

Comparison of Walking Quality Variables between End-Stage Osteonecrosis of Femoral Head Patients and Healthy Subjects by a Footscan Plantar Pressure System

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Acquirement of Walking Pattern Data
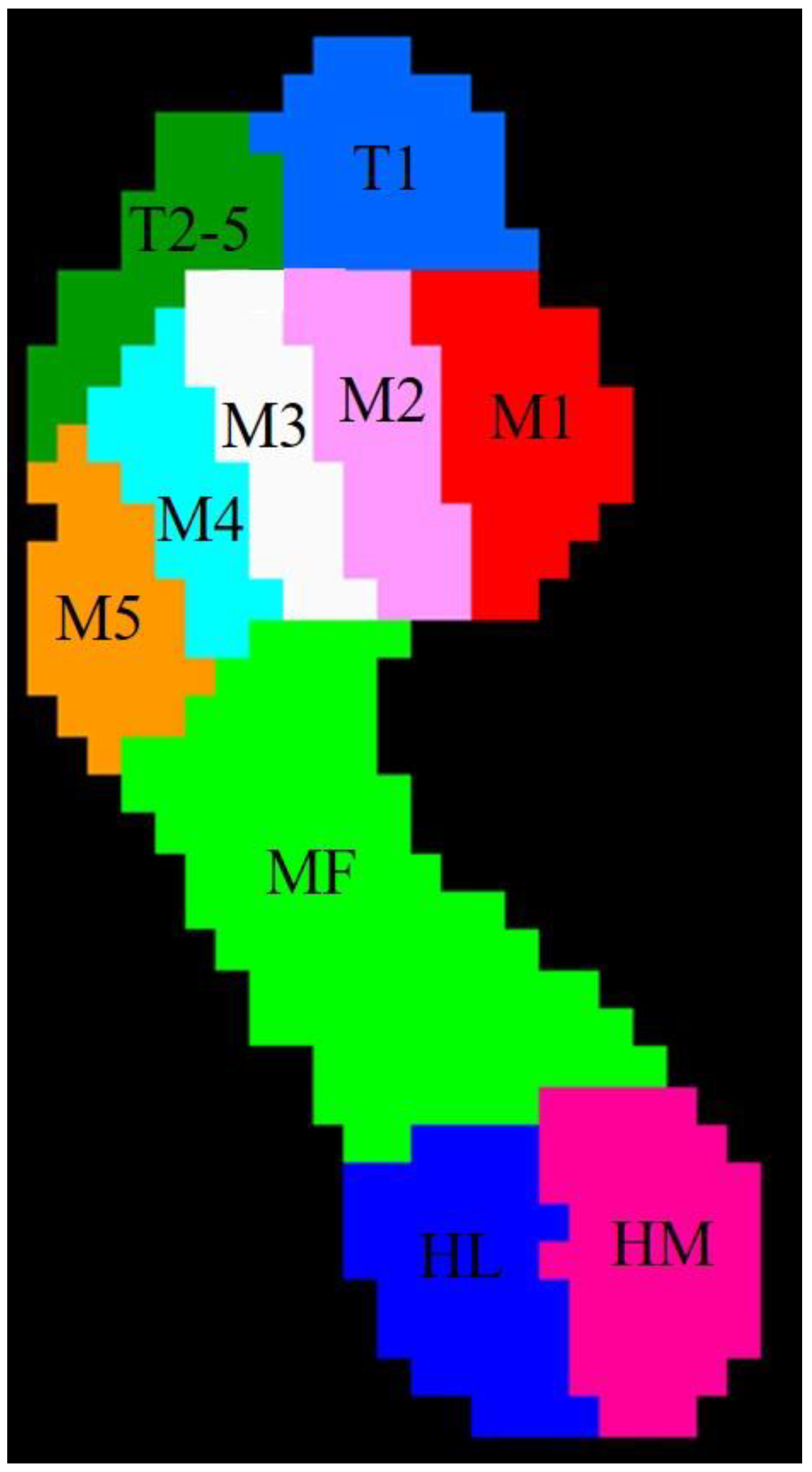
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
3.1. Baseline Demographics
3.2. Spatiotemporal Variables in ONFH and Healthy Groups
3.3. Plantar Pressure Distribution in the ONFH and Healthy Groups
3.3.1. Static Plantar Pressure Distribution in ONFH and Healthy Group
3.3.2. Dynamic Plantar Pressure Distribution in ONFH and Healthy Group
3.4. Regional Impulse Percentage and Contact Area Percentage in Different Regions of ONFH and Healthy Group
3.5. Symmetry Index of ONFH and Healthy Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kamiya, N.; Yamaguchi, R.; Aruwajoye, O.; Adapala, N.S.; Kim, H.K. Development of a mouse model of ischemic osteonecrosis. Clin. Orthop. Relat. Res. 2015, 473, 1486–1498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukushima, W.; Fujioka, M.; Kubo, T.; Tamakoshi, A.; Nagai, M.; Hirota, Y. Nationwide epidemiologic survey of idiopathic osteonecrosis of the femoral head. Clin. Orthop. Relat. Res. 2010, 468, 2715–2724. [Google Scholar] [CrossRef] [Green Version]
- Feng, Y.; Yang, S.H.; Xiao, B.J.; Xu, W.H.; Ye, S.N.; Xia, T.; Zhang, D.; Liu, X.-Z.; Liao, Y.-F. Decreased in the number and function of circulation endothelial progenitor cells in patients with avascular necrosis of the femoral head. Bone 2010, 46, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Mont, M.A.; Salem, H.S.; Piuzzi, N.S.; Goodman, S.B.; Jones, L.C. Nontraumatic Osteonecrosis of the Femoral Head: Where Do We Stand Today?: A 5-Year Update. J. Bone Joint Surg. Am. 2020, 102, 1084–1099. [Google Scholar] [CrossRef] [PubMed]
- Rajaee, S.S.; Campbell, J.C.; Mirocha, J.; Paiement, G.D. Increasing Burden of Total Hip Arthroplasty Revisions in Patients Between 45 and 64 Years of Age. J. Bone Joint Surg. Am. 2018, 100, 449–458. [Google Scholar] [CrossRef]
- Mont, M.A.; Hungerford, D.S. Non-traumatic avascular necrosis of the femoral head. J. Bone Joint Surg. Am. 1995, 77, 459–474. [Google Scholar] [CrossRef]
- Kahlenberg, C.A.; Swarup, I.; Krell, E.C.; Heinz, N.; Figgie, M.P. Causes of Revision in Young Patients Undergoing Total Hip Arthroplasty. J. Arthroplast. 2019, 34, 1435–1440. [Google Scholar] [CrossRef]
- Safayi, S.; Jeffery, N.D.; Shivapour, S.K.; Zamanighomi, M.; Zylstra, T.J.; Bratsch-Prince, J.; Wilson, S.; Reddy, C.G.; Fredericks, D.C.; Gillies, G.T.; et al. Kinematic analysis of the gait of adult sheep during treadmill locomotion: Parameter values, allowable total error, and potential for use in evaluating spinal cord injury. J. Neurol. Sci. 2015, 358, 107–112. [Google Scholar] [CrossRef]
