

Early Onset Intrauterine Growth Restriction—Data from a Tertiary Care Center in a Middle-Income Country
 and
and
Abstract
:1. Introduction
2. Materials and Methods
- ○
- In prestage I (defined as EFW between 10th centile and the 3rd centile), we used weekly US monitoring regardless of the GA—amniotic fluid volume assessment (using the deepest vertical pocket technique—DVP [24]), fetal biophysical profile (BPP) [25] and Doppler interrogation at the two fetal sites (UmbA and MCA), the CPR, both UtA and pulsatility index (PI); in this stage, we used US for EFW every two weeks. If the BPP and Dopplers were normal, expectance was proposed until 32 WG, and the case was discarded from the study. If the BPP was abnormal, the case was followed up daily. If there was a persistent abnormal BPP (below 5, two days consecutively), we performed elective C-section before 32 WG, regardless of the Doppler results.
- ○
- In stage I by Figueras [26] (EFW < 3rd centile or CPR < 5th centile or any UtA PI > 95th centile), we offered the same weekly monitoring protocol and the same management. If the BPP was normal, we monitored until we registered the case as advancing toward stage II or until progressing over 32 WG. If the BPP was abnormal, the case was followed up daily. If the BPP was persistently abnormal (below 5, two days consecutively), we added the DV assessment, and we performed an elective C-section before 32 WG regardless of the Doppler results.
- ○
- In stage II by Figueras [26]—defined as UmbA absent end-diastolic velocity (AEDV)—we offered hospitalization. If the parents declined admittance, we re-examined twice a week. Inpatients were also offered twice-weekly additional cardiotocography (CTG) and DV assessment daily. In this stage, we performed an elective C-section before 32 WG in all cases.
- ○
- In stage III by Figueras [26]—defined as UmbA reversed end-diastolic velocity (REDV), we monitored cases by US daily. In surviving fetuses, we offered delivery by cesarean section before 30 weeks based on the DV assessment.
- ○
- In stage IV by Figueras [26]—defined as reversed flow ductus venosus (DV), we offered immediate delivery after 27 weeks by caesarean section to all couples. Benefits and expectations were extensively explained to the parents in these cases.
Statistical Analysis
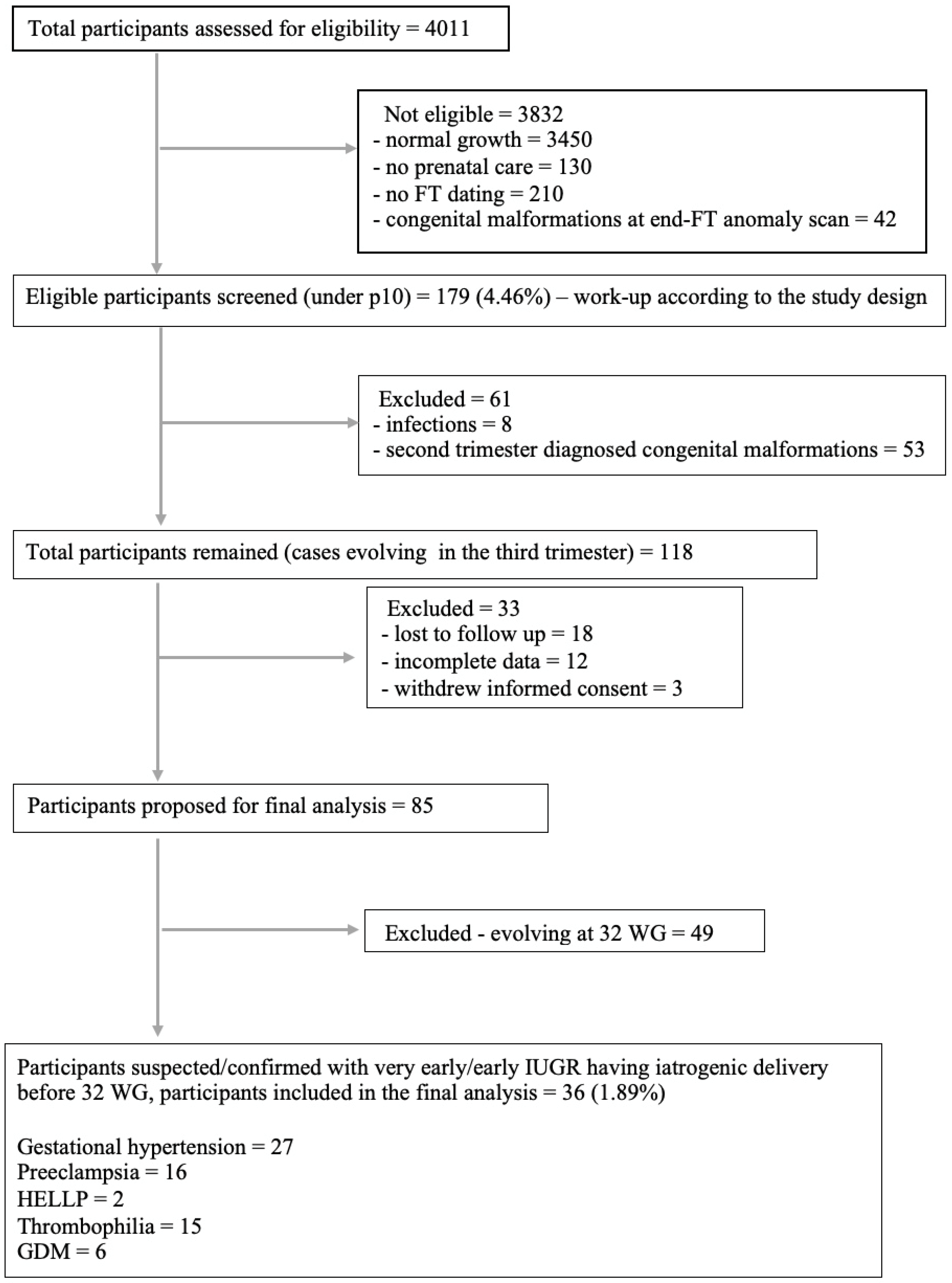
