
Risk Factors for Anticancer Drug-Induced Hyponatremia: An Analysis Using the Japanese Adverse Drug Report (JADER) Database
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Definitions of Side Effects and Medication
2.3. Analysis of the ROR
2.4. Analysis of Onset of Adverse Events
3. Results
3.1. Crude RORs and the Number of Cases of Each Anticancer Drug Associated with Hyponatremia
3.2. Crude RORs and the Number of Cases of Each Cancer Site Associated with Hyponatremia
3.3. Analysis of Adjusted ROR for the Patient Character with Hyponatremia
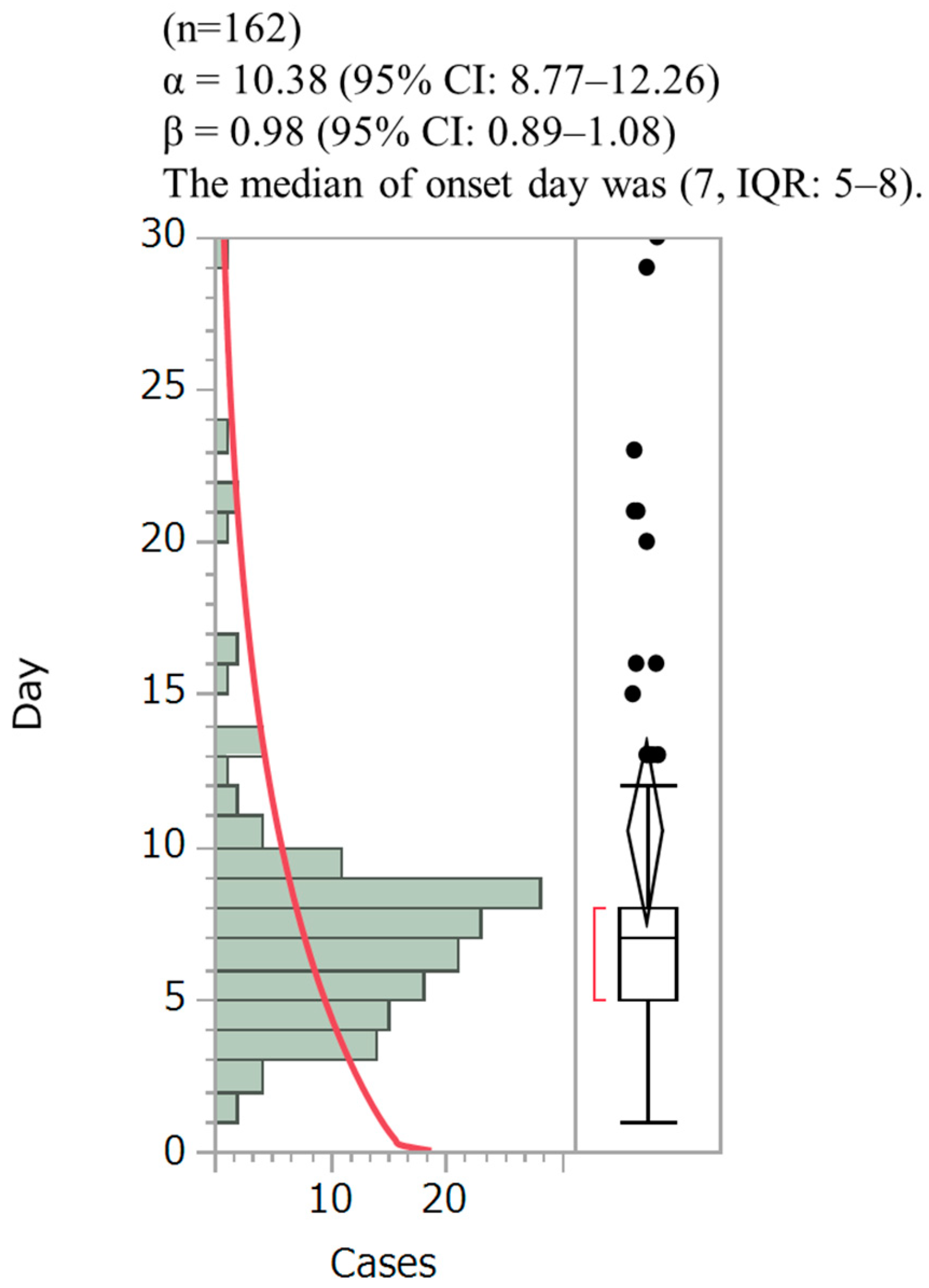
3.4. The Onset of Hyponatremia in Patients Treated with Cisplatin
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Doshi, S.M.; Sha, P.; Lei, X.; Lahoti, A.; Salahudeen, A.K. Hyponatremia in hospitalized cancer patients and its impact on clinical outcomes. Am. J. Kidney Dis. 2012, 59, 222–228. [Google Scholar] [CrossRef]
- Spasovski, G.; Vanholder, R.; Allolio, B.; Annane, D.; Ball, S.; Bichet, D.; Decaux, G.; Fenske, W.; Hoorn, E.J.; Ichai, C.; et al. Hyponatraemia Guideline Development Group. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Eur. J. Endocrinol. 2014, 170, G1–G47. [Google Scholar] [CrossRef] [Green Version]
- David, R.B.; Theodore, W. Post Clinical Physiology of Acid-Base and Electrolyte Disorders; McGraw-Hill: New York, NY, USA, 2001. [Google Scholar]
- Rondon-Berrios, H.; Agaba, E.I.; Tzamaloukas, A.H. Hyponatremia: Pathophysiology, classification, manifestations and management. Int. Urol. Nephrol. 2014, 46, 2153–2165. [Google Scholar] [CrossRef]
- Burst, V. Etiology and Epidemiology of Hyponatremia. Front. Horm. Res. 2019, 52, 24–35. [Google Scholar] [CrossRef]
- Davila, C.D.; Udelson, J.E. Hypervolemic hyponatremia in heart failure. Front. Horm. Res. 2019, 52, 113–129. [Google Scholar] [CrossRef]
- Solà, E.; Ginès, P. Hypervolemic hyponatremia (liver). Front. Horm. Res. 2019, 52, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Berghmans, T. Hyponatremia related to medical anticancer treatment. Support. Care Cancer 1996, 4, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Abu Zeinah, G.F.; Al-Kindi, S.G.; Hassan, A.A.; Allam, A. Hyponatraemia in cancer: Association with type of cancer and mortality. Eur. J. Cancer Care 2015, 24, 224–231. [Google Scholar] [CrossRef]
- Berghmans, T.; Paesmans, M.; Body, J.J. A prospective study on hyponatraemia in medical cancer patients: Epidemiology, aetiology and differential diagnosis. Support. Care Cancer 2000, 8, 192–197. [Google Scholar] [CrossRef]
- Berardi, R.; Rinaldi, S.; Caramanti, M.; Grohè, C.; Santoni, M.; Morgese, F.; Torniai, M.; Savini, A.; Fiordoliva, I.; Cascinu, S. Hyponatremia in cancer patients: Time for a new approach. Crit. Rev. Oncol. Hematol. 2016, 102, 15–25. [Google Scholar] [CrossRef]
