
Airway and Respiratory Devices in the Prevention of Ventilator-Associated Pneumonia

Abstract
:1. Introduction
2. Subglottic Secretion Drainage
3. Cuff Shape and Material
4. Continuous Cuff Pressure Control
5. Low-Volume Low-Pressure Cuff
6. Coated Endotracheal Tubes and Mucus Shaver
7. Heat and Moisture Exchangers
8. Ventilator Circuit Change
9. Closed Tracheal Suctioning System
10. Discussion
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martin-Loeches, I.; Povoa, P.; Rodriguez, A.; Curcio, D.; Suarez, D.; Mira, J.P.; Cordero, M.L.; Lepecq, R.; Girault, C.; Candeias, C. Incidence and prognosis of ventilator-associated tracheobronchitis (TAVeM): A multicentre, prospective, observational study. Lancet Respir. Med. 2015, 3, 859–868. [Google Scholar] [CrossRef] [PubMed]
- Melsen, W.G.; Rovers, M.M.; Groenwold, R.H.; Bergmans, D.C.; Camus, C.; Bauer, T.T.; Hanisch, E.W.; Klarin, B.; Koeman, M.; Krueger, W.A. Attributable mortality of ventilator-associated pneumonia: A meta-analysis of individual patient data from randomised prevention studies. Lancet Infect. Dis. 2013, 13, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Papazian, L.; Klompas, M.; Luyt, C.E. Ventilator-associated pneumonia in adults: A narrative review. Intensive Care Med. 2020, 46, 888–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Barat, L.; Torres, A. Biofilms in ventilator-associated pneumonia. Future Microbiol. 2016, 11, 1599–1610. [Google Scholar] [CrossRef] [PubMed]
- Perkins, S.D.; Woeltje, K.F.; Angenent, L.T. Endotracheal tube biofilm inoculation of oral flora and subsequent colonization of opportunistic pathogens. Int. J. Med. Microbiol. 2010, 300, 503–511. [Google Scholar] [CrossRef]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of Adults with Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef] [Green Version]
- Martin-Loeches, I.; Deja, M.; Koulenti, D.; Dimopoulos, G.; Marsh, B.; Torres, A.; Niederman, M.S.; Rello, J. Potentially resistant microorganisms in intubated patients with hospital-acquired pneumonia: The interaction of ecology, shock and risk factors. Intensive Care Med. 2013, 39, 672–681. [Google Scholar] [CrossRef]
- Klompas, M. Prevention of Intensive Care Unit-Acquired Pneumonia. Semin. Respir. Crit. Care Med. 2019, 40, 548–557. [Google Scholar] [CrossRef]
- Hsieh, S.J.; Otusanya, O.; Gershengorn, H.B.; Hope, A.A.; Dayton, C.; Levi, D.; Garcia, M.; Prince, D.; Mills, M.; Fein, D.; et al. Staged Implementation of Awakening and Breathing, Coordination, Delirium Monitoring and Management, and Early Mobilization Bundle Improves Patient Outcomes and Reduces Hospital Costs. Crit. Care Med. 2019, 47, 885–893. [Google Scholar] [CrossRef]
- Klompas, M.; Kalil, A.C. Rethinking Ventilator Bundles. Crit. Care Med. 2018, 46, 1201–1203. [Google Scholar] [CrossRef]
- Muscedere, J.; Rewa, O.; McKechnie, K.; Jiang, X.; Laporta, D.; Heyland, D.K. Subglottic secretion drainage for the prevention of ventilator-associated pneumonia: A systematic review and meta-analysis. Crit. Care Med. 2011, 39, 1985–1991. [Google Scholar] [CrossRef]
- Safdar, N.; Crnich, C.J.; Maki, D.G. The pathogenesis of ventilator-associated pneumonia: Its relevance to developing effective strategies for prevention. Respir. Care 2005, 50, 725–739. [Google Scholar]
