

Informal Caregiving and Alzheimer’s Disease: The Psychological Effect


Abstract
:1. Introduction
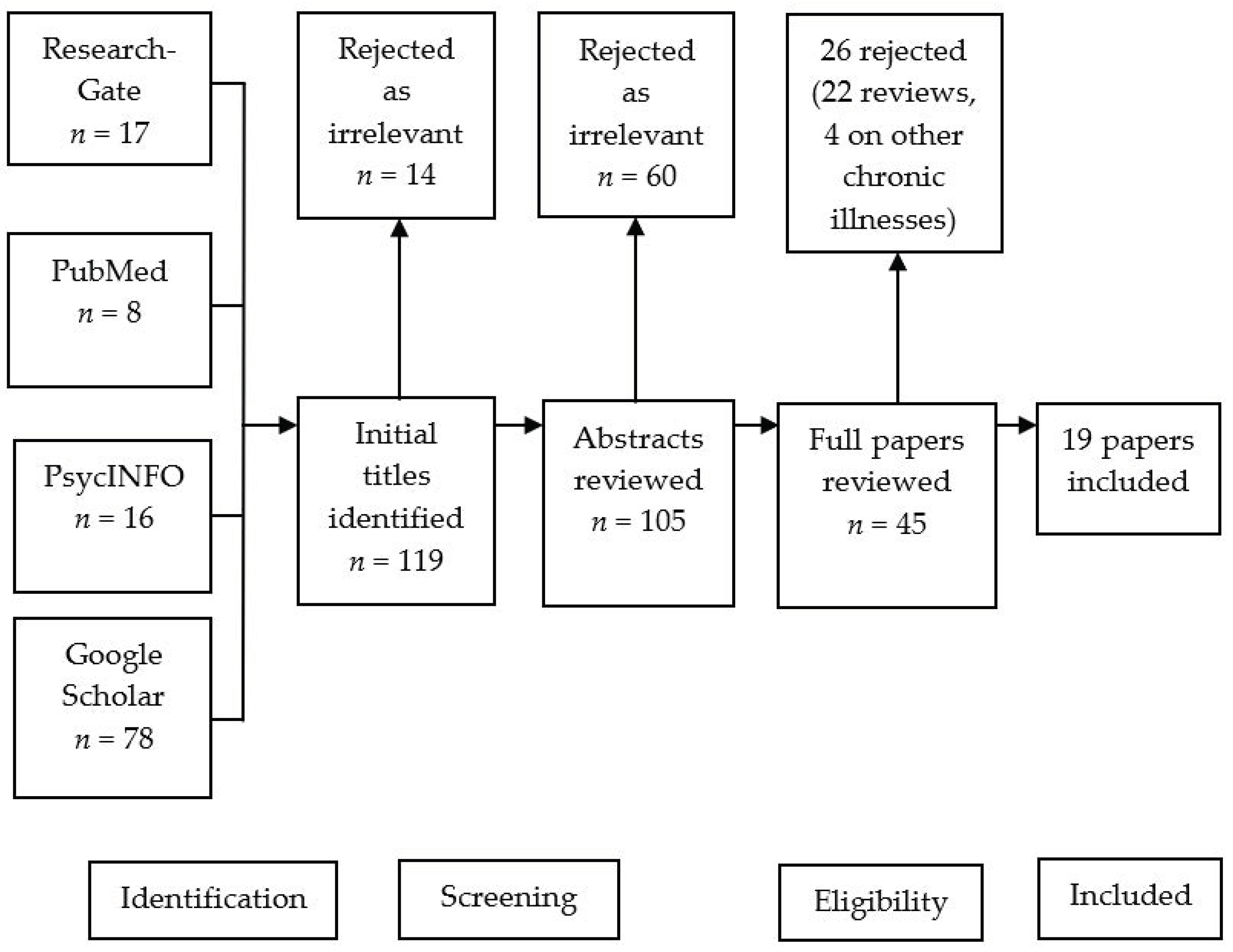
2. Materials and Methods
3. Results
3.1. Traditional Caregiving Ideologies
3.2. Non-Traditional Caregiving Ideologies (Exhaustion Factors)

{kind=link}
{kind=link}
| Authors | Method/Data Collection | Subjects | Country Setting | Findings |
|---|---|---|---|---|
| Miyawaki (2020) [17] | Structured interviews | n = 40 caregivers Description: 2nd, 2.5 and 3rd generation female Chinese-American caregivers caring after older relatives, some with dementia (NB. dementia type and number of carers for people with dementia not specified) | USA (Seattle and Houston) | Later generation caregivers had higher acculturation Filial responsibility remained high across generations Traditional caregiving was seen across all generations If the interviewed caregivers needed care in the future, their views upon this differed. Thus, caregivers from Seattle preferred the concept of longer-term care facilities whilst caregivers from Houston preferred being cared for by their children. This research emphasised the importance of caregiving attitudes and preferences being generationally and ethnically specific, and the importance of our understanding of this in a geographical context. |
| Sterritt and Pokorny (1998) [18] | Semi-structured interviews | n = 9 caregivers, with 3–8 years in caregiving; male and female African American Caregiver’s of relatives with Alzheimer’s Disease | South-Eastern USA | Found that caregiving is seen as a traditional family value Caregiving is thought of as an act of love Social support can be considered a mediator of caregiving burden Caregiving is considered to be a female role |
| Gray et al. (2009) [20] | Structured Interviews | n = 236 white, Hispanic, and Chinese-American women caring for relatives with either a diagnosis of Alzheimer’s Disease (or other dementia) | USA (San Francisco Bay area) | Attitudes and beliefs regarding AD/Dementia seen in Hispanic and Chinese caregivers may delay help-seeking activities for people with AD/Dementia. Hispanic and Chinese subjects were more likely to believe it to be a normal part of ageing diagnosable via a blood test than their white counterparts. This was attributed to their traditional and cultural beliefs. |
| Jones et al. (2011) [23] | Scale development | Questionnaires completed by 593 individuals. Filial concepts from scales using African-, Asian-, Euro-, Latino-, and Native American subjects were examined. | USA (Southern California and Native Americans) | Filial values predicted caregiving activities and caregiver health Three filial concepts were identified: Responsibility, Respect, and Care. These reflect attitudes and beliefs inherent in the complex multidimensional construct of filial values. A positive relationship between adult children professed filial values and their actual filial conduct was found. There was a stronger association between responsibility and care in males than females. Asians and African Americans displayed more filial responsibility. |