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Gordijn, S.J.; Beune, I.M.; Thilaganathan, B.; Papageorghiou, A.; Baschat, A.A.; Baker, P.N.; Silver, R.M.; Wynia, K.; Ganzevoort, W. Consensus definition of fetal growth restriction: A Delphi procedure. Ultrasound Obstet. Gynecol. 2016, 48, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Ganzevoort, W.; Alfirevic, Z.; von Dadelszen, P.; Kenny, L.; Papageorghiou, A.; van Wassenaer-Leemhuis, A.; Gluud, C.; Mol, B.W.; Baker, P.N. STRIDER: Sildenafil Therapy In Dismal prognosis Early-onset intrauterine growth Restriction—A protocol for a systematic review with individual participant data and aggregate data meta-analysis and trial sequential analysis. Syst. Rev. 2014, 3, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Dadelszen, P.; Dwinnell, S.; Magee, L.A.; Carleton, B.C.; Gruslin, A.; Lee, B.; Lim, K.I.; Liston, R.M.; Miller, S.P.; Rurak, D.; et al. Sildenafil citrate therapy for severe early-onset intrauterine growth restriction. BJOG 2011, 118, 624–628. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Conner, E.L.; Charafeddine, L.; Woods, J.R., Jr.; Del Priore, G. A critical birth weight and other determinants of survival for infants with severe intrauterine growth restriction. Ann. N. Y. Acad. Sci. 2001, 943, 326–339. [Google Scholar] [CrossRef]
- Batton, D.G.; DeWitte, D.B.; Espinosa, R.; Swails, T.L. The impact of fetal compromise on outcome at the border of viability. Am. J. Obstet. Gynecol. 1998, 178, 909–915. [Google Scholar] [CrossRef]
- Petersen, S.G.; Wong, S.F.; Urs, P.; Gray, P.H.; Gardener, G.J. Early onset, severe fetal growth restriction with absent or reversed end-diastolic flow velocity waveform in the umbilical artery: Perinatal and long-term outcomes. Aust. N. Z. J. Obstet. Gynaecol. 2009, 49, 45–51. [Google Scholar] [CrossRef]
- Ganzevoort, W.; Rep, A.; de Vries, J.I.; Bonsel, G.J.; Wolf, H.; PETRA-Investigators. Prediction of maternal complications and adverse infant outcome at admission for temporizing management of early-onset severe hypertensive disorders of pregnancy. Am. J. Obstet. Gynecol. 2006, 195, 495–503. [Google Scholar] [CrossRef]
- Guellec, I.; Lapillonne, A.; Renolleau, S.; Charlaluk, M.L.; Roze, J.C.; Marret, S.; Vieux, R.; Monique, K.; Ancel, P.Y.; Group, E.S. Neurologic outcomes at school age in very preterm infants born with severe or mild growth restriction. Pediatrics 2011, 127, e883–e891. [Google Scholar] [CrossRef] [PubMed]