- Krizsan-Agbas, D.; Winter, M.K.; Eggimann, L.S.; Meriwether, J.; Berman, N.E.; Smith, P.G.; McCarson, K.E. Gait analysis at multiple speeds reveals differential functional and structural outcomes in response to graded spinal cord injury. J. Neurotrauma 2014, 31, 846–856. [Google Scholar] [CrossRef] [Green Version]
- Klopfer-Kramer, I.; Brand, A.; Wackerle, H.; Mussig, J.; Kroger, I.; Augat, P. Gait analysis-Available platforms for outcome assessment. Injury 2020, 51 (Suppl. S2), S90–S96. [Google Scholar] [CrossRef]
- Jeans, K.A.; Karol, L.A. Plantar pressures following Ponseti and French physiotherapy methods for clubfoot. J. Pediatr. Orthop. 2010, 30, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Wei, J.; Yan, Y.B.; Shang, L.; Yang, X.J.; Huang, L.Y.; Lei, W. Pedobarographic Analysis following Ponseti Treatment for Unilateral Neglected Congenital Clubfoot. Sci. Rep. 2018, 8, 6270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeans, K.A.; Tulchin-Francis, K.; Crawford, L.; Karol, L.A. Plantar pressures following anterior tibialis tendon transfers in children with clubfoot. J. Pediatr. Orthop. 2014, 34, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Zhang, F.; Wang, B.; Liu, B.; Li, L.; Kim, S.Y.; Goodman, S.B.; Hernigou, P.; Cui, Q.; Lineaweaver, W.C.; et al. Guidelines for clinical diagnosis and treatment of osteonecrosis of the femoral head in adults (2019 version). J. Orthop. Transl. 2020, 21, 100–110. [Google Scholar] [CrossRef]
- Li, X.; Huang, H.; Wang, J.; Yu, Y.; Ao, Y. The Analysis of Plantar Pressure Data Based on Multimodel Method in Patients with Anterior Cruciate Ligament Deficiency during Walking. BioMed. Res. Int. 2016, 2016, 7891407. [Google Scholar] [CrossRef] [Green Version]
- Periyasamy, R.; Mishra, A.; Anand, S.; Ammini, A.C. Preliminary investigation of foot pressure distribution variation in men and women adults while standing. Foot 2011, 21, 142–148. [Google Scholar] [CrossRef]
- Periyasamy, R.; Anand, S. The effect of foot arch on plantar pressure distribution during standing. J. Med. Eng. Technol. 2013, 37, 342–347. [Google Scholar] [CrossRef]
- Lim, B.O.; O’Sullivan, D.; Choi, B.G.; Kim, M.Y. Comparative gait analysis between children with autism and age-matched controls: Analysis with temporal-spatial and foot pressure variables. J. Phys. Ther. Sci. 2016, 28, 286–292. [Google Scholar] [CrossRef] [Green Version]