- Ishida, T.; Kawada, K.; Jobu, K.; Kawazoe, T.; Tamura, N.; Miyamura, M. Analysis of drug-induced liver injury from bofutsushosan administration using Japanese Adverse Drug Event Report (JADER) Database. Biol. Pharm. Bull. 2022, 45, 460–466. [Google Scholar] [CrossRef]
- Hiromi, K.; Jun, S.; Masanori, A.; Yasuo, T. Drug-induced hyperglycemia in the Japanese Adverse Drug Event Report database: Association of evelolimus use with diabetes. Endocr. J. 2019, 66, 571–574. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, Y.; Suzuki, H.; Umetsu, R.; Uranishi, H.; Abe, J.; Nishibata, Y.; Sekiya, Y.; Miyamura, N.; Hara, H.; Tsuchiya, T.; et al. analysis of the interaction between clopidogrel, aspirin and proton pump inhibitors using the FDA Adverse Event Reporting System database. Biol. Pharm. Bull. 2015, 38, 680–686. [Google Scholar] [CrossRef] [Green Version]
- Shimada, K.; Hasegawa, S.; Nakao, S.; Mukai, R.; Sasaoka, S.; Ueda, N.; Kato, Y.; Abe, J.; Mori, T.; Yoshimura, T.; et al. Adverse reaction profiles of hemorrhagic adverse reactions caused by direct oral anticoagulants analyzed using the Food and Drug Administration Adverse Event Reporting System (FAERS) database and the Japanese Adverse Drug Event Report (JADER) database. Int. J. Med. Sci. 2019, 16, 1295–1303. [Google Scholar] [CrossRef] [Green Version]
- Sauzet, O.; Carvajal, A.; Escudero, A.; Molokhia, M.; Cornelius, V.R. Illustration of the weibull shape parameter signal detection tool using electronic healthcare record data. Drug Saf. 2013, 36, 995–1006. [Google Scholar] [CrossRef] [PubMed]
- Ellison, D.H.; Berl, T. Clinical practice. The syndrome of inappropriate antidiuresis. N. Engl. J. Med. 2007, 356, 2064–2072. [Google Scholar] [CrossRef] [PubMed]
- Iyer, A.V.; Krasnow, S.H.; Dufour, D.R.; Arcenas, A.S. Sodium-wasting nephropathy caused by cisplatin in a patient with small-cell lung cancer. Clin. Lung Cancer 2003, 5, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Jorge, J.C.; Marc, V.; Eric, J. Diagnosis and management of hyponatremia in cancer patients. Oncologist 2012, 17, 756–765. [Google Scholar] [CrossRef] [Green Version]
- Christopher, R.; Lucy, M.; William, R.J.; Raj, S. Cisplatin-induced acute kidney injury and renal salt wasting syndrome. Fed. Pract. 2021, 38, 606–611. [Google Scholar] [CrossRef]
- Cunningham, D.; Starling, N.; Rao, S.; Iveson, T.; Nicolson, M.; Coxon, F.; Middleton, G.; Daniel, F.; Oates, J.; Norman, A.R. Upper Gastrointestinal Clinical Studies Group of the National Cancer Research Institute of the United Kingdom. Capecitabine and oxaliplatin for advanced esophagogastric cancer. N. Engl. J. Med. 2008, 358, 36–46. [Google Scholar] [CrossRef]