- Carter, E.B.; Tuuli, M.G.; Caughey, A.B.; Odibo, A.O.; Macones, G.A.; Cahill, A.G. Number of prenatal visits and pregnancy outcomes in low-risk women. J. Perinatol. 2016, 36, 178–181. [Google Scholar] [CrossRef] [Green Version]
- Peleg, D.; Kennedy, C.M.; Hunter, S.K. Intrauterine growth restriction: Identification and management. Am. Fam. Physician 1998, 58, 453–460, 466–467. [Google Scholar]
- Cosmi, E.; Fanelli, T.; Visentin, S.; Trevisanuto, D.; Zanardo, V. Consequences in infants that were intrauterine growth restricted. J. Pregnancy 2011, 2011, 364381. [Google Scholar] [CrossRef] [PubMed]
- Hadlock, F.P.; Harrist, R.B.; Carpenter, R.J.; Deter, R.L.; Park, S.K. Sonographic estimation of fetal weight. The value of femur length in addition to head and abdomen measurements. Radiology 1984, 150, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Iliescu, D.; Tudorache, S.; Comanescu, A.; Antsaklis, P.; Cotarcea, S.; Novac, L.; Cernea, N.; Antsaklis, A. Improved detection rate of structural abnormalities in the first trimester using an extended examination protocol. Ultrasound Obstet. Gynecol. 2013, 42, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Tudorache, S.; Cara, M.; Iliescu, D.G.; Novac, L.; Cernea, N. First trimester two- and four-dimensional cardiac scan: Intra- and interobserver agreement, comparison between methods and benefits of color Doppler technique. Ultrasound Obstet. Gynecol. 2013, 42, 659–668. [Google Scholar] [CrossRef] [Green Version]
- Strauss, K.J.; Kaste, S.C. The ALARA (as low as reasonably achievable) concept in pediatric interventional and fluoroscopic imaging: Striving to keep radiation doses as low as possible during fluoroscopy of pediatric patients—A white paper executive summary. Pediatr. Radiol. 2006, 36 (Suppl. S2), 110–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhide, A.; Acharya, G.; Baschat, A.; Bilardo, C.M.; Brezinka, C.; Cafici, D.; Ebbing, C.; Hernandez-Andrade, E.; Kalache, K.; Kingdom, J.; et al. ISUOG Practice Guidelines (updated): Use of Doppler velocimetry in obstetrics. Ultrasound Obstet. Gynecol. 2021, 58, 331–339. [Google Scholar] [CrossRef]
- Shennan, A.; Suff, N.; Jacobsson, B.; FIGO Working Group for Preterm Birth. FIGO good practice recommendations on magnesium sulfate administration for preterm fetal neuroprotection. Int. J. Gynecol. Obstet. 2021, 155, 31–33. [Google Scholar] [CrossRef]
