
An Observational Study of 147 Psoriasis Patients: Overweightness and Obesity as a Significant Clinical Factors Correlated with Psoriasis
 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.3. Statistical Analysis
3. Results
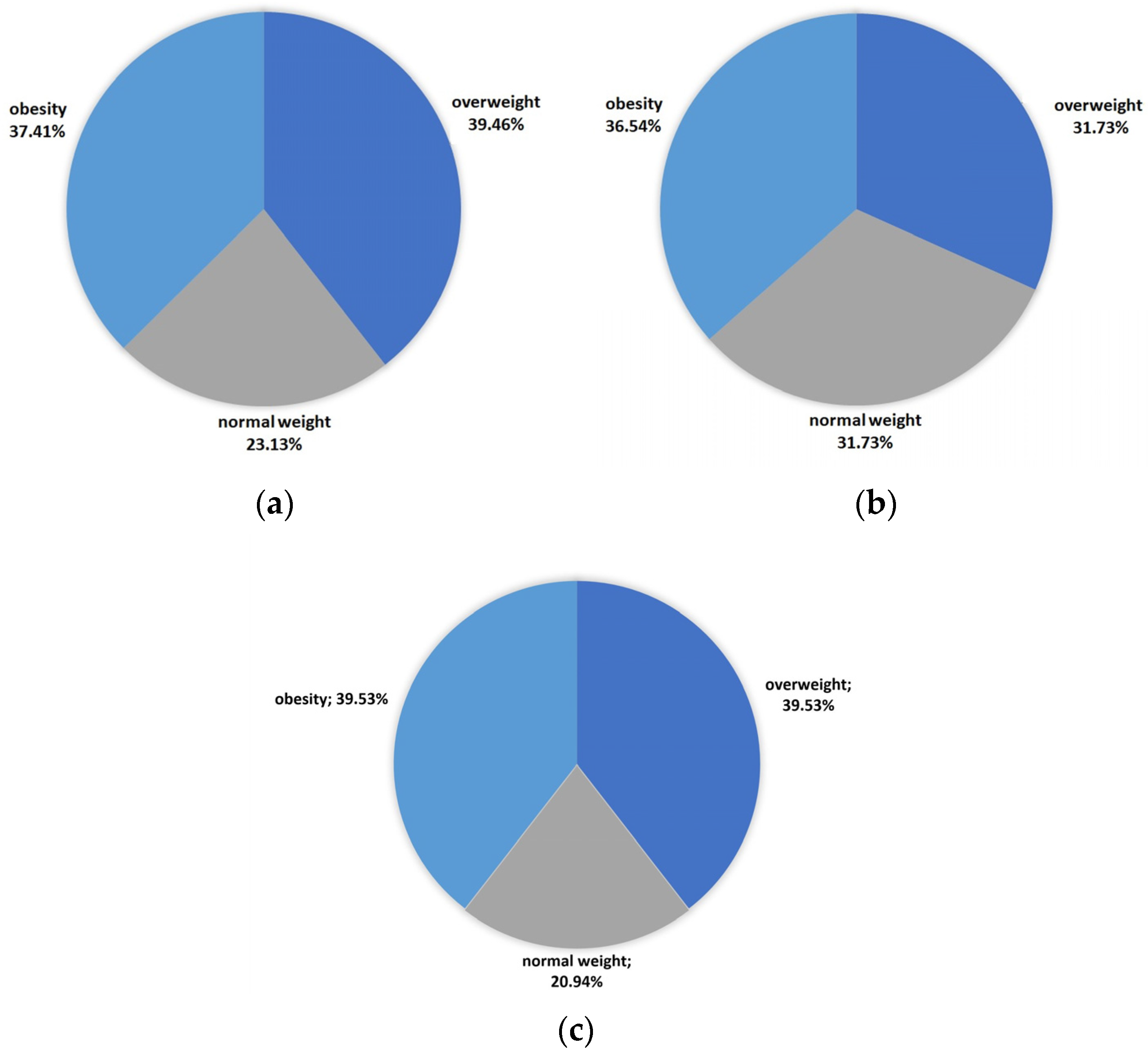
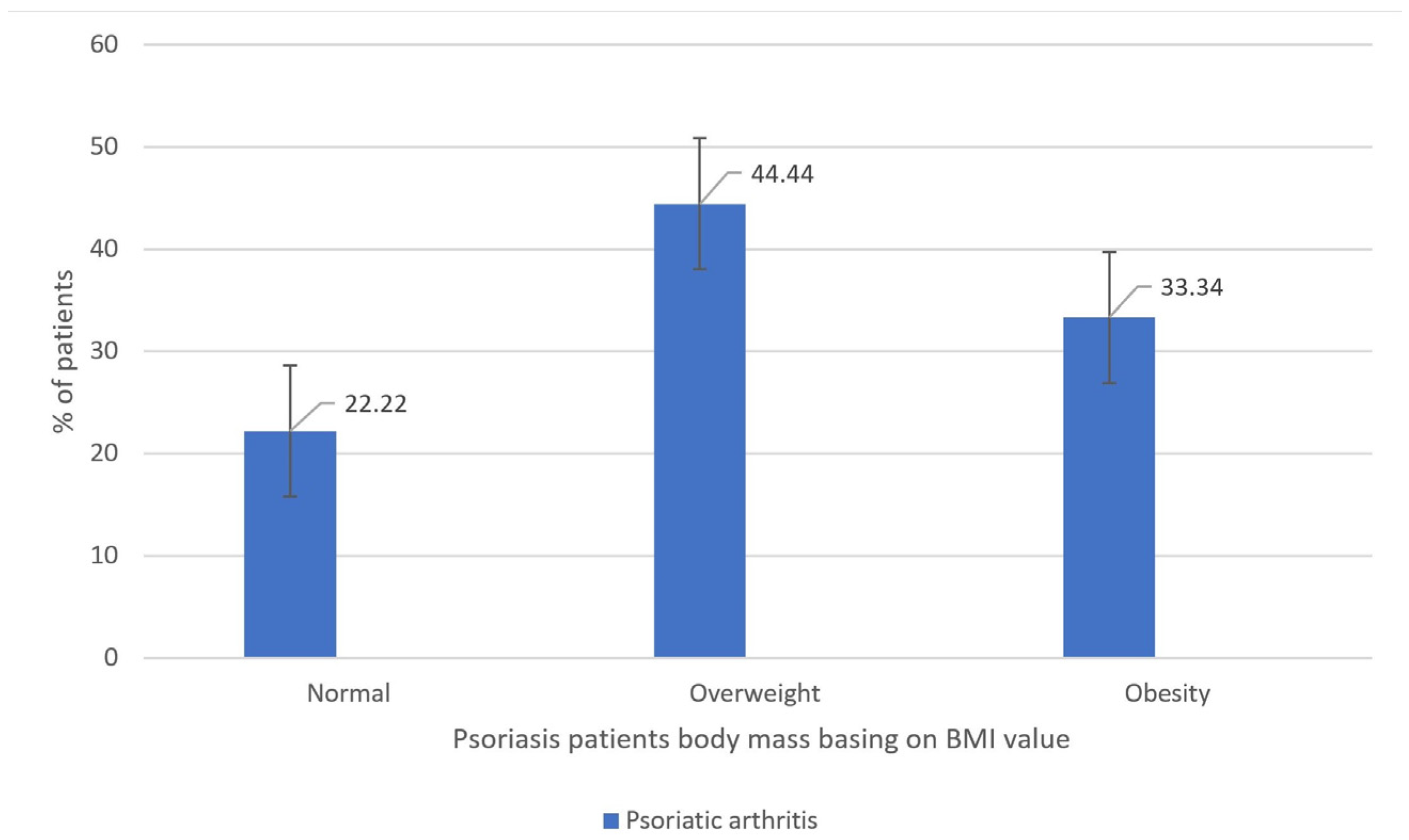
3.1. Analysis of Overweightness and Obesity Prevalences among Psoriatic Patients
3.2. Analysis of the Role of Environmental Factors in Psoriatic Patients
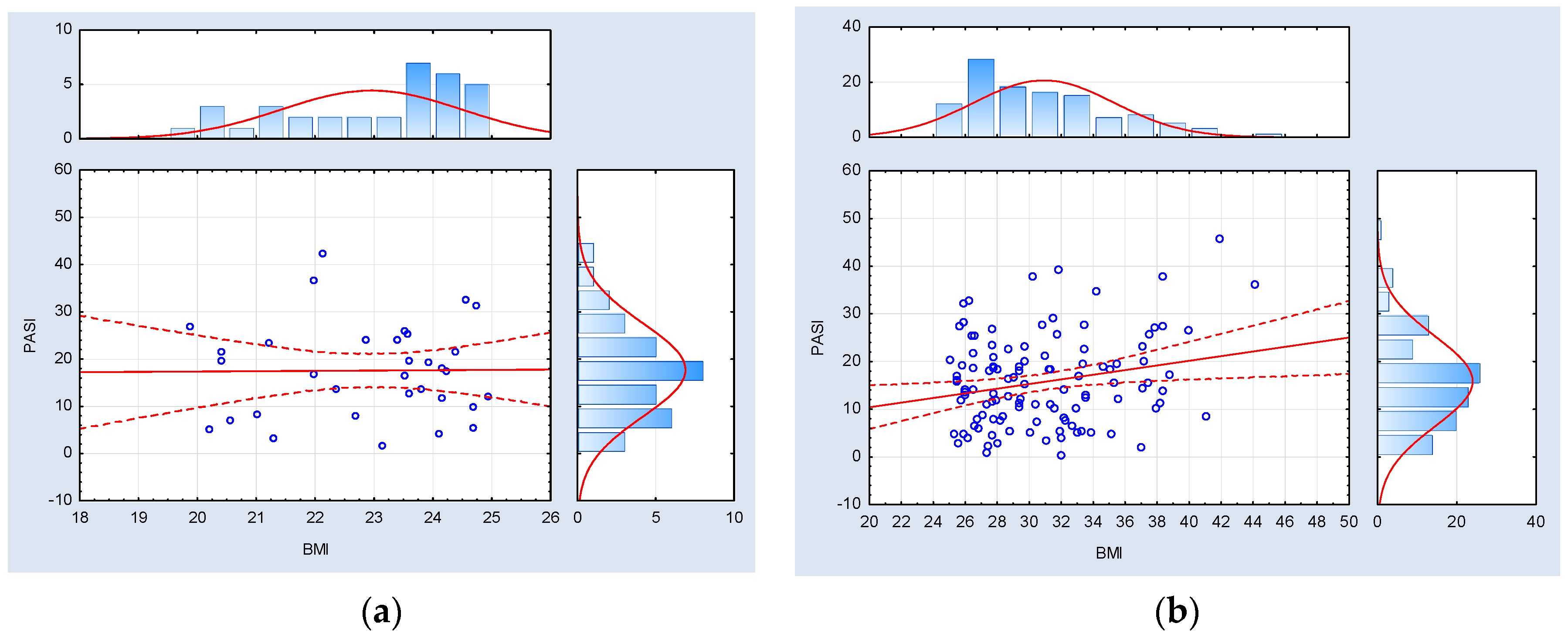
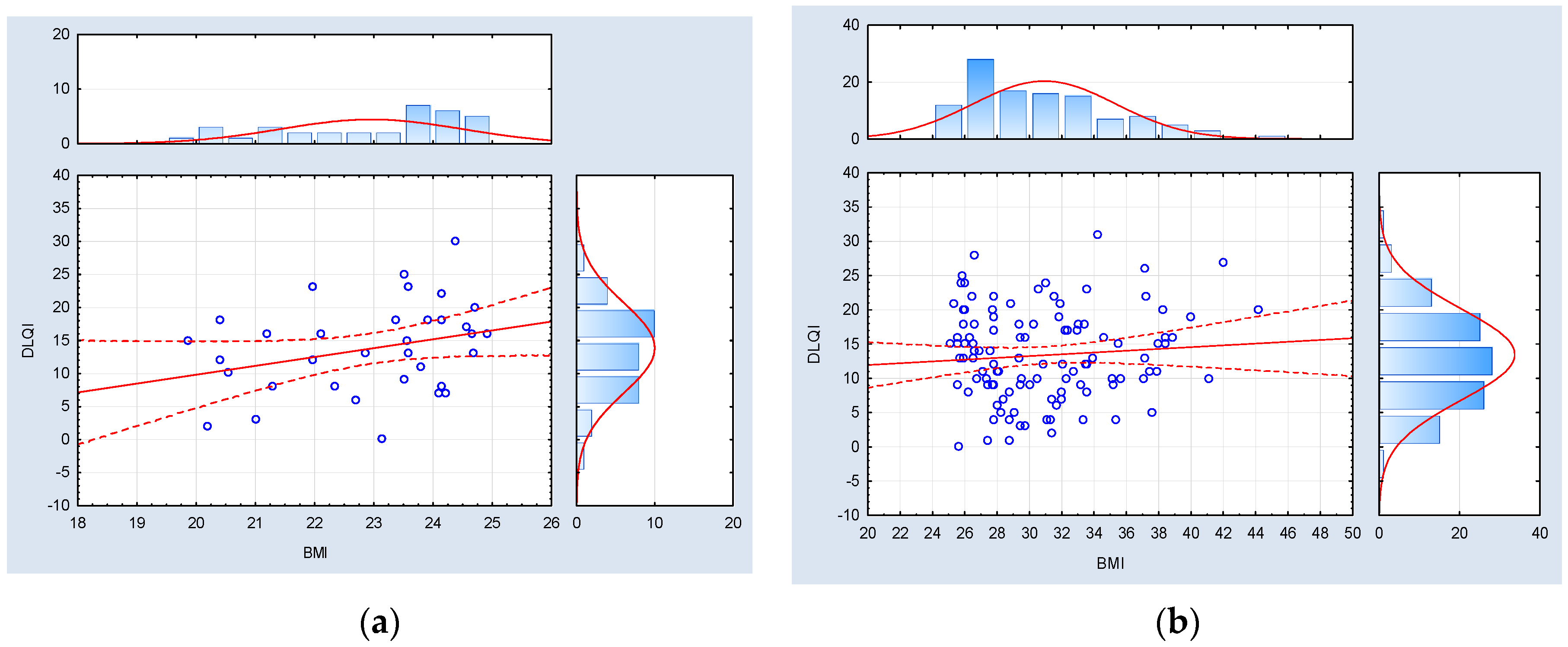
3.3. Analysis of the Body Mass Influence on Psoriasis Disease Course and Severity
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parisi, R.; Iskandar, I.Y.K.; Kontopantelis, E.; Augustin, M.; Griffiths, C.E.M.; Ashcroft, D.M. Global Psoriasis Atlas. National, regional, and worldwide epidemiology of psoriasis: Systematic analysis and modelling study. BMJ 2020, 369, m1590. [Google Scholar] [CrossRef]
- Kamiya, K.; Kishimoto, M.; Sugai, J.; Komine, M.; Ohtsuki, M. Risk Factors for the Development of Psoriasis. Int. J. Mol. Sci. 2019, 20, 4347. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.; Kirby, B. Psoriasis is a systemic disease with multiple cardiovascular and metabolic comorbidities. Dermatol. Clin. 2015, 33, 41–55. [Google Scholar] [CrossRef] [PubMed]
- Boehncke, W.H. Systemic Inflammation and Cardiovascular Comorbidity in Psoriasis Patients: Causes and Consequences. Front. Immunol. 2018, 9, 579. [Google Scholar] [CrossRef] [PubMed]
- Barros, G.; Duran, P.; Vera, I.; Bermúdez, V. Exploring the Links between Obesity and Psoriasis: A Comprehensive Review. Int. J. Mol. Sci. 2022, 23, 7499. [Google Scholar] [CrossRef]
- Norden, A.; Rekhtman, S.; Strunk, A.; Garg, A. Risk of psoriasis according to body mass index: A retrospective cohort analysis. J. Am. Acad. Dermatol. 2022, 86, 1020–1026. [Google Scholar] [CrossRef]
- El-Boghdady, N.A.; Ismail, M.F.; Abd-Alhameed, M.F.; Ahmed, A.S.; Ahmed, H.H. Bidirectional Association Between Psoriasis and Obesity: Benefits and Risks. J. Interferon Cytokine Res. 2018, 38, 12–19. [Google Scholar] [CrossRef]