| Holland et al. (2010) [24] | Interventional study | n = 47 Chinese American dementia caregivers | USA (San Francisco Bay area) | Caregivers were found to report significant levels of distress, depressive symptoms, and also showed indications of resiliency—High levels of self-efficacy, positive caregiving experiences, and problem solving. Stronger beliefs in Asian values were associated with more normal cortisol patterns, less depressive symptoms, and greater self-efficacy, highlighting the salience of culture in shaping the caregiving experience of Chinese Americans. |
| Zhan (2004) [25] | Interviews | n = 4 Chinese-American caregivers of family members with AD | USA | There were ethnocultural and structural barriers facing the subjects; stigmatism of AD in the Chinese community, lack of knowledge about AD, a lack of culturally and linguistically appropriate AD services. There were negative impacts on mental and physical health. |
| Jones et al. (2001) [26] | Questionnaire based study | n = 50 Asian-American Women caregivers for aging parents (29 Chinese-American; 21 Filipino-American). All participants born outside of the USA. | USA | Involvement in caregiving was associated with health in Chinese-American women. Caregiving role integration was positively associated with all three perceived health measures in the Filipino group, but not in the Chinese group. Caregiving role satisfaction was consistently high in both groups. Caregiving role satisfaction and psychological well-being were significantly correlated for the combined group and for the Filipino caregivers. Total caregiving role stress was significantly correlated with overall health and current health only in the combined group. Support that helps to decrease role stress and to increase role satisfaction may be more effective than efforts to decrease the extent of role involvement. |
| Lawrence et al. (2008) [27] | In-depth interviews | n = 32 male and female caregivers of people with dementia (PwD) | UK (four socially and ethnically diverse south London boroughs: Lambeth, Southwark, Lewisham and Croydon) | Caregivers were identified as holding “traditional” or “non-traditional” caregiving ideologies. Within traditional ideologies caregiving was seen as a natural and honourable concept, something that is expected to happen. The majority of the South Asian, half of the Black Caribbean and a minority of the White British participants were found to possess a traditional ideology. |
| van de Ree et al. (2018) [29] | Structured Interviews | n = 123 informal caregivers of older adults (n = 22, 17.9%. had dementia; subtype not specified) | Netherlands (North Brabant) | Partners of the older adults provided more informal care than any other relative relationship. Female caregivers were 3-fold more likely to experiences relational problems due to caregiving. Majority of caregivers reported physical, mental and relational strain due to the intense nature of caregiving, particularly in the first six months. |
| Kang et al. (2016) [35] | Questionnaire based study | n = 87 caregivers of PwD (subtype unspecified) | Korea (Busan) | Caregiver burden, knowledge of dementia and levels of education predicted the quality of care given. Caregivers’ decreased QoLcame from caregiving burdens. Interventional and educational programmes aimed at reducing these burdens and increasing knowledge were deemed necessary to improve QoL and the quality of care given. |