- Dullenkopf, A.; Gerber, A.; Weiss, M. Fluid leakage past tracheal tube cuffs: Evaluation of the new Microcuff endotracheal tube. Intensive Care Med. 2003, 29, 1849–1853. [Google Scholar] [CrossRef] [Green Version]
- Mahul, P.; Auboyer, C.; Jospe, R.; Ros, A.; Guerin, C.; el Khouri, Z.; Galliez, M.; Dumont, A.; Gaudin, O. Prevention of nosocomial pneumonia in intubated patients: Respective role of mechanical subglottic secretions drainage and stress ulcer prophylaxis. Intensive Care Med. 1992, 18, 20–25. [Google Scholar] [CrossRef]
- Leasure, A.R.; Stirlen, J.; Lu, S.H. Prevention of ventilator-associated pneumonia through aspiration of subglottic secretions: A systematic review and meta-analysis. Dimens. Crit. Care Nurs. 2012, 31, 102–117. [Google Scholar] [CrossRef]
- Klompas, M.; Branson, R.; Cawcutt, K.; Crist, M.; Eichenwald, E.C.; Greene, L.R.; Lee, G.; Maragakis, L.L.; Powell, K.; Priebe, G.P.; et al. Strategies to prevent ventilator-associated pneumonia, ventilator-associated events, and nonventilator hospital-acquired pneumonia in acute-care hospitals: 2022 Update. Infect. Control Hosp. Epidemiol. 2022, 43, 687–713. [Google Scholar] [CrossRef]
- Alvarez-Lerma, F.; Palomar-Martinez, M.; Sanchez-Garcia, M.; Martinez-Alonso, M.; Alvarez-Rodriguez, J.; Lorente, L.; Arias-Rivera, S.; García, R.; Gordo, F.; Añón, J.M.; et al. Prevention of Ventilator-Associated Pneumonia: The Multimodal Approach of the Spanish ICU “Pneumonia Zero” Program. Crit. Care Med. 2018, 46, 181–188. [Google Scholar] [CrossRef] [Green Version]
- Leone, M.; Bouadma, L.; Bouhemad, B.; Brissaud, O.; Dauger, S.; Gibot, S.; Hraiech, S.; Jung, B.; Kipnis, E.; Launey, Y.; et al. Hospital-acquired pneumonia in ICU. Anaesth. Crit. Care Pain Med. 2018, 37, 83–98. [Google Scholar] [CrossRef]
- Caroff, D.A.; Li, L.; Muscedere, J.; Klompas, M. Subglottic Secretion Drainage and Objective Outcomes: A Systematic Review and Meta-Analysis. Crit. Care Med. 2016, 44, 830–840. [Google Scholar] [CrossRef]
- Mao, Z.; Gao, L.; Wang, G.; Liu, C.; Zhao, Y.; Gu, W.; Kang, H.; Zhou, F. Subglottic secretion suction for preventing ventilator-associated pneumonia: An updated meta-analysis and trial sequential analysis. Crit. Care 2016, 20, 353. [Google Scholar] [CrossRef] [Green Version]
- Pozuelo-Carrascosa, D.P.; Herraiz-Adillo, A.; Alvarez-Bueno, C.; Anon, J.M.; Martinez-Vizcaino, V.; Cavero-Redondo, I. Subglottic secretion drainage for preventing ventilator-associated pneumonia: An overview of systematic reviews and an updated meta-analysis. Eur. Respir. Rev. 2020, 29, 190107. [Google Scholar] [CrossRef] [PubMed]
- Pozuelo-Carrascosa, D.P.; Klompas, M.; Alvarez-Bueno, C.; Anon, J.M.; Martinez-Vizcaino, V.; Cavero-Redondo, I.; Herráiz-Adillo, A. Correction to subglottic secretion drainage for preventing ventilator-associated pneumonia: An overview of systematic reviews and an updated meta-analysis. Eur. Respir. Rev. 2022, 31, 220013. [Google Scholar] [CrossRef] [PubMed]