- Owczarczyk-Saczonek, A.; Purzycka-Bohdan, D.; Nedoszytko, B.; Reich, A.; Szczerkowska-Dobosz, A.; Bartosińska, J.; Batycka-Baran, A.; Czajkowski, R.; Dobrucki, I.T.; Dobrucki, L.W.; et al. Pathogenesis of psoriasis in the “omic” era. Part III. Metabolic disorders, metabolomics, nutrigenomics in psoriasis. Postep. Dermatol. Alergol. 2020, 37, 452–467. [Google Scholar] [CrossRef]
- Takeshita, J.; Grewal, S.; Langan, S.M.; Mehta, N.N.; Ogdie, A.; Van Voorhees, A.S.; Gelfand, J.M. Psoriasis and comorbid diseases: Epidemiology. J. Am. Acad. Dermatol. 2017, 76, 377–390. [Google Scholar] [CrossRef]
- Abuabara, K.; Azfar, R.S.; Shin, D.B.; Neimann, A.L.; Troxel, A.B.; Gelfand, J.M. Cause-specific mortality in patients with severe psoriasis: A population-based cohort study in the UK. Br. J. Dermatol. 2010, 163, 586–592. [Google Scholar] [CrossRef]
- Gisondi, P.; Del Giglio, M.; Girolomoni, G. Considerations for Systemic Treatment of Psoriasis in Obese Patients. Am. J. Clin. Dermatol. 2016, 17, 609–615. [Google Scholar] [CrossRef]
- Puig, L. Obesity and psoriasis: Body weight and body mass index influence the response to biological treatment. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 1007–1011. [Google Scholar] [CrossRef]
- Camela, E.; Potestio, L.; Fabbrocini, G.; Pallotta, S.; Megna, M. The holistic approach to psoriasis patients with comorbidities: The role of investigational drugs. Expert Opin. Investig. Drugs 2023, 32, 537–552. [Google Scholar] [CrossRef]
- Duchnik, E.; Kruk, J.; Tuchowska, A.; Marchlewicz, M. The Impact of Diet and Physical Activity on Psoriasis: A Narrative Review of the Current Evidence. Nutrients 2023, 15, 840. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Sim, N.; Fotouhi, A.; Daveluy, S. Vegan Diet in Dermatology: A Review. J. Clin. Med. 2023, 12, 5800. [Google Scholar] [CrossRef] [PubMed]
- Pereira-Santos, M.; Costa, P.R.; Assis, A.M.; Santos, C.A.; Santos, D.B. Obesity and vitamin D deficiency: A systematic review and meta-analysis. Obes. Rev. 2015, 16, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Karampinis, E.; Goudouras, G.; Ntavari, N.; Bogdanos, D.P.; Roussaki-Schulze, A.V.; Zafiriou, E. Serum vitamin D levels can be predictive of psoriasis flares up after COVID-19 vaccination: A retrospective case control study. Front. Med. 2023, 10, 1203426. [Google Scholar] [CrossRef] [PubMed]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut Off Points. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023; Available online: https://www.ncbi.nlm.nih.gov/books/NBK541070/ (accessed on 21 October 2023).