| Shepherd-Banigan et al. (2020) [36] | Cross-sectional approach | n = 1509 familial caregivers of PwD within the Veteran Affairs (VA) programme (PwD = 44.9%) | USA (Nationwide) | Caregivers who care for veterans with trauma-based co-morbidities as well as cognitive decline reported high levels of depression, loneliness and financial strain even though they were part of the enhanced support system of the VA programme. Authors suggest a planned expansion of the programme to address these issues. |
| Harding et al. (2015) [37] | Secondary analysis | Data from 4 UK studies of informal caregivers of people with cancer (n = 105), dementia (n = 131; dementia subtype not specified) and acquired brain injury (n = 215) | UK (Sites not specified) | Caregivers’ burden was highest in those caring for acquired brain injury (ABI) and was followed by dementia caregivers’ burden. Total, subscale, and most individual elements of caregiver subjective burden differ between cancer, dementia, and ABI caregivers. However, concepts of duty, responsibility, and perception of financial situation were similar between the 3 groups. These should be considered when designing future intervention strategies to reduce caregivers’ burden in these groups. |
| Ku et al. (2019) [38] | Longitudinal study using interviews | n = 231 caregivers of PwD in a dementia clinic in Southern Taiwan | Taiwan (Tainan) | Behavioural disturbance [measured by the Neuropsychiatric Inventory (NPI)] showed no impact on the cost of care but was a significant predictor for caregiver burden. Caregiver burden was also associated with a functional decline in ADLs. Financial stability was associated with lower caregiver burden. These findings denote that financial assistance for low-income caregivers and educational training for behavioural disturbances are required to reduce caregiver burden. |
| Kang (2021) [39] | Secondary analysis | n = 956 unpaid family caregivers (National Long Term Care Survey, USA) | USA | The caregivers’ perceived burden was associated with financial strain, with variations due to familial relationships. The identification of these correlates can help with the development of effective interventions for caregivers’ burden. |
| Semiatin and O’Connor (2012) [40] | Interviews | n = 57 family caregivers of people with Alzheimer’s Disease | USA (Boston and Bedford) | Self-efficacy accounted for a significant percentage of the variance in positive aspects of caregiving after controlling for other factors commonly associated with positive aspects of caregiving including caregiver demographics, care recipient neuropsychiatric symptoms, and caregiver depression. High self-efficacy relates to caregivers’ perception of positive aspects of the caregiving experience. |
| Pendergrass et al. (2019) [41] | Cross-sectional study | n = 734 informal caregivers of PwD and other chronic illnesses | Germany (Bavaria) | There was an association between a higher experience of benefits, care duration, increase in depressive symptoms, increased physical grievances and a higher level of burden. |
