
Minimally Invasive Facetectomy and Fusion for Resection of Extensive Dumbbell Tumors in the Lumbar Spine

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
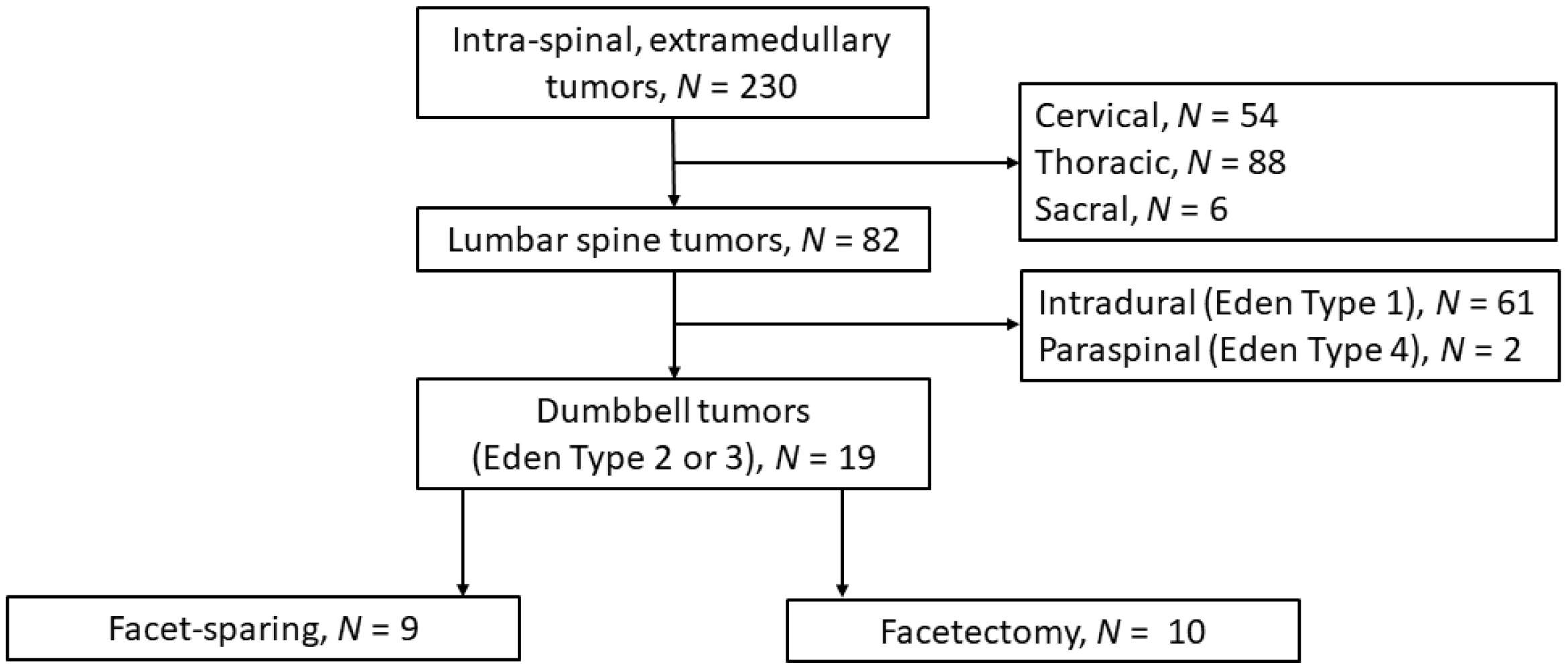
2.2. Participants
2.3. Data and Variables
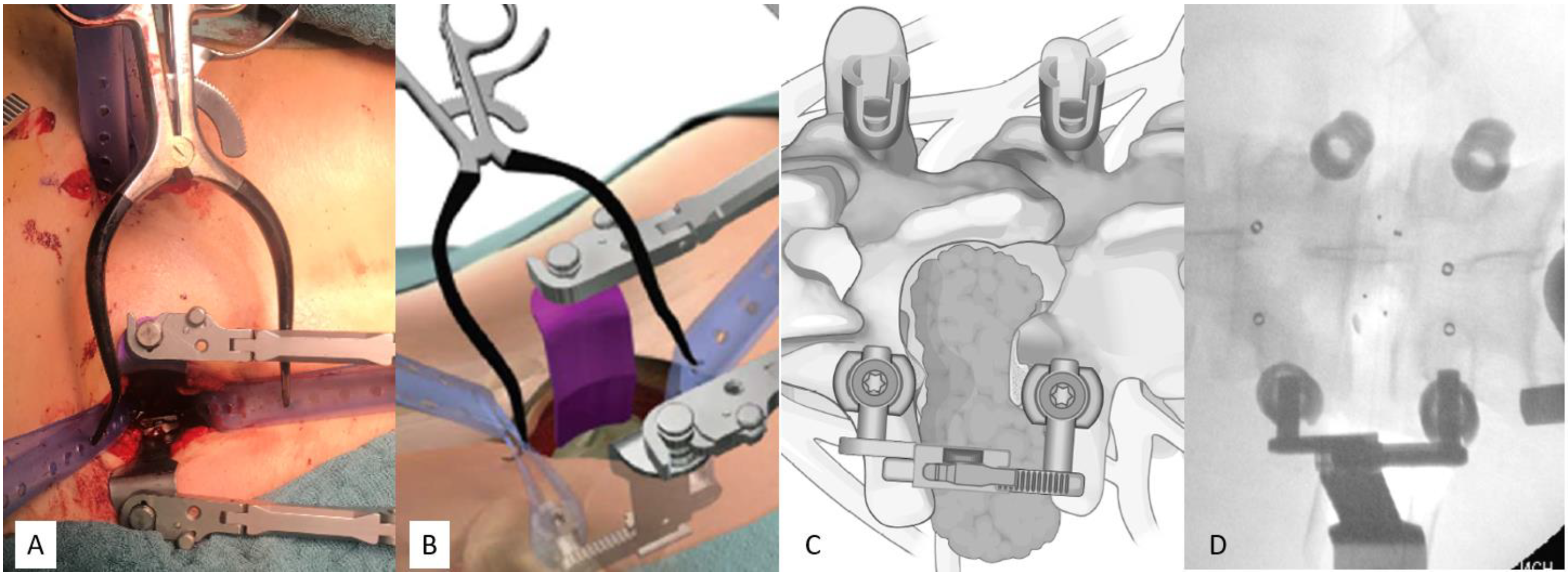
2.4. Surgical Techniques
2.5. Statistics
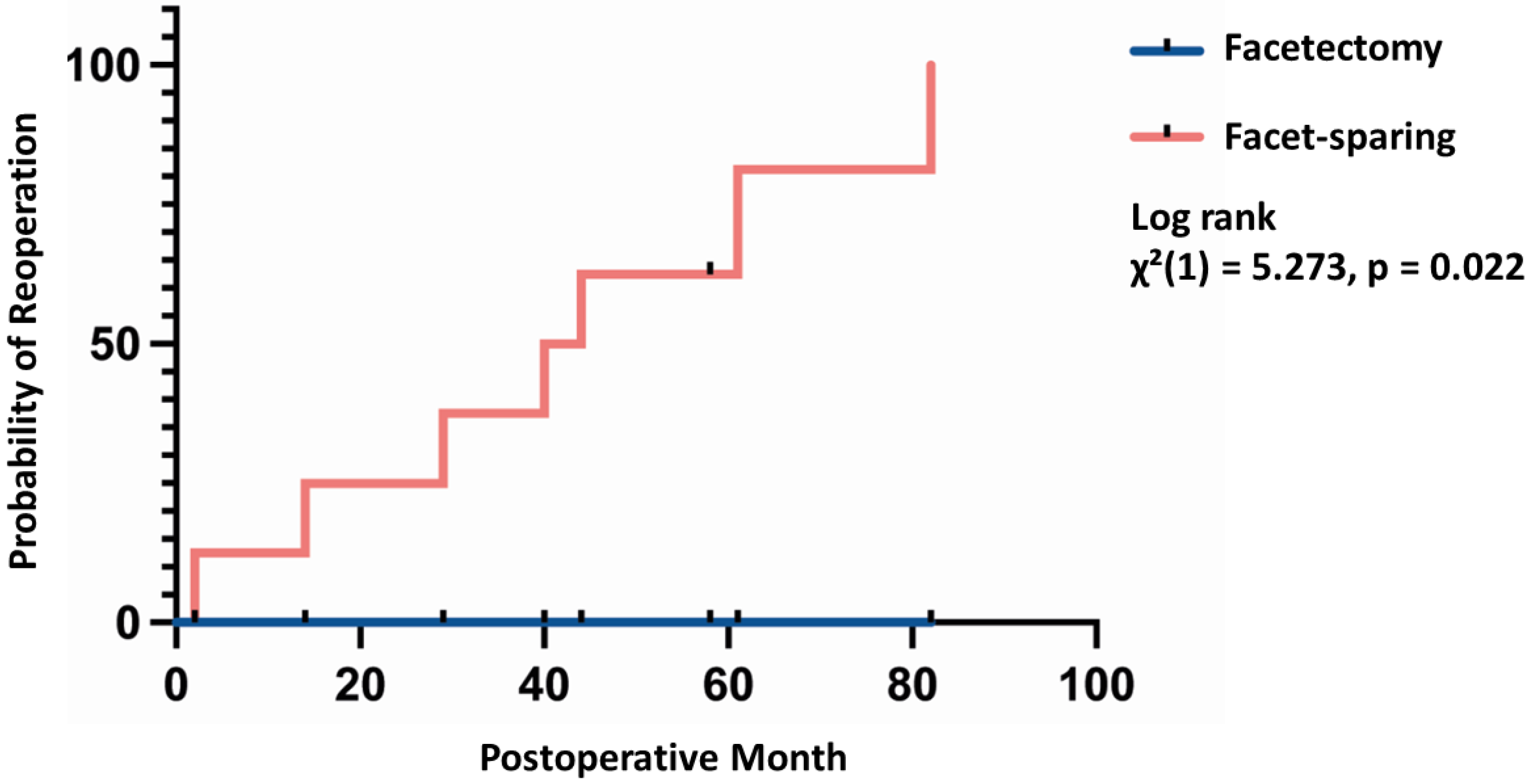
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eden, K. The dumb-bell tumours of the spine. Br. J. Surg. 1941, 28, 549–570. [Google Scholar] [CrossRef]
- Ozawa, H.; Kokubun, S.; Aizawa, T.; Hoshikawa, T.; Kawahara, C. Spinal dumbbell tumors: An analysis of a series of 118 cases. J. Neurosurg. Spine 2007, 7, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Ottenhausen, M.; Ntoulias, G.; Bodhinayake, I.; Ruppert, F.H.; Schreiber, S.; Förschler, A.; Boockvar, J.A.; Jödicke, A. Intradural spinal tumors in adults—Update on management and outcome. Neurosurg. Rev. 2019, 42, 371–388. [Google Scholar] [CrossRef] [PubMed]
- Safaee, M.; Oh, T.; Barbaro, N.M.; Chou, D.; Mummaneni, P.V.; Weinstein, P.R.; Tihan, T.; Ames, C.P. Results of Spinal Fusion After Spinal Nerve Sheath Tumor Resection. World Neurosurg. 2016, 90, 6–13. [Google Scholar] [CrossRef]
- Safaee, M.; Parsa, A.T.; Barbaro, N.M.; Chou, D.; Mummaneni, P.V.; Weinstein, P.R.; Tihan, T.; Ames, C.P. Association of tumor location, extent of resection, and neurofibromatosis status with clinical outcomes for 221 spinal nerve sheath tumors. Neurosurg. Focus 2015, 39, E5. [Google Scholar] [CrossRef] [Green Version]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [Green Version]
- Macnab, I. Negative disc exploration. An analysis of the causes of nerve-root involvement in sixty-eight patients. J. Bone Jt. Surg Am. 1971, 53, 891–903. Available online: https://pubmed.ncbi.nlm.nih.gov/4326746/ (accessed on 9 June 2022). [CrossRef]