- Mrowietz, U.; Kragballe, K.; Reich, K.; Spuls, P.; Griffiths, C.E.; Nast, A.; Franke, J.; Antoniou, C.; Arenberger, P.; Balieva, F.; et al. Definition of treatment goals for moderate to severe psoriasis: A European consensus. Arch. Dermatol. Res. 2011, 303, 1–10. [Google Scholar] [CrossRef]
- Finlay, A.Y.; Khan, G.K. Dermatology Life Quality Index (DLQI)—A simple practical measure for routine clinical use. Clin. Exp. Dermatol. 1994, 19, 210–216. [Google Scholar] [CrossRef]
- Purzycka-Bohdan, D.; Kisielnicka, A.; Zabłotna, M.; Nedoszytko, B.; Nowicki, R.J.; Reich, A.; Samotij, D.; Szczęch, J.; Krasowska, D.; Bartosińska, J.; et al. Chronic Plaque Psoriasis in Poland: Disease Severity, Prevalence of Comorbidities, and Quality of Life. J. Clin. Med. 2022, 11, 1254. [Google Scholar] [CrossRef]
- Chen, L.; Tsai, T.F. HLA-Cw6 and psoriasis. Br. J. Dermatol. 2018, 178, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Queiro, R.; Torre, J.C.; González, S.; López-Larrea, C.; Tinturé, T.; López-Lagunas, I. HLA antigens may influence the age of onset of psoriasis and psoriatic arthritis. J. Rheumatol. 2003, 30, 505–507. [Google Scholar]
- Stoś, K.; Rychlik, E.; Woźniak, A.; Ołtarzewski, M.; Jankowski, M.; Gujski, M.; Juszczyk, G. Prevalence and Sociodemographic Factors Associated with Overweight and Obesity among Adults in Poland: A 2019/2020 Nationwide Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2022, 19, 1502. [Google Scholar] [CrossRef] [PubMed]
- Jacobi, A.; Langenbruch, A.; Purwins, S.; Augustin, M.; Radtke, M.A. Prevalence of Obesity in Patients with Psoriasis: Results of the National Study PsoHealth3. Dermatology 2015, 231, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.; Devjani, S.; Collier, M.R.; Maul, J.T.; Wu, J.J. Association Between Psoriasis and Obesity Among US Adults in the 2009–2014 National Health and Nutrition Examination Survey. Cutis 2023, 112, 49–51. [Google Scholar] [CrossRef]