| Horrell et al. (2015) [42] | Qualitative | n = 60 informal caregivers | New Zealand | The authors studied how emotions underpin informal caregiving. A caregiver’s choice of how they lived their lives was often influenced by their emotional attachment to the cared for, with higher attachment being associated with a decrease in wellbeing. The selflessness shown by the caregivers emphasised caregiving’s relational nature and challenged the prevalent perspective of caregiver burden documented previously. |
| Abreu et al. (2018) [43] | Cross-sectional study | n = 54 informal caregivers of PwD (n = 28 Alzheimer’s Disease, n = 12 vascular dementia, n = 9 mixed dementia, n = 2 Dementia with Lewy Bodies, n = 3 frontotemporal lobe dementia) | Portugal (Porto district) | Psychological distress was documented in half of the caregivers. Somatization, obsessive–compulsion, interpersonal sensitivity, anxiety, and paranoid ideation were seen in a large proportion of caregivers. The authors suggested placing focus on the alleviation of caregivers through education and additional support to help decrease their distress and burden |
| Laparidou et al. (2019) [44] | Qualitative | n = 35, 18 caregivers, 17 healthcare professionals | UK (Lincolnshire) | Primary stressors on caregivers came from lack of knowledge regarding Dementias and the challenge of diagnosis, often due to lack of understanding by healthcare-professionals. Secondary stressors were due the need for support and communication issues with healthcare professionals. The authors suggest that these stressors may be effecting the caregivers’ wellbeing r and may lead to an unnecessary move to institutionalised care for the care-recipient. |
3.3. Financial Status
3.4. Personal Growth
3.5. Ability to Care and Level of Support
4. Discussion
4.1. Traditional Caregiving Ideologies
4.2. Non-Traditional Caregiving Ideologies (Exhaustion Factors)
4.3. Financial Status
4.4. Personal Growth
4.5. Ability to Care and Level of Support
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aburto, J.M.; Kashyap, R.; Schöley, J.; Angus, C.; Ermisch, J.; Mills, M.C.; Dowd, J.B. Estimating the burden of the COVID-19 pandemic on mortality, life expectancy and lifespan inequality in England and Wales: A population-level analysis. J. Epidemiol. Community Health 2021, 75, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, L.; Richards, C.; Cohen, L. Older adults and perspectives for researchers and clinicians working in health psychology and behavioral medicine. In The Wiley Encyclopaedia of Health Psychology; Sweeny, M.L., Robbins, M.L., Cohen, L.M., Eds.; Wiley: New York, NY, USA, 2020; pp. 365–371. [Google Scholar] [CrossRef]
- Office for National Statistics. Overview of the UK Population; Office for National Statistics: London, UK, 2021.
- Graham, R. Facts about Carers. Care UK Policy Briefing. 2019. Available online: https://www.carersuk.org/images/Facts_about_Carers_2019.pdf (accessed on 10 October 2021).
- Licchetta, M.; Stelmach, M. Fiscal Sustainability and Public Spending on Health; Office for Budget Responsibility: London, UK, 2016.