- Müther, M.; Lüthge, S.; Gerwing, M.; Stummer, W.; Schwake, M. Management of Spinal Dumbbell Tumors via a Minimally Invasive Posterolateral Approach and Carbon Fiber-Reinforced Polyether Ether Ketone Instrumentation: Technical Note and Surgical Case Series. World Neurosurg. 2021, 151, 277–283.e1. [Google Scholar] [CrossRef]
- Emel, E.; Abdallah, A.; Sofuoglu, O.E.; Ofluoglu, A.E.; Gunes, M.; Guler, B.; Bilgic, B. Long-term Surgical Outcomes of Spinal Schwannomas: Retrospective Analysis of 49 Consecutive Cases. Turk. Neurosurg. 2017, 27, 217–225. [Google Scholar] [CrossRef] [Green Version]
- Sebai, M.A.; Kerezoudis, P.; Alvi, M.A.; Yoon, J.W.; Spinner, R.J.; Bydon, M. Need for arthrodesis following facetectomy for spinal peripheral nerve sheath tumors: An institutional experience and review of the current literature. J. Neurosurg. Spine 2019, 31, 112–122. [Google Scholar] [CrossRef]
- Safaee, M.M.; Lyon, R.; Barbaro, N.M.; Chou, D.; Mummaneni, P.V.; Weinstein, P.R.; Chin, C.T.; Tihan, T.; Ames, C.P. Neurological outcomes and surgical complications in 221 spinal nerve sheath tumors. J. Neurosurg. Spine 2017, 26, 103–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghogawala, Z.; Dziura, J.; Butler, W.E.; Dai, F.; Terrin, N.; Magge, S.N.; Coumans, J.-V.C.; Harrington, J.F.; Amin-Hanjani, S.; Schwartz, J.S.; et al. Laminectomy plus Fusion versus Laminectomy Alone for Lumbar Spondylolisthesis. N. Engl. J. Med. 2016, 374, 1424–1434. [Google Scholar] [CrossRef] [PubMed]
- Montano, N.; D’Alessandris, Q.G.; D’Ercole, M.; Lauretti, L.; Pallini, R.; di Bonaventura, R.; La Rocca, G.; Bianchi, F.; Fernandez, E. Tumors of the peripheral nervous system: Analysis of prognostic factors in a series with long-term follow-up and review of the literature. J. Neurosurg. 2016, 125, 363–371. [Google Scholar] [CrossRef] [Green Version]