- Dai, Y.X.; Shen, Y.J.; Chou, Y.J.; Chang, Y.T.; Chen, T.J.; Li, C.P.; Wu, C.Y. Obesity, but Not Metabolic Diseases, Is Associated with Risk of Psoriasis: A Population-Based Cohort Study in Taiwan. Dermatology 2020, 236, 521–528. [Google Scholar] [CrossRef]
- Aune, D.; Snekvik, I.; Schlesinger, S.; Norat, T.; Riboli, E.; Vatten, L.J. Body mass index, abdominal fatness, weight gain and the risk of psoriasis: A systematic review and dose-response meta-analysis of prospective studies. Eur. J. Epidemiol. 2018, 33, 1163–1178. [Google Scholar] [CrossRef]
- Herédi, E.; Csordás, A.; Clemens, M.; Adám, B.; Gáspár, K.; Törőcsik, D.; Nagy, G.; Adány, R.; Gaál, J.; Remenyik, E.; et al. The prevalence of obesity is increased in patients with late compared with early onset psoriasis. Ann. Epidemiol. 2013, 23, 688–692. [Google Scholar] [CrossRef]
- Douroudis, K.; Ramessur, R.; Barbosa, I.A.; Baudry, D.; Duckworth, M.; Angit, C.; Capon, F.; Chung, R.; Curtis, C.J.; Di Meglio, P.; et al. Differences in Clinical Features and Comorbid Burden between HLA-C∗06:02 Carrier Groups in >9,000 People with Psoriasis. J. Investig. Dermatol. 2022, 142, 1617–1628.e10. [Google Scholar] [CrossRef]
- Solvin, Å.Ø.; Bjarkø, V.V.; Thomas, L.F.; Berrospi, P.; Hveem, K.; Saunes, M.; Åsvold, B.O.; Løset, M. Body Composition, Cardiometabolic Risk Factors and Comorbidities in Psoriasis and the Effect of HLA-C*06:02 Status: The HUNT Study, Norway. Acta Derm. Venereol. 2023, 103, adv5209. [Google Scholar] [CrossRef]
- Queiro, R.; Coto-Segura, P.; Braña, I.; Pino, M.; Burger, S. Potential Differences in the Cardiometabolic Risk Profile of Patients with Psoriatic Disease according to Their HLA-C∗06 Status. BioMed Res. Int. 2022, 2022, 1451193. [Google Scholar] [CrossRef]
- Brazzelli, V.; Carugno, A.; Alborghetti, A.; Grasso, V.; Cananzi, R.; Fornara, L.; De Silvestri, A.; Borroni, G. Prevalence, severity and clinical features of psoriasis in fingernails and toenails in adult patients: Italian experience. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 1354–1359. [Google Scholar] [CrossRef]