- Stoye, G.; Zaranko, B. UK Health Spending; (No. R165); IFS Report; Institute for Fiscal Studies: London, UK, 2019. [Google Scholar]
- Allen, A.P.; Buckley, M.M.; Cryan, J.F.; Ní Chorcoráin, A.; Dinan, T.G.; Kearney, P.M.; Molloy, D.W. Informal caregiving for dementia patients: The contribution of patient characteristics and behaviours to caregiver burden. Age Ageing 2019, 49, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Fields, B.; Makaroun, L.; Rodriguez, K.L.; Robinson, C.; Forman, J.; Rosland, A.M. Caregiver role development in chronic disease: A qualitative study of informal caregiving for veterans with diabetes. Chronic. Illn. 2022, 18, 193–205. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Kumar, A.; Sidhu, J.; Goyal, A.; Tsao, J.W. Alzheimer disease. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Stall, N.M.; Kim, S.J.; Hardacre, K.A.; Shah, P.S.; Straus, S.E.; Bronskill, S.E.; Lix, L.M.; Bell, C.M.; Rochon, P.A. Association of informal caregiver distress with health outcomes of community-dwelling dementia care recipients: A systematic review. J. Am. Geriatr. Soc. 2019, 67, 609–617. [Google Scholar] [CrossRef]
- Wittenberg, R.; Knapp, M.; Hu, B.; Comas-Herrera, A.; King, D.; Rehill, A.; Shi, C.; Banerjee, S.; Patel, A.; Jagger, C.; et al. The costs of dementia in England. Int. J. Geriatr. Psychiatry 2019, 34, 1095–1103. [Google Scholar] [CrossRef] [Green Version]
- Williams, K.N.; Perkhounkova, Y.; Shaw, C.A.; Hein, M.; Vidoni, E.D.; Coleman, C.K. Supporting family caregivers with technology for dementia home care: A randomized controlled trial. Innov. Aging 2019, 3, igz037. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, N.M.; Gitlin, L.N.; Parisi, J.M.; Roth, D.L.; Gross, A.L. Association of physical functioning of persons with dementia with caregiver burden and depression in dementia caregivers: An integrative data analysis. Aging Ment. Health 2019, 23, 587–594. [Google Scholar] [CrossRef]
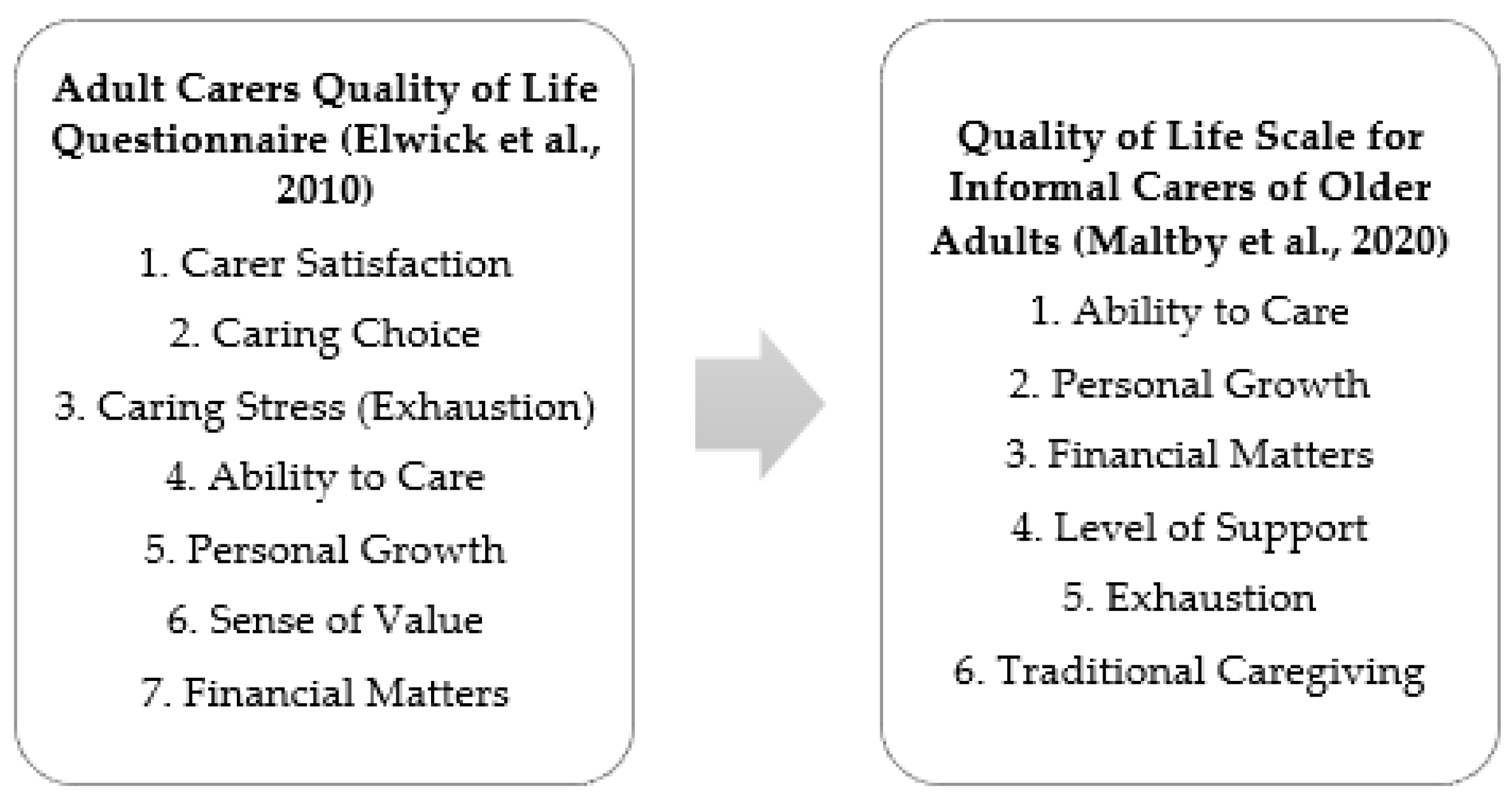
- Maltby, J.; Hogervorst, E.; Stephan, B.; Sun, X.; Tang, P.; Law, E.; Mukaetova-Ladinska, E.B. The development of a Quality of Life Scale for Informal Carers for Older Adults. Gerontol. Geriatr. Med. 2020, 6, 2333721420920424. [Google Scholar] [CrossRef]
- Elwick, H.; Joseph, S.; Becker, S.; Becker, F. Manual for the Adult Carer Quality of Life Questionnaire (AC-QoL); The Princess Royal Trust for Carers: London, UK, 2010. [Google Scholar]
- Miyawaki, C.E. Caregiving attitudes and needs of later-generation Chinese-American family caregivers of older adults. J. Fam. Issues 2020, 41, 2377–2399. [Google Scholar] [CrossRef]
- Sterritt, P.F.; Pokorny, M.E. African-American caregiving for a relative with Alzheimer’s disease. Geriatr. Nurs. 1990, 19, 127–134. [Google Scholar] [CrossRef]
