
Matrix Metalloproteinase-9 Level in Synovial Fluid—Association with Joint Destruction in Early Rheumatoid Arthritis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Measurements
2.2.1. MMP–9 Measurement
2.2.2. Laboratory Analyses
2.2.3. Radiography of Joints
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scott, L.D.; Wolfe, F.; Huizinga, T.W. Rheumatoid Arthritis. Lancet 2010, 376, 1094–1108. [Google Scholar] [CrossRef]
- Xue, M.; McKelvey, K.; Shen, K.; Minhas, N.; March, L.; Park, S.-Y.; Jackson, C.J. Endogenous MMP-9 and not MMP-2 promotes rheumatoid synovial fibroblast survival, inflammation and cartilage degradation. Rheumatology 2014, 53, 2270–2279. [Google Scholar] [CrossRef] [Green Version]
- Cabral-Pacheco, G.A.; Garza-Veloz, I.; Castruita-De la Rosa, C.; Ramirez-Acuña, J.M.; Perez-Romero, B.A.; Guerrero-Rodriguez, J.F.; Martinez-Avila, N.; Martinez-Fierro, M.L. The Roles of Matrix Metalloproteinases and Their Inhibitors in Human Diseases. Int. J. Mol. Sci. 2020, 21, 9739. [Google Scholar] [CrossRef] [PubMed]
- Giannelli, G.; Erriquez, R.; Iannon, F.; Marinosci, F.; Lapadula, G.; Antonaci, S. MMP-2, MMP-9, TIMP-1 and TIMP-2 levels in patients with rheumatoid arthritis and psoriatic arthritis. Clin. Exp. Rheumatol. 2004, 22, 335–338. [Google Scholar] [PubMed]
- Ahrens, D.; Koch, A.E.; Pope, R.M.; Stein-Picarella, M.; Niedbala, M.J. Expression of matrix metalloproteinase 9 (96-kd gelatinase B) in human rheumatoid arthritis. Arthritis Rheum. 1996, 39, 1576–1587. [Google Scholar] [CrossRef]
- Xue, M.; March, L.; Sambrook, P.N.; Jackson, C.J. Differential regulation of matrix metalloproteinase 2 and matrix metalloproteinase 9 by activated protein C: Relevance to inflammation in rheumatoid arthritis. Arthritis Rheum 2007, 56, 2864–2874. [Google Scholar] [CrossRef] [PubMed]
- Itoh, T.; Matsuda, H.; Tanioka, M.; Kuwabara, K.; Itohara, S.; Suzuki, R. The Role of Matrix Metalloproteinase-2 and Matrix Metalloproteinase-9 in Antibody-Induced arthritis. J. Immunol. 2002, 169, 2643–2647. [Google Scholar] [CrossRef] [Green Version]