- Tłustochowicz, M.; Wierzba, W.; Marczak, M.; Tłustochowicz, W.; Śliwczyński, A.; Raciborski, F.; Kwiatkowska, B.; Brzozowska, M.; Jacyna, A.; Kisiel, B. Trends in psoriatic arthritis epidemiology in Poland. Rheumatol. Int. 2021, 41, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Zabotti, A.; De Lucia, O.; Sakellariou, G.; Batticciotto, A.; Cincinelli, G.; Giovannini, I.; Idolazzi, L.; Maioli, G.; Tinazzi, I.; Aletaha, D.; et al. Predictors, Risk Factors, and Incidence Rates of Psoriatic Arthritis Development in Psoriasis Patients: A Systematic Literature Review and Meta-Analysis. Rheumatol. Ther. 2021, 8, 1519–1534. [Google Scholar] [CrossRef]
- El Miedany, Y.; El Gaafary, M.; Youssef, S.; Ahmed, I.; Nasr, A. Tailored approach to early psoriatic arthritis patients: Clinical and ultrasonographic predictors for structural joint damage. Clin. Rheumatol. 2015, 34, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Soltani-Arabshahi, R.; Wong, B.; Feng, B.J.; Goldgar, D.E.; Duffin, K.C.; Krueger, G.G. Obesity in early adulthood as a risk factor for psoriatic arthritis. Arch. Dermatol. 2010, 146, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Green, A.; Shaddick, G.; Charlton, R.; Snowball, J.; Nightingale, A.; Smith, C.; Tillett, W.; McHugh, N.; PROMPT study group. Modifiable risk factors and the development of psoriatic arthritis in people with psoriasis. Br. J. Dermatol. 2020, 182, 714–720. [Google Scholar] [CrossRef]
- Porta, S.; Otero-Losada, M.; Kölliker Frers, R.A.; Cosentino, V.; Kerzberg, E.; Capani, F. Adipokines, Cardiovascular Risk, and Therapeutic Management in Obesity and Psoriatic Arthritis. Front. Immunol. 2021, 11, 590749. [Google Scholar] [CrossRef]
- Gisondi, P.; Bellinato, F.; Maurelli, M.; Geat, D.; Zabotti, A.; McGonagle, D.; Girolomoni, G. Reducing the Risk of Developing Psoriatic Arthritis in Patients with Psoriasis. Psoriasis 2022, 12, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Herbert, D.; Franz, S.; Popkova, Y.; Anderegg, U.; Schiller, J.; Schwede, K.; Lorz, A.; Simon, J.C.; Saalbach, A. High-Fat Diet Exacerbates Early Psoriatic Skin Inflammation Independent of Obesity: Saturated Fatty Acids as Key Players. J. Investig. Dermatol. 2018, 138, 1999–2009. [Google Scholar] [CrossRef]