- Connell, C.M.; Gibson, G.D. Racial, ethnic, and cultural differences in dementia caregiving: Review and analysis. Gerontologist 1997, 37, 355–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gray, H.L.; Jimenez, D.E.; Cucciare, M.A.; Tong, H.Q.; Gallagher-Thompson, D. Ethnic differences in beliefs regarding Alzheimer disease among dementia family caregivers. Am. J. Geriatr. Psychiatry 2009, 17, 925–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bieber, A.; Nguyen, N.; Meyer, G.; Stephan, A. Influences on the access to and use of formal community care by people with dementia and their informal caregivers: A scoping review. BMC Health Serv. Res. 2019, 19, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weng, S.S.; Nguyen, P.V. Factors affecting elder caregiving in multigenerational Asian American families. Fam. Soc. J. Contemp. Soc. Serv. (FIS) 2011, 92, 329–335. [Google Scholar] [CrossRef]
- Jones, P.S.; Lee, J.W.; Zhang, X.E. Clarifying and measuring filial concepts across five cultural groups. Res. Nurs. Health 2011, 34, 310–326. [Google Scholar] [CrossRef] [Green Version]
- Holland, J.M.; Thompson, L.W.; Tzuang, M.; Gallagher-Thompson, D. Psychosocial factors among Chinese American women dementia caregivers and their association with salivary cortisol: Results of an exploratory study. Ageing Int. 2010, 35, 109–127. [Google Scholar] [CrossRef]
- Zhan, L. Caring for family members with Alzheimer’s disease: Perspectives from Chinese American caregivers. J. Gerontol. Nurs. 2004, 30, 19–29. [Google Scholar] [CrossRef]
- Jones, P.S.; Jaceldo, K.B.; Lee, J.R.; Zhang, X.E.; Meleis, A.I. Role integration and perceived health in Asian American women caregivers. Res. Nurs. Health 2001, 24, 133–144. [Google Scholar] [CrossRef]
- Lawrence, V.; Murray, J.; Samsi, K.; Banerjee, S. Attitudes and support needs of Black Caribbean, South Asian and White British carers of people with dementia in the UK. Br. J. Psychiatry 2008, 193, 240–246. [Google Scholar] [CrossRef]
- Cross, A.J.; Garip, G.; Sheffield, D. The psychosocial impact of caregiving in dementia and quality of life: A systematic review and meta-synthesis of qualitative research. Psychol. Health 2018, 33, 1321–1342. [Google Scholar] [CrossRef]
- van de Ree, C.L.; Ploegsma, K.; Kanters, T.A.; Roukema, J.A.; De Jongh, M.A.; Gosens, T. Care-related Quality of Life of informal caregivers of the elderly after a hip fracture. J. Patient Rep. Outcomes 2018, 2, 23. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Heffernan, C.; Tan, J. Caregiver burden: A concept analysis. Int. J. Nur. Sci. 2020, 7, 438–445. [Google Scholar] [CrossRef]
- Walker, A.J.; Pratt, C.C.; Eddy, L. Informal caregiving to aging family members: A critical review. Fam. Relat. 1995, 44, 402–411. [Google Scholar] [CrossRef]
- Given, B.A.; Sherwood, P.; Given, C.W. Support for caregivers of cancer patients: Transition after active treatment. Cancer Epidemiol. Biomark. Prev. 2011, 20, 2015–2021. [Google Scholar] [CrossRef] [Green Version]
- Ribé, J.M.; Salamero, M.; Pérez-Testor, C.; Mercadal, J.; Aguilera, C.; Cleris, M. Quality of life in family caregivers of schizophrenia patients in Spain: Caregiver characteristics, caregiving burden, family functioning, and social and professional support. Int. J. Psychiatry Clin. Pract. 2018, 22, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Molassiotis, A.; Tan, J.Y.; Chung, B.P.M.; Huang, H.Q. Prevalence and correlates of unmet palliative care needs in dyads of Chinese patients with advanced cancer and their informal caregivers: A cross-sectional survey. Support. Care Cancer 2021, 29, 1683–1698. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.M.; Kim, J.S.; Jeong, J.H. Factors influencing quality of caregiving by caregivers for elders with dementia. J. Korean Acad. Community Health Nurs. 2016, 27, 193–201. [Google Scholar] [CrossRef] [Green Version]
