
A Surgical Challenge Generated by Colonic Malakoplakia in Disguise as a Locally Advanced Colonic Malignancy—A Case Report

Abstract
:1. Introduction
2. Case Report
- left liver lobe = 58 mm,
- right lobe of the liver = 144 mm, with slightly increased echogenicity and microgranular structure,
- PV (portal vein) = 12 mm,
- CBP (main biliary duct) = 5 mm,
- non-dilated CBIH (intrahepatic biliary duct),
- folded gallbladder in lower 1/3, with micro calculus of 5–6 mm,
- homogeneous pancreas,
- homogeneous spleen with 81 mm long axis,
- RK (right kidney) of normal size, IP retained, calculi of 5–6 mm, no pyelocaliceal dilations,
- LK (left kidney) of normal size, IP retained, calculi of 5–6 mm, no pyelocaliceal dilations,
- the urinary bladder half-full, without changes,
- marked aerocolia on the colic frame, without free intraperitoneal fluid.
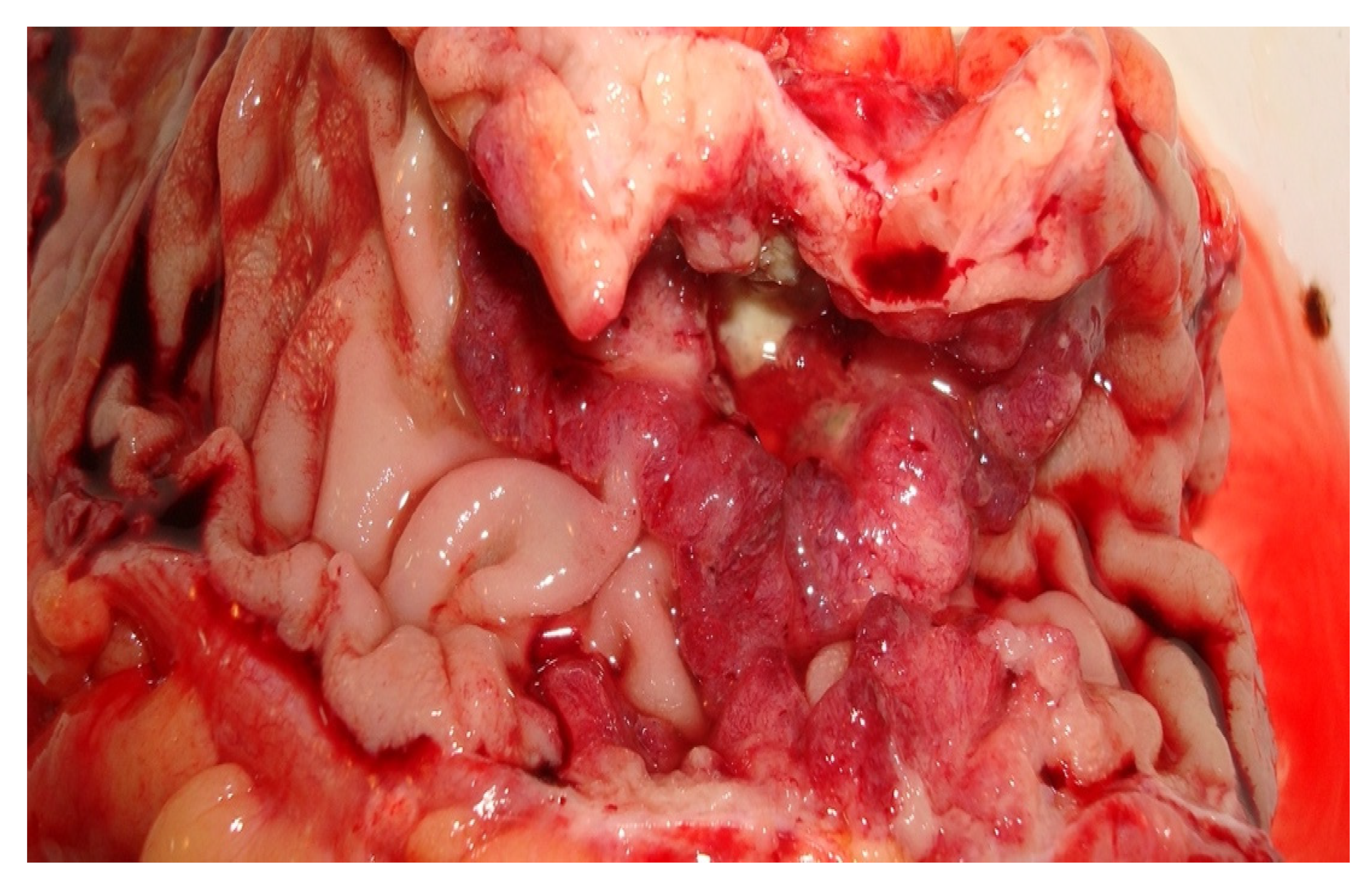
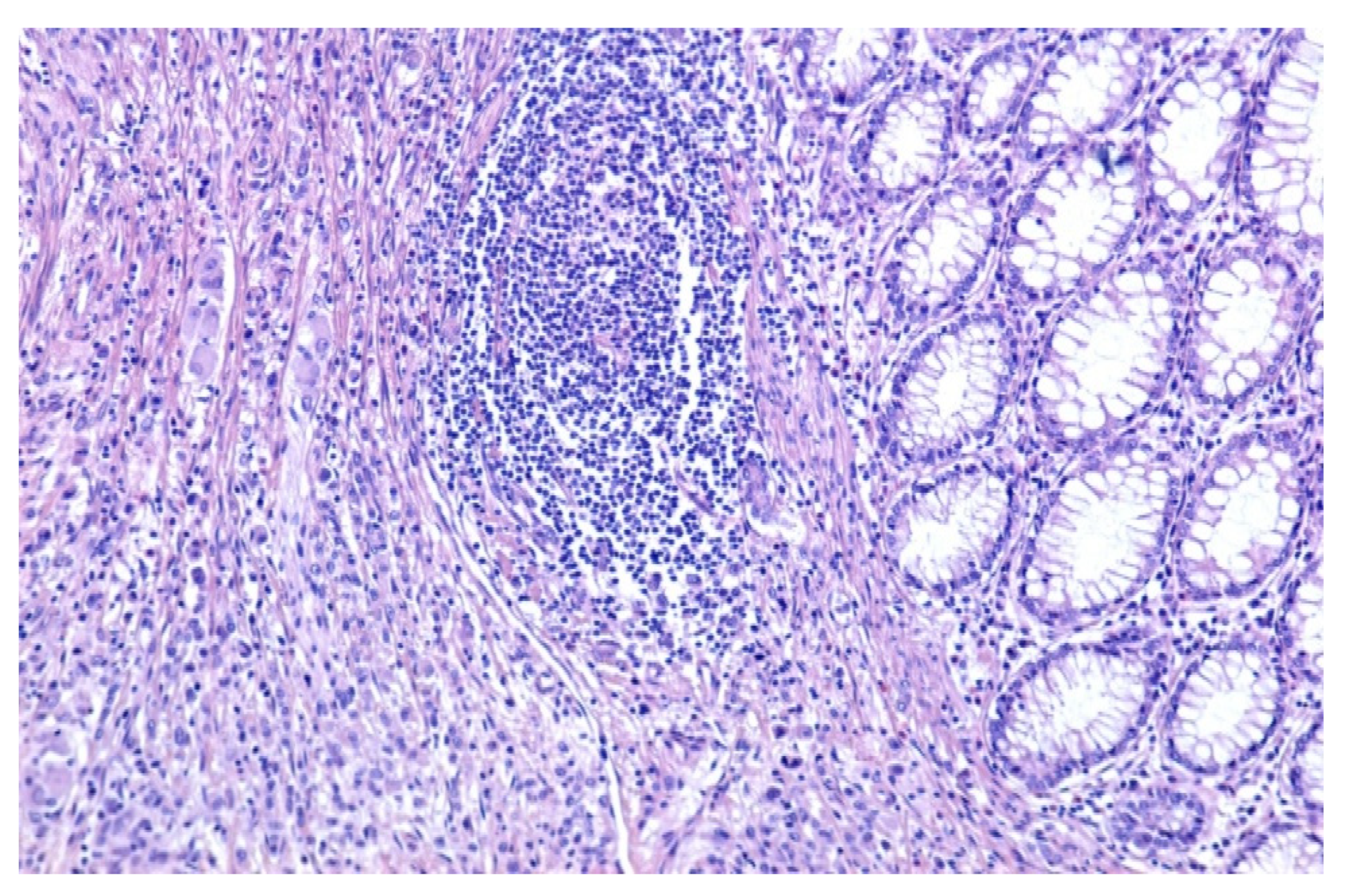
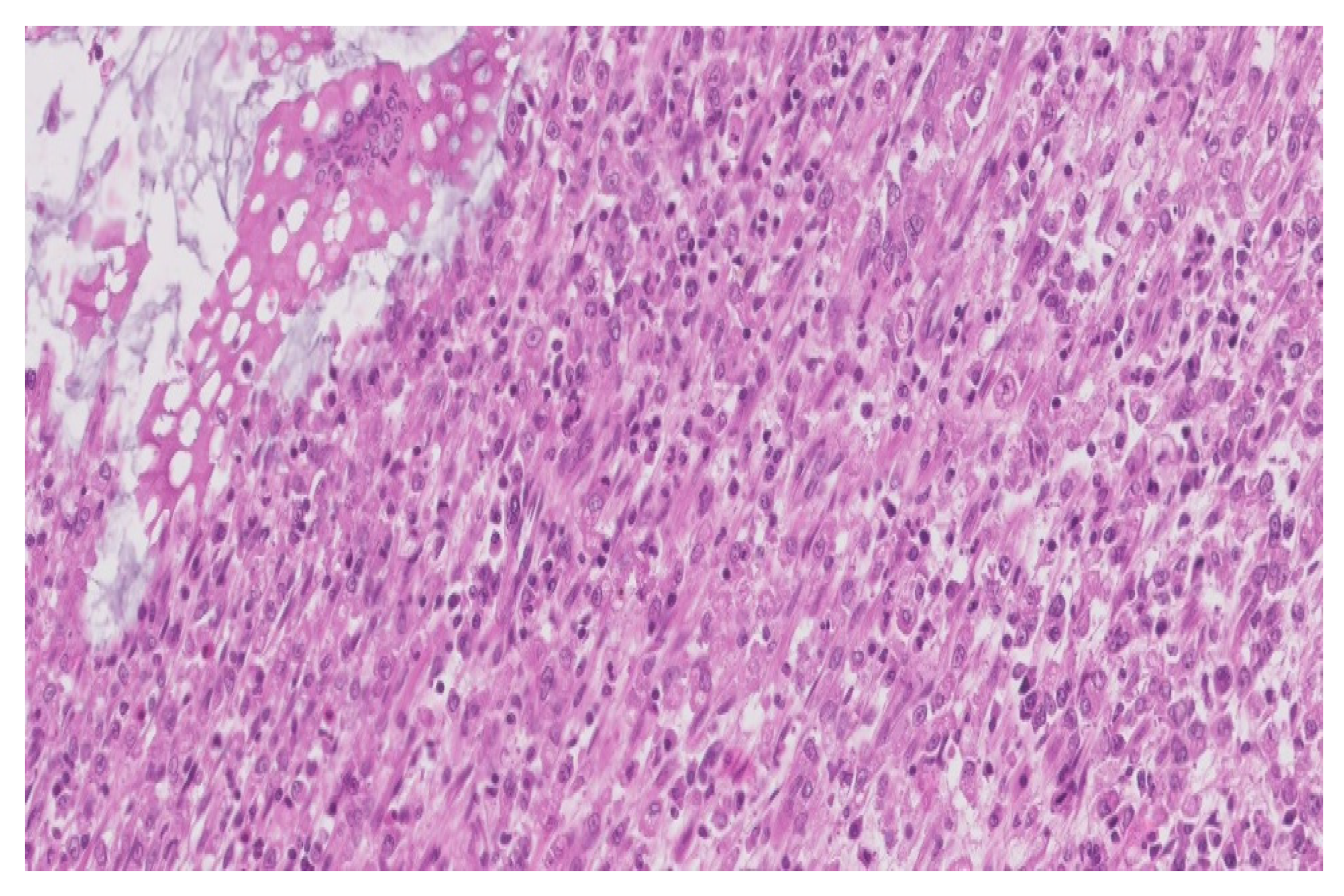
3. Pathologic Findings
