

Bone Regenerative Potential of Cross-Linked Collagen Membrane in Peri-Implant Osseous Defect: Case Series with Histologic/Micro-Computed Tomographic Findings

Abstract
:1. Introduction
2. Case Presentation
2.1. Surgical Procedure
2.1.1. Implant Placement and GBR
2.1.2. Uncovering Procedure
2.2. Micro-Computed Tomographic (Micro-CT) Examination and Histologic Evaluation
3. Results
3.1. Clinical Findings
3.2. Micro-CT Findings
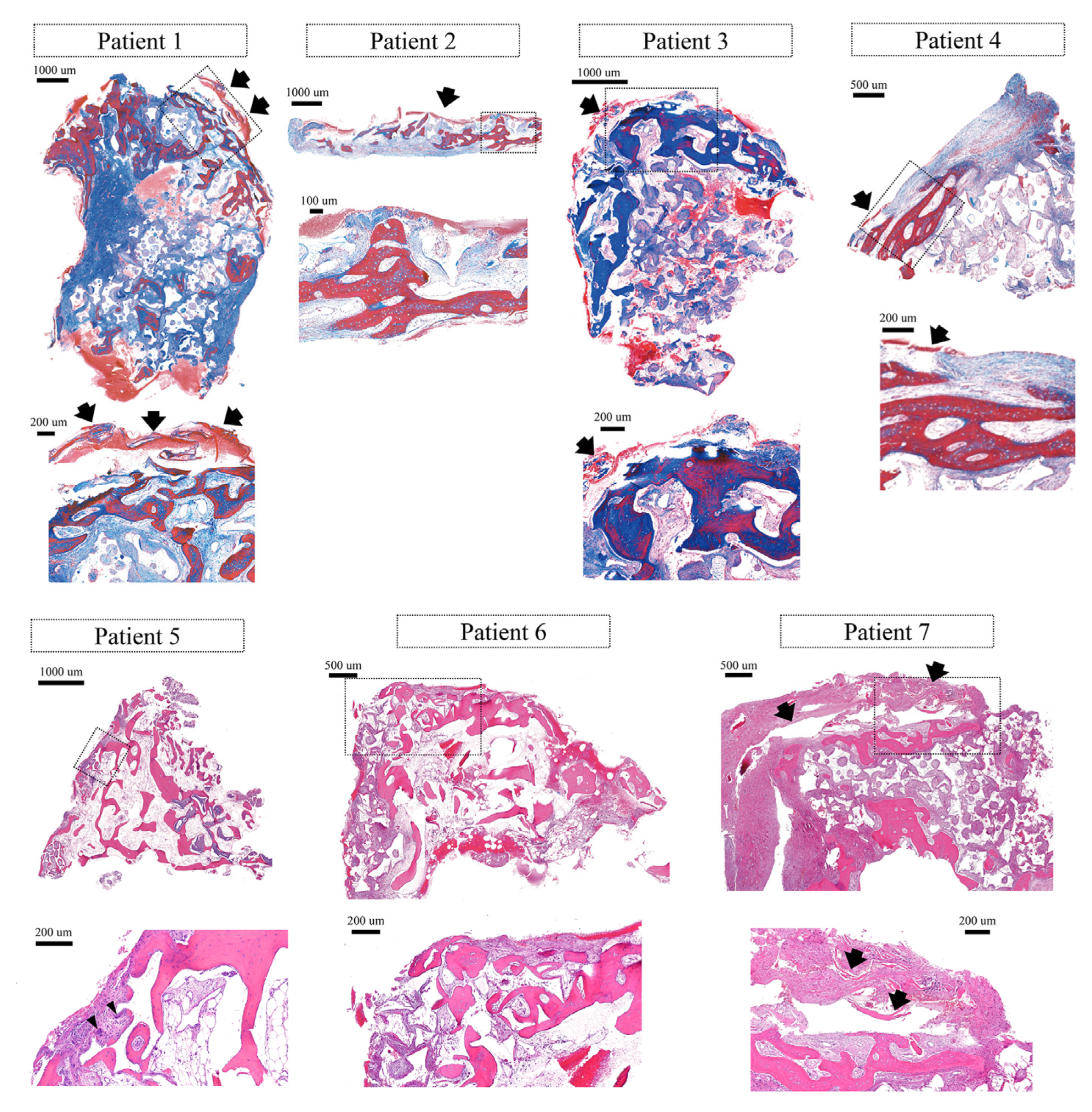
3.3. Histological Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dahlin, C.; Linde, A.; Gottlow, J.; Nyman, S. Healing of Bone Defects by Guided Tissue Regeneration. Plast. Reconstr. Surg. 1988, 81, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Schenk, R.K.; Buser, D.; Hardwick, W.R.; Dahlin, C. Healing pattern of bone regeneration in membrane-protected defects: A histologic study in the canine mandible. Int. J. Oral Maxillofac. Implant. 1994, 9, 13–29. [Google Scholar]
- Simion, M.; Dahlin, C.; Rocchietta, I.; Stavropoulos, A.; Sánchez, R.; Karring, T. Vertical ridge augmentation with guided bone regeneration in association with dental implants: An experimental study in dogs. Clin. Oral Implant. Res. 2007, 18, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Fontana, F.; Santoro, F.; Maiorana, C.; Iezzi, G.; Piattelli, A.; Simion, M. Clinical and histologic evaluation of allogeneic bone matrix versus autogenous bone chips associated with titanium-reinforced e-PTFE membrane for vertical ridge augmentation: A prospective pilot study. Int. J. Oral Maxillofac. Implant. 2008, 23, 1003–1012. [Google Scholar]
- Chiapasco, M.; Zaniboni, M. Clinical outcomes of GBR procedures to correct peri-implant dehiscences and fenestrations: A systematic review. Clin. Oral Implant. Res. 2009, 20 (Suppl. S4), 113–123. [Google Scholar] [CrossRef]
- Soldatos, N.K.; Stylianou, P.; Angelov, N.; Koidou, P.; Yukna, R.; Romanos, G.E. Limitations and options using resorbable versus nonresorbable membranes for successful guided bone regeneration. Quintessence Int. 2017, 48, 131–147. [Google Scholar]
- Sheikh, Z.; Qureshi, J.; Alshahrani, A.M.; Nassar, H.; Ikeda, Y.; Glogauer, M.; Ganss, B. Collagen based barrier membranes for periodontal guided bone regeneration applications. Odontology 2016, 105, 1–12. [Google Scholar] [CrossRef]