- Razak, A.H.; Zayegh, A.; Begg, R.K.; Wahab, Y. Foot plantar pressure measurement system: A review. Sensors 2012, 12, 9884–9912. [Google Scholar] [CrossRef] [Green Version]
- Sendur, S.N.; Oguz, S.; Dagdelen, S.; Erbas, T. Assessment of static and dynamic plantar data of patients with acromegaly. Pituitary 2019, 22, 373–380. [Google Scholar] [CrossRef]
- Orlin, M.; Stetson, K.; Skowronski, J.; Pierrynowski, M. Foot pressure distribution: Methodology and clinical application for children with ankle rheumatoid arthritis. Clin. Biomech. 1997, 12, S17. [Google Scholar] [CrossRef] [PubMed]
- Kul-Panza, E.; Berker, N. Pedobarographic findings in patients with knee osteoarthritis. Am. J. Phys. Med. Rehabil. 2006, 85, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.N.; Liang, W.D.; Zhou, F.H.; Li, H.T.; Zhang, L.X.; Zhang, Z.Q.; Li, J.J. Comparison of walking quality variables between incomplete spinal cord injury patients and healthy subjects by using a footscan plantar pressure system. Neural. Regen. Res. 2019, 14, 354–360. [Google Scholar] [PubMed]
- Qiu, X.; Tian, D.H.; Han, C.L.; Chen, W.; Wang, Z.J.; Mu, Z.Y.; Li, X.; Liu, K.-Z. Risk factors correlated with plantar pressure in Chinese patients with type 2 diabetes. Diabetes. Technol. Ther. 2013, 15, 1025–1032. [Google Scholar] [CrossRef] [PubMed]
- Buldt, A.K.; Forghany, S.; Landorf, K.B.; Levinger, P.; Murley, G.S.; Menz, H.B. Foot posture is associated with plantar pressure during gait: A comparison of normal, planus and cavus feet. Gait Posture 2018, 62, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.H.; Zhang, K.; Tan, G.Q.; Yang, J.; Liu, Z.C. Effects of obesity on dynamic plantar pressure distribution in Chinese prepubescent children during walking. Gait Posture 2013, 37, 37–42. [Google Scholar] [CrossRef]
- Aguirre-Guemez, A.V.; Perez-Sanpablo, A.I.; Quinzanos-Fresnedo, J.; Perez-Zavala, R.; Barrera-Ortiz, A. Walking speed is not the best outcome to evaluate the effect of robotic assisted gait training in people with motor incomplete Spinal Cord Injury: A Systematic Review with meta-analysis. J. Spinal Cord Med. 2019, 42, 142–154. [Google Scholar] [CrossRef]
- Yu, C.H.; Hung, Y.C.; Lin, Y.H.; Chen, G.X.; Wei, S.H.; Huang, C.H.; Chen, C.S. A 3D mathematical model to predict spinal joint and hip joint force for trans-tibial amputees with different SACH foot pylon adjustments. Gait Posture 2014, 40, 545–548. [Google Scholar] [CrossRef]
- Hsu, A.L.; Tang, P.F.; Jan, M.H. Analysis of impairments influencing gait velocity and asymmetry of hemiplegic patients after mild to moderate stroke. Arch. Phys. Med. Rehabil. 2003, 84, 1185–1193. [Google Scholar] [CrossRef]