- a significant architectural remodeling of the colonic mucosa and submucosa with dense cellular inflammatory infiltrate,
- the dense cellular inflammatory infiltrate-composed of epithelioid macrophages with wide eosinophilic cytoplasm, variable-sized nuclei, with occasional nucleoli,
- dispersed syncytia with the appearance of multinucleated giant cells, with chaotically disposed nuclei and
- amorphous cytoplasmatic inclusions of cellular detritus type, with sporadic intercalated lymphocytes.
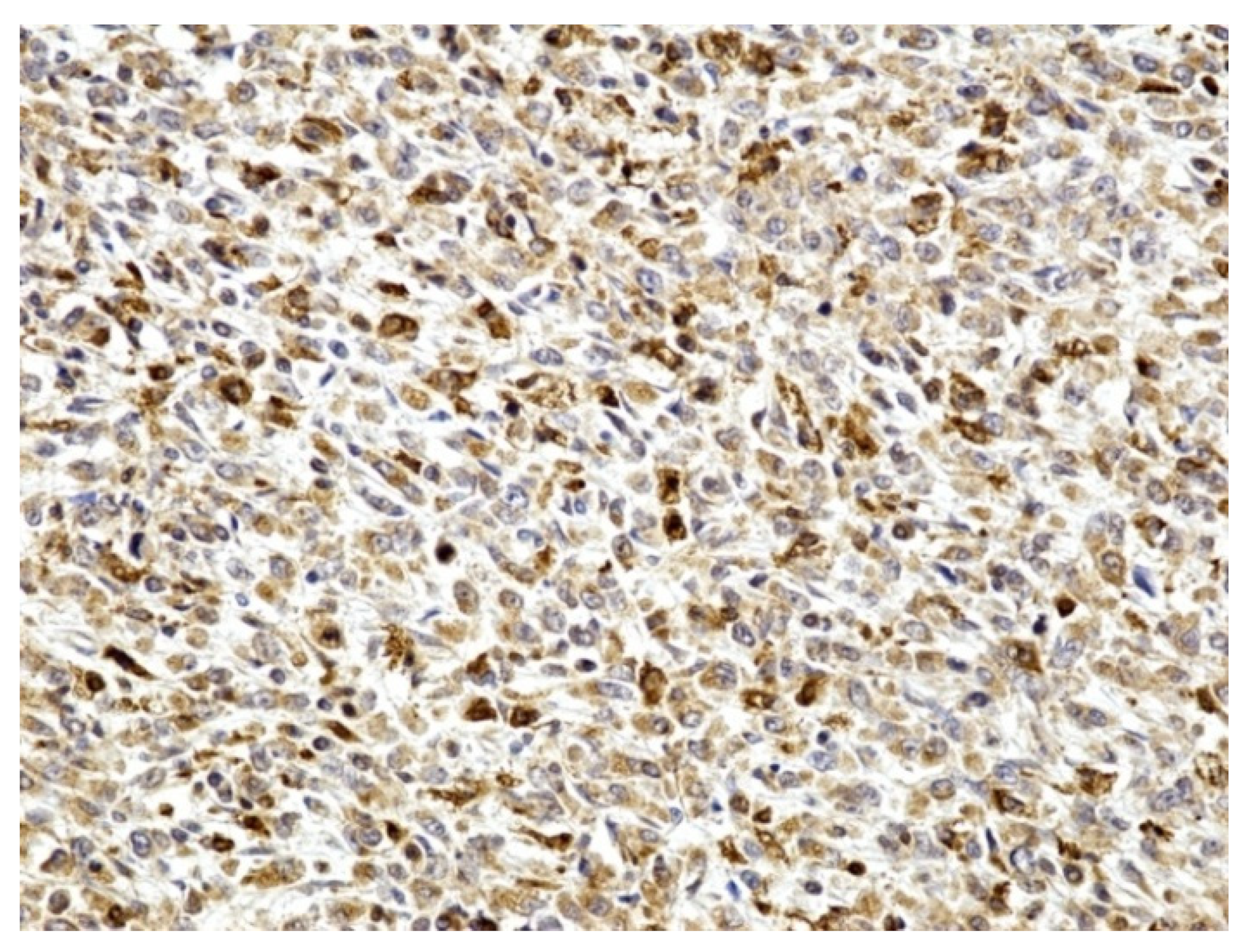
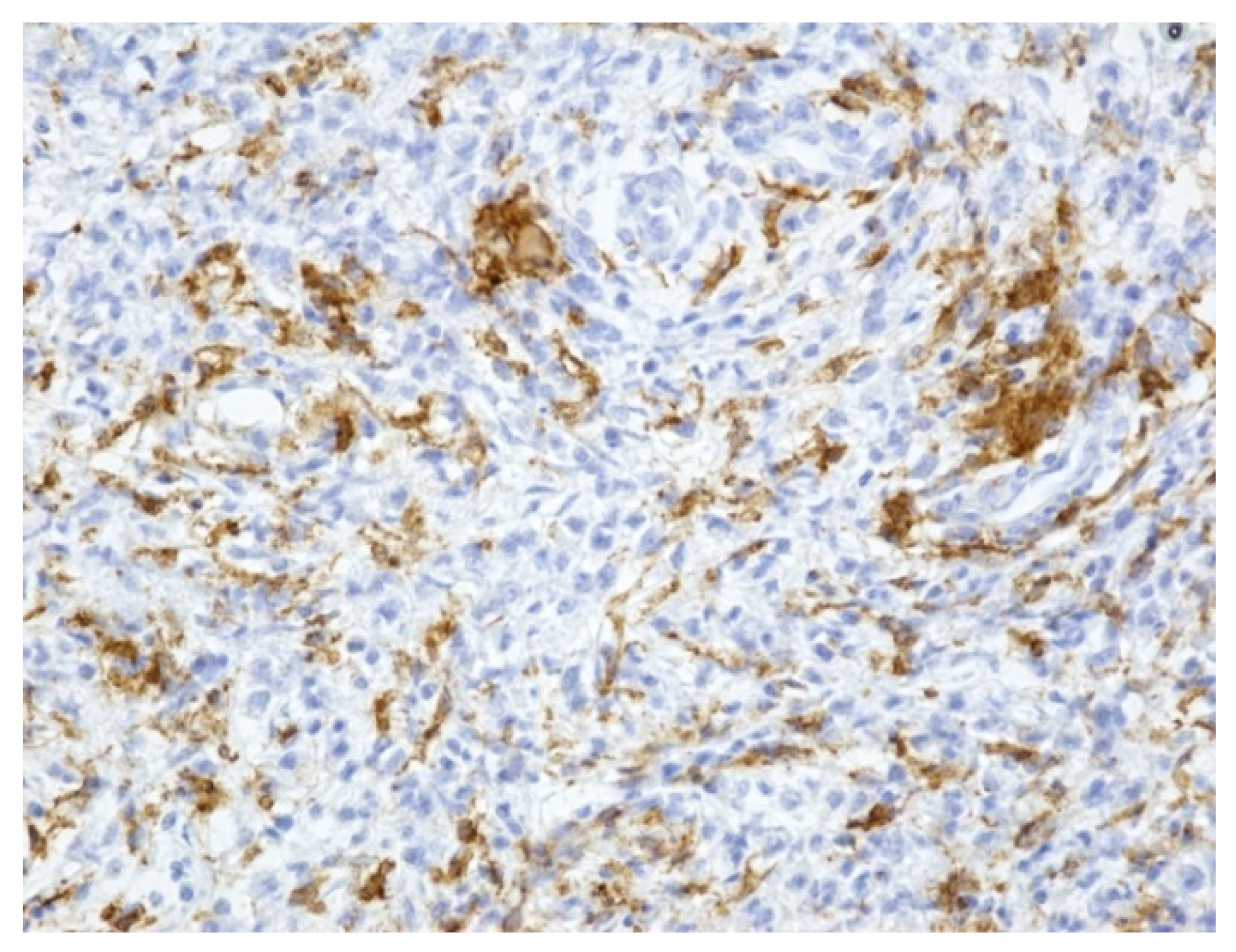
- macrophages (positive CD68)-illustrated in the Figure 4
- with rare dispersed T lymphocytes (positive CD3),
- rare B lymphocytes (alpha positive CD20, CD79) especially in the lamina propria,
- rare plasmacytes (alpha positive CD79),
- as well as rare mast cells (positive tryptase).

4. Discussions
- rectal bleeding,
- diarrhea,
- abdominal pain in different grades,
- fever,
- weight loss in the recent period before presenting to the hospital,
- night sweats and
- intestinal tract obstruction.