- Friedmann, A.; Strietzel, F.P.; Maretzki, B.; Pitaru, S.; Bernimoulin, J.-P. Histological assessment of augmented jaw bone utilizing a new collagen barrier membrane compared to a standard barrier membrane to protect a granular bone substitute material. Clin. Oral Implant. Res. 2002, 13, 587–594. [Google Scholar] [CrossRef]
- Naenni, N.; Schneider, D.; Jung, R.E.; Hüsler, J.; Hämmerle, C.H.F.; Thoma, D.S. Randomized clinical study assessing two membranes for guided bone regeneration of peri-implant bone defects: Clinical and histological outcomes at 6 months. Clin. Oral Implant. Res. 2017, 28, 1309–1317. [Google Scholar] [CrossRef] [Green Version]
- Zitzmann, N.U.; Naef, R.; Schärer, P. Resorbable versus nonresorbable membranes in combination with Bio-Oss for guided bone regeneration. Int. J. Oral Maxillofac. Implant. 1997, 12, 844–852. [Google Scholar]
- Poomprakobsri, K.; Kan, J.Y.; Rungcharassaeng, K.; Lozada, J.; Oyoyo, U. Exposure of Barriers Used in Guided Bone Regeneration: Rate, Timing, Management, and Effect on Grafted Bone—A Retrospective Analysis. J. Oral Implant. 2022, 48, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Naenni, N.; Lim, H.-C.; Strauss, F.-J.; Jung, R.E.; Hämmerle, C.H.F.; Thoma, D.S. Local tissue effects of various barrier membranes in a rat subcutaneous model. J. Periodontal Implant. Sci. 2020, 50, 327–339. [Google Scholar] [CrossRef] [PubMed]
- Sbricoli, L.; Guazzo, R.; Annunziata, M.; Gobbato, L.; Bressan, E.; Nastri, L. Selection of Collagen Membranes for Bone Regeneration: A Literature Review. Materials 2020, 13, 786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, I.; Khalid, A.W.; Pae, H.-C.; Cha, J.-K.; Lee, J.-S.; Paik, J.-W.; Jung, U.-W.; Choi, S.-H. Distinctive bone regeneration of calvarial defects using biphasic calcium phosphate supplemented ultraviolet-crosslinked collagen membrane. J. Periodontal Implant. Sci. 2020, 50, 14–27. [Google Scholar] [CrossRef]
- Hong, I.; Khalid, A.W.; Pae, H.-C.; Song, Y.W.; Cha, J.-K.; Lee, J.-S.; Paik, J.-W.; Choi, S.-H. Diverse patterns of bone regeneration in rabbit calvarial defects depending on the type of collagen membrane. J. Periodontal Implant. Sci. 2021, 51, 40–52. [Google Scholar] [CrossRef]
- Urban, I.; Traxler, H.; Romero-Bustillos, M.; Farkasdi, S.; Bartee, B.; Baksa, G.; Avila-Ortiz, G. Effectiveness of Two Different Lingual Flap Advancing Techniques for Vertical Bone Augmentation in the Posterior Mandible: A Comparative, Split-Mouth Cadaver Study. Int. J. Periodontics Restor. Dent. 2018, 38, 35–40. [Google Scholar] [CrossRef]