- Schutz, F.A.; Xie, W.; Donskov, F.; Sircar, M.; McDermott, D.F.; Rini, B.I.; Agarwal, N.; Pal, S.K.; Srinivas, S.; Kollmannsberger, C.; et al. The impact of low serum sodium on treatment outcome of targeted therapy in metastatic renal cell carcinoma: Results from the International Metastatic Renal Cell Cancer Database Consortium. Eur. Urol. 2014, 65, 723–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Kidney Cancer (Version 1.2021). 2019. Available online: https://www.nccn.org/ (accessed on 15 May 2020).
- Ezoe, Y.; Mizusawa, J.; Katayama, H.; Kataoka, K.; Muto, M. An integrated analysis of hyponatremia in cancer patients receiving platinum-based or nonplatinum-based chemotherapy in clinical trials (JCOG1405-A). Oncotarget 2017, 9, 6595–6606. [Google Scholar] [CrossRef] [Green Version]
- Hesketh, P.J.; Kris, M.G.; Grunberg, S.M.; Beck, T.; Hainsworth, J.D.; Harker, G.; Aapro, M.S.; Gandara, D.; Lindley, C.M. Proposal for classifying the acute emetogenicity of cancer chemotherapy. J. Clin. Oncol. 1997, 15, 103–109. [Google Scholar] [CrossRef]
- American Society of Clinical Oncology practice guideline update. J. Clin. Oncol. 2017, 35, 3240–3261. [CrossRef] [PubMed] [Green Version]
- NCCN Clinical Practice Guidelines in Oncology Version 1. Antiemesis National Comprehensive Cancer Network. 2018. Available online: https://www.nccn.org/guidelines/category_1 (accessed on 15 May 2020).
- Edwards, C.M.; Carmichael, J.; Baylis, P.H.; Harris, A. Arginine vasopressin—A mediator of chemotherapy induced emesis? Br. J. Cancer 1989, 59, 467–470. [Google Scholar] [CrossRef] [Green Version]
- Kugler, J.P.; Hustead, T. Hyponatremia and hypernatremia in the elderly. Am. Fam. Physician 2000, 61, 3623–3630. [Google Scholar] [PubMed]
- Hotta, T. Present status and future perspectives of cancer practice in elderly. Health Eval. Promot. 2017, 44, 341–348. [Google Scholar] [CrossRef] [Green Version]
- Kurtzberg, J.; Dennis, V.W.; Kinney, T.R. Cisplatinum-induced renal salt wasting. Med. Pediatr. Oncol. 1984, 12, 150–154. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Drugs | Total (n) | Case (n) | Non-Case (n) | Ratio (%) | Crude ROR (95% CI) | p-Values |
|---|---|---|---|---|---|---|
| Total | 595,121 | 2943 | 592,178 | 0.49 | ||
| Cisplatin | 11,468 | 221 | 11,247 | 1.93 | 4.19 (3.64–4.82) | <0.001 |
| Pemetrexed | 3471 | 48 | 3423 | 1.38 | 2.85 (2.09–3.80) | <0.001 |
| Etoposide | 5307 | 45 | 5262 | 0.85 | 1.73 (1.27–2.32) | <0.001 |
| Carboplatin | 9266 | 56 | 9210 | 0.60 | 1.22 (0.92–1.60) | 0.14 |
| Vincristine | 6179 | 34 | 6145 | 0.55 | 1.11 (0.77–1.56) | 0.52 |
| Pembrolizumab | 5505 | 30 | 5475 | 0.54 | 1.10 (0.74–1.58) | 0.56 |
| Nivolumab | 9307 | 49 | 9258 | 0.53 | 1.07 (0.79–1.41) | 0.65 |
| Cyclophosphamide | 10,889 | 54 | 10,835 | 0.50 | 1.00 (0.75–1.31) | 0.95 |
| Docetaxel | 7848 | 39 | 7809 | 0.50 | 1.00 (0.71–1.37) | 0.94 |
| Paclitaxel | 11,161 | 54 | 11,107 | 0.48 | 0.98 (0.73–1.28) | 0.95 |
| Doxorubicin | 6555 | 31 | 6524 | 0.47 | 0.96 (0.65–1.36) | 0.92 |