- Sessile or polypoid masses isolated in the rectosigmoid colon; the lumen may be narrowed which may suggest malignant stenosis. The inflammatory process may be transmural, similar to the Crohn’s disease.
- Diffuse involvement of the entire colon either with serpiginous polypoid lesions or with diffuse ulcerations; variant often identified in patients with compromised immunity, including the patients with renal transplant, immunosuppressive drug therapy and hereditary immunodeficiency.
- malignant tumors,
- miliary tuberculosis and
- Crohn’s disease.
- Microscopically, the malakoplakia may be similar to:
- the Whipple disease,
- ceroid-like colonic histiocytosis,
- Wolman disease,
- Chediak-Higashi syndrome,
- sarcoidosis, or
- other granulomatous diseases [12].
- antibiotic therapy using agents that interact directly with the macrophages, like the quinolones or trimethoprim-sulfamethoxazole
- diminution or even suspension of the doses prescribed for the immunosuppressive therapy
- a good control of the associated immunosuppressive pathology
- endoscopic resections for the cases with localized lesions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Michaelis, L.; Gutmann, C. Ueber Einschlusse in Blasentumoren. Z. Klin. Med. 1992, 47, 208–215. [Google Scholar]
- Sagaert, X.; Tousseyn, T.; De Hertogh, G.; Geboes, K. Macrophage-related diseases of the gut: A pathologist’s perspective. Virchows Arch. 2012, 460, 555–567. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Byrnes, K.; Lam-Himlin, D.; Pittman, M.; Pezhouh, M.; Gonzalez, R.S.; Alruwaii, Z.; Larman, T.; Miller, J.A.; Matoso, A.; et al. Gastrointestinal Malakoplakia. Am. J. Surg. Pathol. 2020, 44, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Stanton, J.; Maxted, W. Malacoplakia: A study of the literature and current concepts of pathogenesis, diagnosis and treatment. J. Urol. 1981, 125, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Flint, A.; Murad, T.M. Malakoplakia and malakoplakia like lesions of the upper gastrointestinal tract. Ultrastruct. Pathol. 1984, 7, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Matter, M.J.; Gygi, C.; Gillet, M.; Bouzourene, H. Malacoplakia simulating organ invasion in a rectosigmoid adenocarcinoma: Report of a case. Dis. Colon. Rectum. 2001, 44, 1371–1375. [Google Scholar] [CrossRef]
- Park, J.W.; Baek, D.H.; Lee, S.J. Multiple polypoid lesions in the sigmoid colon. Gastroenterology 2020, 158, 482–484. [Google Scholar] [CrossRef] [Green Version]
- Nyhan, W.L.; Barshop, B.; Ozand, P. Atlas of Metabolic Diseases, 2nd ed.; Hodder Arnold: London, UK, 2005; pp. 501–503, 546–550. [Google Scholar]
- Jonsson, C.A.; Carlsten, H. Mycophenolic acid inhibits inosine 5′-monophosphate dehydrogenase and suppresses immunoglobulin and cytokine production of B cells. Int. Immunopharmacol. 2002, 3, 31–37. [Google Scholar] [CrossRef]
- Gu, J.J.; Stegmann, S.; Gathy, K.; Murray, R.; Laliberte, J.; Ayscue, L.; Mitchell, B.S. Inhibition of T lymphocyte activation in mice heterozygous for loss of the IMPDH II gene. J. Clin. Investig. 2000, 106, 599–606. [Google Scholar] [CrossRef] [Green Version]
- Long, I.P.; Althausen, A.F. Malacoplakia: A 25-year experience with a review of the literature. J. Urol. 1989, 141, 1328–1331. [Google Scholar] [CrossRef]
- Mitchell, A.; Dugas, A. Malakoplakia of the colon following renal transplantation in a 73 year old woman: Report of a case presenting as intestinal perforation. Diagn. Pathol. 2019, 14, 22. [Google Scholar] [CrossRef] [PubMed]
- Achufusi, T.G.; Jessamy, K.; Chebaya, P.; Rawlins, S. Rectal malakoplakia. Bayl. Univ. Med. Cent. Proc. 2020, 33, 389–390. [Google Scholar] [CrossRef]
- Yen, J.M.; Soh, N.W.Y.; Petersson, F.; Pandya, G. Rectosigmoid malakoplakia. BMJ Case Rep. 2017, 2017, bcr2017219464. [Google Scholar] [CrossRef] [PubMed]
- Guha, S.; Liu, H. Malakoplakia of the Pancreas with Simultaneous Colon Involvement: Case Report and Review of the Literature. Case Rep. Pathol. 2015, 2015, 649136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ennibi, K.; Mikdame, M.; Bahrouch, L.; Châari, J.; Toloune, F.; Archane, M.I. Malacoplakie digestive [Digestive malacoplakia]. Presse Med. 2002, 31, 1263–1265. (In French) [Google Scholar] [PubMed]
- Arenas Márquez, H.; López Neblina, F.; Barrera Torres, H.; Flores Márquez, M.R. Hemorragia masiva del aparato digestivo, secundaria a malacoplaquia colonica ulcerada [Massive hemorrhage of the digestive system secondary to ulcerated colonic malacoplakia]. Rev. Gastroenterol. Mex. 1994, 59, 49–51. (In Spanish) [Google Scholar] [PubMed]
- Musonza, T.; Tschen, J.A. Appendiceal malakoplakia masquerading as a cecal mass. J. Surg. Case Rep. 2020, 2020, rjaa140. [Google Scholar] [CrossRef] [PubMed]