- Norman, J.; Shennan, A.; Jacobsson, B.; Stock, S.J.; FIGO Working Group for Preterm Birth. FIGO good practice recommendations on the use of prenatal corticosteroids to improve outcomes and minimize harm in babies born preterm. Int. J. Gynaecol. Obstet. 2021, 155, 26–30. [Google Scholar] [CrossRef]
- Gomez, O.; Figueras, F.; Fernandez, S.; Bennasar, M.; Martinez, J.M.; Puerto, B.; Gratacos, E. Reference ranges for uterine artery mean pulsatility index at 11–41 weeks of gestation. Ultrasound Obstet. Gynecol. 2008, 32, 128–132. [Google Scholar] [CrossRef]
- Acharya, G.; Wilsgaard, T.; Berntsen, G.K.; Maltau, J.M.; Kiserud, T. Reference ranges for serial measurements of umbilical artery Doppler indices in the second half of pregnancy. Am. J. Obstet. Gynecol. 2005, 192, 937–944. [Google Scholar] [CrossRef]
- Figueras, F.; Fernandez, S.; Eixarch, E.; Gomez, O.; Martinez, J.M.; Puerto, B.; Gratacos, E. Middle cerebral artery pulsatility index: Reliability at different sampling sites. Ultrasound Obstet. Gynecol. 2006, 28, 809–813. [Google Scholar] [CrossRef]
- Kessler, J.; Rasmussen, S.; Hanson, M.; Kiserud, T. Longitudinal reference ranges for ductus venosus flow velocities and waveform indices. Ultrasound Obstet. Gynecol. 2006, 28, 890–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciobanu, A.; Wright, A.; Syngelaki, A.; Wright, D.; Akolekar, R.; Nicolaides, K.H. Fetal Medicine Foundation reference ranges for umbilical artery and middle cerebral artery pulsatility index and cerebroplacental ratio. Ultrasound Obstet. Gynecol. 2019, 53, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Magann, E.F.; Chauhan, S.P.; Washington, W.; Whitworth, N.S.; Martin, J.N.; Morrison, J.C. Ultrasound estimation of amniotic fluid volume using the largest vertical pocket containing umbilical cord: Measure to or through the cord? Ultrasound Obstet. Gynecol. 2002, 20, 464–467. [Google Scholar] [CrossRef]
- Manning, F.A.; Platt, L.D.; Sipos, L. Antepartum fetal evaluation: Development of a fetal biophysical profile. Am. J. Obstet. Gynecol. 1980, 136, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Figueras, F.; Gratacos, E. Update on the diagnosis and classification of fetal growth restriction and proposal of a stage-based management protocol. Fetal Diagn. Ther. 2014, 36, 86–98. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes, A. Gestational diabetes mellitus. Diabetes Care 2003, 26 (Suppl. S1), S103–S105. [Google Scholar] [CrossRef] [Green Version]
