
Neurological Outcome and Respiratory Insufficiency in Intramedullary Tumors of the Upper Cervical Spine
 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Surgery Protocol and Postoperative Management
2.2. Medical and Surgical Data
2.3. Statistical Analysis
3. Results
3.1. Entities and Presentation
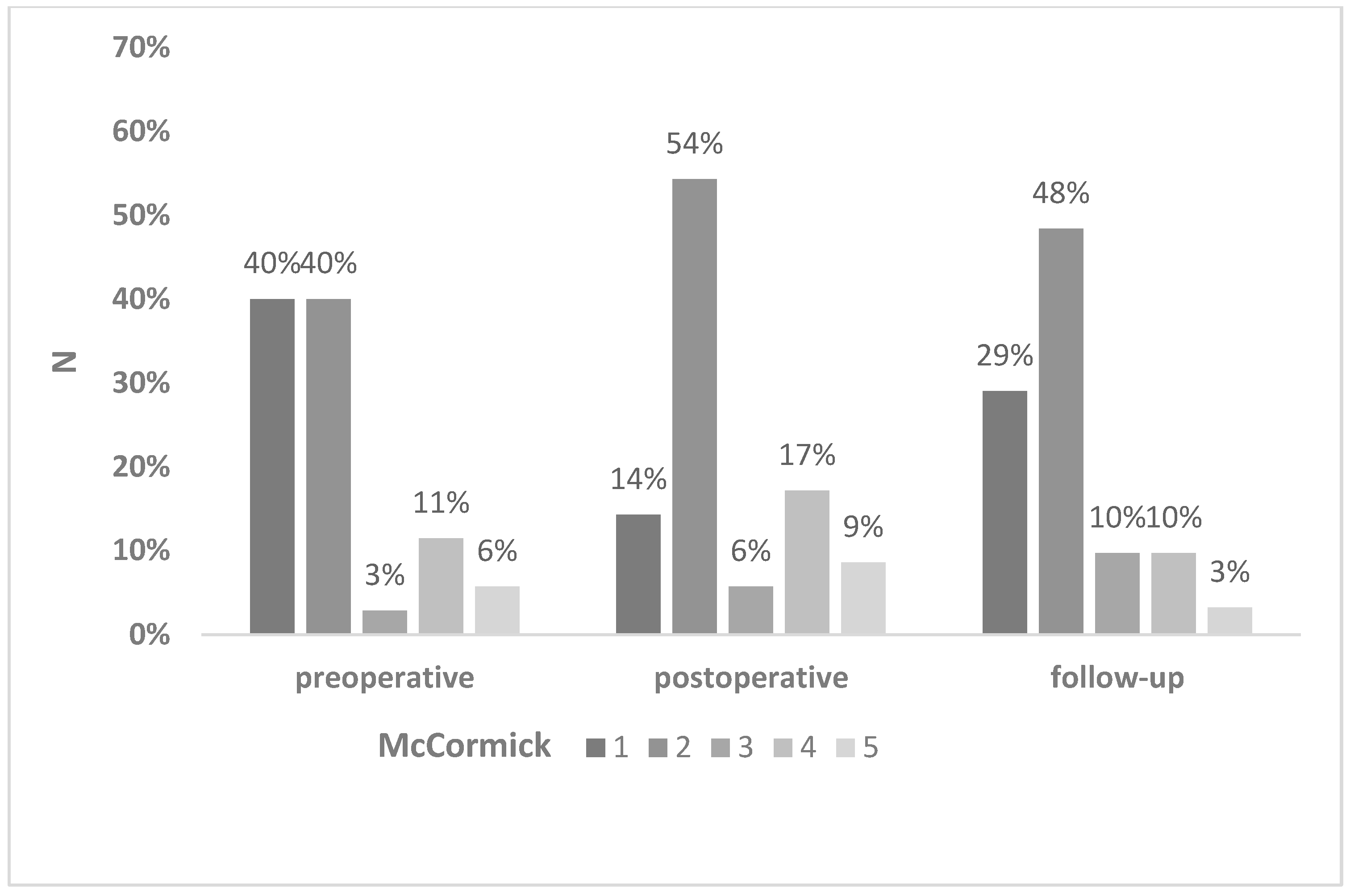
3.2. Surgical and Clinical Outcome
3.3. Respiratory Dysfunction
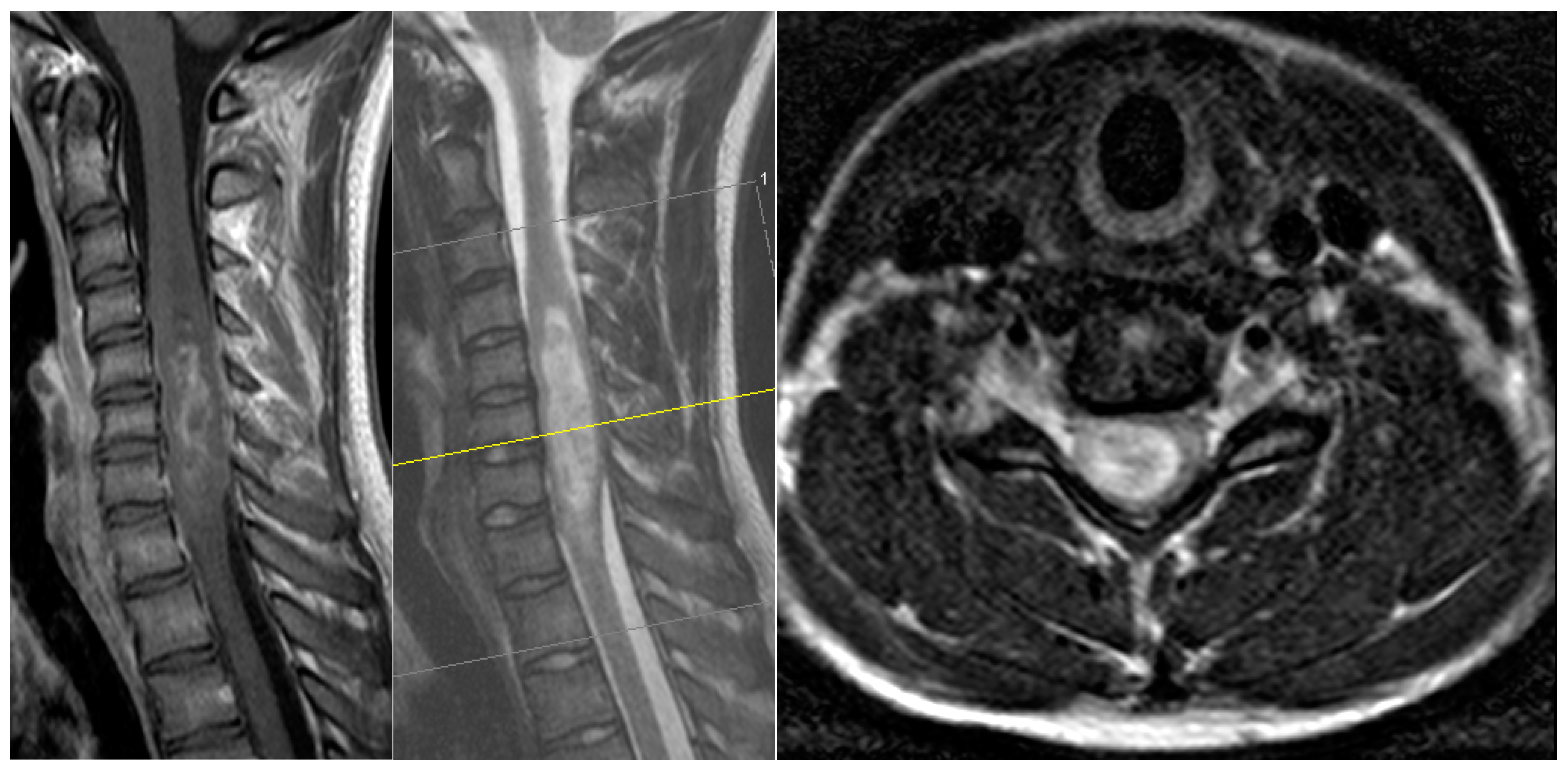
3.4. Case Presentation
4. Discussion
4.1. Clinical Outcome
4.2. Prognostic Factors for Neurologic Deterioration
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Samartzis, D.; Gillis, C.C.; Shih, P.; O’Toole, J.E.; Fessler, R.G. Intramedullary Spinal Cord Tumors: Part I-Epidemiology, Pathophysiology, and Diagnosis. Glob. Spine J. 2015, 5, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Butenschoen, V.M.; Schwendner, M.; Hubertus, V.; Onken, J.; Koegl, N.; Mohme, T.; Maurer, S.; Boeckh-Behrens, T.; Eicker, S.O.; Thomé, C.; et al. Preoperative angiographic considerations and neurological outcome after surgical treatment of intradural spinal hemangioblastoma: A multicenter retrospective case series. J. Neurooncol. 2023, 161, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Wostrack, M.; Ringel, F.; Eicker, S.O.; Jagersberg, M.; Schaller, K.; Kerschbaumer, J.; Thomé, C.; Shiban, E.; Stoffel, M.; Friedrich, B.; et al. Spinal ependymoma in adults: A multicenter investigation of surgical outcome and progression-free survival. J. Neurosurg. Spine 2018, 28, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Hersh, A.M.; Antar, A.; Pennington, Z.; Aygun, N.; Patel, J.; Goldsborough, E., 3rd; Porras, J.L.; Elsamadicy, A.A.; Lubelski, D.; Wolinsky, J.P.; et al. Predictors of survival and time to progression following operative management of intramedullary spinal cord astrocytomas. J. Neurooncol. 