- Díaz, A.R.L.; Pezet, S.G.; González, O.S.; Trueba, M.G.; Alonso, I.A.M.; Ramirez, M.A.L. Multivisceral Resection for Colonic Splenic Flexure Malakoplakia: A Minimally Invasive Approach. Ann. Coloproctol. 2021. Online ahead of print. [Google Scholar] [CrossRef]
- Koutserimpas, C.; Ioannidis, A.; Demonakou, M.; Siaperas, P.; Skarpas, A.; Velimezis, G.; Karanikas, I. Malakoplakia of the large intestine: An incidental extremely rare finding. G. Chir. 2018, 39, 97–100. [Google Scholar]
- Yared, R.A.; Badran, H.A.; Kamareddine, M.H.; Ghosn, Y.; Khalil, R.B.; El Ajamy, K.; Chouairy, C.; Farhat, S.G. Colonic Malakoplakia: A Rare Finding in a Healthy Male. Case Rep. Gastroenterol. 2018, 12, 453–456. [Google Scholar] [CrossRef]
- Hyun, K.H.; Shin, H.D.; Kim, D.H. Malakoplakia in a healthy young female patient. Korean J. Intern. Med. 2013, 28, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Shafijan, S. Colonic malakoplakia in a cardiac transplant recipient: A case report. Indian J. Pathol. Microbiol. 2020, 63, 322–324. [Google Scholar] [CrossRef] [PubMed]
- Krüger, S.; Katscher, T.; Johannisson, R.; Feller, A.C. Malakoplakie des Kolons [Malakoplakia of the colon]. Der Pathol. 1999, 20, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Mackay, E.H. Malakoplakia in ulcerative colitis. Arch. Pathol. Lab. Med. 1978, 102, 140–145. [Google Scholar]
- Taher, M.; Shahsia, R.; Daryani, N.E. Malakoplakia as a Rare Cause of Diarrhea: Case Presentation and Review of Literature. Middle East J. Dig. Dis. 2021, 13, 71–74. [Google Scholar] [CrossRef]
- Meredith, T.; Dharan, N.; Killen, L.; Anandabaskaran, S.; Kim, A.; Yang, T.; Marriott, D.; Hayward, C.; Macdonald, P. Colonic malakoplakia in a dual stem cell and cardiac transplant recipient: A case report and literature review. Transpl. Infect. Dis. 2020, 23, e13488. [Google Scholar] [CrossRef]
- Kim, P.T.; E Davis, J.; Erb, S.R.; Yoshida, E.M.; Steinbrecher, U.P. Colonic malakoplakia in a liver transplant recipient. Can. J. Gastroenterol. 2007, 21, 753–755. [Google Scholar] [CrossRef]
- Koklu, H.; Imamoglu, E.; Tseveldorj, N.; Sokmensuer, C.; Kav, T. Chronic Diarrhea Related to Colonic Malakoplakia Successfully Treated with Budesonide in a Kidney Transplant Recipient. Am. J. Gastroenterol. 2018, 113, 1906–1908. [Google Scholar] [CrossRef]
- Bae, G.E.; Yoon, N.; Park, H.Y.; Ha, S.Y.; Cho, J.; Lee, Y.; Kim, K.-M.; Park, C.K. Silent Colonic Malakoplakia in a Living-Donor Kidney Transplant Recipient Diagnosed during Annual Medical Examination. Korean J. Pathol. 2013, 47, 163–166. [Google Scholar] [CrossRef] [Green Version]
- Berger, S.; Marginean, C.; Kaur, M. A Case of Rectal Malakoplakia in an Immunocompromised Woman With Chronic Colonic Bacterial Infections. Clin. Gastroenterol. Hepatol. 2022, 20, A27–A28. [Google Scholar] [CrossRef]
- Ng, I.O.L.; Ng, M. Colonic malacoplakia: Unusual association with ulcerative colitis. J. Gastroenterol. Hepatol. 1993, 8, 110–115. [Google Scholar] [CrossRef] [PubMed]
- César Peres, L.; Barbieri Neto, J.; Rossi, M.A. Malacoplakia of the cecum: Report of a case. Acta Med. Port. 1984, 5, 281–283. [Google Scholar] [PubMed]
- Christensen, M.; Knuhtsen, S.; Knudsen, E. Malokoplaki i colon behandlet med sulfamethizol og trimetoprim [Colonic malacoplakia treated with sulfamethizole and trimethoprim]. Ugeskr. Laeger. 2011, 173, 509–510. (In Danish) [Google Scholar] [PubMed]
- Guinaudeau, E.; Person, B.; Valo, I.; Tuech, J.J.; Rousselet, M.C. Association d’une malacoplakie colique et d’une rectocolite hémorragique: À propos d’un cas [Colonic malacoplakia and ulcerative colitis: Report of a case]. Gastroenterol. Clin. Biol. 2002, 26, 174–177. (In French) [Google Scholar]
- De la Garza, T.; Nuñez-Rasilla, V.; Alegre-Palafox, R.; Albores-Saavedra, J. Malacoplakia of the colon: Report of a case, with a review of eight previous case reports. Dis. Colon Rectum 1973, 16, 216–223. [Google Scholar] [CrossRef]
- Yang, C.C.J.; Huang, T.Y.; Tsung, S.H.; Han, D.C.S. Rectal malacoplakia in a patient with Hodgkin’s disease. Dis. Colon Rectum 1983, 26, 129–132. [Google Scholar] [CrossRef]
- Le Bourgeois, P.; Parlier, H.R.; Gompel, H.E.; Baglin, A.C.; Lang, F.M.; Malafosse, M.; Lévy, R.E.; Betourné, C. Malakoplakie recto-colique diffuse: Association à une colite cryptogénétique et rémission après antibiothérapie prolongée [Diffuse recto-colic malacoplakia: Association with cryptogenic colitis and remission following long-term antibiotic therapy]. Gastroenterol. Clin. Biol. 1984, 8, 426–429. (In French) [Google Scholar]
- Irarrázaval-Mainguyague, M.J.; Cabreras, M.; Oksenberg, S.; A Pulgar, M.; Rojas, F.; Álvarez, M.; Quezada-Diaz, F.F. Malakoplakia mimicking a locally advanced colorectal neoplasm. J. Surg. Case Rep. 2021, 2021, rjab225. [Google Scholar] [CrossRef]