- Wang, H.-L.; Boyapati, L. “PASS” Principles for Predictable Bone Regeneration. Implant. Dent. 2006, 15, 8–17. [Google Scholar] [CrossRef] [Green Version]
- Alajmi, B.; Karobari, M.I.; Aldowah, O. Treatment of a large through and through periapical lesion using guided tissue regeneration: A case report of 2 years follow-up. Clin. Case Rep. 2022, 10, e6405. [Google Scholar] [CrossRef]
- Wessing, B.; Lettner, S.; Zechner, W. Guided Bone Regeneration with Collagen Membranes and Particulate Graft Materials: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 87–100. [Google Scholar] [CrossRef]
- Owens, K.W.; Yukna, R.A. Collagen Membrane Resorption in Dogs: A Comparative Study. Implant. Dent. 2001, 10, 49–58. [Google Scholar] [CrossRef]
- Rothamel, D.; Schwarz, F.; Sager, M.; Herten, M.; Sculean, A.; Becker, J. Biodegradation of differently cross-linked collagen membranes: An experimental study in the rat. Clin. Oral Implant. Res. 2005, 16, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-Y.; Jung, I.-H.; Kim, Y.-K.; Lim, H.-C.; Lee, J.-S.; Jung, U.-W.; Choi, S.-H. Guided bone regeneration using 1-ethyl-3-(3-dimethylaminopropyl) carbodiimide (EDC)-cross-linked type-I collagen membrane with biphasic calcium phosphate at rabbit calvarial defects. Biomater. Res. 2015, 19, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cha, J.; Pla, R.; Vignoletti, F.; Jung, U.; Sanz-Esporrin, J.; Sanz, M. Immunohistochemical characteristics of lateral bone augmentation using different biomaterials around chronic peri-implant dehiscence defects: An experimental in vivo study. Clin. Oral Implant. Res. 2021, 32, 569–580. [Google Scholar] [CrossRef]
- Zubery, Y.; Goldlust, A.; Alves, A.; Nir, E. Ossification of a Novel Cross-Linked Porcine Collagen Barrier in Guided Bone Regeneration in Dogs. J. Periodontol. 2007, 78, 112–121. [Google Scholar] [CrossRef]
- Zubery, Y.; Nir, E.; Goldlust, A. Ossification of a Collagen Membrane Cross-Linked by Sugar: A Human Case Series. J. Periodontol. 2008, 79, 1101–1107. [Google Scholar] [CrossRef]
- Cucchi, A.; Sartori, M.; Aldini, N.N.; Vignudelli, E.; Corinaldesi, G. A Proposal of Pseudo-periosteum Classification after GBR by Means of Titanium-Reinforced d-PTFE Membranes or Titanium Meshes Plus Cross-Linked Collagen Membranes. Int. J. Periodontics Restor. Dent. 2019, 39, e157–e165. [Google Scholar] [CrossRef]
