breschi, L.; Mazzoni, A.; Nato, F.; Carrilho, M.; Visintini, E.; Tjäderhane, L.; Ruggeri, A.; Tay, F.R.; Dorigo Ede, S.; Pashley, D.H. Chlorhexidine stabilizes the adhesive interface: A 2-year in vitro study. Dent. Mater. 2010, 26, 320–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tărăboanță, I.; Buhățel, D.; Brînză Concită, C.A.; Andrian, S.; Nica, I.; Tărăboanță-Gamen, A.C.; Brânzan, R.; Stoleriu, S. Evaluation of the Surface Roughness of Bulk-Fill Composite Resins after Submission to Acidic and Abrasive Aggressions. Biomedicines 2022, 10, 1008. [Google Scholar] [CrossRef] [PubMed]
- Sioustis, I.A.; Martu, M.A.; Aminov, L.; Pavel, M.; Cianga, P.; Kappenberg-Nitescu, D.C.; Luchian, I.; Solomon, S.M.; Martu, S. Salivary metalloproteinase-8 and metalloproteinase-9 evaluation in patients undergoing fixed orthodontic treatment before and after periodontal therapy. Int. J. Environ. Res. Public Health 2021, 18, 1583. [Google Scholar] [CrossRef]
- Lokhande, N.M.; Manjunath, S.H.; Patil, A.K.; Bawa, P.D.; Mahajan, R.; Mahajan, H. Effect of Different Cavity Disinfectants on Marginal Sealing Ability of a Seventh-generation Dentin Bonding Agent: An In Vitro Study. J. Contemp. Dent. Pract. 2020, 21, 242–248. [Google Scholar]
- Galo, R.; Marinho, M.T.; da Silva Telles, P.D.; Borsatto, M.C. Shear bond strength of the adhesive/dentin interface after different etching protocols. J. Conserv. Dent. 2021, 24, 393. [Google Scholar] [CrossRef]
- Costa, A.R.; Naves, L.Z.; Garcia-Godoy, F.; Tsuzuki, F.M.; Correr, A.B.; Correr-Sobrinho, L.; Puppin-Rontani, R.M. CHX stabilizes the resin/demineralized dentin interface. Braz. Dent. J. 2021, 32, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Scarabello Stape, T.H.; Menezes, M.D.; Barreto, B.D.; Naves, L.Z.; Baggio Aguiar, F.H.; Quagliatto, P.S.; Marcondes Martins, L.R. Influence of chlorhexidine on dentin adhesive interface micromorphology and nanoleakage expression of resin cements. Microsc. Res. Tech. 2013, 76, 788–794. [Google Scholar] [CrossRef]
- Bin-Shuwaish, M.S.; AlHussaini, A.A.; AlHudaithy, L.H.; AlDukhiel, S.A.; Al-Jamhan, A.S. An in vitro evaluation of microleakage of resin based composites bonded to chlorhexidine-pretreated dentin by different protocols of a universal adhesive system. Saudi. Dent. J. 2021, 33, 503–510. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Manufacturer | Type | Batch no. | Composition |
|---|---|---|---|---|
| Single Bond Universal | 3M ESPE, St. Paul, MN, USA | Universal Adhesive | 7601156 | 10-MDP phosphate monomer, Vitrebond copolymer, HEMA, dimethacrylate resins, filler, silan, initiatiors, ethanol, water |
| Filtek One Bulk Fill Restorative | 3M ESPE, St. Paul, MN, USA | Bulk Fill composite resin | NC90177 | Bis-GMA, UDMA, Bis-EMA, TEGDMA, EDMAB, silica/zirconia, YbF3 |
| GROUP | SUBGROUP | ||||||
|---|---|---|---|---|---|---|---|
| I | A | Control group (n = 20) | Etch-and-rinse technique |  | Adhesive | ||
| B | Study group (n = 20) | Etch-and-rinse technique |  | Pretreatment with 2% Chlorhexidine solution | | Adhesive | |
| II | A | Control group (n = 20) | Self-etch technique | | Adhesive | ||
| B | Study group (n = 20) | Self-etch technique | | Pretreatment with 2% Chlorhexidine solution | | Adhesive | |
| Oclusal | Cervical | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| subgroups | subgroups | ||||||||
| IA | IB | IIA | IIB | IA | IB | IIA | IIB | ||
| IA | - | * 0.416 | * 0.816 | * 0.629 | A | - | * 0.731 | * 0.748 | * 0.867 |
| IB | * 0.416 | - | * 0.451 | * 0.399 | B | * 0.731 | - | * 0.859 | * 0.813 |
| IIA | * 0.816 | * 0.451 | - | * 0.653 | C | * 0.748 | * 0.859 | - | * 0.639 |
| IIB | * 0.629 | * 0.399 | * 0.653 | - | D | * 0.867 | * 0.813 | * 0.639 | - |
| Subgroups | IA | IB | IIA | IIB |
|---|---|---|---|---|
| Cervical | ||||
| Occlusal | ** 0.001 | * 0.473 | * 0.143 | * 0.075 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boaru, M.-O.; Tărăboanță, I.; Stoleriu, S.; Andrian, S.; Pancu, G.; Nica, I.; Sufaru, I.-G.; Iovan, G. The Influence of Chlorhexidine Gluconate Dentine Pre-Treatment on Adhesive Interface and Marginal Sealing. Medicina 2023, 59, 278. https://doi.org/10.3390/medicina59020278
Boaru M-O, Tărăboanță I, Stoleriu S, Andrian S, Pancu G, Nica I, Sufaru I-G, Iovan G. The Influence of Chlorhexidine Gluconate Dentine Pre-Treatment on Adhesive Interface and Marginal Sealing. Medicina. 2023; 59(2):278. https://doi.org/10.3390/medicina59020278
Chicago/Turabian StyleBoaru, Mihai-Octavian, Ionuț Tărăboanță, Simona Stoleriu, Sorin Andrian, Galina Pancu, Irina Nica, Irina-Georgeta Sufaru, and Gianina Iovan. 2023. "The Influence of Chlorhexidine Gluconate Dentine Pre-Treatment on Adhesive Interface and Marginal Sealing" Medicina 59, no. 2: 278. https://doi.org/10.3390/medicina59020278