- Lee, M.; Ko, H.M.; Rubino, A.; Lee, H.; Gill, R.; Lagana, S.M. Malakoplakia of the gastrointestinal tract: Clinicopathologic analysis of 23 cases. Diagn. Pathol. 2020, 15, 97. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| organ transplantation |
| neoplasms |
| ulcerative colitis |
| malnutrition |
| tuberculosis |
| allergic conditions |
| sarcoidosis |
| poorly controlled diabetes |
| cytotoxic chemotherapy |
| acquired immunodeficiency syndrome (AIDS) |
| steroid use |
| alcohol abuse |
| Reference Article Number | Patient Gender | Patient Age | Clinical Presentation | Additional Findings | Location of the Lesion/s | Therapeutic Conduct | Evolution of the Patient |
|---|---|---|---|---|---|---|---|
| 1 | female | 72 | abdominal pain, vaginal bleeding | cadaveric renal transplant for chronic renal failure (10 months previously) | mesocolon—one adjacent to the descending colon and another involving the sigmoid colon | resection of the sigmoid lesion and a cutaneous fistula for the descending colon lesion | 9 months of antibiotic therapy relapse of the masses with the persistence of the lesions |
| 2 | male | 33 | painless hematochezia | warfarin therapy for lower-extremity deep venous thrombosis and a complex neurosurgical history, chemotherapy and radiation | nonobstructing circumferential mass in the rectum | biopsies and glucocorticoid therapy, followed by bowel resection | exitus by severe sepsis due to a urinary tract infection |
| 3 | female | 61 | lower respiratory tract infection | diabetes mellitus, hypertension and hyperlipidemia | multiple sessile and inflammatory colonic polyps with ulcerative edges | biopsies and antibiotic therapy | persistent cluster of polyps at rectosigmoid junction with no evidence of malakoplakia |
| 4 | male | 59 | asymptomatic | anemia | sessile polyp in the sigmoid colon and a second one within the ascending colona mass involving the pancreatic head | resection of the colonic polyps, antibiotic therapy, Whipple procedure | improvement after surgery recurrent ascites 3 months after surgery |
| 5 | 26 cases range from 24 to 83 years old | 16 women 10 men | abdominal pain, diarrhea, appendicitis | — | colorectum appendix stomach | biopsies and resections | favorable evolution with no additional instances of malakoplakia |
| 6 | male | 37 | chronic diarrhea | edematous-ascitic syndrome and bilateral pleurisy | tumoral stenosis of the sigmoid-colic junction | wide left colectomy | improvement after surgery |
| 7 | female | 55 | massive hemorrhage of the rectum | — | duodenum, colon and lymph nodes in the mesentery | laparotomy and proctocolectomy | — |
| 8 | male | 66 | abdominal pain and chronic intermittent diarrhea | compensated alcoholic liver disease, hypertension, emphysema, chronic obstructive pulmonary disease and irritable bowel syndrome | multiple polyps in the ascending, descending and sigmoid colon cecal mass | biopsies laparoscopic right hemicolectomy | — |
| 9 | female | 38 | lower gastrointestinal hemorrhage | diabetes | splenic flexure mass involving the spleen and the left kidney | biopsies antibiotic therapy laparoscopic en bloc colectomy and partial nephrectomy | pancreatic fistula postoperatively, successfully treated with percutaneous drainage and antibiotics |
| 10 | male | 68 | abdominal pain | — | incarcerated ventral hernia and sigmoid-colon rupture | Hartmann’s procedure, antibiotic therapy associated with cholinergic agonists (bethanechol and ascorbic acid) | reversal of the Hartmann’s procedure 4 months after the initial surgery |
| 11 | male | 65 | abdominal pain and unintentional weight loss | — | lesion of the transverse colon | antibiotic therapy | — |
| 12 | female | 19 | low abdominal pain and multiple loose stools with blood for the last 3 months | — | multiple polyps throughout the colon, particularly in the sigmoid colon | antibiotic therapy associated with cholinergic agonists (bethanechol and ascorbic acid) for 6 months | abnormal colonoscopy findings were remarkably improved after 6 months of follow-up, and returned to normal after the end of 12 months currently healthy |
| 13 | male | 38 | 6 months history of diarrhea associated with fecal incontinence | cardiac transplant 4 years previously for severe heart failure due to dilated cardiomyopathy | upper gastrointestinal endoscopy was normal and the mucosa of ileum and colon was colonoscopically normal | rectal biopsies and antibiotic therapy | 1 month later, the patient did not have diarrhea |
| 14 | female | 62 | melena | — | polypoid lesions of the cecum | antibiotic therapy | no melena detectable over a period of 6 months |