- Nagase, H.; Visse, R.; Murphy, G. Structure and function of matrix metalloproteinases and TIMPs. Cardiovasc. Res. 2006, 69, 562–573. [Google Scholar] [CrossRef] [Green Version]
- Takaishi, H.; Kimura, T.; Dalal, S.; Okada, Y.; D’Armiento, J. Joint diseases and matrix metalloproteinases: A role for MMP-13. Curr. Pharm. Biotechnol. 2008, 9, 47–54. [Google Scholar] [CrossRef]
- Smolen, J.S.; Landewé, R.B.; Bijlsma, J.W.; Burmester, G.R.; Dougados, M.; Kerschbaumer, A.; McInnes, I.B.; Sepriano, A.; van Vollenhoven, R.F.; de Wit, M.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann. Rheum. Dis. 2020, 79, 685–699. [Google Scholar] [CrossRef]
- Aletaha, D.; Smolen, J.S. Joint damage in rheumatoid arthritis progresses in remission according to the Disease Activity Score in 28 joints and is driven by residual swollen joints. Arthritis Rheum. 2011, 63, 3702–3711. [Google Scholar] [CrossRef]
- Hambardzumyan, K.; Bolce, R.; Saevarsdottir, S.; Cruickshank, S.E.; Sasso, E.H.; Chernoff, D.; Forslind, K.; Petersson, I.F.; Geborek, P.; van Vollenhoven, R.F. Pretreatment multi-biomarker disease activity score and radiographic progression in early RA: Results from the SWEFOT trial. Ann. Rheum. Dis. 2015, 74, 1102–1109. [Google Scholar] [CrossRef] [PubMed]
- Grillet, B.; Yu, K.; Ugarte-Berzal, E.; Janssens, R.; Pereira, R.V.S.; Boon, L.; Martens, E.; Berghmans, N.; Ronsse, I.; Van Aelst, I.; et al. Proteoform Analysis of Matrix Metalloproteinase-9/Gelatinase B and Discovery of Its Citrullination in Rheumatoid Arthritis Synovial Fluids. Front Immunol. 2021, 12, 763832. [Google Scholar] [CrossRef] [PubMed]
- Baggio, C.; Boscaro, C.; Oliviero, F.; Trevisi, L.; Ramaschi, G.; Ramonda, R.; Bolego, C.; Cignarella, A. Gender differences and pharmacological regulation of angiogenesis induced by synovial fluids in inflammatory arthritis. Biomed. Pharmacother. 2022, 152, 113181. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Doherty, M.; Peat, G.; Bierma-Zeinstra, M.A.; Arden, N.K.; Bresnihan, B.; Herrero-Beaumont, G.; Kirschner, S.; Leeb, B.F.; Lohmander, L.S.; et al. EULAR evidence-based recommendations for the diagnosis of knee osteoarthritis. Ann. Rheum. Dis. 2010, 69, 483–489. [Google Scholar] [CrossRef] [Green Version]