- Joseph, G.B.; Hilton, J.F.; Jungmann, P.M.; Lynch, J.A.; Lane, N.E.; Liu, F.; Nevitt, M.C. Do persons with asymmetric hip pain or radiographic hip OA have worse pain and structure outcomes in the knee opposite the more affected hip? Data from the Osteoarthritis Initiative. Osteoarthr. Cartil. 2016, 24, 427–435. [Google Scholar] [CrossRef]
- Jungmann, P.M.; Nevitt, M.C.; Baum, T.; Liebl, H.; Nardo, L.; Liu, F.; Link, T.M. Relationship of unilateral total hip arthroplasty (THA) to contralateral and ipsilateral knee joint degeneration-a longitudinal 3T MRI study from the Osteoarthritis Initiative (OAI). Osteoarthr. Cartil. 2015, 23, 1144–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillam, M.H.; Lie, S.A.; Salter, A.; Furnes, O.; Graves, S.E.; Havelin, L.I.; Ryan, P. The progression of end-stage osteoarthritis: Analysis of data from the Australian and Norwegian joint replacement registries using a multi-state model. Osteoarthr. Cartil. 2013, 21, 405–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, W.; Huang, Z.; Wang, H.; Wang, D.; Luo, Z.; Bai, Y.; Zhou, Z. Supercapsular percutaneously-assisted total hip (SuperPath) versus posterolateral total hip arthroplasty in bilateral osteonecrosis of the femoral head: A pilot clinical trial. BMC Musculoskelet Disord 2019, 21, 2. [Google Scholar] [CrossRef] [Green Version]
- Xu, C.; Wen, X.X.; Huang, L.Y.; Shang, L.; Cheng, X.X.; Yan, Y.B.; Lei, W. Normal foot loading parameters and repeatability of the Footscan(R) platform system. J. Foot Ankle Res. 2017, 10, 30. [Google Scholar] [CrossRef] [Green Version]
- Favre, P.; Exner, G.U.; Drerup, B.; Schmid, D.; Wetz, H.H.; Jacob, H.A. The contralateral foot in children with unilateral clubfoot: A study of pressures and forces involved in gait. J. Pediatr. Orthop. 2007, 27, 54–59. [Google Scholar] [CrossRef]
- Lapointe, R.; Lajoie, Y.; Serresse, O.; Barbeau, H. Functional community ambulation requirements in incomplete spinal cord injured subjects. Spinal Cord. 2001, 39, 327–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pramodhyakul, N.; Amatachaya, P.; Sooknuan, T.; Arayawichanon, P.; Amatachaya, S. Effects of a visuotemporal cue on walking ability of independent ambulatory subjects with spinal cord injury as compared with healthy subjects. Spinal Cord. 2014, 52, 220–224. [Google Scholar] [CrossRef] [Green Version]
- Ismailidis, P.; Nuesch, C.; Kaufmann, M.; Clauss, M.; Pagenstert, G.; Eckardt, A.; Ilchmann, T.; Mündermann, A. Measuring gait kinematics in patients with severe hip osteoarthritis using wearable sensors. Gait Posture 2020, 81, 49–55. [Google Scholar] [CrossRef]