- Damas, P.; Frippiat, F.; Ancion, A.; Canivet, J.L.; Lambermont, B.; Layios, N.; Massion, P.; Morimont, P.; Nys, M.; Piret, S.; et al. Prevention of ventilator-associated pneumonia and ventilator-associated conditions: A randomized controlled trial with subglottic secretion suctioning. Crit. Care Med. 2015, 43, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Berra, L.; De Marchi, L.; Panigada, M.; Yu, Z.X.; Baccarelli, A.; Kolobow, T. Evaluation of continuous aspiration of subglottic secretion in an in vivo study. Crit. Care Med. 2004, 32, 2071–2078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valles, J.; Millan, S.; Diaz, E.; Castanyer, E.; Gallardo, X.; Martin-Loeches, I.; Andreu, M.; Prenafeta, M.; Saludes, P.; Lema, J.; et al. Incidence of airway complications in patients using endotracheal tubes with continuous aspiration of subglottic secretions. Ann. Intensive Care. 2017, 7, 109. [Google Scholar] [CrossRef] [Green Version]
- Rouze, A.; Martin-Loeches, I.; Nseir, S. Airway Devices in Ventilator-Associated Pneumonia Pathogenesis and Prevention. Clin. Chest Med. 2018, 39, 775–783. [Google Scholar] [CrossRef]
- Deem, S.; Treggiari, M.M. New endotracheal tubes designed to prevent ventilator-associated pneumonia: Do they make a difference? Respir. Care 2010, 55, 1046–1055. [Google Scholar]
- Young, P.J.; Pakeerathan, S.; Blunt, M.C.; Subramanya, S. A low-volume, low-pressure tracheal tube cuff reduces pulmonary aspiration. Crit. Care Med. 2006, 34, 632–639. [Google Scholar] [CrossRef] [Green Version]
- Maertens, B.; Blot, K.; Blot, S. Prevention of Ventilator-Associated and Early Postoperative Pneumonia Through Tapered Endotracheal Tube Cuffs: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Crit. Care Med. 2018, 46, 316–323. [Google Scholar] [CrossRef]
- Jaillette, E.; Girault, C.; Brunin, G.; Zerimech, F.; Behal, H.; Chiche, A.; Broucqsault-Dedrie, C.; Fayolle, C.; Minacori, F.; Alves, I.; et al. Impact of tapered-cuff tracheal tube on microaspiration of gastric contents in intubated critically ill patients: A multicenter cluster-randomized cross-over controlled trial. Intensive Care Med. 2017, 43, 1562–1571. [Google Scholar] [CrossRef]
- Gentile, M.A.; Siobal, M.S. Are specialized endotracheal tubes and heat-and-moisture exchangers cost-effective in preventing ventilator associated pneumonia? Respir. Care 2010, 55, 184–196. [Google Scholar]
- Blot, S.I.; Rello, J.; Koulenti, D. The value of polyurethane-cuffed endotracheal tubes to reduce microaspiration and intubation-related pneumonia: A systematic review of laboratory and clinical studies. Crit. Care 2016, 20, 203. [Google Scholar] [CrossRef] [Green Version]
- Diaz, E.; Rodriguez, A.H.; Rello, J. Ventilator-associated pneumonia: Issues related to the artificial airway. Respir. Care 2005, 50, 900–906. [Google Scholar]
- Rouze, A.; Jaillette, E.; Poissy, J.; Preau, S.; Nseir, S. Tracheal Tube Design and Ventilator-Associated Pneumonia. Respir. Care 2017, 62, 1316–1323. [Google Scholar] [CrossRef]
- Valencia, M.; Ferrer, M.; Farre, R.; Navajas, D.; Badia, J.R.; Nicolas, J.M.; Torres, A. Automatic control of tracheal tube cuff pressure in ventilated patients in semirecumbent position: A randomized trial. Crit. Care Med. 2007, 35, 1543–1549. [Google Scholar] [CrossRef]