2022, 158, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Butenschoen, V.M.; Hubertus, V.; Janssen, I.K.; Onken, J.; Wipplinger, C.; Mende, K.C.; Eicker, S.O.; Kehl, V.; Thomé, C.; Vajkoczy, P.; et al. Surgical treatment and neurological outcome of infiltrating intramedullary astrocytoma WHO II-IV: A multicenter retrospective case series. J. Neurooncol. 2021, 151, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Galeiras Vazquez, R.; Rascado Sedes, P.; Mourelo Farina, M.; Montoto Marques, A.; Ferreiro Velasco, M.E. Respiratory management in the patient with spinal cord injury. Biomed. Res. Int. 2013, 2013, 168757. [Google Scholar] [CrossRef] [PubMed]
- McCormick, P.C.; Torres, R.; Post, K.D.; Stein, B.M. Intramedullary ependymoma of the spinal cord. J. Neurosurg. 1990, 72, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Gembruch, O.; Chihi, M.; Haarmann, M.; Parlak, A.; Oppong, M.D.; Rauschenbach, L.; Michel, A.; Jabbarli, R.; Ahmadipour, Y.; Sure, U.; et al. Surgical outcome and prognostic factors in spinal cord ependymoma: A single-center, long-term follow-up study. Ther. Adv. Neurol. Disord. 2021, 14, 17562864211055694. [Google Scholar] [CrossRef] [PubMed]
- Hussain, I.; Parker, W.E.; Barzilai, O.; Bilsky, M.H. Surgical Management of Intramedullary Spinal Cord Tumors. Neurosurg. Clin. N. Am. 2020, 31, 237–249. [Google Scholar] [CrossRef] [PubMed]
- Fei, X.; Jia, W.; Gao, H.; Yang, C.; Li, D.; Qian, Z.; Han, B.; Wang, D.; Xu, Y. Clinical characteristics and surgical outcomes of ependymomas in the upper cervical spinal cord: A single-center experience of 155 consecutive patients. Neurosurg. Rev. 2021, 44, 1665–1673. [Google Scholar] [CrossRef] [PubMed]
- Takami, T.; Naito, K.; Yamagata, T.; Ohata, K. Surgical management of spinal intramedullary tumors: Radical and safe strategy for benign tumors. Neurol. Med. Chir. 2015, 55, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Bostrom, A.; Kanther, N.C.; Grote, A.; Bostrom, J. Management and outcome in adult intramedullary spinal cord tumours: A 20-year single institution experience. BMC Res. Notes 2014, 7, 908. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Cho, Y.E.; Kwon, Y.M. Neurological outcome after surgical treatment of intramedullary spinal cord tumors. Korean J. Spine 2014, 11, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Houten, J.K.; Cooper, P.R. Spinal cord astrocytomas: Presentation, management and outcome. J. Neurooncol. 2000, 47, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Azad, T.D.; Jiang, B.; Bettegowda, C. Molecular foundations of primary spinal tumors-implications for surgical management. Ann. Transl. Med. 2019, 7, 222. [Google Scholar] [CrossRef] [PubMed]
- Grady, C.; Melnick, K.; Porche, K.; Dastmalchi, F.; Hoh, D.J.; Rahman, M.; Ghiaseddin, A. Glioma Immunotherapy: Advances and Challenges for Spinal Cord Gliomas. Neurospine 2022, 19, 13–29. [Google Scholar] [CrossRef] [PubMed]
- Payer, S.; Mende, K.C.; Westphal, M.; Eicker, S.O. Intramedullary spinal cord metastases: An increasingly common diagnosis. Neurosurg. Focus. 2015, 39, E15. [Google Scholar] [CrossRef] [PubMed]
- Wostrack, M.; Pape, H.; Kreutzer, J.; Ringel, F.; Meyer, B.; Stoffel, M. Surgical treatment of spinal intradural carcinoma metastases. Acta Neurochir. 2012, 154, 349–357. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | No. (%) of Mean ± SD |
|---|---|
| Male | 20 (57%) |
| Mean age overall in yrs | 45 ± 16 |
| Histopathology | |
| Ependymoma (WHO°1–2) | 22 (62.8%) |
| Astrocytoma (WHO°2–4) | 4 (11.4%) |
| Hemangioblastoma WHO 1 | 6 (17.1%) |
| Metastases | 2 (5.7%) |
| Other | 1 (2.86%) |
| Patients with neurofibromatosis type 2 | 4 (11.4%) |
| Median duration of symptoms in month | 3 ± 48 |
| Mean tumor vol in cm3 | 1.86 ± 2.58 |
| Presence of syringomyelia | 8 (23%) |
| Extent of tumor resection | |
| Gross total resection | 25 (71.5%) |
| Subtotal resection | 7 (20.0%) |
| Biopsy | 3 (8.6%) |
| Symptom | No. (%) |
|---|---|
| Sensoric deficit | 41.7 |
| Motoric deficit | 38.9 |
| Pain | 25.0 |
| Gait ataxia | 19.4 |