- Barrea, L.; Megna, M.; Cacciapuoti, S.; Frias-Toral, E.; Fabbrocini, G.; Savastano, S.; Colao, A.; Muscogiuri, G. Very low-calorie ketogenic diet (VLCKD) in patients with psoriasis and obesity: An update for dermatologists and nutritionists. Crit. Rev. Food Sci. Nutr. 2022, 62, 398–414. [Google Scholar] [CrossRef]
- Hayran, Y.; Yalçın, B. Smoking habits amongst patients with psoriasis and the effect of smoking on clinical and treatment-associated characteristics: A cross-sectional study. Int. J. Clin. Pract. 2021, 75, e13751. [Google Scholar] [CrossRef]
- Wei, L.; Chen, S.; Zhang, Z.; Kuai, L.; Zhang, R.; Yu, N.; Shi, Y.; Li, B.; Wang, R. Prevalence of Tobacco Smoking and Its Association with Disease Severity Among Patients with Psoriasis in China: A Cross-Sectional Study. Front. Med. 2022, 9, 883458. [Google Scholar] [CrossRef] [PubMed]
- Attwa, E.; Swelam, E. Relationship between smoking-induced oxidative stress and the clinical severity of psoriasis. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Semenov, Y.R.; Herbosa, C.M.; Rogers, A.T.; Huang, A.; Kwatra, S.G.; Cohen, B.; Anadkat, M.J.; Silverberg, J.I. Psoriasis and mortality in the United States: Data from the National Health and Nutrition Examination Survey. J. Am. Acad. Dermatol. 2021, 85, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Harskamp, C.T.; Dhillon, J.S.; Armstrong, E.J. Psoriasis and smoking: A systematic review and meta-analysis. Br. J. Dermatol. 2014, 170, 304–314. [Google Scholar] [CrossRef]
- Owczarczyk-Saczonek, A.; Nowicki, R. The association between smoking and the prevalence of metabolic syndrome and its components in patients with psoriasis aged 30 to 49 years. Adv. Dermatol. Allergol. Postępy Dermatol. Alergol. 2015, 32, 331–336. [Google Scholar] [CrossRef]
- Benowitz, N.L.; Hatsukami, D. Gender differences in the pharmacology of nicotine addiction. Addict. Biol. 1998, 3, 383–404. [Google Scholar] [CrossRef]
- Bhole, V.M.; Choi, H.K.; Burns, L.C.; Vera Kellet, C.; Lacaille, D.V.; Gladman, D.D.; Dutz, J.P. Differences in body mass index among individuals with PsA, psoriasis, RA and the general population. Rheumatology 2012, 51, 552–556. [Google Scholar] [CrossRef]
- Duarte, G.V.; Oliveira, M.F.; Cardoso, T.M.; Follador, I.; Silva, T.S.; Cavalheiro, C.M.; Nonato, W.; Carvalho, E.M. Association between obesity measured by different parameters and severity of psoriasis. Int. J. Dermatol. 2013, 52, 177–181. [Google Scholar] [CrossRef]