- Larsen, A. How to applay Larsen score in evaluating radiographs of rheumatoid arthritis in long-term studies. J. Rheumatol. 1995, 22, 1974–1975. [Google Scholar] [PubMed]
- Zeng, G.Q.; Chen, A.B.; Li, W.; Song, J.H.; Gao, C.Y. High MMP-1, MMP-2, and MMP-9 protein levels in osteoarthritis. Genet Mol Res. 2015, 23, 14811–14822. [Google Scholar] [CrossRef]
- Meehan, R.T.; Regan, E.A.; Hoffman, E.D.; Wolf, M.L.; Gill, M.T.; Crooks, J.L.; Parmar, P.J.; Scheuring, R.A.; Hill, J.C.; Pacheco, K.A.; et al. Synovial Fluid Cytokines, Chemokines and MMP Levels in Osteoarthritis Patients with Knee Pain Display a Profile Similar to Many Rheumatoid Arthritis Patients. J. Clin. Med. 2021, 10, 5027. [Google Scholar] [CrossRef]
- Yoshihara, Y.; Nakamura, H.; Obata, K.; Yamada, H.; Hayakawa, T.; Fujikawa, K.; Okada, Y. Matrix metalloproteinases and tissue inhibitors of metalloproteinases in synovial fluids from patients with rheumatoid arthritis or osteoarthritis. Ann. Rheum. Dis. 2000, 59, 455–461. [Google Scholar] [CrossRef]
- Ryu, J.H.; Lee, A.; Huh, M.S.; Chu, J.; Kim, K.; Kim, B.S.; Choi, K.; Kwon, I.C.; Park, J.W.; Youn, I. Measurement of MMP Activity in Synovial Fluid in Cases of Osteoarthritis and Acute Inflammatory Conditions of the Knee Joints Using a Fluorogenic Peptide Probe-Immobilized Diagnostic Kit. Theranostics 2012, 2, 198–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tchetverikov, I.; Ronday, H.K.; Van El, B.; Kiers, G.H.; Verzijl, N.; TeKoppele, J.M.; Huizinga, T.W.; DeGroot, J.; Hanemaaijer, R. MMP profile in paired serum and synovial fluid samples of patients with rheumatoid arthritis. Ann. Rheum. Dis. 2004, 63, 881–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tchetverikov, I.; Lard, L.R.; De