- Porta, M.; Pau, M.; Leban, B.; Deidda, M.; Sorrentino, M.; Arippa, F.; Marongiu, G. Lower Limb Kinematics in Individuals with Hip Osteoarthritis during Gait: A Focus on Adaptative Strategies and Interlimb Symmetry. Bioengineering 2021, 8, 47. [Google Scholar] [CrossRef]
- Soames, R.W. Foot pressure patterns during gait. J. Biomed. Eng. 1985, 7, 120–126. [Google Scholar] [CrossRef]
- Rusu, L.; Neamtu, M.C.; Rosulescu, E.; Cosma, G.; Dragomir, M.; Marin, M.I. Analysis of foot and ankle disorders and prediction of gait in multiple sclerosis rehabilitation. Eur. J. Med. Res. 2014, 19, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyrell, C.M.; Roos, M.A.; Rudolph, K.S.; Reisman, D.S. Influence of systematic increases in treadmill walking speed on gait kinematics after stroke. Phys. Ther. 2011, 91, 392–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, S.H.; Kim, C.O.; Kim, K.J.; Jeon, J.; Chang, H.; Kim, E.S.; Park, H. Quantitative analysis of the bilateral coordination and gait asymmetry using inertial measurement unit-based gait analysis. PLoS ONE 2019, 14, e0222913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plotnik, M.; Bartsch, R.P.; Zeev, A.; Giladi, N.; Hausdorff, J.M. Effects of walking speed on asymmetry and bilateral coordination of gait. Gait Posture 2013, 38, 864–869. [Google Scholar] [CrossRef] [Green Version]
- Reisman, D.S.; McLean, H.; Keller, J.; Danks, K.A.; Bastian, A.J. Repeated split-belt treadmill training improves poststroke step length asymmetry. Neurorehabil Neural Repair. 2013, 27, 460–468. [Google Scholar] [CrossRef] [Green Version]
- Silver, K.H.; Macko, R.F.; Forrester, L.W.; Goldberg, A.P.; Smith, G.V. Effects of aerobic treadmill training on gait velocity, cadence, and gait symmetry in chronic hemiparetic stroke: A preliminary report. Neurorehabil Neural Repair. 2000, 14, 65–71. [Google Scholar] [CrossRef]
- Awad, L.N.; Palmer, J.A.; Pohlig, R.T.; Binder-Macleod, S.A.; Reisman, D.S. Walking speed and step length asymmetry modify the energy cost of walking after stroke. Neurorehabil Neural Repair. 2015, 29, 416–423. [Google Scholar] [CrossRef] [Green Version]
- Savin, D.N.; Morton, S.M.; Whitall, J. Generalization of improved step length symmetry from treadmill to overground walking in persons with stroke and hemiparesis. Clin. Neurophysiol. 2014, 125, 1012–1020. [Google Scholar] [CrossRef] [Green Version]
- el-Gamal, Y.; Aly, R.H.; Hossny, E.; Afify, E.; el-Taliawy, D. Response of Egyptian infants with protein calorie malnutrition to hepatitis B vaccination. J. Trop. Pediatr. 1996, 42, 144–145. [Google Scholar] [CrossRef]


{kind=link}
| Items | Healthy Group | ONFH Group | p Value |