- American College of Obstetricians and Gynecologists. Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222. Obstet. Gynecol. 2020, 135, e237–e260. [Google Scholar] [CrossRef]
- Haram, K.; Svendsen, E.; Abildgaard, U. The HELLP syndrome: Clinical issues and management. A Review. BMC Pregnancy Childbirth 2009, 9, 8. [Google Scholar] [CrossRef] [Green Version]
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins–Obstetrics. ACOG Practice Bulletin No. 197: Inherited Thrombophilias in Pregnancy. Obstet. Gynecol. 2018, 132, e18–e34. [Google Scholar] [CrossRef]
- Lee, A.C.; Cousens, S.; Wall, S.N.; Niermeyer, S.; Darmstadt, G.L.; Carlo, W.A.; Keenan, W.J.; Bhutta, Z.A.; Gill, C.; Lawn, J.E. Neonatal resuscitation and immediate newborn assessment and stimulation for the prevention of neonatal deaths: A systematic review, meta-analysis and Delphi estimation of mortality effect. BMC Public Health 2011, 11 (Suppl. S3), S12. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Kalache, K.D.; Kadar, N. Timing the delivery of the preterm severely growth-restricted fetus: Venous Doppler, cardiotocography or the biophysical profile? Ultrasound Obstet. Gynecol. 2002, 19, 118–121. [Google Scholar] [CrossRef] [PubMed]
- Bilardo, C.M.; Hecher, K.; Visser, G.H.A.; Papageorghiou, A.T.; Marlow, N.; Thilaganathan, B.; Van Wassenaer-Leemhuis, A.; Todros, T.; Marsal, K.; Frusca, T.; et al. Severe fetal growth restriction at 26–32 weeks: Key messages from the TRUFFLE study. Ultrasound Obstet. Gynecol. 2017, 50, 285–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirzaei, F.; Farzad-Mahajeri, Z. Association of hereditary thrombophilia with intrauterine growth restriction. Iran. J. Reprod. Med. 2013, 11, 275–278. [Google Scholar]
- Jaddoe, V.W.; Verburg, B.O.; de Ridder, M.A.; Hofman, A.; Mackenbach, J.P.; Moll, H.A.; Steegers, E.A.; Witteman, J.C. Maternal smoking and fetal growth characteristics in different periods of pregnancy: The generation R study. Am. J. Epidemiol. 2007, 165, 1207–1215. [Google Scholar] [CrossRef] [Green Version]
- Quinton, A.E.; Cook, C.M.; Peek, M.J. The relationship between cigarette smoking, endothelial function and intrauterine growth restriction in human pregnancy. BJOG 2008, 115, 780–784. [Google Scholar] [CrossRef]