| 15 | female | — | — | 30-years history of ulcerative colitis | — | proctocolectomy after failure of medical therapy | — |
| 16 | male | 58 | abdominal cramps and chronic diarrhea | unintentional weight loss, Sjogren syndrome and lupus nephritis | multiple polyps in the rectum | biopsies and antibiotic therapy | symptoms improved after 3 months of follow-up |
| 17 | male | — | persistent diarrhea and recurrent E coli bacteremia | dual stem cell and cardiac transplant recipient | areas of colonic thickening | biopsies antimicrobial therapy and reduction of immunosuppression | exitus from sepsis |
| 18 | female | 58 | chronic diarrhea | liver transplant recipient | patchy mucosal edema | biopsies antibiotic therapy and reduction of immunosuppression | — |
| 19 | female | 51 | chronic recurrent diarrhea | kidney transplant surgery and hypertension | flat elevated lesions involving the ascending colon | biopsies and corticosteroids therapy | no recurring symptoms during the 9-month follow-up |
| 20 | female | 55 | routine cancer surveillance | liver transplant and a second liver transplant 10 months later | diffuse wall thickening of the sigmoid colon | biopsies no therapy | no symptoms at the 1 year check-up |
| 21 | female | 45 | diarrhea and unintentional weight loss | variable immunodeficiency and interstitial lung disease | multiple mucosal nodules in the rectum | biopsies and antibiotic therapy | improvement of the symptoms |
| 22 | female | 44 | — | ulcerative colitis | colon | discontinuation of high-dose systemic steroid | gradually remissions of the symptoms |
| 23 | male | 56 | palpable, movable and painful tumoral mass in the right iliac fossa | paracoccidioidal osteomyelitis of the right clavicle and the 6th left rib one and two years previously | mucosal irregularities and wall stiffness in the cecum and diverticulosis of the colon | — | exitus by bilateral bronchopneumo- nia and acute renal failure |
| 24 | female | 78 | diarrhea and malaise | anemia and elevated inflammatory parameters | macroscopic yellowish nodular changes throughout the colon | biopsies and antibiotic therapy | remission of the pathology after 3 months of antibiotic therapy |
| 25 | female | 58 | — | ulcerative colitis | colonic perforation was suspected | sub-total colectomy and antibiotic therapy | gradually disappearance of malakoplakia |
| 26 | female | 47 | — | emaciated | the ascending and transverse portions of the colon | — | exitus by large intestinal obstruction syndrome |
| 27 | male | 37 | rectal bleeding | stage IV Hodgkin disease | sigmoid colon | biopsies | — |
| 28 | male | 22 | fever, rectal bleeding with fistula | inflammatory bowel disease | pseudo tumoral masses and multiple colorectal ulcerations | biopsies and colonic diversion associated with broad spectrum antibiotherapy | favorable outcome |
| 29 | male | 75 | intense abdominal pain | elevated serum creatinine, elevated glycated hemoglobin and urinary infection | parietal thickening of the descending colon, left kidney, iliopsoas muscle and retroperitoneum involvement | surgery for symptomatic colonic neoplasm—left segmental colectomy, left partial nephrectomy and retroperitoneal soft tissue resection | — |
| 30 | 23 cases 11 males and 12 females | mean age 57 | diagnostic screening (n = 7) diarrhea (n = 3) rule out rejection (n = 1) gastrointestinal bleeding (n = 1) abdominal pain (n = 1) follow up of Barrett’s esophagus (n = 1) | most patients were immuno-suppressed (organ transplantation n = 4, cancer n = 9, autoimmune condition n = 5 and/or medication effect | sigmoid colon, rectum (n = 10) transverse and descending colon (n = 4) stomach/gastroesophageal junction (n = 4) appendix (n = 2) cecum (n = 1) small bowel (n = 1) perianal area (n = 1) | biopsies and resections | — |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Șerban, C.; Toma, A.; Voicu, D.C.; Popazu, C.; Firescu, D.; Țocu, G.; Mihailov, R.; Rebegea, L. A Surgical Challenge Generated by Colonic Malakoplakia in Disguise as a Locally Advanced Colonic Malignancy—A Case Report. Medicina 2023, 59, 156. https://doi.org/10.3390/medicina59010156
Șerban C, Toma A, Voicu DC, Popazu C, Firescu D, Țocu G, Mihailov R, Rebegea L. A Surgical Challenge Generated by Colonic Malakoplakia in Disguise as a Locally Advanced Colonic Malignancy—A Case Report. Medicina. 2023; 59(1):156. https://doi.org/10.3390/medicina59010156
Chicago/Turabian StyleȘerban, Cristina, Alexandra Toma, Dragoș Cristian Voicu, Constantin Popazu, Dorel Firescu, George Țocu, Raul Mihailov, and Laura Rebegea. 2023. "A Surgical Challenge Generated by Colonic Malakoplakia in Disguise as a Locally Advanced Colonic Malignancy—A Case Report" Medicina 59, no. 1: 156. https://doi.org/10.3390/medicina59010156