|---|---|---|---|
| Age (mean ± SD, years) | 54.71 ± 12.07 b | 56.00 ± 13.20 b | 0.69 |
| Female/male (n) | 14/17 | 17/14 | 1 |
| Height (mean ± SD, cm) | 163.77 ± 6.54 b | 164.77 ± 9.83 a | 0.64 |
| Body mass (mean ± SD, kg) | 66.19 ± 8.42 a | 70.06 ± 10.14 a | 0.11 |
| Body mass index (mean ± SD, kg/m2) | 24.66 ± 2.66 a | 25.85 ± 3.46 a | 0.14 |
| Variables | Healthy Group | ONFH Group | p Value |
|---|---|---|---|
| Walking speed (m/s) | 1.11 ± 0.24 a | 0.61 ± 0.20 a,* | <0.01 |
| Stride time (s) | 1.09 ± 0.10 a | 1.30 ± 0.16 b,* | <0.01 |
| Stance time (s) | 0.73 ± 0.07 a | 0.93 ± 0.12 a,* | <0.01 |
| Stance phase percentage (%) | 66.88 ± 5.29 a | 72.35 ± 6.21 a,* | <0.01 |
| Stride length (m) | 1.05 ± 0.10 a | 0.76 ± 0.19 a,* | <0.01 |
| Step length (m) | 0.53 ± 0.05 a | 0.37 ± 0.10 b,* | <0.01 |
| Healthy Group | Affected Side of ONFH Group | Healthy Side of ONFH Group | p Value | ||
|---|---|---|---|---|---|
| p a | p b | ||||
| Forefoot (%) | 21.49 ± 2.82 a | 20.19 ± 3.65 a | 23.24 ± 6.89 a | 0.12 | 0.20 |
| Hindfoot (%) | 29.87 ± 3.64 a | 23.67 ± 5.67 a,* | 32.90 ± 5.88 a,* | <0.01 | 0.02 |
| Total (%) | 51.36 ± 4.45 a | 43.87 ± 6.99 a,* | 56.13 ± 6.99 a,* | <0.01 | <0.01 |
| Healthy Group | Affected Side of ONFH Group | Healthy Side of ONFH Group | p Value | ||
|---|---|---|---|---|---|
| p a | p b | ||||
| T1(N/cm2) | 6.33 ± 2.42 a | 4.85 ± 2.84 a,* | 4.75 ± 2.95 a,* | 0.30 | 0.02 |
| T2-5(N/cm2) | 2.37 ± 1.80 b | 1.47 ± 1.21 b,* | 2.03 ± 1.82 b | 0.02 | 0.47 |
| M1(N/cm2) | 7.12 ± 3.58 a | 5.36 ± 3.19 a,* | 7.36 ± 4.28 a | 0.04 | 0.81 |
| M2(N/cm2) | 13.28 ± 3.76 b | 10.15 ± 5.0 a,* | 11.61 ± 4.88 a | <0.01 | 0.14 |
| M3(N/cm2) | 17.51 ± 5.18 a | 12.42 ± 4.89 a,* | 11.98 ± 5.33 a,* | <0.01 | <0.01 |
| M4(N/cm2) | 11.60 ± 4.4 a | 8.73 ± 4.05 a,* | 10.23 ± 5.44 b | 0.01 | 0.28 |
| M5(N/cm2) | 7.17 ± 4.69 b | 4.98 ± 3.59 b,* | 6.43 ± 4.15 b | 0.04 | 0.51 |
| MF(N/cm2) | 4.53 ± 1.73 b | 3.61 ± 1.4 a,* | 3.78 ± 1.26 a | 0.03 | 0.06 |
| HM(N/cm2) | 9.96 ± 2.28 a | 8.58 ± 2.72 a,* | 10.59 ± 3.27 a | 0.04 | 0.38 |
| HL(N/cm2) | 10.22 ± 3.22 b | 8.14 ± 2.41 a,* | 9.52 ± 3.07 a | <0.01 | 0.38 |
| Healthy Group | Affected Side of ONFH Group | Healthy Side of ONFH Group | p Value | ||
|---|---|---|---|---|---|
| p a | p b | ||||
| T1(%) | 6.20 ± 4.46 b | 6.52 ± 5.66 b | 5.30 ± 4.11 b | 0.80 | 0.42 |
| T2-5(%) | 1.46 ± 1.43 b | 1.36 ± 1.66 b | 1.60 ± 2.33 b | 0.79 | 0.78 |
| M1(%) | 6.63 ± 3.71 a | 8.48 ± 6.37 b | 8.02 ± 4.40 a | 0.17 | 0.18 |
| M2(%) | 12.33 ± 3.05 a | 10.05 ± 4.41 a,* | 11.69 ± 3.83 a | 0.02 | 0.48 |
| M3(%) | 13.01 ± 3.64 a | 9.93 ± 3.48 a,* | 10.06 ± 4.03 a,* | <0.01 | <0.01 |