- Maertens, B.; Lin, F.; Chen, Y.; Rello, J.; Lathyris, D.; Blot, S. Effectiveness of Continuous Cuff Pressure Control in Preventing Ventilator-Associated Pneumonia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Crit. Care Med. 2022, 50, 1430–1439. [Google Scholar] [CrossRef]
- Mietto, C.; Pinciroli, R.; Patel, N.; Berra, L. Ventilator associated pneumonia: Evolving definitions and preventive strategies. Respir. Care 2013, 58, 990–1007. [Google Scholar] [CrossRef] [Green Version]
- Fernandez, J.F.; Levine, S.M.; Restrepo, M.I. Technologic advances in endotracheal tubes for prevention of ventilator-associated pneumonia. Chest 2012, 142, 231–238. [Google Scholar] [CrossRef] [Green Version]
- Berra, L.; Kolobow, T.; Laquerriere, P.; Pitts, B.; Bramati, S.; Pohlmann, J.; Marelli, C.; Panzeri, M.; Brambillasca, P.; Villa, F.; et al. Internally coated endotracheal tubes with silver sulfadiazine in polyurethane to prevent bacterial colonization: A clinical trial. Intensive Care Med. 2008, 34, 1030–1037. [Google Scholar] [CrossRef]
- Kollef, M.H.; Afessa, B.; Anzueto, A.; Veremakis, C.; Kerr, K.M.; Margolis, B.D.; Craven, D.E.; Roberts, P.R.; Arroliga, A.C.; Hubmayr, R.D.; et al. Silver-coated endotracheal tubes and incidence of ventilator-associated pneumonia: The NASCENT randomized trial. JAMA 2008, 300, 805–813. [Google Scholar] [CrossRef] [Green Version]
- Tokmaji, G.; Vermeulen, H.; Muller, M.C.; Kwakman, P.H.; Schultz, M.J.; Zaat, S.A. Silver-coated endotracheal tubes for prevention of ventilator-associated pneumonia in critically ill patients. Cochrane Database Syst. Rev. 2015, 2015, CD009201. [Google Scholar] [CrossRef] [PubMed]
- Berra, L.; Coppadoro, A.; Bittner, E.A.; Kolobow, T.; Laquerriere, P.; Pohlmann, J.R.; Bramati, S.; Moss, J.; Pesenti, A. A clinical assessment of the Mucus Shaver: A device to keep the endotracheal tube free from secretions. Crit. Care Med. 2012, 40, 119–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinciroli, R.; Mietto, C.; Piriyapatsom, A.; Chenelle, C.T.; Thomas, J.G.; Pirrone, M.; Bry, L.; Wojtkiewicz, G.R.; Nahrendorf, M.P.; Kacmarek, R.M.; et al. Endotracheal Tubes Cleaned with a Novel Mechanism for Secretion Removal: A Randomized Controlled Clinical Study. Respir. Care 2016, 61, 1431–1439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hess, D.R.; Kallstrom, T.J.; Mottram, C.D.; Myers, T.R.; Sorenson, H.M.; Vines, D.L. Care of the ventilator circuit and its relation to ventilator-associated pneumonia. Respir. Care 2003, 48, 869–879. [Google Scholar] [PubMed]
- Branson, R.D. The ventilator circuit and ventilator-associated pneumonia. Respir. Care 2005, 50, 774–785. [Google Scholar]
- Siempos, I.I.; Vardakas, K.Z.; Kopterides, P.; Falagas, M.E. Impact of passive humidification on clinical outcomes of mechanically ventilated patients: A meta-analysis of randomized controlled trials. Crit. Care Med. 2007, 35, 2843–2851. [Google Scholar]
- Craven, D.E.; Connolly, M.G., Jr.; Lichtenberg, D.A.; Primeau, P.J.; McCabe, W.R. Contamination of mechanical ventilators with tubing changes every 24 or 48 hours. N. Engl. J. Med. 1982, 306, 1505–1509. [Google Scholar] [CrossRef]