- Shepherd-Banigan, M.; Sherman, S.R.; Lindquist, J.H.; Miller, K.E.; Tucker, M.; Smith, V.A.; Van Houtven, C.H. Family caregivers of veterans experience high levels of burden, distress, and financial strain. J. Am. Geriatr. Soc. 2020, 68, 2675–2683. [Google Scholar] [CrossRef]
- Harding, R.; Gao, W.; Jackson, D.; Pearson, C.; Murray, J.; Higginson, I.J. Comparative analysis of informal caregiver burden in advanced cancer, dementia, and acquired brain injury. J. Pain Symptom Manag. 2015, 50, 445–452. [Google Scholar] [CrossRef]
- Ku, L.J.E.; Chang, S.M.; Pai, M.C.; Hsieh, H.M. Predictors of caregiver burden and care costs for older persons with dementia in Taiwan. Int. Psychogeriatr. 2019, 31, 885–894. [Google Scholar] [CrossRef]
- Kang, S.Y. Financial strain among unpaid family caregivers of frail elders in community. J. Hum. Behav. Soc. Environ. 2021, 31, 582–598. [Google Scholar] [CrossRef]
- Semiatin, A.M.; O’Connor, M.K. The relationship between self-efficacy and positive aspects of caregiving in Alzheimer’s disease caregivers. Aging Ment. Health 2012, 16, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Pendergrass, A.; Mittelman, M.; Graessel, E.; Özbe, D.; Karg, N. Predictors of the personal benefits and positive aspects of informal caregiving. Aging Ment. Health 2019, 23, 1533–1538. [Google Scholar] [CrossRef] [PubMed]
- Horrell, B.; Stephens, C.; Breheny, M. Capability to care: Supporting the health of informal caregivers for older people. Health Psychol. 2015, 34, 339–348. [Google Scholar] [CrossRef]
- Reinhard, S.C.; Given, B.; Petlick, N.H.; Bemis, A. Supporting family caregivers in providing care. In Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2008. [Google Scholar]
- Laparidou, D.; Middlemass, J.; Karran, T.; Siriwardena, A.N. Caregivers’ interactions with health care services–Mediator of stress or added strain? Experiences and perceptions of informal caregivers of people with dementia—A qualitative study. Dementia 2019, 8, 2526–2542. [Google Scholar] [CrossRef]
- Bastawrous, M. Caregiver burden—A critical discussion. Int. J. Nurs. Stud. 2013, 50, 431–441. [Google Scholar] [CrossRef]
- Spencer, S.; Swinglehurst, D. Supporting carers. InnovAiT 2020, 13, 213–217. [Google Scholar] [CrossRef]
- Jones, C. Spotlight on carers. Int. Psychogeriatr. 2022, 34, 775–777. [Google Scholar] [CrossRef]
- Swartz, K.; Collins, L.G. Caregiver care. Am. Fam. Physician 2019, 99, 699–706. [Google Scholar]
- Tremont, G. Family caregiving in dementia. Med. Health Rhode Isl. 2011, 94, 36–38. [Google Scholar]
- National Research Council. Informal caregivers in the United States: Prevalence, caregiver characteristics, and ability to provide care. In The Role of Human Factors in Home Health Care: Workshop Summary; National Academies Press (US): Washington, DC, USA, 2010. [Google Scholar]