- Pels, A.; Beune, I.M.; van Wassenaer-Leemhuis, A.G.; Limpens, J.; Ganzevoort, W. Early-onset fetal growth restriction: A systematic review on mortality and morbidity. Acta Obstet. Gynecol. Scand. 2020, 99, 153–166. [Google Scholar] [CrossRef] [Green Version]
- Lees, C.; Marlow, N.; Arabin, B.; Bilardo, C.M.; Brezinka, C.; Derks, J.B.; Duvekot, J.; Frusca, T.; Diemert, A.; Ferrazzi, E.; et al. Perinatal morbidity and mortality in early-onset fetal growth restriction: Cohort outcomes of the trial of randomized umbilical and fetal flow in Europe (TRUFFLE). Ultrasound Obstet. Gynecol. 2013, 42, 400–408. [Google Scholar] [CrossRef]
- Unterscheider, J.; Cuzzilla, R. Severe early-onset fetal growth restriction: What do we tell the prospective parents? Prenat. Diagn. 2021, 41, 1363–1371. [Google Scholar] [CrossRef]
- Gardosi, J.; Giddings, S.; Buller, S.; Southam, M.; Williams, M. Preventing stillbirths through improved antenatal recognition of pregnancies at risk due to fetal growth restriction. Public Health 2014, 128, 698–702. [Google Scholar] [CrossRef]
- Verlijsdonk, J.W.; Winkens, B.; Boers, K.; Scherjon, S.; Roumen, F. Suspected versus non-suspected small-for-gestational age fetuses at term: Perinatal outcomes. J. Matern. Fetal Neonatal Med. 2012, 25, 938–943. [Google Scholar] [CrossRef] [PubMed]
- Ewigman, B.G.; Crane, J.P.; Frigoletto, F.D.; LeFevre, M.L.; Bain, R.P.; McNellis, D. Effect of prenatal ultrasound screening on perinatal outcome. RADIUS Study Group. N. Engl. J. Med. 1993, 329, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Lees, C.C.; Stampalija, T.; Baschat, A.; da Silva Costa, F.; Ferrazzi, E.; Figueras, F.; Hecher, K.; Kingdom, J.; Poon, L.C.; Salomon, L.J.; et al. ISUOG Practice Guidelines: Diagnosis and management of small-for-gestational-age fetus and fetal growth restriction. Ultrasound Obstet. Gynecol. 2020, 56, 298–312. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics and the Society forMaternal-FetalMedicin. ACOG Practice Bulletin No. 204: Fetal Growth Restriction. Obstet. Gynecol. 2019, 133, e97–e109. [Google Scholar] [CrossRef] [PubMed]
- Grivell, R.M.; Wong, L.; Bhatia, V. Regimens of fetal surveillance for impaired fetal growth. Cochrane Database Syst. Rev. 2012, 2012, CD007113. [Google Scholar] [CrossRef] [Green Version]