| Irinotecan | 8695 | 41 | 8654 | 0.47 | 0.95 (0.68–1.30) | 0.82 |
| Gemcitabine | 5338 | 21 | 5317 | 0.39 | 0.79 (0.49–1.22) | 0.33 |
| Oxaliplatin | 11,973 | 27 | 11,946 | 0.23 | 0.45 (0.30–0.66) | <0.001 |
| Cancer Site | Total (n) | Case (n) | Non-Case (n) | Ratio (%) | Crude ROR (95% CI) | p-Values |
|---|---|---|---|---|---|---|
| Total | 595,121 | 2,943 | 592,178 | 0.49 | ||
| Esophageal | 1607 | 17 | 1590 | 1.06 | 2.20 (1.25–3.47) | 0.032 |
| Lung | 15,256 | 138 | 15,118 | 0.90 | 1.80 (1.70–2.40) | <0.001 |
| Renal | 7706 | 58 | 7648 | 0.75 | 1.50 (1.16–1.99) | 0.002 |
| Stomach | 8202 | 52 | 8150 | 0.63 | 1.30 (0.96–1.70) | 0.080 |
| Prostate | 7944 | 41 | 7903 | 0.52 | 1.00 (0.75–1.42) | 0.75 |
| Colorectal | 15,913 | 50 | 15,863 | 0.31 | 0.63 (0.46–0.83) | <0.001 |
| Breast | 12,604 | 18 | 12,586 | 0.14 | 0.30 (0.17–0.45) | <0.001 |
| Total (n) | Case (n) | p-Values | Adjusted ROR (95% CI) | p-Values | |
|---|---|---|---|---|---|
| Total | 595,121 | 2943 | |||
| Reporting year | — | — | — | 0.99 (0.99–1.00) | 0.061 |
| Sex, Female | 289,118 | 1574 | <0.001 | 1.33 (1.24–1.44) | <0.001 |
| Age | |||||
| ≥60 years | 378,055 | 2430 | <0.001 | 2.73 (2.48–3.00) | <0.001 |
| Cancer site | |||||
| Renal | 7706 | 58 | 0.002 | 1.57 (1.23–2.01) | <0.001 |
| Lung | 15,256 | 138 | <0.001 | 1.49 (1.25–1.78) | <0.001 |
| Esophageal | 1607 | 17 | 0.003 | 1.06 (0.65–1.74) | 0.17 |
| Drugs | |||||
| Cisplatin | 11,468 | 221 | <0.001 | 4.05 (3.47–4.73) | <0.001 |
| Etoposide | 5307 | 45 | <0.001 | 1.23 (0.85–1.58) | 0.19 |
| Pemetrexed | 3471 | 48 | <0.001 | 1.16 (0.85–1.58) | 0.36 |
| Interaction | |||||
| Cisplatin and Lung | — | — | — | 1.50 (1.00–2.26) | 0.051 |
| Cisplatin and Renal | — | — | — | 1.18 (0.16–8.84) | 0.87 |
| Cisplatin and Female | — | — | — | 0.98 (0.74–1.31) | 0.91 |
| Cisplatin and ≥age 60 | — | — | — | 0.71 (0.50–1.00) | 0.053 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamura, N.; Ishida, T.; Kawada, K.; Jobu, K.; Morisawa, S.; Yoshioka, S.; Miyamura, M. Risk Factors for Anticancer Drug-Induced Hyponatremia: An Analysis Using the Japanese Adverse Drug Report (JADER) Database. Medicina 2023, 59, 166. https://doi.org/10.3390/medicina59010166
Tamura N, Ishida T, Kawada K, Jobu K, Morisawa S, Yoshioka S, Miyamura M. Risk Factors for Anticancer Drug-Induced Hyponatremia: An Analysis Using the Japanese Adverse Drug Report (JADER) Database. Medicina. 2023; 59(1):166. https://doi.org/10.3390/medicina59010166
Chicago/Turabian StyleTamura, Naohisa, Tomoaki Ishida, Kei Kawada, Kohei Jobu, Shumpei Morisawa, Saburo Yoshioka, and Mitsuhiko Miyamura. 2023. "Risk Factors for Anticancer Drug-Induced Hyponatremia: An Analysis Using the Japanese Adverse Drug Report (JADER) Database" Medicina 59, no. 1: 166. https://doi.org/10.3390/medicina59010166