- Han, J.; Liu, Y. Effect of ventilator circuit changes on ventilator-associated pneumonia: A systematic review and meta-analysis. Respir. Care 2010, 55, 467–474. [Google Scholar]
- Jongerden, I.P.; Rovers, M.M.; Grypdonck, M.H.; Bonten, M.J. Open and closed endotracheal suction systems in mechanically ventilated intensive care patients: A meta-analysis. Crit. Care Med. 2007, 35, 260–270. [Google Scholar] [CrossRef]
- Kuriyama, A.; Umakoshi, N.; Fujinaga, J.; Takada, T. Impact of closed versus open tracheal suctioning systems for mechanically ventilated adults: A systematic review and meta-analysis. Intensive Care Med. 2015, 41, 402–411. [Google Scholar] [CrossRef]
- Siempos, I.I.; Vardakas, K.Z.; Falagas, M.E. Closed tracheal suction systems for prevention of ventilator-associated pneumonia. Br. J. Anaesth. 2008, 100, 299–306. [Google Scholar] [CrossRef]


{kind=link}
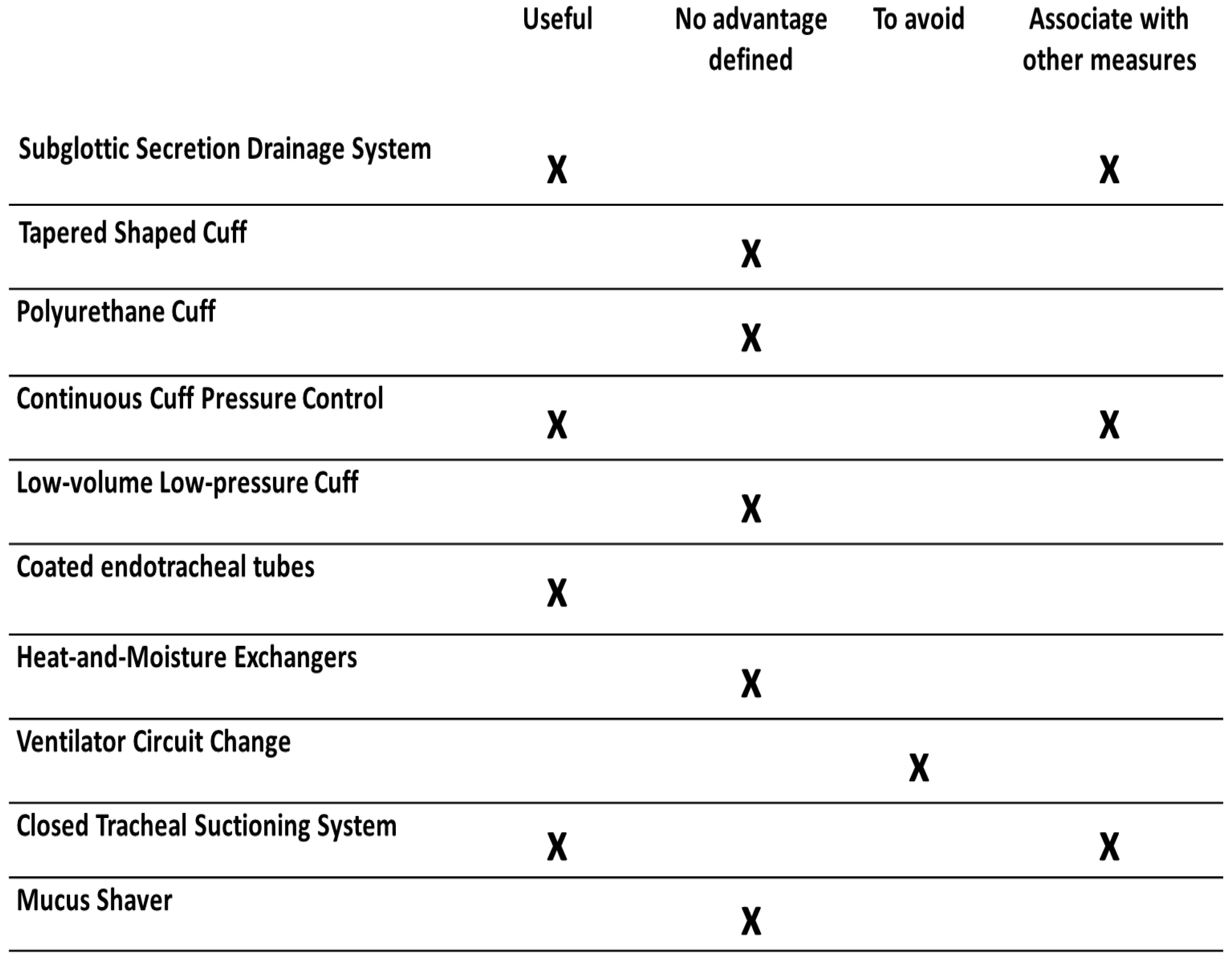
| Devices | Advantages | Limitations |
|---|---|---|
| Subglottic Secretion Drainage System | Reduced incidence of VAP. Recommended in VAP prevention guidelines. | No reduction in the duration of MV, ICU length of stay, or mortality. |
| Tapered-Shaped Cuff | No advantages. | No reduction in the incidence of VAP, duration of MV, ICU length of stay, or mortality. |
| Polyurethane Cuff | Low evidence in the prevention of VAP. Additional data required. | Inaccurate cuff pressure measurement due to cuff condensation. |
| Continuous Cuff Pressure Control | Reduced risk of VAP, duration of MV, or ICU length of stay. | No effect on mortality. Cost-effectiveness not evaluated. No definite recommendation. |
| Low-volume Low-pressure Cuff | Reduction of microaspiration. Lower VAP rates in small clinical trials. | Evidence from small clinical trials. No definite recommendation. |
| Coated endotracheal tubes | Less bacterial colonization. Lower VAP rates. | Effectiveness decreases over time on MV. No definite recommendation. |
| Heat and Moisture Exchangers | No advantages. | No reduction in the incidence of VAP. Associated with a higher risk of atelectasis and increased dead space. Not recommended. |
| Ventilator Circuit Change | No advantages. | Scheduled change associated with risk of VAP. Not recommended. |
| Closed Tracheal Suctioning System | Lower VAP rates. | No reduction in the duration of MV, ICU length of stay, or mortality. No definite recommendation. |
| Mucus Shaver | Allows the removal of mucus and secretions from inside the ETT. | No impact on ETT colonization. No reduction in the incidence of VAP. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coelho, L.; Moniz, P.; Guerreiro, G.; Póvoa, P. Airway and Respiratory Devices in the Prevention of Ventilator-Associated Pneumonia. Medicina 2023, 59, 199. https://doi.org/10.3390/medicina59020199
Coelho L, Moniz P, Guerreiro G, Póvoa P. Airway and Respiratory Devices in the Prevention of Ventilator-Associated Pneumonia. Medicina. 2023; 59(2):199. https://doi.org/10.3390/medicina59020199
Chicago/Turabian StyleCoelho, Luis, Patricia Moniz, Gonçalo Guerreiro, and Pedro Póvoa. 2023. "Airway and Respiratory Devices in the Prevention of Ventilator-Associated Pneumonia" Medicina 59, no. 2: 199. https://doi.org/10.3390/medicina59020199