Groot, J.; Verzijl, N.; TeKoppele, J.M.; Breedveld, F.C.; Huizinga, T.W.; Hanemaaijer, R. Matrix metalloproteinases-3, -8, -9 as markers of disease activity and joint damage progression in early rheumatoid arthritis. Ann. Rheum. Dis. 2003, 62, 1094–1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuncer, T.; Arzu Kaya, A.; Gulkesen, A.; Ayden Kal, G.; Kaman, D.; Akgol, G. Matrix metalloproteinase-3 levels in relation to disease activity and radiological progression in rheumatoid arthritis. Adv. Clin. Exp. Med. 2019, 28, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, H.; Matsuda, Y.; Tanaka, M.; Sendo, W.; Nakajima, H.; Taniguchi, A.; Kamatani, N. Serum matrix metalloproteinase 3 as a predictor of the degree of joint destruction during the six months after measurement, in patients with early rheumatoid arthritis. Arthritis Rheum. 2000, 4, 852–888. [Google Scholar] [CrossRef]
- Stojanovic, S.; Stamenkovic, B.; Stoimenov, T.; Nedovic, J.; Zivkovic, V.; Despotovic, M.; Pavlovic, D. Association of tumor necrosis factor-α (G-308A) genetic variant with matrix metalloproteinase-9 activity and joint destruction in early rheumatoid arthritis. Clin. Rheumatol. 2017, 36, 1479–1485. [Google Scholar] [CrossRef] [PubMed]
- Mouterde, G.; Lukas, C.; Logeart, I.; Flipo, R.M.; Rincheval, R.; Daures, J.P.; Combe, B. Predictors of radiographic progression in the ESPOIR cohort: The season of first symptoms may influence the short-term outcome in early rheumatoid artrhitis. Ann. Rheuamtic Dis. 2011, 70, 1251–1256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stojanovic, S. Predictors of Prognosis of Rheumatoid Arthritis. Master’s Thesis, Medical Faculty, University of Nis, Nis, Serbia, 2005. [Google Scholar]
- Végh, E.; Gaál, J.; Géher, P.; Gömöri, E.; Kovács, A.; Kovács, L.; Nagy, K.; Posta, E.F.; Tamási, L.; Tóth, E.; et al. Assessing the risk of rapid radiographic progression in Hungarian rheumatoid arthritis patients. BMC Musculoskelet. Disord. 2021, 22, 325. [Google Scholar] [CrossRef]