- Sowash, M.; Barzilai, O.; Kahn, S.; McLaughlin, L.; Boland, P.; Bilsky, M.H.; Laufer, I. Clinical outcomes following resection of giant spinal schwannomas: A case series of 32 patients. J. Neurosurg. Spine 2017, 26, 494–500. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, T.; Hirai, T.; Yoshii, T.; Inose, H.; Yuasa, M.; Matsukura, Y.; Morishita, S.; Kobayashi, Y.; Utagawa, K.; Kawabata, A.; et al. Risk factors for recurrence and regrowth of spinal schwannoma. J. Orthop. Sci. 2022. [Google Scholar] [CrossRef]
- Fehlings, M.G.; Nater, A.; Zamorano, J.J.; Tetreault, L.A.; Varga, P.P.; Gokaslan, Z.L.; Boriani, S.; Fisher, C.G.; Rhines, L.; Bettegowda, C.; et al. Risk Factors for Recurrence of Surgically Treated Conventional Spinal Schwannomas: Analysis of 169 Patients From a Multicenter International Database. Spine 2016, 41, 390–398. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.; Liang, Z.Y.; Chen, Y.; Chen, C.M. Comparison of the Clinical Efficacy of Transforaminal Endoscopy and Microtubular Technology for the Treatment of Lumbar Dumbbell-Shaped Tumors. Neurospine 2022, 19, 513–523. [Google Scholar] [CrossRef]
- Jiang, Y.W.; Xu, X.J.; Wang, R.; Chen, C.M. Tubular minimally invasive resection of McCormick type II paraspinal schwannoma: Preliminary experience. Br. J. Neurosurg. 2022, 1–6. [Google Scholar] [CrossRef]
- Poblete, J.; Martinez Anda, J.J.; Mendoza, A.A.R.; Torales, J.; di Somma, A.; Torne, R.; Fuster, S.; Enseñat, J. Minimally Invasive Surgical Technique for the Management of Giant Dumbbell Spinal Schwannoma. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2021. [Google Scholar] [CrossRef]
- Pekmezci, M.; Dirican, B.; Yapici, B.; Yazici, M.; Alanay, A.; Gürdalli, S. Spinal implants and radiation therapy: The effect of various configurations of titanium implant systems in a single-level vertebral metastasis model. J. Bone Jt. Surg Am. 2006, 88, 1093–1100. [Google Scholar] [CrossRef]