- Vollgraff Heidweiller-Schreurs, C.A.; De Boer, M.A.; Heymans, M.W.; Schoonmade, L.J.; Bossuyt, P.M.M.; Mol, B.W.J.; De Groot, C.J.M.; Bax, C.J. Prognostic accuracy of cerebroplacental ratio and middle cerebral artery Doppler for adverse perinatal outcome: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2018, 51, 313–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oros, D.; Ruiz-Martinez, S.; Staines-Urias, E.; Conde-Agudelo, A.; Villar, J.; Fabre, E.; Papageorghiou, A.T. Reference ranges for Doppler indices of umbilical and fetal middle cerebral arteries and cerebroplacental ratio: Systematic review. Ultrasound Obstet. Gynecol. 2019, 53, 454–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meher, S.; Hernandez-Andrade, E.; Basheer, S.N.; Lees, C. Impact of cerebral redistribution on neurodevelopmental outcome in small-for-gestational-age or growth-restricted babies: A systematic review. Ultrasound Obstet. Gynecol. 2015, 46, 398–404. [Google Scholar] [CrossRef]
- Cnossen, J.S.; Morris, R.K.; ter Riet, G.; Mol, B.W.; van der Post, J.A.; Coomarasamy, A.; Zwinderman, A.H.; Robson, S.C.; Bindels, P.J.; Kleijnen, J.; et al. Use of uterine artery Doppler ultrasonography to predict pre-eclampsia and intrauterine growth restriction: A systematic review and bivariable meta-analysis. CMAJ 2008, 178, 701–711. [Google Scholar] [CrossRef] [Green Version]
- Unterscheider, J.; Daly, S.; Geary, M.P.; Kennelly, M.M.; McAuliffe, F.M.; O’Donoghue, K.; Hunter, A.; Morrison, J.J.; Burke, G.; Dicker, P.; et al. Optimizing the definition of intrauterine growth restriction: The multicenter prospective PORTO Study. Am. J. Obstet. Gynecol. 2013, 208, 290.e1-6. [Google Scholar] [CrossRef]
- Gaccioli, F.; Aye, I.; Sovio, U.; Charnock-Jones, D.S.; Smith, G.C.S. Screening for fetal growth restriction using fetal biometry combined with maternal biomarkers. Am. J. Obstet. Gynecol. 2018, 218, S725–S737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hecher, K.; Bilardo, C.M.; Stigter, R.H.; Ville, Y.; Hackeloer, B.J.; Kok, H.J.; Senat, M.V.; Visser, G.H. Monitoring of fetuses with intrauterine growth restriction: A longitudinal study. Ultrasound Obstet. Gynecol. 2001, 18, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Miranda, J.; Rodriguez-Lopez, M.; Triunfo, S.; Sairanen, M.; Kouru, H.; Parra-Saavedra, M.; Crovetto, F.; Figueras, F.; Crispi, F.; Gratacos, E. Prediction of fetal growth restriction using estimated fetal weight vs a combined screening model in the third trimester. Ultrasound Obstet. Gynecol. 2017, 50, 603–611. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | susp Early IUGR | Control | p |