- Abreu, W.; Rodrigues, T.; Sequeira, C.; Pires, R.; Sanhudo, A. The experience of psychological distress in family caregivers of people with dementia: A cross-sectional study. Perspec. Psychiatr. Care 2018, 54, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Hampton, M.M.; Newcomb, P. Self-efficacy and stress among informal caregivers of individuals at end of life. J. Hosp. Palliat. Nurs. 2018, 20, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Vandepitte, S.; Van Den Noortgate, N.; Putman, K.; Verhaeghe, S.; Verdonck, C.; Annemans, L. Effectiveness of respite care in supporting informal caregivers of persons with dementia: A systematic review. Int. J. Geriatr. Psychiatry 2016, 31, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, C.; Balamurali, T.B.S.; Gill Livingston, G. A systematic review of the prevalence and covariates of anxiety in caregivers of people with dementia. Int. Psychogeriatr. 2007, 19, 175–195. [Google Scholar] [CrossRef] [PubMed]
- Belanche, D.; Casaló, L.V.; Flavián, C.; Schepers, J. Service robot implementation: A theoretical framework and research agenda. Serv. Ind. J. 2020, 40, 203–225. [Google Scholar] [CrossRef] [Green Version]
- Blott, J. Smart homes for the future of dementia care. Lancet Neurol. 2021, 20, 264. [Google Scholar] [CrossRef]
- Fields, N.; Xu, L.; Greer, J.; Murphy, E. Shall I compare thee… to a robot? An exploratory pilot study using participatory arts and social robotics to improve psychological well-being in later life. Aging Ment. Health 2021, 25, 575–584. [Google Scholar] [CrossRef]
- Garcia-Constantino, M.F.; Orr, C.; Synnott, J.; Shewell, C.P.; Ennis, A.; Cleland, I.; Nugent, C.; Raffert, J.; Morrison, G.; Larkham, L.; et al. Design and implementation of a smart home in a box to monitor the wellbeing of residents with dementia in care homes. Front. Digit. Health 2021, 3, 798889. [Google Scholar] [CrossRef]
- Goodall, G.; Taraldsen, K.; Serrano, J.A. The use of technology in creating individualized, meaningful activities for people living with dementia: A systematic review. Dementia 2021, 20, 1442–1469. [Google Scholar] [CrossRef]


| Participant Identification Terms | Caregiving Terms | Wellbeing Terms | Further Terms |
|---|---|---|---|
| Dementia | Caregiver | Stress | Ability to Care |
| Alzheimer’s | Carer | Depression | Finance |
| Alzheimer’s Disease | Informal Caregiver | Anxiety | Money |
| Elderly | Caregiving | Quality of Life | Personal Growth |
| Old Age | Support | Depressive Symptoms | Positive Experience |
| Older Age | Anxious Symptoms | Negative Experience | |
| Cognitive Decline | Mental Health | Traditional Views | |
| Wellbeing | Non-traditional views | ||
| Caregiving Views | |||
| Ideologies |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hellis, E.; Mukaetova-Ladinska, E.B. Informal Caregiving and Alzheimer’s Disease: The Psychological Effect. Medicina 2023, 59, 48. https://doi.org/10.3390/medicina59010048
Hellis E, Mukaetova-Ladinska EB. Informal Caregiving and Alzheimer’s Disease: The Psychological Effect. Medicina. 2023; 59(1):48. https://doi.org/10.3390/medicina59010048
Chicago/Turabian StyleHellis, Emily, and Elizabeta B. Mukaetova-Ladinska. 2023. "Informal Caregiving and Alzheimer’s Disease: The Psychological Effect" Medicina 59, no. 1: 48. https://doi.org/10.3390/medicina59010048