- Ahdout, J.; Kotlerman, J.; Elashoff, D.; Kim, J.; Chiu, M.W. Modifiable lifestyle factors associated with metabolic syndrome in patients with psoriasis. Clin. Exp. Dermatol. 2012, 37, 477–483. [Google Scholar] [CrossRef]
- Murray, M.L.; Bergstresser, P.R.; Adams-Huet, B.; Cohen, J.B. Relationship of psoriasis severity to obesity using same-gender siblings as controls for obesity. Clin. Exp. Dermatol. 2009, 34, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Horreau, C.; Pouplard, C.; Brenaut, E.; Barnetche, T.; Misery, L.; Cribier, B.; Jullien, D.; Aractingi, S.; Aubin, F.; Joly, P.; et al. Cardiovascular morbidity and mortality in psoriasis and psoriatic arthritis: A systematic literature review. J. Eur. Acad. Dermatol. Venereol. 2013, 27 (Suppl. S3), 12–29. [Google Scholar] [CrossRef]
- Megna, M.; Camela, E.; Battista, T.; Genco, L.; Martora, F.; Noto, M.; Picone, V.; Ruggiero, A.; Monfrecola, G.; Fabbrocini, G.; et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part I: Focus on pediatric patients. Expert Opin. Drug Saf. 2023, 22, 25–41. [Google Scholar] [CrossRef] [PubMed]
- Megna, M.; Camela, E.; Battista, T.; Genco, L.; Martora, F.; Noto, M.; Picone, V.; Ruggiero, A.; Monfrecola, G.; Fabbrocini, G.; et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part II: Focus on elderly patients. Expert Opin. Drug Saf. 2023, 22, 43–58. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | General n = 147 | Men n = 104 | Women n = 43 | p-Value (Difference between Men and Women) |
|---|---|---|---|---|
| Mean age (years ± SD) | 45.5 ± 15.7 | 44.1 ± 14.3 | 48.9 ± 18.3 | 0.07 |
| Mean age of chronic plaque psoriasis onset (years ± SD) | 27.6 ± 15.4 | 27.6 ± 13.7 | 27.7 ± 18.9 | 0.39 |
| Type of chronic plaque psoriasis (%) | 0.24 | |||
| I | 112 (76.20%) | 82 (78.85%) | 30 (69.77%) | |
| II | 35 (23.80%) | 22 (21.15%) | 13 (30.23%) | |
| Nail involvement (%) | 0.90 | |||
| present | 94 (64.38%) | 66 (64.08%) | 28 (65.12%) | |
| absent | 52 (35.62%) | 37 (35.92%) | 15 (34.88%) | |
| Psoriatic arthritis diagnosis (%) | 0.07 | |||
| present | 27 (18.37%) | 23 (22.12%) | 4 (9.30%) | |