|---|---|---|---|
| Smoking/former smoker | 66.67% | 21.4% | <0.01 |
| Age | 29.17 (19–37) | 27.17 (18–35) | 0.053 |
| BMI | 24.5 (19–27) | 27.0 (17–31) | 0.374 |
| Variable | susp Early IUGR | Control | p |
|---|---|---|---|
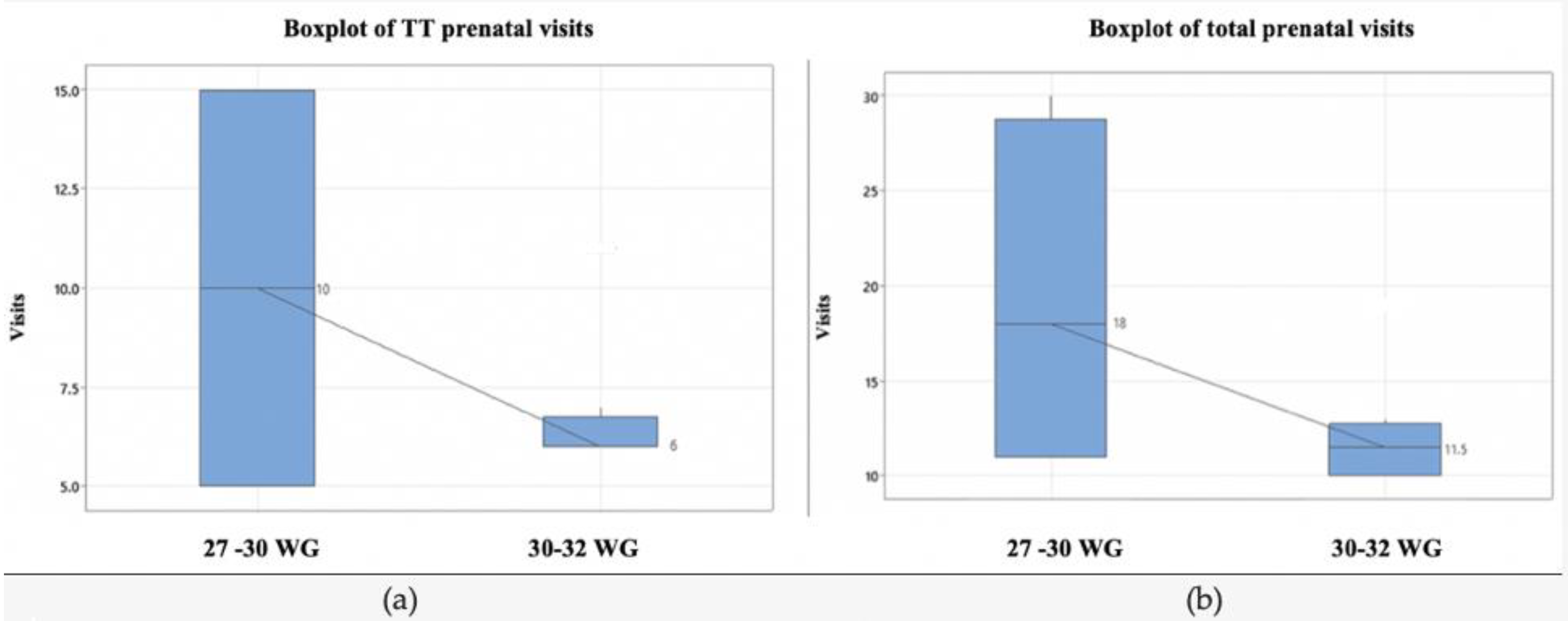
| Nr of prenatal visits | 11.5 (10–30) | 5 (5–6) | <0.01 |
| Nr of prenatal visits in the TT | 6 (5–15) | 2 (1–3) | <0.01 |
| Characteristic/Complications | susp Early IUGR | Controls | p |
|---|---|---|---|
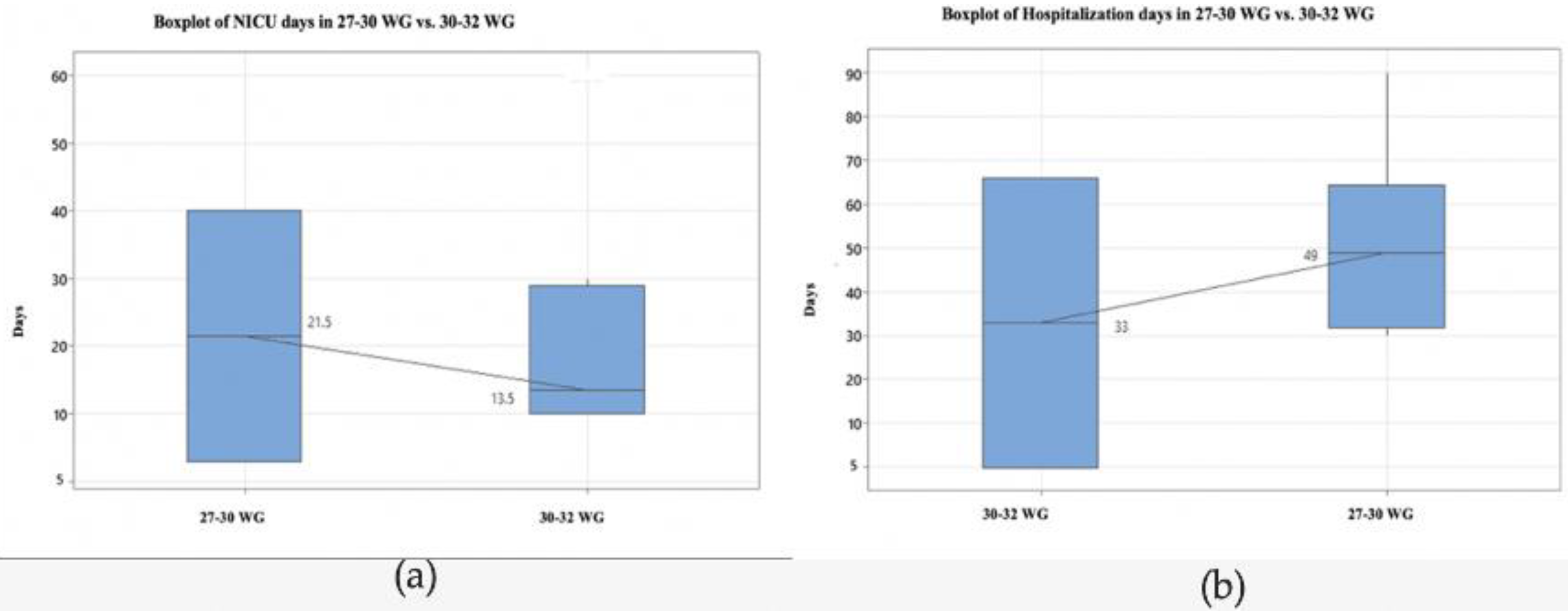
| Hospitalization days | 36 (22–90) | 3.8 (2–5) | <0.01 |
| Apgar Score | 5.5 (1–8) | ||
| Resuscitation | 17 (47.2%) | ||
| Birth percentile | 1% (1–10%) | ||
| NICU days | 10.5 (0–60) | ||
| Respiratory Distress Syndrome | 20 (55.5%) | ||
| Bronchopulmonary Dysplasia | 1 (2.7%) | ||
| Transient Apnea | 36 (100%) | ||
| Hypotension | 4 (11.1%) | ||
| PDA | 15 (41.6%) | ||
| IVH | 6 (16.6%) | ||
| PVL | 2 (5.5%) | ||
| Hypothermia | 0 | ||
| Immature GI System | 32 (88.8%) | ||
| NEC | 1 (2.7%) | ||
| Anemia | 36 (100%) | ||
| Jaundice | 10 (27.7%) | ||
| Transient Hypoglycaemia | 16 (44.4%) | ||
| Infection | 9 (25%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dinu, M.; Badiu, A.M.; Hodorog, A.D.; Stancioi-Cismaru, A.F.; Gheonea, M.; Grigoras Capitanescu, R.; Sirbu, O.C.; Tanase, F.; Bernad, E.; Tudorache, S. Early Onset Intrauterine Growth Restriction—Data from a Tertiary Care Center in a Middle-Income Country. Medicina 2023, 59, 17. https://doi.org/10.3390/medicina59010017
Dinu M, Badiu AM, Hodorog AD, Stancioi-Cismaru AF, Gheonea M, Grigoras Capitanescu R, Sirbu OC, Tanase F, Bernad E, Tudorache S. Early Onset Intrauterine Growth Restriction—Data from a Tertiary Care Center in a Middle-Income Country. Medicina. 2023; 59(1):17. https://doi.org/10.3390/medicina59010017
Chicago/Turabian StyleDinu, Marina, Anne Marie Badiu, Andreea Denisa Hodorog, Andreea Florentina Stancioi-Cismaru, Mihaela Gheonea, Razvan Grigoras Capitanescu, Ovidiu Costinel Sirbu, Florentina Tanase, Elena Bernad, and Stefania Tudorache. 2023. "Early Onset Intrauterine Growth Restriction—Data from a Tertiary Care Center in a Middle-Income Country" Medicina 59, no. 1: 17. https://doi.org/10.3390/medicina59010017