| M4(%) | 9.29 ± 3.29 a | 7.73 ± 3.78 a | 8.65 ± 3.66 a | 0.09 | 0.47 |
| M5(%) | 7.38 ± 3.91 b | 5.20 ± 3.82 b,* | 5.49 ± 3.40 b,* | 0.03 | 0.05 |
| MF(%) | 18.68 ± 7.72 a | 17.84 ± 10.01 b | 16.39 ± 6.18 b | 0.72 | 0.20 |
| HM(%) | 13.50 ± 4.13 a | 19.22 ± 7.09 a,* | 18.86 ± 7.63 b,* | <0.01 | <0.01 |
| HL(%) | 11.43 ± 3.53 a | 13.54 ± 5.53 b,* | 13.78 ± 5.01 b,* | 0.08 | 0.04 |
| Healthy Group | Affected Side of ONFH Group | Healthy Side of ONFH Group | p Value | ||
|---|---|---|---|---|---|
| p a | p b | ||||
| T1(%) | 10.53 ± 1.76 a | 9.60 ± 2.32 b | 9.25 ± 3.56 a | 0.08 | 0.08 |
| T2-5(%) | 7.24 ± 3.29 b | 6.71 ± 3.55 a | 6.81 ± 3.53 a | 0.55 | 0.62 |
| M1(%) | 7.54 ± 1.22 b | 9.29 ± 2.45 a,* | 9.21 ± 2.11 a,* | <0.01 | <0.01 |
| M2(%) | 6.93 ± 0.51 b | 7.12 ± 1.81 b | 7.40 ± 0.88 a,* | 0.58 | <0.01 |
| M3(%) | 5.65 ± 0.44 b | 5.58 ± 1.40 b | 5.86 ± 0.88 a | 0.80 | 0.23 |
| M4(%) | 5.69 ± 0.51 b | 5.57 ± 1.49 b | 5.76 ± 1.13 a | 0.69 | 0.73 |
| M5(%) | 7.54 ± 1.13 b | 6.34 ± 1.95 b,* | 6.39 ± 1.72 a,* | <0.01 | <0.01 |
| MF(%) | 28.12 ± 2.87 b | 27.23 ± 7.01 b | 26.99 ± 4.67 b | 0.52 | 0.26 |
| HM(%) | 11.26 ± 1.27 b | 12.18 ± 1.83 a,* | 12.10 ± 1.26 a,* | 0.03 | <0.01 |
| HL(%) | 9.50 ± 1.14 b | 10.37 ± 1.69 a,* | 10.23 ± 1.17 a,* | 0.02 | <0.01 |
| Variables | Healthy Group | ONFH Group | p Value |
|---|---|---|---|
| Stride time SI | 0.02 ± 0.01 b | 0.05 ± 0.04 b,* | <0.01 |
| Stance time SI | 0.04 ± 0.05 b | 0.10 ± 0.09 b,* | <0.01 |
| Step length SI | 0.04 ± 0.04 a | 0.15 ± 0.16 b,* | <0.01 |
| Max F SI | 0.09 ± 0.06 b | 0.19 ± 0.17 b,* | <0.01 |
| Impulse SI | 0.11 ± 0.06 a | 0.22 ± 0.20 b,* | <0.01 |
| Contact area SI | 0.04 ± 0.03 a | 0.08 ± 0.10 b,* | 0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Z.; Mao, X.; Guo, Z.; Zhao, R.; Feng, T.; Xiang, C. Comparison of Walking Quality Variables between End-Stage Osteonecrosis of Femoral Head Patients and Healthy Subjects by a Footscan Plantar Pressure System. Medicina 2023, 59, 59. https://doi.org/10.3390/medicina59010059
Wang Z, Mao X, Guo Z, Zhao R, Feng T, Xiang C. Comparison of Walking Quality Variables between End-Stage Osteonecrosis of Femoral Head Patients and Healthy Subjects by a Footscan Plantar Pressure System. Medicina. 2023; 59(1):59. https://doi.org/10.3390/medicina59010059
Chicago/Turabian StyleWang, Zehua, Xingjia Mao, Zijian Guo, Ruipeng Zhao, Tengda Feng, and Chuan Xiang. 2023. "Comparison of Walking Quality Variables between End-Stage Osteonecrosis of Femoral Head Patients and Healthy Subjects by a Footscan Plantar Pressure System" Medicina 59, no. 1: 59. https://doi.org/10.3390/medicina59010059