- Versteeg, G.A.; Steunebrink, L.; Vonkeman, H.E.; Ten Klooster, P.M.; Van Der Bijl, A.E.; Van De Laar, M. Early radiological progression remains associated with long-term joint damage in real-world rheumatoid arthritis patients treated to the target of remission. Scand. J. Rheumatol. 2022, 51, 87–96. [Google Scholar] [CrossRef]
- Steunebrink, L.M.; Vonkeman, H.E.; ten Klooster, P.M.; Hoekstra, M.; van Riel, P.L.; van de Laar, M.A. Recently diagnosed rheumatoid arthritis patients benefit from a treat-to-target strategy: Results from the DREAM registry. Clin. Rheumatol. 2016, 35, 609–615. [Google Scholar] [CrossRef]
- de Rooy, D.P.; Zhernakova, A.; Tsonaka, R.; Willemze, A.; Kurreeman, B.A.; Trynka, G.; van Toorn, L.; Toes, R.E.; Huizinga, T.W.; Houwing-Duistermaat, J.J.; et al. A genetic variant in the region of MMP-9 is associated with serum levels and progression of joint damage in rheumatoid arthritis. Ann. Rheum. Dis. 2014, 73, 1163–1169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpenter, L.; Norton, S.; Nikiphorou, E.; Jayakumar, K.; McWilliams, D.F.; Rennie, K.L.; Dixey, J.; Kiely, P.; Walsh, D.A.; Young, A. Early Rheumatoid Arthritis Study and the Early Rheumatoid Arthritis Network. Reductions in Radiographic Progression in Early Rheumatoid Arthritis Over Twenty-Five Years: Changing Contribution From Rheumatoid Factor in Two Multicenter UK Inception Cohorts. Arthritis Care Res. 2017, 69, 1809–1817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honda, S.; Ikari, K.; Yano, K.; Terao, C.; Tanaka, E.; Harigai, M.; Kochi, Y. Association of Polygenic Risk Scores With Radiographic Progression in Patients With Rheumatoid Arthritis. Arthritis Rheumarism. 2022, 74, 791–800. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group | Mean ± SD (ng/mL) | 95% CI | Median | CV | |
|---|---|---|---|---|---|
| Plasma | RA (n = 84) | 19.26 ± 7.54 ** | 17.5–20.5 | 19.76 | 41.56 |
| Controls (n = 72) | 14.57 ± 3.11 | 13.3–14.7 | 14.57 | 21.57 | |