- Paeng, K.; Cha, J.; Thoma, D.S.; Jung, R.E.; Jung, U.; Benic, G.I. Effect of collagen membrane and of bone substitute on lateral bone augmentation with titanium mesh: An experimental in vivo study. Clin. Oral Implant. Res. 2022, 33, 413–423. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Case | Age/Sex | Smoking | Systemic Diseases | GBR Sites | Implant Timing | Defect Morphology | Implant Diameter × Length | Wound Dehiscence/Membrane Exposure | Healing Period (Months) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 73/M | No | No self-reported | #13 #14 | immediate | wide gap defect, partial loss of septal bone, fenestration on the #13 area | 3.8 × 12 3.8 × 12 | No | 5 |
| 2 | 59/M | No | Hypertension, Diabetes mellitus | #35 #36 | immediate | wide gap defect, substantial loss of the buccal bone plate | 4.3 × 10 4.8 × 10 | No | 5 |
| 3 | 72/F | No | No self-reported | #16 #17 | immediate | exposure of thread on the coronal half of the #17 implant | 4.3 × 10 4.3 × 10 | No | 6 |
| 4 | 75/M | No | No self-reported | #14 | 2 months after extraction | large dehiscence on the buccal and palatal aspects | 4.3 × 12 | No | 4 |
| 5 | 67/M | Yes | No self-reported | #24 #25 | 2 months after extraction | wide gap defect, total loss of the buccal bone plate on the #24 implant | 4.3 × 10 4.3 × 10 | No | 7 |
| 6 | 62/M | Yes | No self-reported | #46 | 2 months after extraction | gap defect with partial loss of the buccal bone plate | 6.0 × 10 | No | 6 |
| 7 | 72/M | No | No self-reported | #46 | 2 months after extraction | gap defect on the coronal 1/3 of the #46 implant | 4.3 × 10 | No | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, W.-B.; Crasto, G.J.; Han, J.-Y.; Kang, P.; Lim, H.-C. Bone Regenerative Potential of Cross-Linked Collagen Membrane in Peri-Implant Osseous Defect: Case Series with Histologic/Micro-Computed Tomographic Findings. Medicina 2023, 59, 176. https://doi.org/10.3390/medicina59010176
Park W-B, Crasto GJ, Han J-Y, Kang P, Lim H-C. Bone Regenerative Potential of Cross-Linked Collagen Membrane in Peri-Implant Osseous Defect: Case Series with Histologic/Micro-Computed Tomographic Findings. Medicina. 2023; 59(1):176. https://doi.org/10.3390/medicina59010176
Chicago/Turabian StylePark, Won-Bae, Gazelle Jean Crasto, Ji-Young Han, Philip Kang, and Hyun-Chang Lim. 2023. "Bone Regenerative Potential of Cross-Linked Collagen Membrane in Peri-Implant Osseous Defect: Case Series with Histologic/Micro-Computed Tomographic Findings" Medicina 59, no. 1: 176. https://doi.org/10.3390/medicina59010176