- Jackson, J.B.; Crimaldi, A.J.; Peindl, R.; Norton, H.J.; Anderson, W.E.; Patt, J.C. Effect of Polyether Ether Ketone on Therapeutic Radiation to the Spine: A Pilot Study. Spine 2017, 42, E1–E7. [Google Scholar] [CrossRef] [PubMed]
- Poel, R.; Belosi, F.; Albertini, F.; Walser, M.; Gisep, A.; Lomax, A.J.; Weber, D.C. Assessing the advantages of CFR-PEEK over titanium spinal stabilization implants in proton therapy—A phantom study. Phys. Med. Biol. 2020, 65, 245031. [Google Scholar] [CrossRef] [PubMed]
- Ringel, F.; Ryang, Y.M.; Kirschke, J.S.; Müller, B.S.; Wilkens, J.J.; Brodard, J.; Combs, S.E.; Meyer, B. Radiolucent Carbon Fiber–Reinforced Pedicle Screws for Treatment of Spinal Tumors: Advantages for Radiation Planning and Follow-Up Imaging. World Neurosurg. 2017, 105, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Lindtner, R.A.; Schmid, R.; Nydegger, T.; Konschake, M.; Schmoelz, W. Pedicle screw anchorage of carbon fiber-reinforced PEEK screws under cyclic loading. Eur. Spine J. 2018, 27, 1775–1784. [Google Scholar] [CrossRef] [Green Version]
- Eicker, S.O.; Krajewski, K.; Payer, S.; Krätzig, T.; Dreimann, M. First experience with Carbon/PEEK pedicle screws. J. Neurosurg. Sci. 2017, 61, 222–224. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, S.; Albers, C.E.; Elfiky, T.; Deml, M.C.; Milavec, H.; Bigdon, S.F.; Benneker, L.M. First Results of a New Vacuum Plasma Sprayed (VPS) Titanium-Coated Carbon/PEEK Composite Cage for Lumbar Interbody Fusion. J. Funct. Biomater. 2018, 9, 23. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Facetectomy, N = 10 | Facet-Sparing, N = 9 | p Value | |
|---|---|---|---|
| M/F (N) | 6/4 | 8/1 | 0.3034 |
| Median age (IQR) | 49 years (30–53) | 38 years (33–46) | 0.596 |
| Median surgery time (IQR) | 246 min (218–278) | 215 min (139–250) | 0.34 |
| Median tumor volume (IQR) | 9.64 mL (5.13–15.40) | 7.75 mL (4.37–28.90) | 0.39 |
| Tumor Eden type 2 | 2 | 2 | 1 |
| Tumor Eden type 3 | 8 | 7 | 1 |