| Synovial fluid | RA (n = 84) | 16.17 ± 12.25 *** | 13.4–18.6 | 14.21 | 84.82 |
| Controls (n = 72) | 0.75 ± 0.53 | 0.74–0.76 | 0.82 | 62.68 |
| MMP-9 Level | Erosive RA (n = 48) | Non-Erosive RA (n = 36) |
|---|---|---|
| Plasma (ng/mL) (mean ± SD) | 21.37 ± 10.50 | 18.62 ± 6.37 |
| Synovial fluid (ng/mL)(mean ± SD) | 18.43 ± 12.87 * | 9.36 ± 7.72 |
| Factor | OR | 95% CI | p |
|---|---|---|---|
| Age | 1.11 | 1.02–1.22 | 0.019 |
| RA duration | 1.16 | 1.01–1.32 | 0.030 |
| MMP-9 level in plasma | 0.95 | 0.85–1.06 | 0.330 |
| MMP-9 level in synovial fluid | 2.80 | 1.24–6.30 | 0.012 |
| Larsen Score | Erosive RA (n = 48) | Non-Erosive RA (n = 36) |
|---|---|---|
| Before MTX therapy (mean ± SD) | 48.58 ± 20.84 | 18.78 ± 12.91 * |
| After 12 months of MTX therapy (mean ± SD) | 65.32 ± 22.24 | 26.48 ± 13.27 *** |
| ∆LS (mean ± SD) | 11.14 ± 4.75 | 6.13 ± 2.72 ** |
| Parameter | RF | ACPA |
|---|---|---|
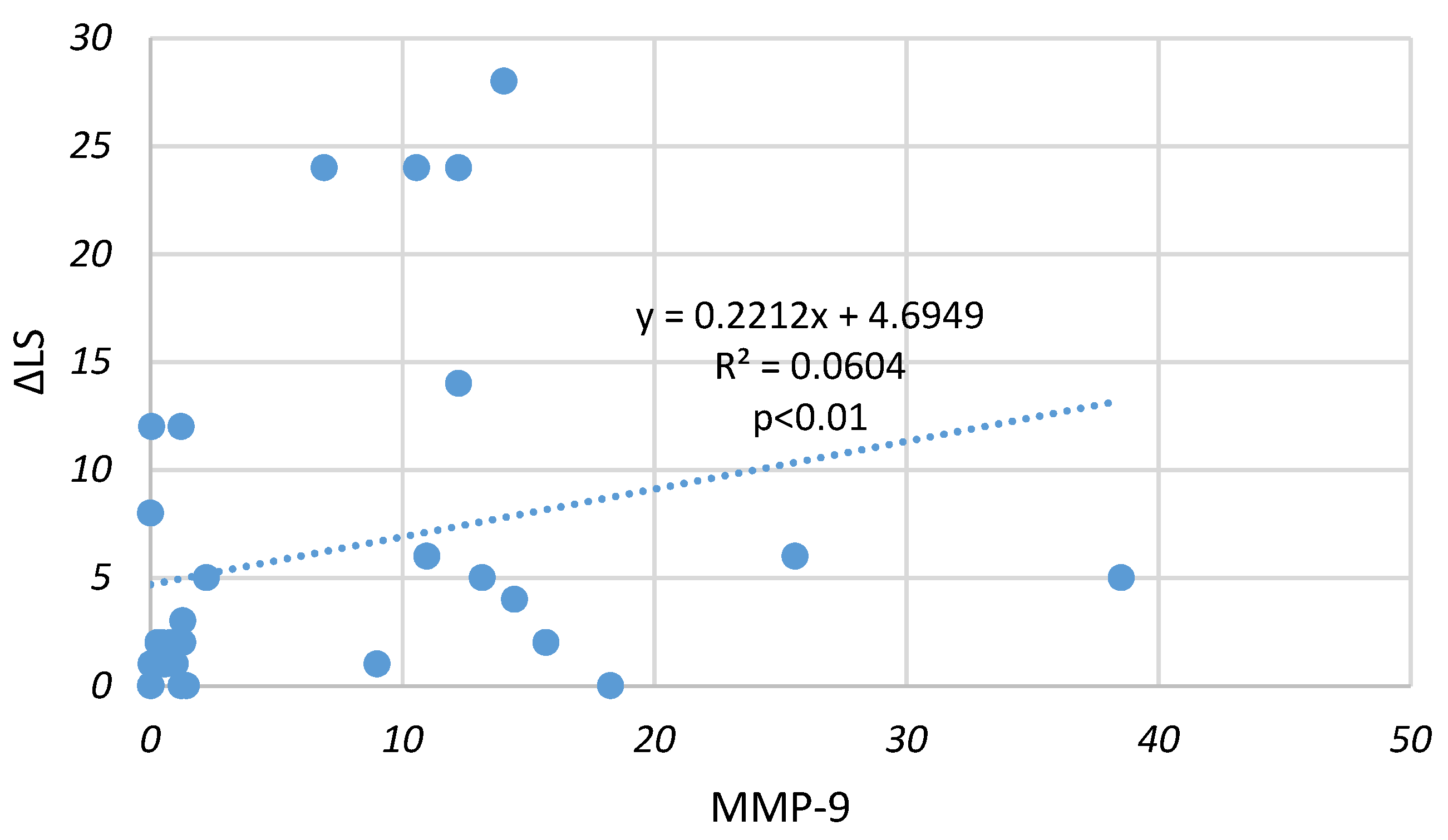
| MMP-9 level in plasma (ng/mL) | −0.20 | 0.18 |
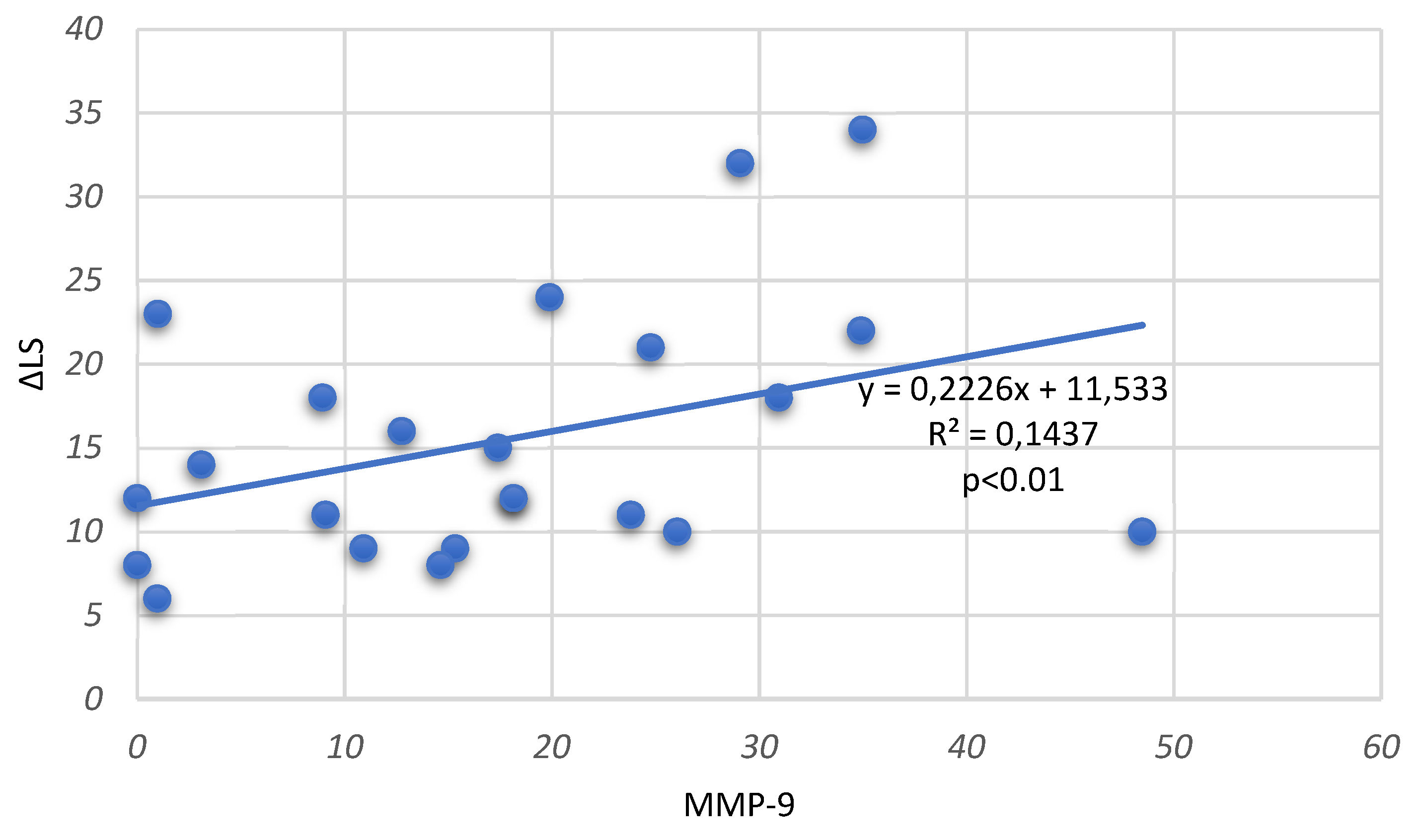
| MMP-9 level in synovial fluid (ng/mL) | −0.06 | 0.48 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stojanovic, S.K.; Stamenkovic, B.N.; Cvetkovic, J.M.; Zivkovic, V.G.; Apostolovic, M.R.A. Matrix Metalloproteinase-9 Level in Synovial Fluid—Association with Joint Destruction in Early Rheumatoid Arthritis. Medicina 2023, 59, 167. https://doi.org/10.3390/medicina59010167
Stojanovic SK, Stamenkovic BN, Cvetkovic JM, Zivkovic VG, Apostolovic MRA. Matrix Metalloproteinase-9 Level in Synovial Fluid—Association with Joint Destruction in Early Rheumatoid Arthritis. Medicina. 2023; 59(1):167. https://doi.org/10.3390/medicina59010167
Chicago/Turabian StyleStojanovic, Sonja K., Bojana N. Stamenkovic, Jovana M. Cvetkovic, Valentina G. Zivkovic, and Marija R. Andjelkovic Apostolovic. 2023. "Matrix Metalloproteinase-9 Level in Synovial Fluid—Association with Joint Destruction in Early Rheumatoid Arthritis" Medicina 59, no. 1: 167. https://doi.org/10.3390/medicina59010167