| Preoperative Deficit | Postoperative Deficit | New Motor Deficit | New Sensory Deficit | Motor Deficit at FU | Sensory Deficit at FU |
|---|---|---|---|---|---|
| gait ataxia, hypesthesia sub C5 | accentuation of hypesthesia | no | yes | No | Yes |
| ASIA D | hemiplegia | yes | no | Yes | no |
| intermittent urinary incontinence | arm paresis MMT 3/5 | yes | yes | Yes | no |
| hypesthesia | gait ataxia | no | yes | lost to FU | lost to FU |
| mild tetraparesis MMT 4/5 | aggraviation of distal arm paresis | yes | yes | No | no |
| no deficit (neck pain) | hypesthesia | no | yes | No | yes |
| gait ataxia | mild arm paresis | yes | no | Yes | no |
| tingling sensation | aggraviation of tingling sensation/hypesthesia | no | yes | no | yes |
| no deficit (shoulder pain) | mild arm paresis, hypesthesia | yes | yes | no | no |
| hemiparesis | aggraviation of hemihypesthesia | no | yes | no | yes |
| hemihypesthesia | = | no | no | no | no |
| no deficit (vertigo) | hemihypesthesia | no | yes | lost to FU | lost to FU |
| mild arm paresis | new hemihypesthesia | no | yes | no | no |
| ASIA C | aggraviation of motor deficit | yes | no | lost to FU | lost to FU |
| gait ataxia | aggraviation of gait ataxia | no | yes | no | no |
| no deficit (neck pain) | hemiparesis | yes | yes | yes | yes |
| no deficit (neck pain) | hemiparesis | yes | yes | yes | yes |
| gait ataxia, hypesthesia sub C6 | ASIA C | yes | yes | lost to FU | lost to FU |
| no deficit (neck and arm pain) | diffuse hypesthesia | no | yes | no | no |
| no deficit (neck and arm pain) | diffuse hypesthesia | no | yes | no | yes |
| gait ataxia | mild arm paresis | yes | yes | no | yes |
| fine motor disability | = | no | no | yes | yes |
| allodynia | = | no | no | no | no |
| mild arm paresis | accentuation of arm paresis | yes | no | yes | no |
| mild arm paresis | ASIA D | yes | yes | no | no |
| ASIA B | ASIA B | no | no | no | no |
| no deficit (neck and arm pain) | hemihypesthesia | no | yes | no | yes |