| absent | 120 (81.63%) | 81 (77.88%) | 39 (90.70%) |
| Variable | General n = 147 | Men n = 104 | Women n = 43 | p-Value (Difference between Men and Women) | Type I Psoriasis n = 112 | Type II Psoriasis n = 35 | p-Value (Difference between Type I and Type II) |
|---|---|---|---|---|---|---|---|
| Mean PASI (points ± SD) | 16.14 ± 9.49 | 17.59 ± 10.19 | 12.63 ± 6.36 | 0.007 | 15.97 ± 9.79 | 16.70 ± 8.54 | 0.47 |
| Mean BSA (% ± SD) | 30.27 ± 21.68 | 31.88 ± 23.87 | 26.39 ± 14.74 | 0.53 | 29.97 ± 22.09 | 31.21 ± 20.59 | 0.63 |
| Mean DLQI (points ± SD) | 13.05 ± 6.97 | 13.37 ± 7.41 | 12.28 ± 5.76 | 0.39 | 12.69 ± 7.21 | 14.24 ± 6.04 | 0.19 |
| Mean BMI (points ± SD) | 29.03 ± 5.14 | 28.96 ± 5.13 | 29.18 ± 5.21 | 0.71 | 28.91 ± 5.22 | 29.41 ± 4.94 | 0.46 |
| Variable | General n = 147 | Men n = 104 | Women n = 43 | p-Value (Difference between Men and Women) |
|---|---|---|---|---|
| Diet | 0.05 | |||
| Healthy dietary habits (%) | 24 (16.44%) | 21 (20.39%) | 3 (6.98%) | |
| No dietary habits (%) | 122 (83.56%) | 82 (79.61%) | 40 (93.02%) | |
| Cigarette smoking | 0.01 | |||
| Current and past smokers (%) | 82 (55.78%) | 17 (39.53%) | 65 (62.50%) | |
| Non-smokers (%) | 65 (44.22%) | 26 (60.47%) | 39 (37.50%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Czarnecka, A.; Zabłotna, M.; Purzycka-Bohdan, D.; Nowicki, R.J.; Szczerkowska-Dobosz, A. An Observational Study of 147 Psoriasis Patients: Overweightness and Obesity as a Significant Clinical Factors Correlated with Psoriasis. Medicina 2023, 59, 2006. https://doi.org/10.3390/medicina59112006
Czarnecka A, Zabłotna M, Purzycka-Bohdan D, Nowicki RJ, Szczerkowska-Dobosz A. An Observational Study of 147 Psoriasis Patients: Overweightness and Obesity as a Significant Clinical Factors Correlated with Psoriasis. Medicina. 2023; 59(11):2006. https://doi.org/10.3390/medicina59112006
Chicago/Turabian StyleCzarnecka, Anna, Monika Zabłotna, Dorota Purzycka-Bohdan, Roman J. Nowicki, and Aneta Szczerkowska-Dobosz. 2023. "An Observational Study of 147 Psoriasis Patients: Overweightness and Obesity as a Significant Clinical Factors Correlated with Psoriasis" Medicina 59, no. 11: 2006. https://doi.org/10.3390/medicina59112006