| Primary surgery | 4 (40%) | 7 (78%) | 0.17 |
| Side (left/right) | 7/3 | 6/3 | 1 |
| Pathology | |||
| Schwannoma (WHO grade I) | 9 (9%) | 8 (89%) | 1 |
| Hemangiopericytoma (WHO grade II) | 1 (10%) | 1 (11%) |
| Facetectomy | Facet-Sparing | p Value | |
|---|---|---|---|
| Median blood loss (IQR) | 200 mL (75–875) | 100 mL (50–300) | 0.466 |
| Gross total resection (N, 10%) | 10 (100%) | 1 (11.1%) | <0.001 |
| Number of complications | 0 | 1 | |
| Median length of hospital stay (IQR) | 4 days (3–6) | 6 days (5–8) | 0.121 |
| Macnab score 5 (excellent outcome) | 4 (40%) | 3 (33.3%) | |
| Macnab score 4 (good outcome) | 6 (60%) | 4 (44.45%) | |
| Macnab score 3 (fair outcome) | 1 (11.1%) | ||
| Macnab score 2 (poor outcome) | 1 (11.1%) | ||
| Favorable outcome (Macnab score 4–5)/ Unfavorable outcome (Macnab score 1–3) | 10/0 (100%) | 7/2 (77.7%/22.3%) | 0.19 |
| Second surgery required (%) | N = 0, 0% | N = 8 (88.9%) | <0.001 |
| Mean follow up time | 21 (IQR 14–37) | 44 (IQR 29–61) | 0.171 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwake, M.; Maragno, E.; Gallus, M.; Schipmann, S.; Spille, D.; Al Barim, B.; Stummer, W.; Müther, M. Minimally Invasive Facetectomy and Fusion for Resection of Extensive Dumbbell Tumors in the Lumbar Spine. Medicina 2022, 58, 1613. https://doi.org/10.3390/medicina58111613
Schwake M, Maragno E, Gallus M, Schipmann S, Spille D, Al Barim B, Stummer W, Müther M. Minimally Invasive Facetectomy and Fusion for Resection of Extensive Dumbbell Tumors in the Lumbar Spine. Medicina. 2022; 58(11):1613. https://doi.org/10.3390/medicina58111613
Chicago/Turabian StyleSchwake, Michael, Emanuele Maragno, Marco Gallus, Stephanie Schipmann, Dorothee Spille, Bilal Al Barim, Walter Stummer, and Michael Müther. 2022. "Minimally Invasive Facetectomy and Fusion for Resection of Extensive Dumbbell Tumors in the Lumbar Spine" Medicina 58, no. 11: 1613. https://doi.org/10.3390/medicina58111613