| tingling sensation | hemiparesis | yes | yes | yes | yes |
| no deficit (neck and arm pain) | = | no | no | no | no |
| hypesthesia | = | no | no | no | no |
| gait ataxia, arm paresis | accentuation of arm paresis | yes | yes | yes | yes |
| hemihypesthesia | accentuation of hemihypesthesia | no | yes | no | no |
| severe hemiparsis | = | no | no | lost to FU | lost to FU |
| ASIA A | ASIA A | no | no | no | no |
| severe hemiparsis | accentuation of severe hemiparesis | yes | no | lost to FU | lost to FU |
| 15 | 22 | 9 | 12 | ||
| 43% | 63% | 31% | 41% |
| Variable | p Value |
|---|---|
| Age | 0.518 |
| Sex | 0.257 |
| Tumor vol | 0.070 |
| Duration of symptoms | 0.064 |
| Preop McCormick score | <0.001 *** |
| WHO grade | 0.045 * |
| Surgical approach | 0.483 |
| Extension of resection | 0.415 |
| Syrinx | 0.335 |
| Loss of potentials in IONM | 0.016 * |
| Variable | p Value |
|---|---|
| Age | 0.497 |
| Sex | 0.433 |
| Tumor vol | 0.151 |
| Duration of symptoms | 0.373 |
| Preop McCormick score | <0.001 *** |
| WHO grade | 0.009 * |
| Surgical approach | 0.212 |
| Extension of resection | 0.796 |
| Syrinx | 0.493 |
| Loss of potentials in IONM | 0.202 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goloshchapova, K.; Goldberg, M.; Meyer, B.; Wostrack, M.; Butenschoen, V.M. Neurological Outcome and Respiratory Insufficiency in Intramedullary Tumors of the Upper Cervical Spine. Medicina 2023, 59, 1754. https://doi.org/10.3390/medicina59101754
Goloshchapova K, Goldberg M, Meyer B, Wostrack M, Butenschoen VM. Neurological Outcome and Respiratory Insufficiency in Intramedullary Tumors of the Upper Cervical Spine. Medicina. 2023; 59(10):1754. https://doi.org/10.3390/medicina59101754
Chicago/Turabian StyleGoloshchapova, Kateryna, Maria Goldberg, Bernhard Meyer, Maria Wostrack, and Vicki M. Butenschoen. 2023. "Neurological Outcome and Respiratory Insufficiency in Intramedullary Tumors of the Upper Cervical Spine" Medicina 59, no. 10: 1754. https://doi.org/10.3390/medicina59101754